
Understanding Cancer Screening Behavior in South Korea: A Biopsychosocial Approach to Regional Differences


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Research Framework and Variable Selection
2.3. Participants
2.4. Data Collection and Research Ethics
2.5. Tools
2.5.1. Biological Factors
2.5.2. Psychological Factors
2.5.3. Sociocultural Factors
2.6. Statistical Analysis
3. Results
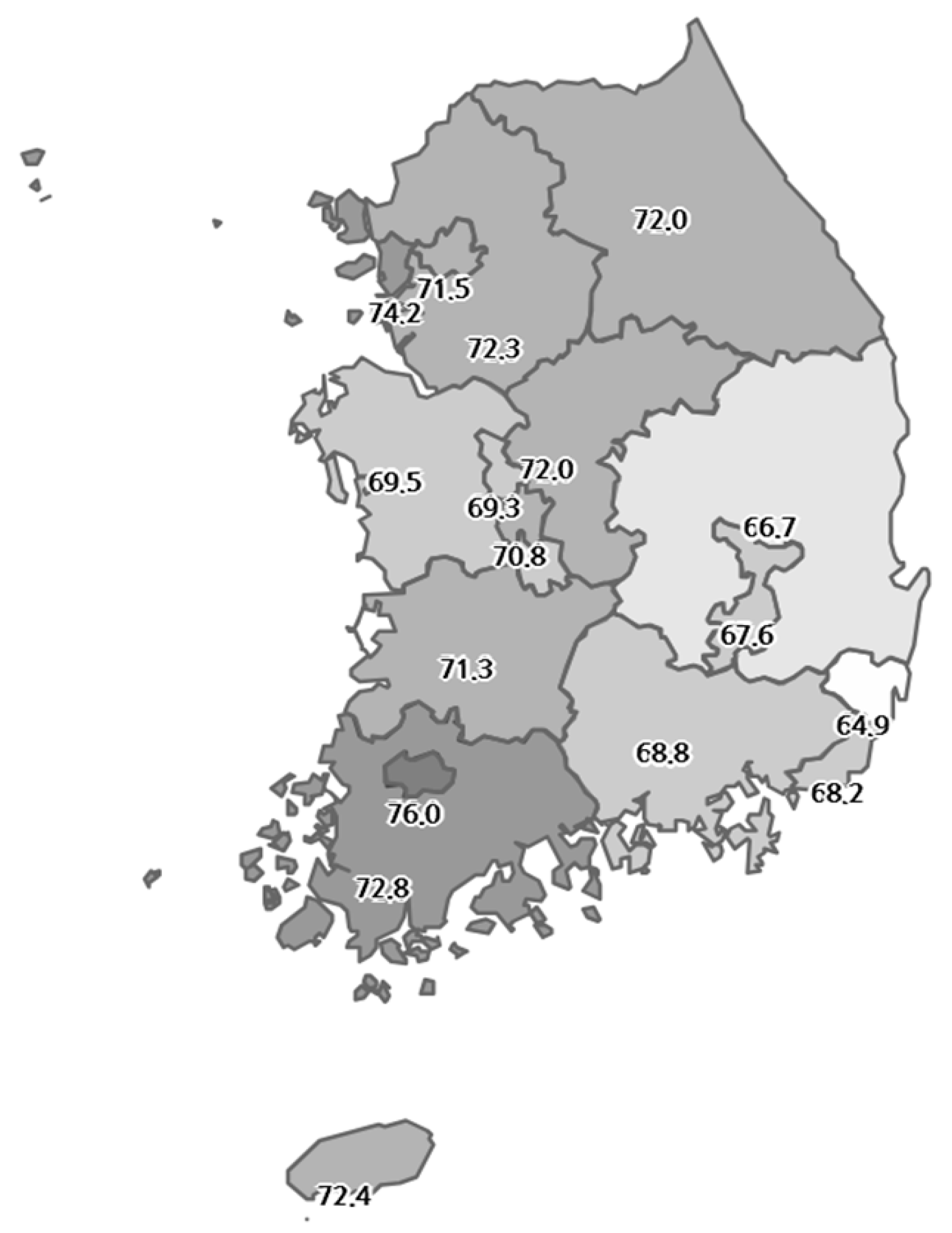
3.1. Cancer Screening Rates by Region
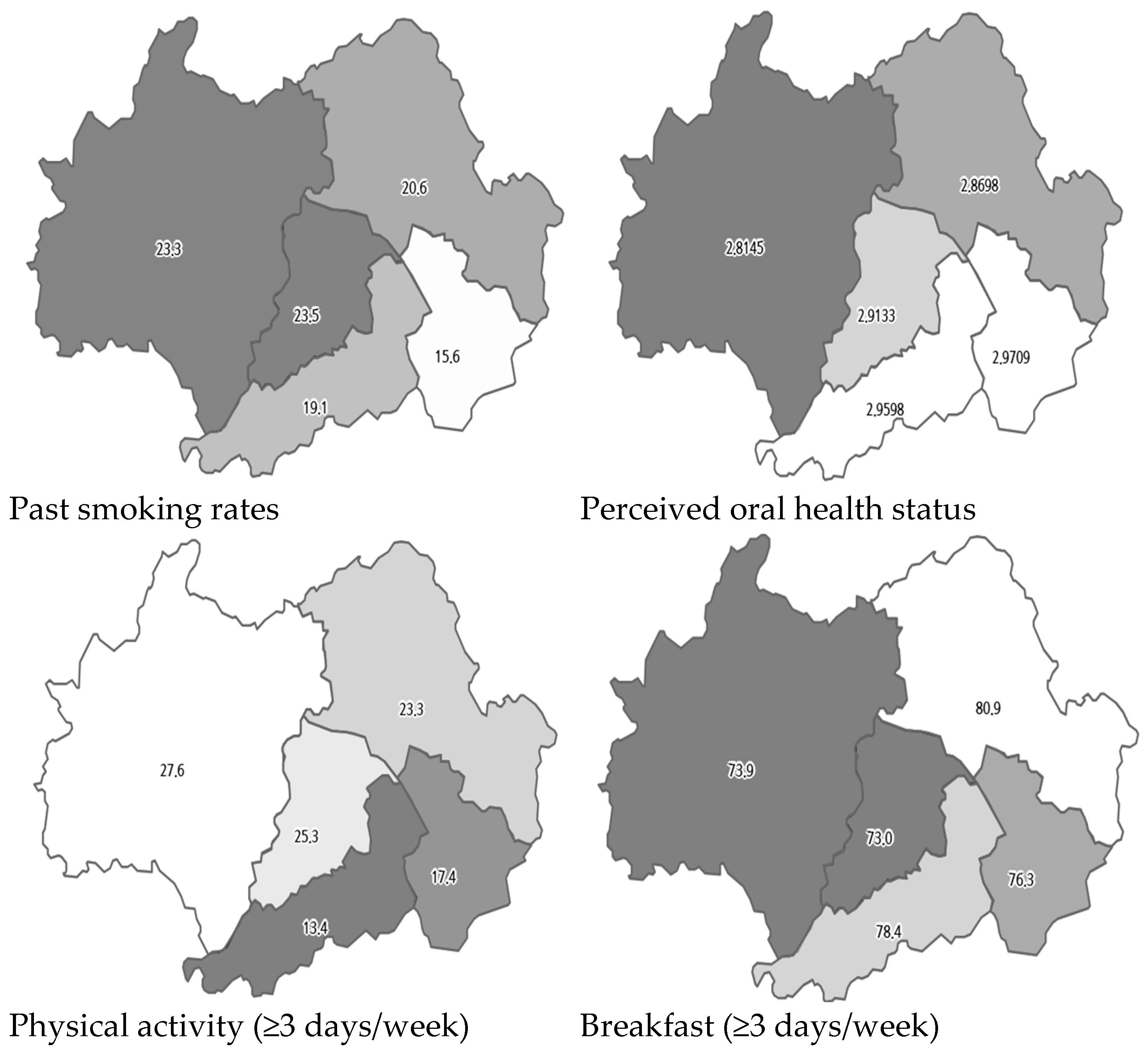
3.2. Biological, Psychological, and Sociocultural Factors in Cities with the Highest and Lowest Cancer Screening Rates
3.3. Factors Associated with Cancer Screening Behavior in Cities with the Highest and Lowest Cancer Screening Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Weiderpass, E.; Soerjomataram, I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer 2021, 127, 3029–3030. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Statistical Results of Causes of Death in 2023. 2024. Available online: https://sri.kostat.go.kr/board.es?mid=a20108100000&bid=11773&act=view&list_no=433679 (accessed on 5 November 2024).
- Schiffman, J.D.; Fisher, P.G.; Gibbs, P. Early detection of cancer: Past, present, and future. Am. Soc. Clin. Oncol. Educ. Book. 2015, 35, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention, Korea Health Information Portal. Introduction to General Health Checkup Program. 2024. Available online: https://health.kdca.go.kr/healthinfo/biz/health/gnrlzHealthInfo/gnrlzHealthInfo/gnrlzHealthInfoView.do (accessed on 3 November 2024).
- Korea National Cancer Center, Introduction to Cancer Screening Program. 2024. Available online: https://www.ncc.re.kr/main.ncc?uri=manage01_4 (accessed on 3 November 2024).
- Korea National Health Insurance Service. Annual Trends in General Health Checkups and Cancer Screening Rates. 2024. Available online: https://www.nhis.or.kr/announce/wbhaec11407m01.do (accessed on 30 September 2024).
- Korean Statistical Information Service. Status of Cancer Screening Target Population and Screening Rate by Region: 2010–2021. 2024. Available online: https://kosis.kr/statHtml/statHtml.do?orgId=350&tblId=DT_35007_N009&vw_cd=MT_ZTITLE&list_id=350_35007_A002&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=MT_ZTITLE (accessed on 2 October 2024).
- Doescher, M.P.; Jackson, J.E. Trends in cervical and breast cancer screening practices among women in rural and urban areas of the United States. J. Public. Health Manag. Pract. 2009, 15, 200–209. [Google Scholar] [CrossRef]
- Cole, A.M.; Jackson, J.E.; Doescher, M. Urban-rural disparities in colorectal cancer screening: Cross-sectional analysis of 1998–2005 data from the Centers for Disease Control’s Behavioral Risk Factor Surveillance Study. Cancer Med. 2012, 1, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Patra, S.; Upadhyay, M.; Chhabra, P. Awareness of cervical cancer and willingness to participate in screening program: Public health policy implications. J. Cancer Res. Ther. 2017, 13, 318. [Google Scholar] [CrossRef]
- Vikraman, S.M.; Khanna, D.; Dandpat, A. Cervical cancer elimination in Indian context: Moving from barriers to facilitators. Cancer 2022, 128, 4041–4046. [Google Scholar] [CrossRef]
- Goodwin, B.C.; Rowe, A.K.; Crawford-Williams, F.; Baade, P.; Chambers, S.K.; Ralph, N.; Aitken, J.F. Geographical disparities in screening and cancer-related health behaviour. Int. J. Environ. Res. Public Health 2020, 17, 1246. [Google Scholar] [CrossRef]
- Leung, J.; Macleod, C.; McLaughlin, D.; Woods, L.M.; Henderson, R.; Watson, A.; Kyle, R.G.; Hubbard, G.; Mullen, R.; Atherton, I. Screening mammography uptake within Australia and Scotland in rural and urban populations. Prev. Med. Rep. 2015, 24, 559–562. [Google Scholar] [CrossRef]
- Choi, B.; Um, T.R.; Lee, K.S. Factors related to cancer screening behaviors. Epidemiol. Health 2018, 29, e2018011. [Google Scholar] [CrossRef]
- Chen, H.; Li, N.; Ren, J.; Feng, X.; Lyu, Z.; Wei, L.; Li, X.; Guo, L.; Zheng, Z.; Zou, S.; et al. Participation and yield of a population-based colorectal cancer screening programme in China. Gut 2019, 68, 1450–1457. [Google Scholar] [CrossRef]
- Amboree, T.L.; Montealegre, J.R.; Parker, S.L.; Garg, A.; Damgacioglu, H.; Schmeler, K.M.; Chiao, E.Y.; Hill, E.G.; Sonawane, K.; Deshmukh, A.A.; et al. National Breast, Cervical, and Colorectal Cancer Screening Use in Federally Qualified Health Centers. JAMA Intern. Med. 2024, 184, 671–679. [Google Scholar] [CrossRef]
- Álvarez, A.S.; Pagani, M.; Meucci, P. The clinical application of the biopsychosocial model in mental health: A research critique. Am. J. Phys. Med. Rehabil. 2012, 91, S173–S180. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, S.N. The rise and fall of the biopsychosocial model. Br. J. Psychiatry 2009, 195, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Hinostroza, F.; Mahr, M.M. The Implementation of the Biopsychosocial Model: Individuals with Alcohol Use Disorder and Post-Traumatic Stress Disorder. Brain Behav. 2025, 15, e70230. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. Community Health Survey Project Overview. 2019. Available online: https://chs.kdca.go.kr/chs/bsnsIntrcn/bsnsSumryMain.do (accessed on 10 August 2024).
- Engel, G.L. The clinical application of the biopsychosocial model. Am. J. Psychiatry 1980, 137, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Shin, Y.J. A Multi-level analysis of factors affecting participation in health screenings in Korea: A focus on household and regional factors. J. Prev. Med. Public Health 2022, 55, 153–163. [Google Scholar] [CrossRef]
- Noguchi, R.; Shen, J. Factors affecting participation in health checkups: Evidence from Japanese survey data. Health Policy 2019, 123, 360–366. [Google Scholar] [CrossRef]
- Welch, C.; Miller, C.W.; James, N.T. Sociodemographic and health-related determinants of breast and cervical cancer screening behavior, 2005. J. Obstet. Gynecol. Neonatal Nurs. 2008, 37, 51–57. [Google Scholar] [CrossRef]
- Jerant, A.F.; Franks, P.; Jackson, J.E.; Doescher, M.P. Age-related disparities in cancer screening: Analysis of 2001 Behavioral Risk Factor Surveillance System data. Ann. Fam. Med. 2004, 2, 481–487. [Google Scholar] [CrossRef]
- Meissner, H.I.; Yabroff, K.R.; Dodd, K.W.; Leader, A.E.; Ballard-Barbash, R.; Berrigan, D. Are patterns of health behavior associated with cancer screening? Am. J. Health Promot. 2009, 23, 168–175. [Google Scholar] [CrossRef]
- Winkleby, M.A.; Snider, J.; Davis, B.; Jennings, M.G.; Ahn, D.K. Cancer-related health behaviors and screening practices among Latinos: Findings from a community and agricultural labor camp survey. Ethn. Dis. 2003, 13, 376–386. [Google Scholar] [PubMed]
- Gong, Y.; Flander, L.B.; Macrae, F.; Wilson, C.; Jenkins, M.A. The association between screening for colorectal cancer and mental and physical health. Cancer Control 2024, 31, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mahabaleshwarkar, R.; Khanna, R.; West-Strum, D.; Yang, Y. Association between health-related quality of life and colorectal cancer screening. Popul. Health Manag. 2013, 16, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.K.; Shin, D.W.; Hwang, S.S.; Oh, J.; Cho, B.L. Regional factors associated with participation in the national health screening program: A multilevel analysis using national data. J. Korean Med. Sci. 2013, 28, 348–356. [Google Scholar] [CrossRef]
- Statistics Korea. Household Income and Expenditure Trends in the Second Quarter of 2024. 2024. Available online: https://kostat.go.kr/board.es?mid=a20106020000&bid=11736&act=view&list_no=433123 (accessed on 2 October 2024).
- Statistical Geographic Information Service. Thematic Maps. 2024. Available online: https://sgis.kostat.go.kr/jsp/english/application.jsp?application8 (accessed on 30 October 2024).
- Korea Centers for Disease Control and Prevention (KCDC). 2023 Korean Community Health Survey (KCHS) Raw Data Usage Guideline. 2024. Available online: https://chs.kdca.go.kr/chs/mnl/mnlBoardMain.do (accessed on 26 February 2024).
- Tucker, C.M.; Wippold, G.M.; Guastello, A.D.; Arthur, T.M.; Desmond, F.F.; Rivers, B.M.; Davis, J.L.; Rivers, D.; Green, B.L. Predictors of Cancer Screening Among Culturally Diverse Men. Am. J. Mens. Health 2018, 12, 837–843. [Google Scholar] [CrossRef]
- Kriaucioniene, V.; Petkeviciene, J. Predictors and Trend in Attendance for Breast Cancer Screening in Lithuania, 2006–2014. Int. J. Environ. Res. Public Health 2019, 16, 4535. [Google Scholar] [CrossRef]
- Lam, A.C.L.; Aggarwal, R.; Cheung, S.; Stewart, E.L.; Darling, G.; Lam, S.; Xu, W.; Liu, G.; Kavanagh, J. Predictors of participant nonadherence in lung cancer screening programs: A systematic review and meta-analysis. Lung Cancer 2020, 146, 134–144. [Google Scholar] [CrossRef]
- Jang, T.W.; Kim, H.R.; Choi, S.E.; Yim, H.W.; Lee, H.E.; Myong, J.P.; Koo, J.W. Smoking rate trends in Korean occupational groups: Analysis of KNHANES 1998–2009 data. J. Occup. Health 2012, 54, 452–458. [Google Scholar] [CrossRef]
- Liang, W.; Shediac-Rizkallah, M.C.; Celentano, D.D.; Rohde, C. A population-based study of age and gender differences in patterns of health-related behaviors. Am. J. Prev. Med. 1999, 17, 8–17. [Google Scholar] [CrossRef]
- Deding, U.; Henig, A.S.; Salling, A.; Torp-Pedersen, C.; Bøggild, H. Sociodemographic predictors of participation in colorectal cancer screening. Int. J. Color. Dis. 2017, 32, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- van de Schootbrugge-Vandermeer, H.J.; Lansdorp-Vogelaar, I.; de Jonge, L.; van Vuuren, A.J.; Dekker, E.; Spaander, M.C.W.; Ramakers, C.R.B.; Nagtegaal, I.D.; van Kemenade, F.J.; van Leerdam, M.E.; et al. Socio-demographic and cultural factors related to non-participation in the Dutch colorectal cancer screening programme. Eur. J. Cancer 2023, 190, 112942. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| City | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All ages (%) | 56.3 | 56.8 | 54.5 | 60.2 | 60.9 | 56.3 | 51.7 | 53.6 | 58.4 | 60.9 | 59.8 | 58.1 | 59.9 | 62.5 | 56.9 | 57.5 | 59.6 |
| Age ≥ 40 (%) | 71.5 | 68.2 | 67.6 | 74.2 | 76.0 | 70.8 | 64.9 | 69.3 | 72.3 | 72.0 | 72.0 | 69.5 | 71.3 | 72.8 | 66.7 | 68.8 | 72.4 |
| Variable | Total (n = 6752) | City G (n = 3272) | City U (n = 3480) | t or Rao–Scott χ2 (p) |
|---|---|---|---|---|
| M ± SE/Unweighted Frequency (Weighted Frequency, %) | ||||
| Cancer screening (yes) | 4693 (71.0) | 2452 (76.0) | 2241 (64.9) | 57.448 (<0.001) |
| Biological factors: general characteristics and health status | ||||
| Gender (male) | 3081 (48.5) | 1486 (47.6) | 1595 (49.6) | 5.262 (0.022) |
| Age (year) | 57.96 ± 0.19 | 58.25 ± 0.26 | 57.59 ± 0.26 | 1.804 (0.072) |
| BMI | 23.64 ± 0.04 | 23.51 ± 3.05 | 23.74 ± 3.05 | −2.613 (0.009) |
| Perceived health status | 3.20 ± 0.01 | 3.18 ± 0.88 | 3.17 ± 0.83 | −0.069 (0.945) |
| Perceived oral health status | 2.88 ± 0.01 | 2.89 ± 0.86 | 2.84 ± 0.86 | 0.923 (0.356) |
| Biological factors: health behaviors | ||||
| Smoking (non-smoking) | 4059 (57.4) | 2101 (61.0) | 1961 (53.0) | 23.247 (<0.001) |
| Smoking (past smoking) | 1473 (22.7) | 697 (21.3) | 896 (24.4) | |
| Smoking (current smoking) | 1220 (19.9) | 474 (17.7) | 623 (22.6) | |
| Drinking (non-drinking) | 2473 (33.1) | 1295 (35.4) | 1178 (30.2) | 9.993 (<0.001) |
| Drinking (less than once a week) | 3057 (47.3) | 1438 (46.6) | 1619 (53.2) | |
| Drinking (more than twice a week) | 1222 (19.6) | 539 (18.0) | 683 (21.5) | |
| Wearing seat belt (yes) | 2464 (39.0) | 1229 (39.9) | 1235 (37.8) | 2.153 (0.143) |
| Physical activity (≥3 days/week) | 1547 (23.9) | 687 (22.8) | 860 (25.2) | 3.673 (0.056) |
| Breakfast (≥3 days/week) | 5243 (76.3) | 2536 (76.7) | 2707 (75.8) | 0.522 (0.470) |
| Reading and using processed food nutrition labels (yes) | 1568 (24.2) | 678 (22.2) | 890 (26.5) | 13.313 (<0.001) |
| Unmet medical care (yes) | 356 (6.0) | 166 (6.1) | 190 (5.9) | 0.079 (0.778) |
| Psychological factors | ||||
| Perceived stress status | 2.06 ± 0.01 | 2.02 ± 0.73 | 2.02 ± 0.75 | 1.707 (0.088) |
| Depressive experience (yes) | 558 (8.4) | 255 (8.4) | 303 (8.5) | 0.049 (0.826) |
| Addiction experience (yes) | 440 (7.0) | 179 (6.2) | 261 (8.1) | 5.751 (0.017) |
| Sociocultural factors: family-related | ||||
| Family structure (single person) | 1103 (15.4) | 585 (17.1) | 494 (12.8) | 16.133 (<0.001) |
| Family structure (≥two people) | 5649 (84.6) | 2687 (82.9) | 2986 (87.0) | |
| Family income (<5 million KRW) | 3933 (61.8) | 1888 (58.7) | 2045 (66.3) | 12.667 (<0.001) |
| Family income (≥5 million KRW) | 2046 (38.2) | 1190 (41.3) | 856 (33.7) | |
| Sociocultural factors: community-related | ||||
| Physical environment satisfaction | 3.99 ± 0.02 | 4.26 ± 1.14 | 3.80 ± 1.35 | 9.506 (<0.001) |
| Social environment satisfaction | 0.98 ± 0.01 | 0.96 ± 0.70 | 1.10 ± 0.79 | −7.678 (<0.001) |
| Variable | City G | City U | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Biological factors: general characteristics and health status | ||||
| Gender (male) | 0.653 | 0.49–0.86 | 0.886 | 0.62–1.22 |
| Age (year) | 0.997 | 0.98–1.01 | 1.009 | 0.99–1.02 |
| BMI | 1.003 | 0.97–1.04 | 1.016 | 0.98–1.05 |
| Perceived health status | 0.917 | 0.80–1.05 | 1.052 | 0.92–1.21 |
| Perceived oral health status | 1.314 | 1.17–1.47 | 1.074 | 0.95–1.21 |
| Biological factors: health behaviors | ||||
| Smoking (past smoking) | 1.814 | 1.28–2.57 | 1.001 | 0.72–1.40 |
| Smoking (current smoking) | 0.839 | 0.60–1.18 | 0.506 | 0.35–0.73 |
| Drinking (less than once a week) | 0.975 | 0.76–1.26 | 1.068 | 0.84–1.36 |
| Drinking (more than twice a week) | 0.901 | 0.66–1.23 | 0.997 | 0.73–1.36 |
| Wearing seat belt (yes) | 1.101 | 0.88–1.38 | 1.196 | 0.97–1.48 |
| Physical activity (≥3 days/week) | 1.297 | 1.01–1.67 | 1.089 | 0.84–1.41 |
| Breakfast (≥3 days/week) | 1.386 | 1.08–1.78 | 1.251 | 0.95–1.64 |
| Reading and using processed food nutrition labels (yes) | 0.930 | 0.70–1.24 | 1.194 | 0.92–1.55 |
| Unmet medical care (yes) | 0.799 | 0.52–1.23 | 0.865 | 0.58–1.28 |
| Psychological factors | ||||
| Perceived stress status | 0.977 | 0.84–1.14 | 1.018 | 0.87–1.19 |
| Depressive experience (yes) | 1.102 | 0.76–1.61 | 0.724 | 0.49–1.06 |
| Addiction experience (yes) | 1.256 | 0.79–1.99 | 1.099 | 0.74–1.63 |
| Sociocultural factors: family-related | ||||
| Family structure (≥two people) | 1.279 | 0.99–1.66 | 1.587 | 1.22–2.07 |
| Family income (≥5 million KRW) | 1.329 | 0.99–1.77 | 1.085 | 0.83–1.42 |
| Sociocultural factors: community-related | ||||
| Physical environment satisfaction | 1.038 | 0.94–1.14 | 0.867 | 0.80–0.94 |
| Social environment satisfaction | 0.994 | 0.85–1.16 | 1.171 | 1.02–1.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, Y.-H.; Lee, J. Understanding Cancer Screening Behavior in South Korea: A Biopsychosocial Approach to Regional Differences. Healthcare 2025, 13, 664. https://doi.org/10.3390/healthcare13060664
Cho Y-H, Lee J. Understanding Cancer Screening Behavior in South Korea: A Biopsychosocial Approach to Regional Differences. Healthcare. 2025; 13(6):664. https://doi.org/10.3390/healthcare13060664
Chicago/Turabian StyleCho, Yoon-Hee, and Joohyun Lee. 2025. "Understanding Cancer Screening Behavior in South Korea: A Biopsychosocial Approach to Regional Differences" Healthcare 13, no. 6: 664. https://doi.org/10.3390/healthcare13060664
APA StyleCho, Y.-H., & Lee, J. (2025). Understanding Cancer Screening Behavior in South Korea: A Biopsychosocial Approach to Regional Differences. Healthcare, 13(6), 664. https://doi.org/10.3390/healthcare13060664