
Predictors of Cataract Surgery Among US Adults: NHANES 2007–2008

Abstract
1. Introduction
2. Materials and Methods
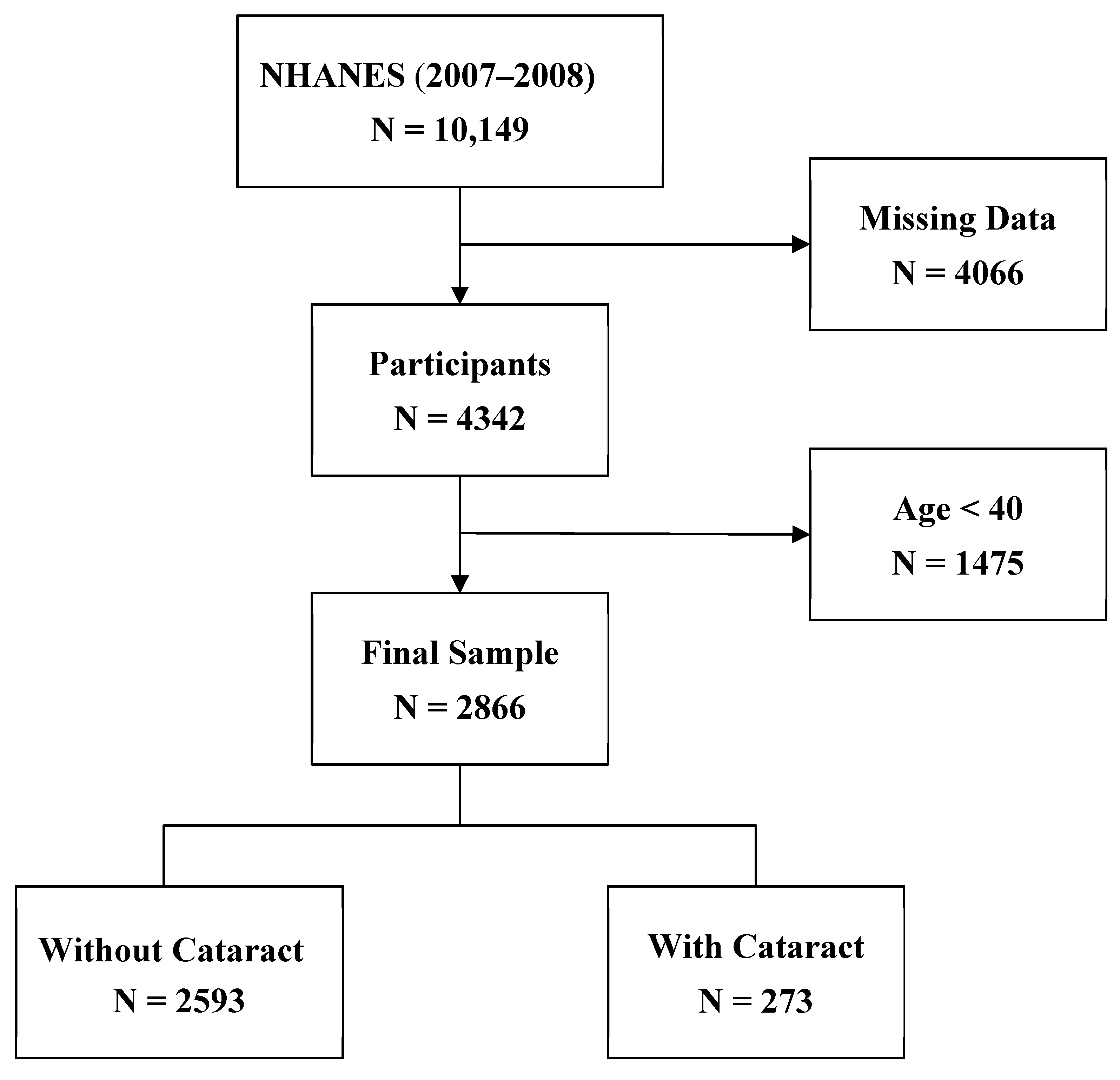
2.1. Study Design and Population
2.2. Measures
3. Results
3.1. Participant Characteristics
3.2. Predictors of Cataract Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.K. The Prevalence of Age-Related Eye Diseases and Visual Impairment in Aging: Current Estimates. Investig. Ophthalmol. Vis. Sci. 2013, 54, ORSF5–ORSF13. [Google Scholar] [CrossRef] [PubMed]
- National Eye Institute. Cataract Tables|Projections for Cataract (2010–2030–2050). 2020. Available online: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics/cataract-data-and-statistics/cataract-tables (accessed on 28 February 2025).
- Rossi, T.; Romano, M.R.; Iannetta, D.; Romano, V.; Gualdi, L.; D’Agostino, I.; Ripandelli, G. Cataract surgery practice patterns worldwide: A survey. BMJ Open Ophthalmol. 2021, 6, e000464. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.C.; Brown, M.M.; Busbee, B.G.; Rapuano, S.B. A Cost-benefit Analysis of 2018 Cataract Surgery in the United States. Clin. Res. Ophthalmol. 2019, 2, 1–13. [Google Scholar]
- Richter, G.M.; Choudhury, F.; Torres, M.; Azen, S.P.; Varma, R.; Los Angeles Latino Eye Study Group. Risk factors for incident cortical, nuclear, posterior subcapsular, and mixed lens opacities: The Los Angeles Latino eye study. Ophthalmology 2012, 119, 2040–2047. [Google Scholar] [CrossRef]
- Hennis, A.; Wu, S.Y.; Nemesure, B.; Leske, M.C.; Barbados Eye Studies Group. Risk factors for incident cortical and posterior subcapsular lens opacities in the Barbados Eye Studies. Arch. Ophthalmol. 2004, 122, 525–530. [Google Scholar] [CrossRef]
- Chang, J.R.; Koo, E.; Agrón, E.; Hallak, J.; Clemons, T.; Azar, D.; Sperduto, R.D.; Ferris, F.L.; Chew, E.Y. Risk factors associated with incident cataracts and cataract surgery in the Age-related Eye Disease Study (AREDS): AREDS report number 32. Ophthalmology 2011, 118, 2113–2119. [Google Scholar] [CrossRef]
- Storey, P.; Munoz, B.; Friedman, D.; West, S. Racial Differences in Lens Opacity Incidence and Progression: The Salisbury Eye Evaluation (SEE) Study. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3010–3018. [Google Scholar] [CrossRef]
- Elam, A.R.; Tseng, V.L.; Rodriguez, T.M.; Mike, E.V.; Warren, A.K.; Coleman, A.L. Disparities in vision health and eye care. Ophthalmology 2022, 129, e89–e113. [Google Scholar] [CrossRef]
- Fang, Z.; Chen, X.Y.; Lou, L.X.; Yao, K. Socio-economic disparity in visual impairment from cataract. Int. J. Ophthalmol. 2021, 14, 1310–1314. [Google Scholar] [CrossRef]
- Wale, M.Z.; Derbew, M.; Tilahun, M.; Terefe, M. Cataract and associated factors among adults visiting ophthalmic clinic at Debre Markos comprehensive specialized hospital, northwest Ethiopia, 2020. SAGE Open Med. 2021, 9, 2050312121989636. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Wang, Y.; Zhao, L.; Wang, Z.; Sun, M.; Chen, D.; Yang, Y.; Xu, Y.; Lv, S.; Yu, Y.; et al. The Association between Socioeconomic Factors and Visual Function among Patients with Age-Related Cataracts. J. Ophthalmol. 2020, 2020, 7236214. [Google Scholar] [CrossRef] [PubMed]
- Nita, M.; Grzybowski, A. Smoking and Eye Pathologies. A Systemic Review. Part I. Anterior Eye Segment Pathologies. Curr. Pharm. Des. 2017, 23, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; He, J.; Wang, C.; Wu, H.; Shi, X.; Zhang, H.; Xie, J.; Lee, S.Y. Smoking and risk of age-related cataract: A meta-analysis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3885–3895. [Google Scholar] [CrossRef]
- Chua, S.Y.; Luben, R.N.; Hayat, S.; Broadway, D.C.; Khaw, K.-T.; Warwick, A.; Britten, A.; Day, A.C.; Strouthidis, N.; Patel, P.J.; et al. Alcohol Consumption and Incident Cataract Surgery in Two Large UK Cohorts. Ophthalmology 2021, 128, 837–847. [Google Scholar] [CrossRef]
- Li, L.; Wan, X.-H.; Zhao, G.-H. Meta-analysis of the risk of cataract in type 2 diabetes. BMC Ophthalmol. 2014, 14, 94. [Google Scholar] [CrossRef]
- Klein, B.E.; Klein, R.; Jensen, S.C.; Linton, K.L. Hypertension and lens opacities from the Beaver Dam Eye Study. Am. J. Ophthalmol. 1995, 119, 640–646. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Lee, J.-I.; Chang, C.-W.; Liu, Y.-H.; Huang, S.-P.; Chen, S.-C.; Geng, J.-H. Chronic kidney disease and its association with cataracts–A cross-sectional and longitudinal study. Front. Public Health 2022, 10, 1029962. [Google Scholar] [CrossRef]
- Erdem, S. Diseases associated with age-related cataract: A health-board-based retrospective study focusing on common physiopathological mechanisms. J. Public Health 2021, 29, 163–167. [Google Scholar] [CrossRef]
- American Academy of Ophthalmology. Diabetes and Cataracts. 10 November 2013. Available online: https://www.aao.org/salud-ocular/consejos/diabetes-cataracts (accessed on 6 August 2024).
- Hu, W.S.; Lin, C.L.; Chang, S.S.; Chen, M.F.; Chang, K.C. Increased risk of ischemic heart disease among subjects with cataracts. Medicine 2016, 95, e4119. [Google Scholar] [CrossRef]
- Sommar, J.N.; Segersson, D.; Flanagan, E.; Oudin, A. Long-term residential exposure to source-specific particulate matter and incidence of diabetes mellitus—A cohort study in northern Sweden. Environ. Res. 2023, 217, 114833. [Google Scholar] [CrossRef] [PubMed]
- Yun, B.; Sim, J.; Lee, S.; Cho, A.; Oh, J.; Kim, S.; Yoon, J. The relationship between occupational dust exposure and incidence of diabetes in male workers: A retrospective cohort study. Diabet. Med. 2022, 39, e14837. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. NHANES—About the National Health and Nutrition Examination Survey. 17 June 2024. Available online: https://wwwn.cdc.gov/nchs/nhanes/default.aspx (accessed on 19 July 2024).
- Wang, W.; Zhang, X. Alcohol Intake and the Risk of Age-Related Cataracts: A Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2014, 9, e107820. [Google Scholar] [CrossRef] [PubMed]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]
- Cedrone, C.; Culasso, F.; Cesareo, M.; Mancino, R.; Ricci, F.; Cupo, G.; Cerulli, L. Prevalence and incidence of age-related cataract in a population sample from Priverno, Italy. Ophthalmic Epidemiol. 1999, 6, 95–103. [Google Scholar] [CrossRef]
- Klein, B.E.K.; Klein, R.; Lee, K.E. Incidence of Age-Related Cataract: The Beaver Dam Eye Study. Arch. Ophthalmol. 1998, 116, 219–225. [Google Scholar] [CrossRef]
- Schuster, A.K.; Nickels, S.; Pfeiffer, N.; Schmidtmann, I.; Wild, P.S.; Münzel, T.; Beutel, M.E.; Lackner, K.J.; Vossmerbaeumer, U. Frequency of cataract surgery and its impact on visual function—Results from the German Gutenberg Health Study. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2223–2231. [Google Scholar] [CrossRef]
- Michael, R.; Bron, A.J. The ageing lens and cataract: A model of normal and pathological ageing. Philos. Trans. R. Soc. B Biol. Sci. 2011, 366, 1278. [Google Scholar] [CrossRef]
- Glynn, R.J.; Rosner, B.; Christen, W.G. Evaluation of Risk Factors for Cataract Types in a Competing Risks Framework. Ophthalmic Epidemiol. 2009, 16, 98. [Google Scholar] [CrossRef]
- Yu, X.; Lyu, D.; Dong, X.; He, J.; Yao, K. Hypertension and Risk of Cataract: A Meta-Analysis. PLoS ONE 2014, 9, e114012. [Google Scholar] [CrossRef]
- Foster, P.J.; Wong, T.Y.; Machin, D.; Johnson, G.J.; Seah, S.K.L. Risk factors for nuclear, cortical and posterior subcapsular cataracts in the Chinese population of Singapore: The Tanjong Pagar Survey. Br. J. Ophthalmol. 2003, 87, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Klein, B.E.; Klein, R.; Moss, S.E. Incidence of cataract surgery in the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Am. J. Ophthalmol. 1995, 119, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Klein, B.E.; Klein, R.; Wang, Q.; Moss, S.E. Older-onset diabetes and lens opacities. The Beaver Dam Eye Study. Ophthalmic Epidemiol. 1995, 2, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Rowe, N.G.; Mitchell, P.G.; Cumming, R.G.; Wans, J.J. Diabetes, fasting blood glucose and age-related cataract: The Blue Mountains Eye Study. Ophthalmic Epidemiol. 2000, 7, 103–114. [Google Scholar] [CrossRef]
- Onakpoya, O.H.; Bekibele, C.O.; Adegbehingbe, S.A. Cataract Surgical Outcomes In Diabetic Patients: Case Control Study. Middle East Afr. J. Ophthalmol. 2009, 16, 88–91. [Google Scholar] [CrossRef]
- Leske, M.C.; Wu, S.Y.; Hennis, A.; Connell, A.M.; Hyman, L.; Schachat, A. Diabetes, hypertension, and central obesity as cataract risk factors in a black population. The Barbados Eye Study. Ophthalmology 1999, 106, 35–41. [Google Scholar] [CrossRef]
- Hiller, R.; Sperduto, R.D.; Ederer, F. Epidemiologic associations with nuclear, cortical, and posterior subcapsular cataracts. Am. J. Epidemiol. 1986, 124, 916–925. [Google Scholar] [CrossRef]
- Klein, B.E.; Klein, R.; Lee, K.E. Diabetes, cardiovascular disease, selected cardiovascular disease risk factors, and the 5-year incidence of age-related cataract and progression of lens opacities: The Beaver Dam Eye Study. Am. J. Ophthalmol. 1998, 126, 782–790. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Total | Cataract Surgery | Cataract Surgery |
|---|---|---|---|
| No | Yes | ||
| N = 2866 | (N = 2593) | (N = 273) | |
| Total N (%) | N (%) | N (%) | |
| Age [Mean, SD] | 58 [10.9] | 56 [10.6] | 70 [7.1] |
| Gender | |||
| Men | 1462 (51.1) | 1333 (50.4) | 129 (39.1) |
| Women | 1404 (48.9) | 1260 (49.6) | 144 (60.9) |
| Race/ethnicity | |||
| Mexican American | 438 (5.8) | 414 (6.0) | 24 (3.3) |
| Non-Hispanic White | 1434 (75.0) | 1269 (74.6) | 165 (81.0) |
| Non-Hispanic Black | 601 (10.2) | 551 (10.4) | 50 (7.9) |
| Other | 393 (9.0) | 359 (9.0) | 34 (7.8) |
| Education | |||
| Less than high school | 853 (18.7) | 750 (18.1) | 103 (26.3) |
| High school degree | 700 (25.8) | 639 (25.9) | 61 (24.7) |
| >High school degree | 1313 (55.5) | 1204 (56.0) | 109 (49.0) |
| Marital status | |||
| Married | 1853 (70.5) | 1700 (71.3) | 153 (60.0) |
| Divorced/Separated/Widowed | 803 (23.1) | 694 (22.2) | 109 (35.4) |
| Never Married | 210 (6.4) | 199 (6.5) | 11 (4.6) |
| Family Income | |||
| <USD 35,000 | 1369 (34.0) | 1204 (32.7) | 165 (51.3) |
| ≥USD 35,000–USD 74,999 | 820 (30.3) | 746 (30.3) | 74 (30.4) |
| USD 75,000 and over | 677 (35.7) | 643 (37.0) | 34 (18.3) |
| Employment at the time of data collection | |||
| Not working | 1367 (37.2) | 1149 (34.5) | 218 (73.9) |
| Working | 1499 (62.8) | 1444 (65.5) | 55 (26.1) |
| Covered by health insurance | |||
| No | 506 (12.6) | 491 (13.4) | 15 (2.9) |
| Yes | 2360 (87.4) | 2102 (86.6) | 258 (97.1) |
| Behavioral Predictors | |||
| Alcohol Consumption [had at least 12 drinks/year] | |||
| No | 863 (27.1) | 764 (26.5) | 99 (34.6) |
| Yes | 2003 (72.9) | 1829 (73.5) | 174 (65.4) |
| Smoking | |||
| Never | 1353 (49.7) | 1234 (49.7) | 119 (41.0) |
| Ever | 1513 (50.3) | 1359 (50.3) | 154 (59.0) |
| Medical Conditions | |||
| High blood pressure ever | |||
| No | 1553 (59.5) | 1460 (61.2) | 93 (37.0) |
| Yes | 1313 (40.5) | 1133 (38.8) | 180 (63.0) |
| Diabetes ever | |||
| No | 2335 (86.3) | 2147 (87.1) | 188 (75.0) |
| Yes | 531 (13.7) | 446 (12.9) | 85 (25.0) |
| Kidney Condition ever | |||
| No | 2776 (97.6) | 2518 (97.8) | 258 (94.5) |
| Yes | 90 (2.4) | 75 (2.2) | 15 (5.5) |
| Presence of heart disease ever | |||
| No | 2710 (95.4) | 2466 (95.8) | 244 (89.1) |
| Yes | 156 (4.6) | 127 (4.2) | 29 (10.9) |
| Occupational Exposures | |||
| Exposure to exhaust fumes | |||
| No | 2128 (73.5) | 1907 (72.9) | 221 (81.5) |
| Yes | 738 (26.5) | 686 (27.1) | 52 (18.5) |
| Mineral Dust | |||
| No | 1913 (66.2) | 1709 (65.5) | 204 (76.2) |
| Yes | 953 (33.8) | 884 (34.5) | 69 (23.8) |
| Organic Dust | |||
| No | 2246 (77.6) | 2017 (77.2) | 229 (83.8) |
| Yes | 620 (22.4) | 576 (22.8) | 44 (16.2) |
| Variable | Odds Ratio | 95% Confidence Interval |
|---|---|---|
| Age | 1.15 | 1.13–1.16 |
| High blood pressure | ||
| No | 1.00 | Referent |
| Yes | 1.38 | 1.11–1.73 |
| Diabetes | ||
| No | 1.00 | Referent |
| Yes | 1.63 | 1.27–2.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwundu, C.N.; Kohir, T.; Heck, J.E. Predictors of Cataract Surgery Among US Adults: NHANES 2007–2008. Healthcare 2025, 13, 641. https://doi.org/10.3390/healthcare13060641
Iwundu CN, Kohir T, Heck JE. Predictors of Cataract Surgery Among US Adults: NHANES 2007–2008. Healthcare. 2025; 13(6):641. https://doi.org/10.3390/healthcare13060641
Chicago/Turabian StyleIwundu, Chisom N., Teija Kohir, and Julia E. Heck. 2025. "Predictors of Cataract Surgery Among US Adults: NHANES 2007–2008" Healthcare 13, no. 6: 641. https://doi.org/10.3390/healthcare13060641
APA StyleIwundu, C. N., Kohir, T., & Heck, J. E. (2025). Predictors of Cataract Surgery Among US Adults: NHANES 2007–2008. Healthcare, 13(6), 641. https://doi.org/10.3390/healthcare13060641