Effect of a Supervised Aerobic Exercise Training Program and Ginkgo Biloba Extract on Metabolic Parameters and Functional Capacity in HIV-Infected Subjects


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Approval of the Study
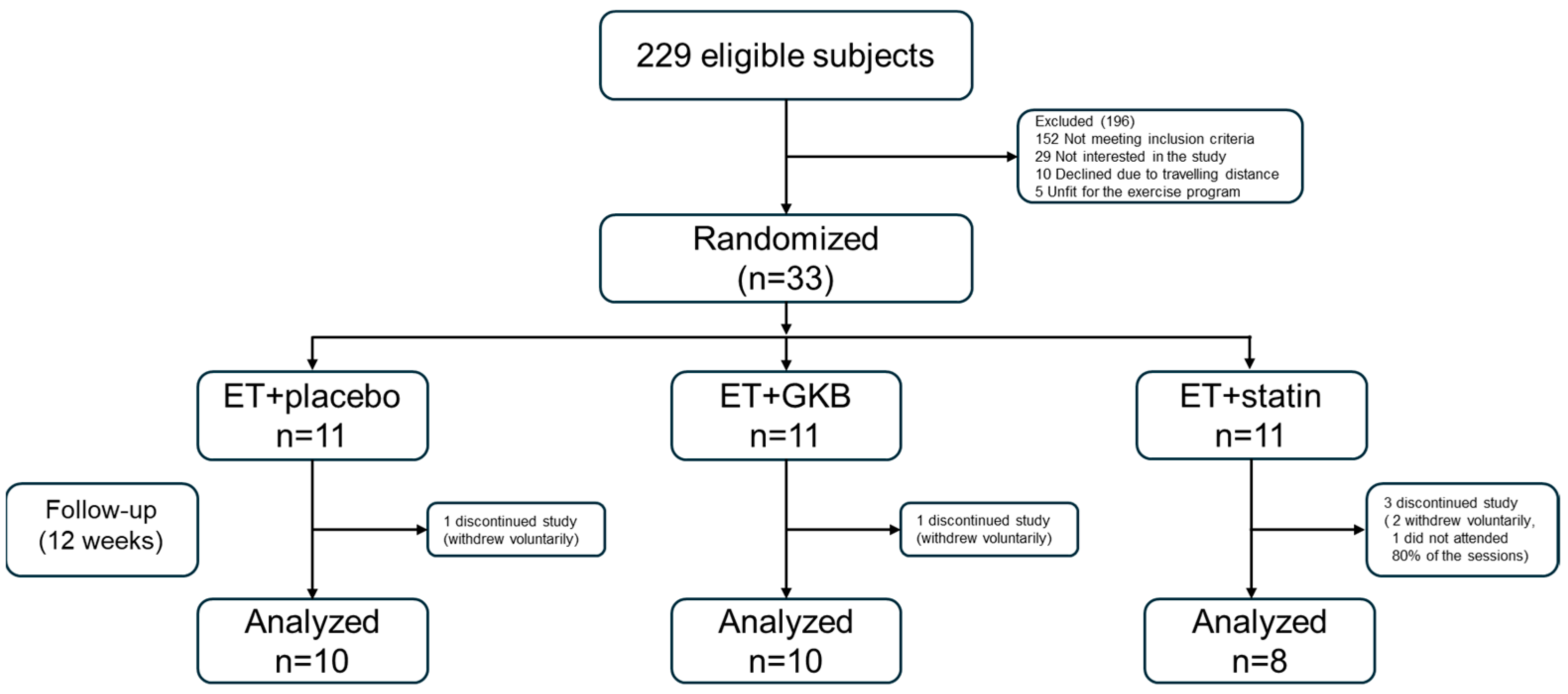
2.2. Randomization and Blinding
2.3. Procedures
2.4. Funcional Capacity Measurements
2.5. Blood Sample Collection and Processing
2.6. Statistical Analysis
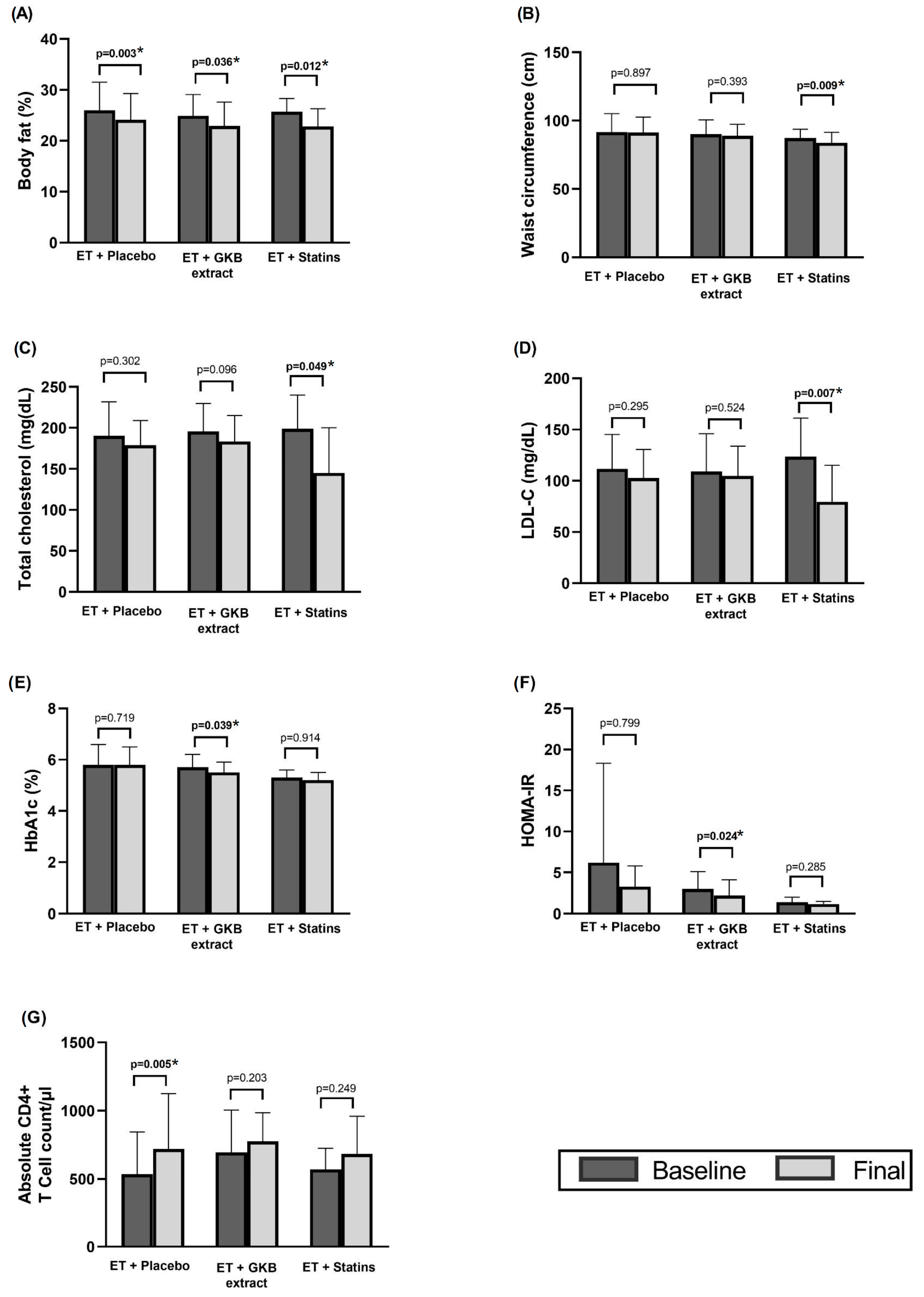
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marcus, J.L.; Leyden, W.A.; Alexeeff, S.E.; Anderson, A.N.; Hechter, R.C.; Hu, H.; Lam, J.O.; Towner, W.J.; Yuan, Q.; Horberg, M.A.; et al. Comparison of Overall and Comorbidity-Free Life Expectancy Between Insured Adults with and Without HIV Infection, 2000–2016. JAMA Netw. Open 2020, 3, e207954. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Westfall, A.O.; Chamot, E.; Willig, A.L.; Mugavero, M.J.; Ritchie, C.; Burkholder, G.A.; Crane, H.M.; Raper, J.L.; Saag, M.S.; et al. Multimorbidity Patterns in HIV-Infected Patients: The Role of Obesity in Chronic Disease Clustering. JAIDS J. Acquir. Immune Defic. Syndr. 2012, 61, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.V.; Stelzle, D.; Lee, K.K.; Beck, E.J.; Alam, S.; Clifford, S.; Longenecker, C.T.; Strachan, F.; Bagchi, S.; Whiteley, W.; et al. Global Burden of Atherosclerotic Cardiovascular Disease in People Living with HIV. Circulation 2018, 138, 1100–1112. [Google Scholar] [CrossRef]
- Hsue, P.Y.; Waters, D.D. Time to Recognize HIV Infection as a Major Cardiovascular Risk Factor. Circulation 2018, 138, 1113–1115. [Google Scholar] [CrossRef]
- Vachiat, A.; McCutcheon, K.; Tsabedze, N.; Zachariah, D.; Manga, P. HIV and Ischemic Heart Disease. J. Am. Coll. Cardiol. 2017, 69, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Lu, M.T.; Foldyna, B.; Zanni, M.V.; Karady, J.; Taron, J.; Zhai, B.K.; Burdo, T.; Fitch, K.V.; Kileel, E.M.; et al. Assessment of Coronary Artery Disease with Computed Tomography Angiography and Inflammatory and Immune Activation Biomarkers Among Adults with HIV Eligible for Primary Cardiovascular Prevention. JAMA Netw. Open 2021, 4, e2114923. [Google Scholar] [CrossRef]
- Farahani, M.; Mulinder, H.; Farahani, A.; Marlink, R. Prevalence and Distribution of Non-AIDS Causes of Death among HIV-Infected Individuals Receiving Antiretroviral Therapy: A Systematic Review and Meta-Analysis. Int. J. STD AIDS 2017, 28, 636–650. [Google Scholar] [CrossRef]
- Sax, P.E.; Erlandson, K.M.; Lake, J.E.; McComsey, G.A.; Orkin, C.; Esser, S.; Brown, T.T.; Rockstroh, J.K.; Wei, X.; Carter, C.C.; et al. Weight Gain Following Initiation of Antiretroviral Therapy: Risk Factors in Randomized Comparative Clinical Trials. Clin. Infect. Dis. 2020, 71, 1379–1389. [Google Scholar] [CrossRef]
- Lake, J.E.; Trevillyan, J. Impact of Integrase Inhibitors and Tenofovir Alafenamide on Weight Gain in People with HIV. Curr. Opin. HIV AIDS 2021, 16, 148–151. [Google Scholar] [CrossRef]
- Mallon, P.W.; Brunet, L.; Hsu, R.K.; Fusco, J.S.; Mounzer, K.C.; Prajapati, G.; Beyer, A.P.; Wohlfeiler, M.B.; Fusco, G.P. Weight Gain before and after Switch from TDF to TAF in a U.S. Cohort Study. J. Int. AIDS Soc. 2021, 24, e25702. [Google Scholar] [CrossRef]
- Neves, J.S.; Guerreiro, V.; Carvalho, D.; Serrão, R.; Sarmento, A.; Freitas, P. Metabolically Healthy or Metabolically Unhealthy Obese HIV-Infected Patients: Mostly a Matter of Age? Front. Endocrinol. 2018, 9, 681. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, J.A.; Sahrmann, J.; Parra-Rodriguez, L.; Vo, D.T.; Butler, A.M.; Olsen, M.A.; Powderly, W.G. Integrase Strand Transfer Inhibitors Are Associated with Incident Diabetes Mellitus in People with Human Immunodeficiency Virus. Clin. Infect. Dis. 2022, 75, 2060–2065. [Google Scholar] [CrossRef] [PubMed]
- Ozemek, C.; Erlandson, K.M.; Jankowski, C.M. Physical Activity and Exercise to Improve Cardiovascular Health for Adults Living with HIV. Prog. Cardiovasc. Dis. 2020, 63, 178–183. [Google Scholar] [CrossRef]
- Voigt, N.; Cho, H.; Schnall, R. Supervised Physical Activity and Improved Functional Capacity among Adults Living with HIV: A Systematic Review. J. Assoc. Nurses AIDS Care 2018, 29, 667–680. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, K.L.; Borges, J.P.; Lopes, G.d.; Pereira, E.N.G.d.S.; Mediano, M.F.F.; Farinatti, P.; Tibiriça, E.; Daliry, A. Influence of Physical Exercise on Advanced Glycation End Products Levels in Patients Living with the Human Immunodeficiency Virus. Front. Physiol. 2018, 9, 1641. [Google Scholar] [CrossRef] [PubMed]
- Pérez Chaparro, C.G.A.; Zech, P.; Schuch, F.; Wolfarth, B.; Rapp, M.; Heiβel, A. Effects of Aerobic and Resistance Exercise Alone or Combined on Strength and Hormone Outcomes for People Living with HIV. A Meta-Analysis. PLoS ONE 2018, 13, e0203384. [Google Scholar] [CrossRef]
- O’Brien, K.K.; Tynan, A.-M.; Nixon, S.A.; Glazier, R.H. Effectiveness of Aerobic Exercise for Adults Living with HIV: Systematic Review and Meta-Analysis Using the Cochrane Collaboration Protocol. BMC Infect. Dis. 2016, 16, 182. [Google Scholar] [CrossRef]
- Martin, K.; Naclerio, F.; Karsten, B.; Vera, J.H. Physical Activity and Quality of Life in People Living with HIV. AIDS Care 2019, 31, 589–598. [Google Scholar] [CrossRef]
- Oursler, K.K.; Sorkin, J.D.; Ryan, A.S.; Katzel, L.I. A Pilot Randomized Aerobic Exercise Trial in Older HIV-Infected Men: Insights into Strategies for Successful Aging with HIV. PLoS ONE 2018, 13, e0198855. [Google Scholar] [CrossRef]
- Zanetti, H.R.; da Cruz, L.G.; Lourenço, C.L.M.; Neves, F.d.F.; Silva-Vergara, M.L.; Mendes, E.L. Non-linear Resistance Training Reduces Inflammatory Biomarkers in Persons Living with HIV: A Randomized Controlled Trial. Eur. J. Sport Sci. 2016, 16, 1232–1239. [Google Scholar] [CrossRef]
- Zanetti, H.R.; da Cruz, L.G.; Lourenço, C.L.M.; Ribeiro, G.C.; de Jesus Leite, M.A.F.; Neves, F.F.; Silva-Vergara, M.L.; Mendes, E.L. Nonlinear Resistance Training Enhances the Lipid Profile and Reduces Inflammation Marker in People Living with HIV: A Randomized Clinical Trial. J. Phys. Act. Health 2016, 13, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Santos, W.R.; Santos, W.R.; Paes, P.P.; Ferreira-Silva, I.A.; Santos, A.P.; Vercese, N.; Machado, D.R.L.; de Paula, F.J.A.; Donadi, E.A.; Navarro, A.M.; et al. Impact of Strength Training on Bone Mineral Density in Patients Infected with HIV Exhibiting Lipodystrophy. J. Strength Cond. Res. 2015, 29, 3466–3471. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Mugisha, J.; De Hert, M.; Probst, M.; Firth, J.; Gorczynski, P.; Stubbs, B. Global Physical Activity Levels among People Living with HIV: A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2018, 40, 388–397. [Google Scholar] [CrossRef]
- Biernacka, P.; Adamska, I.; Felisiak, K. The Potential of Ginkgo biloba as a Source of Biologically Active Compounds—A Review of the Recent Literature and Patents. Molecules 2023, 28, 3993. [Google Scholar] [CrossRef]
- Rodríguez, M.; Ringstad, L.; Schäfer, P.; Just, S.; Hofer, H.W.; Malmsten, M.; Siegel, G. Reduction of Atherosclerotic Nanoplaque Formation and Size by Ginkgo biloba (EGb 761) in Cardiovascular High-Risk Patients. Atherosclerosis 2007, 192, 438–444. [Google Scholar] [CrossRef]
- Zhou, W.; Chai, H.; Lin, P.H.; Lumsden, A.B.; Yao, Q.; Chen, C. Clinical Use and Molecular Mechanisms of Action of Extract of Ginkgo biloba Leaves in Cardiovascular Diseases. Cardiovasc. Drug Rev. 2004, 22, 309–319. [Google Scholar] [CrossRef]
- Mahady, G.B. Ginkgo biloba for the Prevention and Treatment of Cardiovascular Disease: A Review of the Literature. J. Cardiovasc. Nurs. 2002, 16, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Eisvand, F.; Razavi, B.M.; Hosseinzadeh, H. The Effects of Ginkgo biloba on Metabolic Syndrome: A Review. Phytother. Res. 2020, 34, 1798–1811. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yang, L.; Yang, F.; Zhao, X.; Xue, S.; Gong, F. Ginkgo biloba Extract 50 (GBE50) Ameliorates Insulin Resistance, Hepatic Steatosis and Liver Injury in High Fat Diet-Fed Mice. J. Inflamm. Res. 2021, 14, 1959–1971. [Google Scholar] [CrossRef]
- Aziz, T.; Hussain, S.; Mahwi, T.; Ahmed, Z.A.; Rahman, H.; Rasedee, A. The Efficacy and Safety of Ginkgo biloba Extract as an Adjuvant in Type 2 Diabetes Mellitus Patients Ineffectively Managed with Metformin: A Double-Blind, Randomized, Placebo-Controlled Trial. Drug Des. Devel Ther. 2018, 12, 735–742. [Google Scholar] [CrossRef]
- Smith, B.A.; Neidig, J.L.; Nickel, J.T.; Mitchell, G.L.; Para, M.F.; Fass, R.J. Aerobic Exercise: Effects on Parameters Related to Fatigue, Dyspnea, Weight and Body Composition in HIV-Infected Adults. AIDS 2001, 15, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Farahat, F.M.; Alghamdi, Y.S.; Farahat, A.F.; Alqurashi, A.A.; Alburayk, A.K.; Alabbasi, A.A.; Alsaedi, A.A.; Alshamrani, M.M. The Prevalence of Comorbidities among Adult People Diagnosed with HIV Infection in a Tertiary Care Hospital in Western Saudi Arabia. J. Infect. Public Health 2020, 13, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Buchner, D.; Piña, I.L.; Balady, G.J.; Williams, M.A.; Marcus, B.H.; Berra, K.; Blair, S.N.; Costa, F.; Franklin, B.; et al. Exercise and Physical Activity in the Prevention and Treatment of Atherosclerotic Cardiovascular Disease. Circulation 2003, 107, 3109–3116. [Google Scholar] [CrossRef] [PubMed]
- Rossomanno, C.I.; Herrick, J.E.; Kirk, S.M.; Kirk, E.P. A 6-Month Supervised Employer-Based Minimal Exercise Program for Police Officers Improves Fitness. J. Strength Cond. Res. 2012, 26, 2338–2344. [Google Scholar] [CrossRef]
- Vancampfort, D.; Mugisha, J.; Richards, J.; De Hert, M.; Lazzarotto, A.R.; Schuch, F.B.; Probst, M.; Stubbs, B. Dropout from Physical Activity Interventions in People Living with HIV: A Systematic Review and Meta-Analysis. AIDS Care 2017, 29, 636–643. [Google Scholar] [CrossRef]
- Mutimura, E.; Crowther, N.J.; Cade, T.W.; Yarasheski, K.E.; Stewart, A. Exercise Training Reduces Central Adiposity and Improves Metabolic Indices in HAART-Treated HIV-Positive Subjects in Rwanda: A Randomized Controlled Trial. AIDS Res. Hum. Retroviruses 2008, 24, 15–23. [Google Scholar] [CrossRef]
- Brito-Neto, J.G.d.; Andrade, M.F.d.; Almeida, V.D.d.; Paiva, D.C.C.; Morais, N.M.d.; Bezerra, C.M.; Fernandes, J.V.; Nascimento, E.G.C.d.; Fonseca, I.A.T.; Fernandes, T.A.A.d.M. Strength Training Improves Body Composition, Muscle Strength and Increases CD4+ T Lymphocyte Levels in People Living with HIV/AIDS. Infect. Dis. Rep. 2019, 11, 7925. [Google Scholar] [CrossRef]
- Gomes Neto, M.; Conceição, C.S.; Carvalho, V.O.; Brites, C. Effects of Combined Aerobic and Resistance Exercise on Exercise Capacity, Muscle Strength and Quality of Life in HIV-Infected Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138066. [Google Scholar] [CrossRef]
- Barrón-Cabrera, E.; Soria-Rodríguez, R.; Amador-Lara, F.; Martínez-López, E. Physical Activity Protocols in Non-Alcoholic Fatty Liver Disease Management: A Systematic Review of Randomized Clinical Trials and Animal Models. Healthcare 2023, 11, 1992. [Google Scholar] [CrossRef]
- Duncan, A.D.; Peters, B.S.; Rivas, C.; Goff, L.M. Reducing Risk of Type 2 Diabetes in HIV: A Mixed-methods Investigation of the STOP-Diabetes Diet and Physical Activity Intervention. Diabet. Med. 2020, 37, 1705–1714. [Google Scholar] [CrossRef]
- Hernández-Lepe, M.A.; Ortiz-Ortiz, M.; Hernández-Ontiveros, D.A.; Mejía-Rangel, M.J. Inflammatory Profile of Older Adults in Response to Physical Activity and Diet Supplementation: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4111. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Pinacchio, C.; Santinelli, L.; Adami, P.E.; Borrazzo, C.; Cavallari, E.N.; Vullo, A.; Innocenti, G.P.; Mezzaroma, I.; Mastroianni, C.M.; et al. Physical Activity and HIV: Effects on Fitness Status, Metabolism, Inflammation and Immune-Activation. AIDS Behav. 2020, 24, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Chenciner, L.; Barber, T.J. Non-Infective Complications for People Living with HIV. Medicine 2022, 50, 304–307. [Google Scholar] [CrossRef]
- Mhlanga, N.L.; Netangaheni, T.R. Risks of Type 2 Diabetes among Older People Living with HIV: A Scoping Review. S. Afr. Fam. Pract. 2023, 65, e1–e10. [Google Scholar] [CrossRef]
- Kudolo, G.B. The Effect of 3-Month Ingestion of Ginkgo biloba Extract (EGb 761) on Pancreatic Β-Cell Function in Response to Glucose Loading in Individuals with Non-Insulin-Dependent Diabetes Mellitus. J. Clin. Pharmacol. 2001, 41, 600–611. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Meng, Q.; Qian, T.; Yang, Z. Ginkgo biloba Extract Enhances Glucose Tolerance in Hyperinsulinism-Induced Hepatic Cells. J. Nat. Med. 2011, 65, 50–56. [Google Scholar] [CrossRef]
- Kubota, N.; Tobe, K.; Terauchi, Y.; Eto, K.; Yamauchi, T.; Suzuki, R.; Tsubamoto, Y.; Komeda, K.; Nakano, R.; Miki, H.; et al. Disruption of Insulin Receptor Substrate 2 Causes Type 2 Diabetes Because of Liver Insulin Resistance and Lack of Compensatory Beta-Cell Hyperplasia. Diabetes 2000, 49, 1880–1889. [Google Scholar] [CrossRef]
- Dell’Agli, M.; Bosisio, E. Biflavones of Ginkgo biloba Stimulate Lipolysis in 3T3-L1 Adipocytes. Planta Med. 2002, 68, 76–79. [Google Scholar] [CrossRef]
- Siegel, G.; Ermilov, E.; Knes, O.; Rodríguez, M. Combined Lowering of Low Grade Systemic Inflammation and Insulin Resistance in Metabolic Syndrome Patients Treated with Ginkgo biloba. Atherosclerosis 2014, 237, 584–588. [Google Scholar] [CrossRef]
- Bonora, E.; Kiechl, S.; Willeit, J.; Oberhollenzer, F.; Egger, G.; Meigs, J.B.; Bonadonna, R.C.; Muggeo, M. Insulin Resistance as Estimated by Homeostasis Model Assessment Predicts Incident Symptomatic Cardiovascular Disease in Caucasian Subjects From the General Population. Diabetes Care 2007, 30, 318–324. [Google Scholar] [CrossRef]
- Zuliani, G.; Morieri, M.L.; Volpato, S.; Maggio, M.; Cherubini, A.; Francesconi, D.; Bandinelli, S.; Paolisso, G.; Guralnik, J.M.; Ferrucci, L. Insulin Resistance and Systemic Inflammation, but Not Metabolic Syndrome Phenotype, Predict 9 Years Mortality in Older Adults. Atherosclerosis 2014, 235, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Ausk, K.J.; Boyko, E.J.; Ioannou, G.N. Insulin Resistance Predicts Mortality in Nondiabetic Individuals in the U.S. Diabetes Care 2010, 33, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Blaha, M.J.; DeFilippis, A.P.; Rivera, J.J.; Budoff, M.J.; Blankstein, R.; Agatston, A.; Szklo, M.; Lakoski, S.G.; Bertoni, A.G.; Kronmal, R.A.; et al. The Relationship Between Insulin Resistance and Incidence and Progression of Coronary Artery Calcification. Diabetes Care 2011, 34, 749–751. [Google Scholar] [CrossRef]
- Banin, R.M.; Hirata, B.K.S.; Andrade, I.S.; Zemdegs, J.C.S.; Clemente, A.P.G.; Dornellas, A.P.S.; Boldarine, V.T.; Estadella, D.; Albuquerque, K.T.; Oyama, L.M.; et al. Beneficial Effects of Ginkgo biloba Extract on Insulin Signaling Cascade, Dyslipidemia, and Body Adiposity of Diet-Induced Obese Rats. Braz. J. Med. Biol. Res. 2014, 47, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Hypocholesterolemic Effect of Ginkgo biloba Seeds Extract from High Fat Diet Mice. Biomed. Sci. Lett. 2017, 23, 138–143. [Google Scholar] [CrossRef]
- Hirata, B.K.S.; Cruz, M.M.; de Sá, R.D.C.C.; Farias, T.S.M.; Machado, M.M.F.; Bueno, A.A.; Alonso-Vale, M.I.C.; Telles, M.M. Potential Anti-Obesogenic Effects of Ginkgo biloba Observed in Epididymal White Adipose Tissue of Obese Rats. Front. Endocrinol. 2019, 10, 284. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, G.; Wu, D.; Zhu, L.; Ma, B.; Du, Y. Application of GC/MS-Based Metabonomic Profiling in Studying the Lipid-Regulating Effects of Ginkgo biloba Extract on Diet-Induced Hyperlipidemia in Rats. Acta Pharmacol. Sin. 2009, 30, 1674–1687. [Google Scholar] [CrossRef]
- Jie, L.; Hai, H. Clinical Observation of Gingko Biloba Extract Injection in Treating Early Diabetic Nephropathy. Chin. J. Integr. Med. 2005, 11, 226–228. [Google Scholar] [CrossRef]
- Cheng, D.; Liang, B.; Li, Y. Antihyperglycemic Effect of Ginkgo biloba Extract in Streptozotocin-Induced Diabetes in Rats. Biomed. Res. Int. 2013, 2013, 162724. [Google Scholar] [CrossRef]
- Zanetti, H.R.; Gonçalves, A.; Teixeira Paranhos Lopes, L.; Mendes, E.L.; Roever, L.; Silva-Vergara, M.L.; Neves, F.F.; Resende, E.S. Effects of Exercise Training and Statin Use in People Living with Human Immunodeficiency Virus with Dyslipidemia. Med. Sci. Sports Exerc. 2020, 52, 16–24. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics |
ET + Placebo n = 10 |
ET + GKB n = 10 |
ET + Statin n = 8 | p Value |
|---|---|---|---|---|
| Mean age, years (SD) | 41.8 ± 11.0 | 41.8 ± 7.0 | 40.5 ± 10.5 | 0.949 |
| Weight (kg) | 80.7 ± 13.3 | 75.9 ± 12.4 | 76.2 ± 12.5 | 0.277 |
| Waist circumference (cm) | 91.6 ± 13.6 | 90.0 ± 10.5 | 87.2 ± 6.5 | 0.695 |
| Waist-to-hip ratio | 0.90 ± 0.10 | 0.95 ± 0.07 | 0.90 ± 0.05 | 0.253 |
| Waist-to-height ratio | 0.53 ± 0.08 | 0.53 ± 0.08 | 0.52 ± 0.04 | 0.906 |
| BMI (kg/m2) | 28.0 ± 4.1 | 26.6 ± 4.2 | 25.7 ± 2.6 | 0.854 |
| Sum of 8 skinfolds (mm) | 118.8 ± 47.7 | 127.6 ± 40.8 | 129.6 ± 43.9 | 0.855 |
| Body fat mass (%) | 26.0 ± 5.5 | 24.9 ± 4.2 | 25.7 ± 2.6 | 0.854 |
| Lean body mass (%) | 39.0 ± 6.4 | 40.3 ± 4.9 | 40.2 ± 3.4 | 0.827 |
| Bone mass (%) | 13.7 ± 1.4 | 14.3 ± 1.5 | 14.2 ± 0.8 | 0.560 |
| Absolute CD4+ T Cell count/μL, mean | 534.3 ± 310.4 | 694.2 ± 310.1 | 570.6 ± 154.6 | 0.171 |
| HIV-1 RNA (copies/mL), mean | 34.5 (28.7–39.0) | 31.0 (31.0–34.2) | 35.0 (31.0–39.0) | 0.394 |
| Total billirrubin (mg/dL) | 0.80 ± 0.4 | 0.63 ± 0.2 | 0.58 ± 0.2 | 0.683 |
| Direct billirrubin (mg/dL) | 0.14 ± 0.05 | 0.11 ± 0.03 | 0.11 ± 0.06 | 0.335 |
| Total protein (g/dL) | 7.2 ± 0.5 | 7.2 ± 0.4 | 7.1 ± 0.3 | 0.933 |
| Albumin (g/dL) | 4.2 ± 0.1 | 4.2 ± 0.2 | 4.3 ± 0.2 | 0.518 |
| Globulin (g/dL) | 3.1 ± 0.5 | 2.9 ± 0.4 | 2.7 ± 0.4 | 0.374 |
| Alanine aminotransferase (IU/L) | 31.8 ± 11.2 | 36.8 ± 55.0 | 18.7 ± 5.4 | 0.024 * |
| Aspartate aminotransferase (IU/L) | 22.0 ± 5.9 | 30.1 ± 29.0 | 17.2 ± 4.5 | 0.061 |
| Gamma-glutamyl transpeptidase (IU/L) | 45.8 ± 31.0 | 35.7 ± 32.4 | 27.3 ± 15.7 | 0.273 |
| Alkaline phosphatase (IU/L) | 79.7 ± 21.4 | 73.6 ± 14.8 | 69.2 ± 19.5 | 0.533 |
| Lactate dehydrogenase (U/L) | 159.1 ± 35.7 | 174.1 ± 41.2 | 156.8 ± 22.7 | 0.514 |
| Urea (mg/dL) | 34.0 ± 10.9 | 28.3 ± 7.7 | 41.2 ± 11.2 | 0.039 * |
| BUN (mg/dL) | 15.8 ± 5.0 | 13.2 ± 3.5 | 19.3 ± 3.5 | 0.035 * |
| Creatinine (mg/dL) | 0.91 ± 0.12 | 0.096 ± 0.12 | 1.04 ± 0.19 | 0.213 |
| Prothrombin time | 10.8 ± 0.9 | 11.0 ± 0.4 | 10.7 ± 0.6 | 0.824 |
| INR | 0.97 ± 0.09 | 1.00 ± 0.04 | 0.93 ± 0.08 | 0.258 |
| Partial thromboplastin time | 32.4 ± 2.5 | 33.6 ± 4.5 | 31.4 ± 2.7 | 0.487 |
| Fibrinogen (mg/dL) | 421.4 ± 73.9 | 459.0 ± 93.6 | 422.6 ± 82.9 | 0.559 |
| Characteristics |
ET + Placebo
n = 10 |
ET+ GKB
n = 10 |
ET+ Statin
n = 8 | p Value |
|---|---|---|---|---|
| Total cholesterol (mg/dL) | −11.5 ± 33.2 | −12.3 ± 20.9 | −53.7 ± 63.9 | 0.044 * |
| HDL cholesterol (mg/dL) | 0.5 ± 9.1 | 2.1 ± 3.5 | 1.8 ± 7.9 | 0.882 |
| LDL cholesterol (mg/dL) | −8.9 ± 25.3 | −4.3 ± 20.5 | −44.0 ± 32.5 | 0.426 |
| Triglycerides (mg/dL) | −9.5 ± 93.9 | −27.0 ± 90.1 | −0.8 ± 141.5 | 0.522 |
| Glucose (mg/dL) | −5.9 ± 22.2 | −2.4 ± 11.1 | −2.6 ± 19.6 | 0.687 |
| Insulin (µU/mL) | −4.4 ± 20.5 | −3.0 ± 2.7 | −0.9 ± 2.2 | 0.107 |
| Glycated hemoglobin A1c (%) | −0.0 ± 0.2 | −0.1 ± 0.2 | 0.0 ± 0.2 | 0.340 |
| HOMA-IR † | −2.9 ± 10.0 | −0.7 ± 0.7 | −0.2 ± 0.5 | 0.119 |
| Triglycerides/HDL-c ratio | 0.1 ± 2.6 | −1.4 ± 3.0 | −0.6 ± 3.4 | 0.903 |
| Variable |
ET + Placebo n = 10 |
ET + GKB n = 10 |
ET + Statin n = 8 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Basal | Final | p Value | Basal | Final | p Value | Basal | Final | p Value | |
| VO2Máx † | 47.9 ± 5.3 | 59.9 ± 8.9 | 0.001 ** | 46.5 ± 10.1 | 55.0 ± 7.4 | 0.002 ** | 45.0 ± 4.2 | 58.9 ± 7.0 | 0.000 *** |
| Grip strength in non-dominant hand (Kg) | 31.2 ± 5.4 | 33.3 ± 9.0 | 0.333 † | 61.9 ± 90.1 | 33.4 ± 4.9 | 0.674 † | 34.2 ± 8.6 | 346 ± 6.4 | 0.838 |
| Grip strength in dominant hand (Kg) | 33.7 ± 8.6 | 33.3 ± 11.9 | 0.849 | 34.4 ± 4.1 | 35.6 ± 6.1 | 0.380 | 35.6 ± 6.1 | 37.8 ± 6.1 | 0.297 |
| Back strength (Kg) | 36.5 ± 20.7 | 42.8 ± 18.1 | 0.272 | 32.6 ± 11.4 | 40.0 ± 12.9 | 0.025 * | 39.3 ± 18.1 | 39.2 ± 15.0 | 0.978 |
| Lower limb strength (Kg) | 37.7 ± 13.6 | 42.8 ± 16.0 | 0.434 | 35.4 ± 14.3 | 40.0 ± 14.7 | 0.161 | 36.5 ± 18.2 | 39.3 ± 14.3 | 0.635 |
| Flexibility (cm) | 24.3 ± 10.4 | 24.5 ± 10.1 | 0.908 | 16.1 ± 7.4 | 17.5 ± 8.3 | 0.608 | 19.3 ± 7.8 | 25.0 ± 7.5 | 0.027 * |
| Balance | 6.2 ± 5.1 | 3.3 ± 3.1 | 0.053 | 2.3 ± 3.3 | 1.5 ± 2.5 | 0.461 † | 5.6 ± 5.7 | 4.7 ± 5.5 | 0.570 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soria-Rodríguez, R.; Méndez-Magaña, J.; Torres-Castillo, N.; Martínez-López, E.; Jauregui-Ulloa, E.; López-Taylor, J.; Loera-Rodríguez, C.O.d.; Sigala-Arellano, R.; Amador-Lara, F. Effect of a Supervised Aerobic Exercise Training Program and Ginkgo Biloba Extract on Metabolic Parameters and Functional Capacity in HIV-Infected Subjects. Healthcare 2025, 13, 663. https://doi.org/10.3390/healthcare13060663
Soria-Rodríguez R, Méndez-Magaña J, Torres-Castillo N, Martínez-López E, Jauregui-Ulloa E, López-Taylor J, Loera-Rodríguez COd, Sigala-Arellano R, Amador-Lara F. Effect of a Supervised Aerobic Exercise Training Program and Ginkgo Biloba Extract on Metabolic Parameters and Functional Capacity in HIV-Infected Subjects. Healthcare. 2025; 13(6):663. https://doi.org/10.3390/healthcare13060663
Chicago/Turabian StyleSoria-Rodríguez, Raúl, Javier Méndez-Magaña, Nathaly Torres-Castillo, Erika Martínez-López, Edtna Jauregui-Ulloa, Juan López-Taylor, Cesar O. de Loera-Rodríguez, Ramón Sigala-Arellano, and Fernando Amador-Lara. 2025. "Effect of a Supervised Aerobic Exercise Training Program and Ginkgo Biloba Extract on Metabolic Parameters and Functional Capacity in HIV-Infected Subjects" Healthcare 13, no. 6: 663. https://doi.org/10.3390/healthcare13060663
APA StyleSoria-Rodríguez, R., Méndez-Magaña, J., Torres-Castillo, N., Martínez-López, E., Jauregui-Ulloa, E., López-Taylor, J., Loera-Rodríguez, C. O. d., Sigala-Arellano, R., & Amador-Lara, F. (2025). Effect of a Supervised Aerobic Exercise Training Program and Ginkgo Biloba Extract on Metabolic Parameters and Functional Capacity in HIV-Infected Subjects. Healthcare, 13(6), 663. https://doi.org/10.3390/healthcare13060663