
Are Virtual Forests Just for Relaxation, or Can They Enhance the Benefits of Therapy?
 , , and
, , and
Abstract
1. Introduction
1.1. Social Anxiety
1.2. Traditional Intervention to Reduce Social Anxiety
1.3. Access to SAD Treatment
1.4. Real and Virtual Nature
1.5. Research Questions and Hypotheses
- Does the use of a virtual forest setting (with or without therapeutic instruction) reduce social anxiety (and improve self-rated restoration effects) to a greater extent than therapeutic instruction provided without a virtual forest?
- Is therapeutic instruction (either by itself or in a virtual forest setting) more effective at reducing social anxiety (and improving self-rated restoration effects) than virtual forest bathing (without therapeutic instruction)?
- Does the addition of therapeutic instructions make a virtual forest less attractive (measured in terms of user experience, immersiveness, and sentiment) than it would otherwise be?
2. Materials and Methods
2.1. Participants
2.2. Materials and Apparatus
2.2.1. Psychological Measurements
2.2.2. VR Usability Measurements
2.2.3. VR Headset and Software
2.2.4. Experimental Conditions
- Condition A—VR forest only: In this VR condition, participants had to navigate through a virtual forest using controllers and joysticks without receiving any therapeutic exercises.
- Condition B—combined VR forest and therapy exercises: Similar to Condition A, participants in this VR condition still navigated through the same virtual forest, but they had to pause their virtual walk and listen to therapeutic exercise instructions that were designed to reduce social anxiety at each checkpoint.
- Condition Non-VR—therapy exercises only: In this Non-VR condition, participants received therapeutic exercise instructions displayed on a laptop, without exploring or walking in the virtual forest. The exercise instructions, identical in content and design to Condition B, were shown on a lab-developed website, accompanied by the same forest sounds used in Conditions A and B. Before the session started, participants were asked to imagine that they were in a forest.
2.2.5. Therapy Instructions
- Checkpoint 1: In accordance with a typical cognitive behavior therapy first session’s content, this checkpoint focused on psychoeducation [65]. The psychoeducation content was developed based on Andrews’ treatment manual (Pages 3–18). The psychoeducation part was followed by a quick abdominal breathing exercise (from Andrews’ manual) teaching people how to slow down the rate of respiration to cope with shallow and rapid breathing when anxiety level is high.
- Checkpoint 2: This checkpoint introduced the concept of mindfulness, highlighting the concept of focusing on the present moment and becoming aware of thoughts and feelings based on Segal et al.’s mindfulness-based cognitive therapy manual [67]. To help cultivate awareness, participants were asked to engage in the four-senses mindfulness exercise (the five-sense exercise minus taste) to bring awareness to each sense [68].
- Checkpoint 3: We used both Andrews and Segal et al.’s manuals to develop this section of cognitive restructuring [65]. Challenging thoughts and cognitive restructuring are fundamental components of CBT. Participants also received two hypothetical situations, asking the participant to become aware of the thoughts that those situations evoke, to evaluate whether those thoughts are reasonable assessments, and to reappraise the situation if the thoughts were not helpful.
- Checkpoint 4: The fourth checkpoint exercise was the mountain mediation developed by Kabat-Zinn [69].
- Checkpoint 5: Using Andrews’ manual (Pages 33–34), the material in this checkpoint discussed avoidance and its negative impact on social anxiety [65]. While avoidance might seem helpful, it often exacerbates anxiety and prevents personal growth.
- Checkpoint 6: The sixth checkpoint exercise was sound meditation, adapted from Segal et al. to engage participants with forest sound played in the VR headset [67].
- Checkpoint 7: The seventh checkpoint exercise was about self-compassion, which incorporates Hofmann et al.’s Loving-kindness Meditation [70]. It discusses the inevitability of setbacks in conquering social anxiety and emphasizes the importance of treating oneself kindly when encountering those difficult times.
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Social Anxiety Measurement
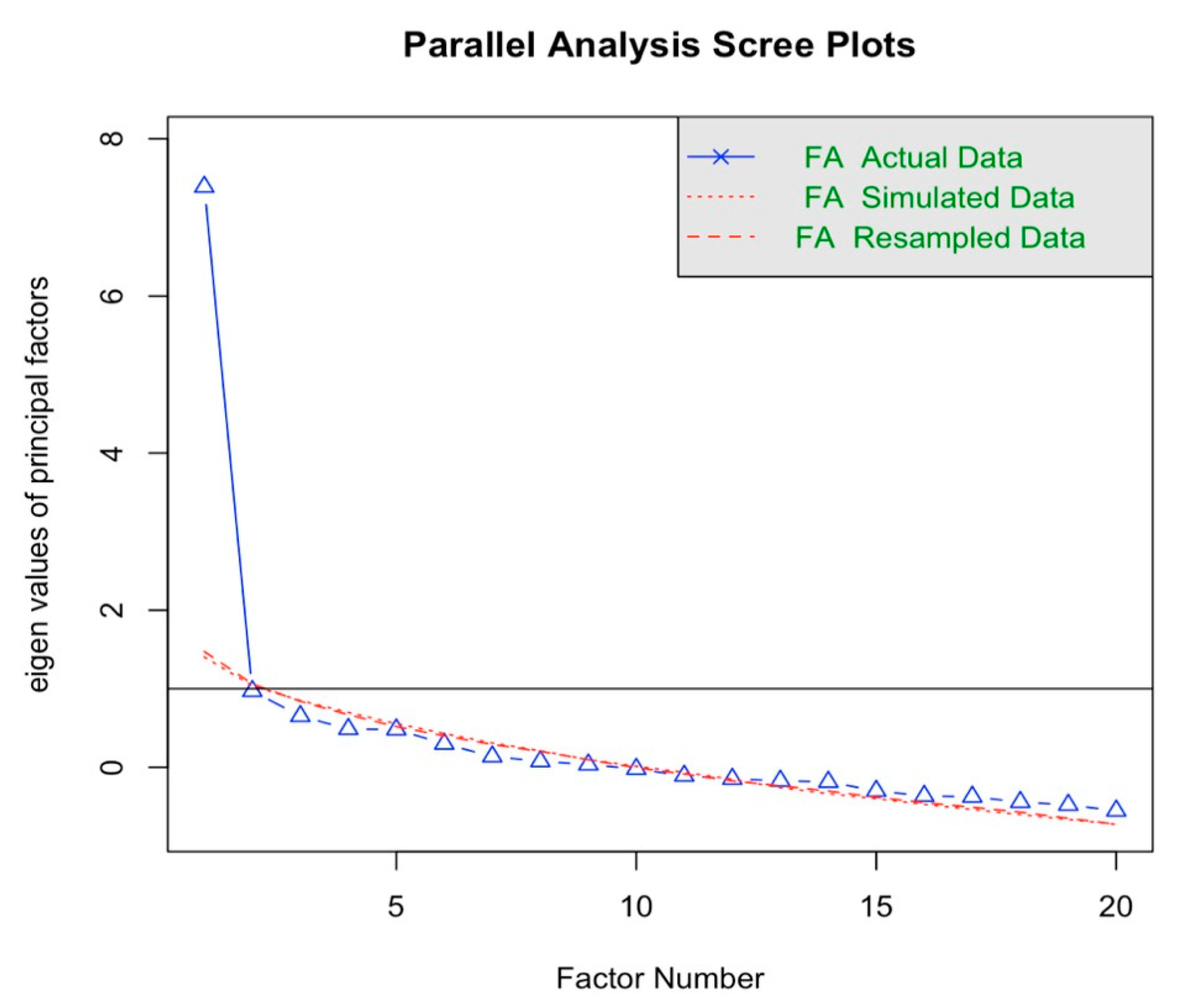
3.1.1. Factor and Reliability Analysis
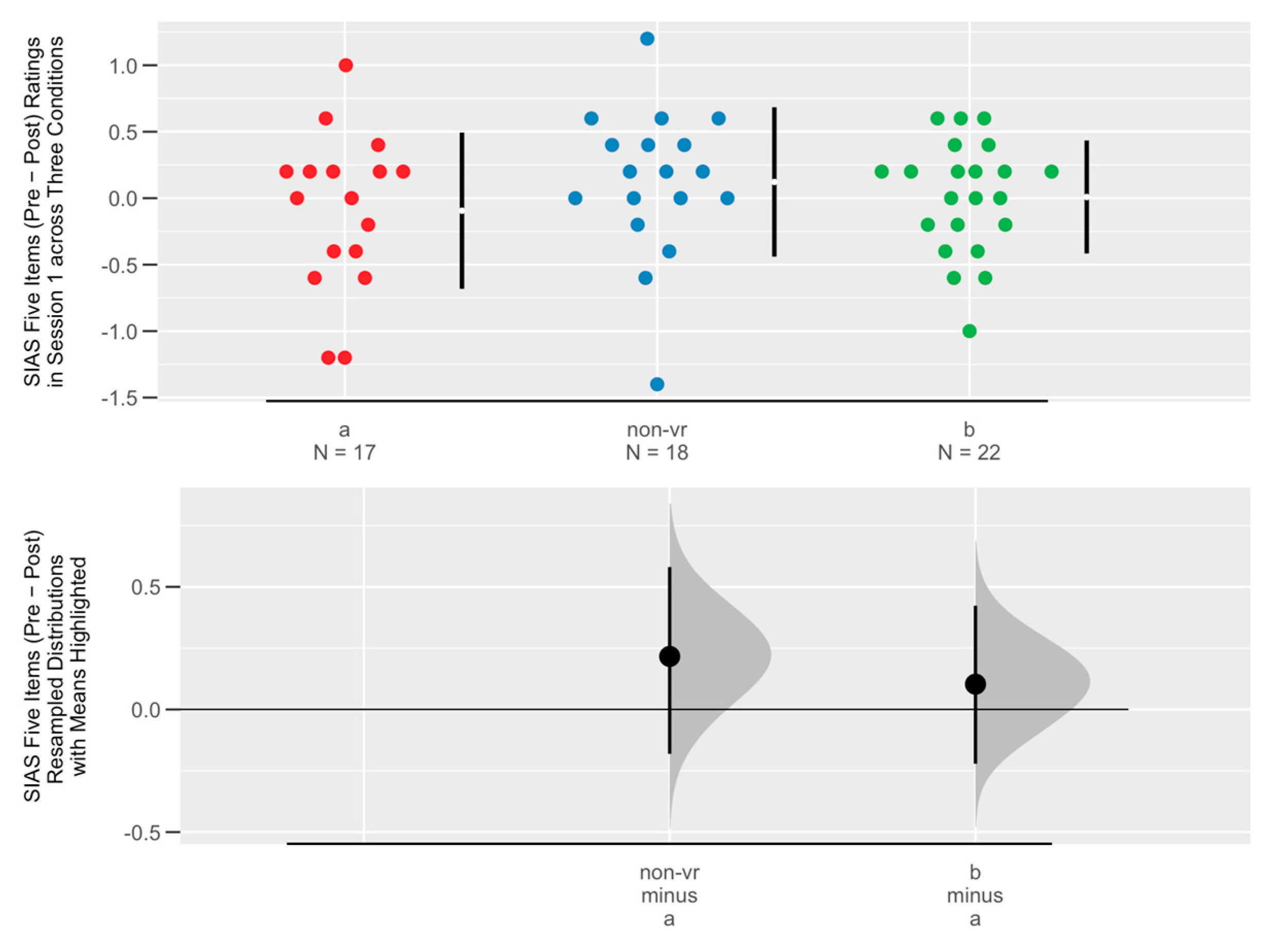
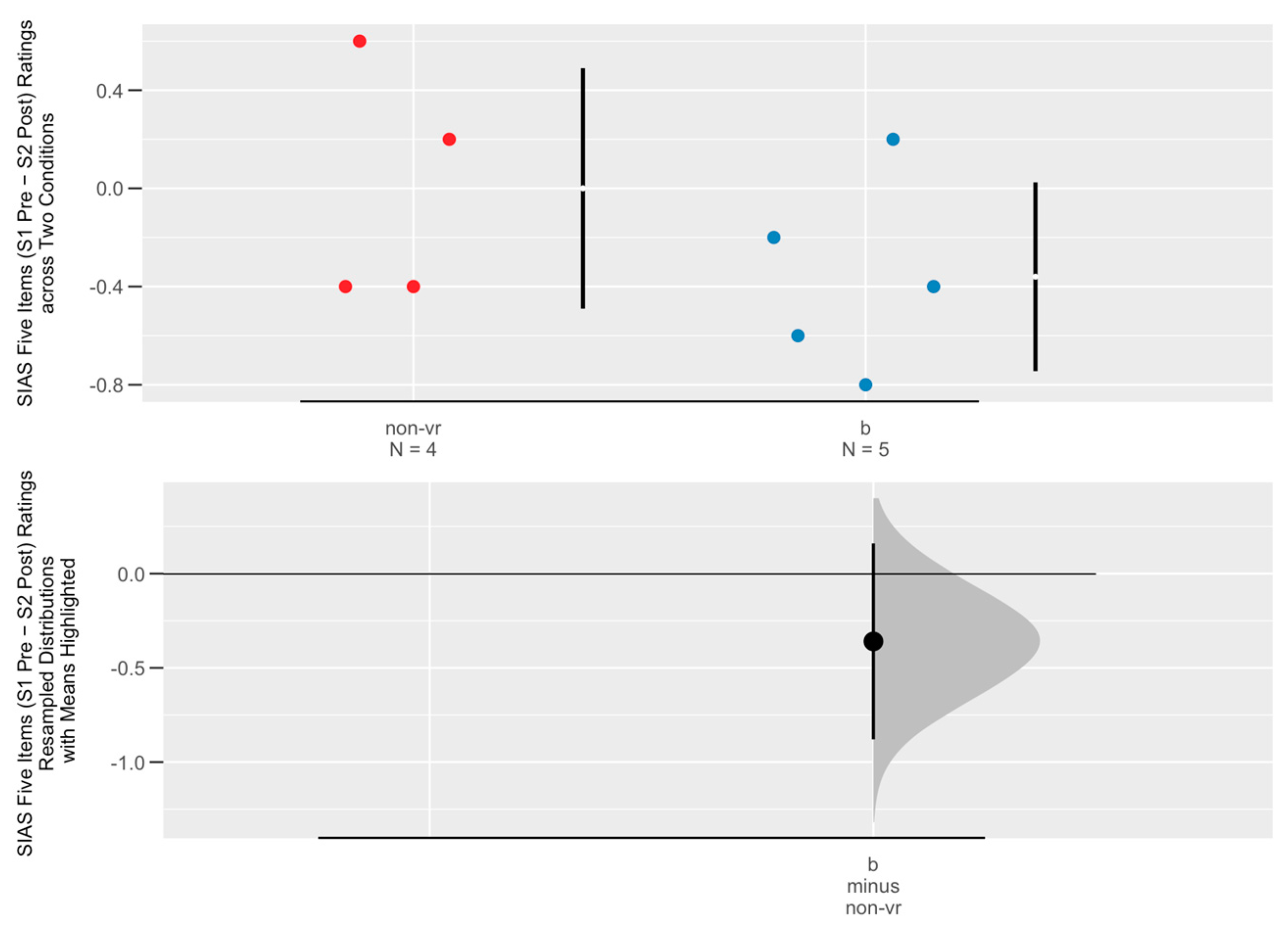
3.1.2. Social Anxiety Change Across Three Conditions
3.2. Checkpoint Quiz Performance
3.3. User Experience Questionnaire
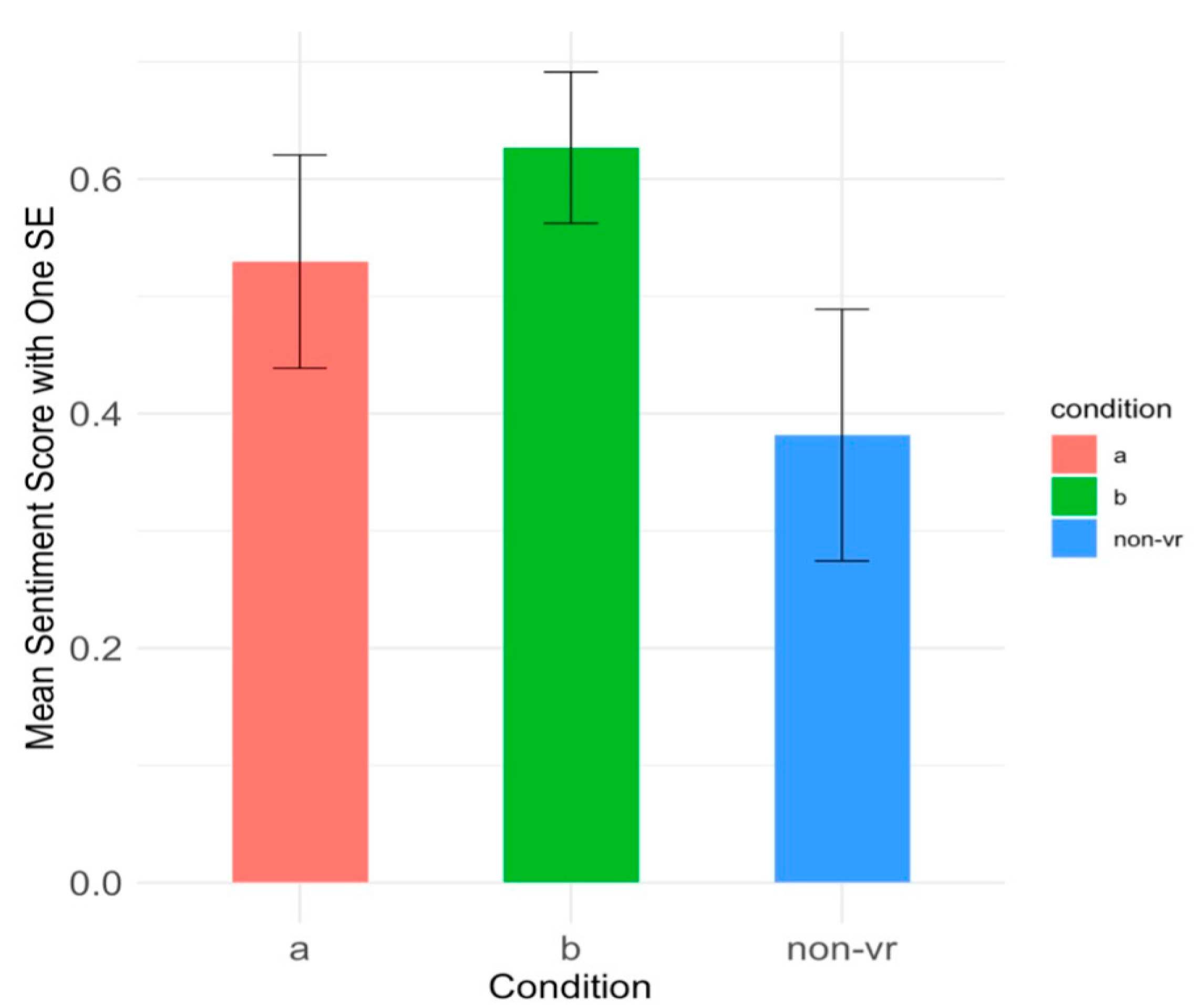
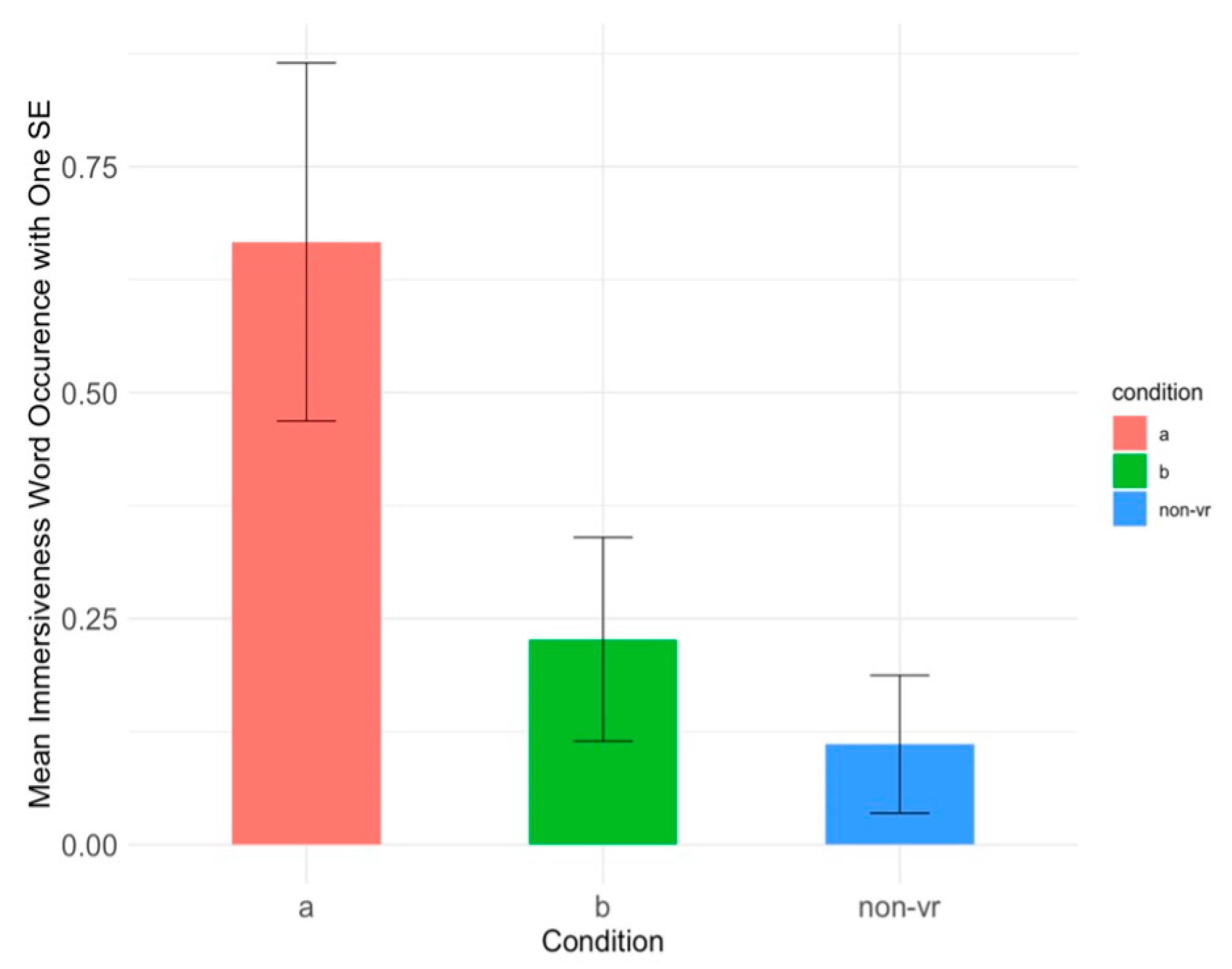
3.4. Open-Ended Comments
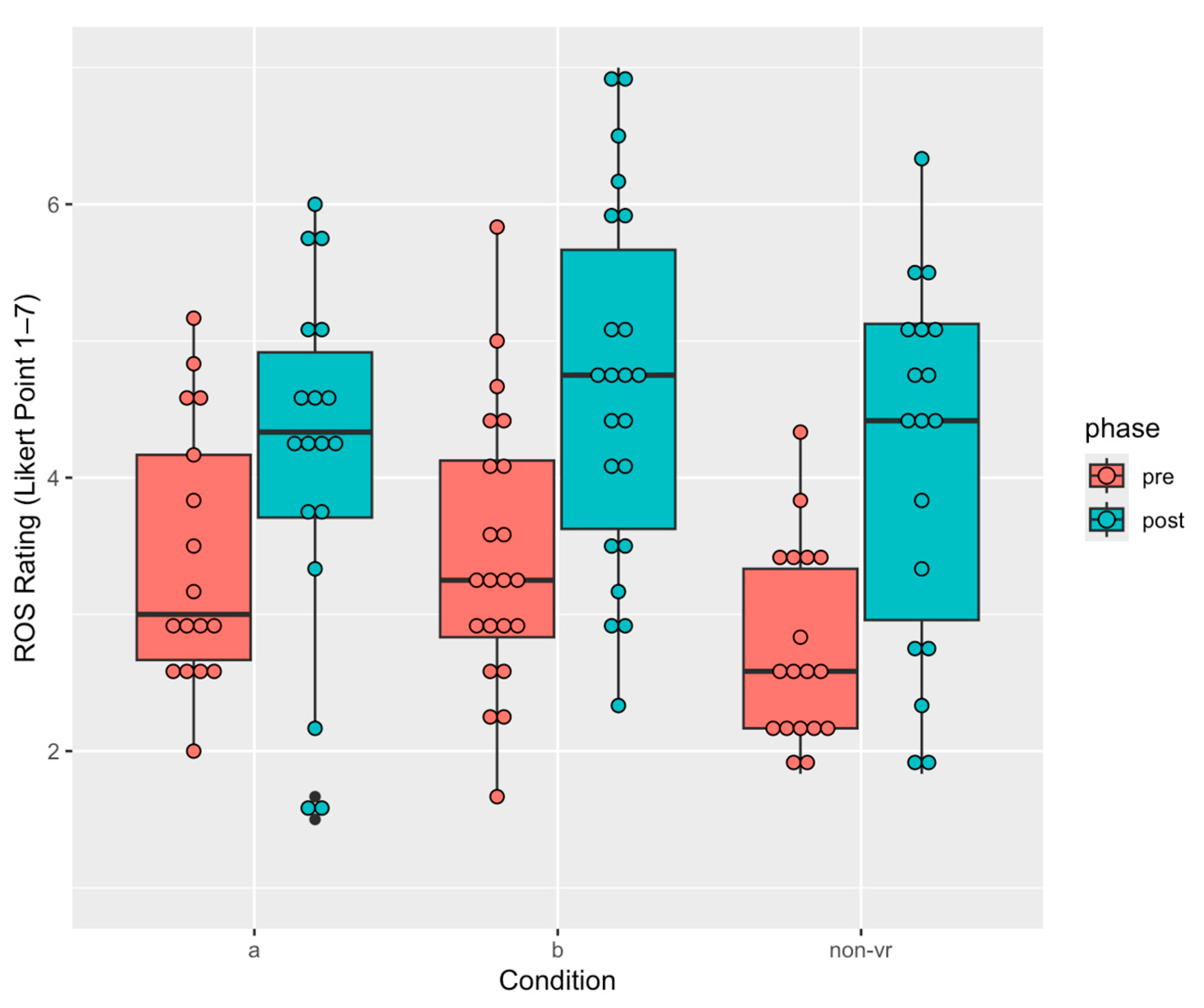
3.5. Restoration Outcome Scale
4. Discussion
4.1. Non-VR (Therapy Only) Condition Shows Potential for Reducing Social Anxiety
4.2. VR Therapy Enhances Long-Term Engagement and Learning of Therapeutic Information
4.3. Forest Sound Played a Significant Role in Enhancing Restoration
5. Limitations and Future Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Psychotherapy Script
Appendix A.1. CHECKPOINT #1: What Is Social Anxiety?
- Will you say something that is embarrassing or awkward?
- Will others notice that you are anxious?
- Will you make a mistake?
Appendix A.2. CHECKPOINT #2: What Is Mindfulness?
- Notice four things that you can see. Look around the forest and try to pick objects that you would not normally notice, like the vein of a leaf.
- Notice three things that you can feel. Bring your attention to sensations that your body is feeling, like maybe the straps of the VR headset on your head.
- Notice two things you can hear. Focus on two things that you can hear in the forest, maybe it is the bird chirping.
- Notice one thing that you can smell. Take a moment to take note of one scent that you smell. Notice that normally, your attention is not focused on the scent, but mindfulness can help us return our attention to the scent when we wish.
Appendix A.3. CHECKPOINT #3: Challenging the Way You Think (Cognitive Restructuring)
- “They aren’t actually busy; they just do not want to hang out with me”
- “I built up the courage to ask, and the result is the same, I’m still lonely”
- “No one likes me”
- “I’m awkward, boring, weird, etc.”
Appendix A.4. CHECKPOINT #4: Mountain Meditation
Appendix A.5. CHECKPOINT #5: Avoidance and Aversion
Appendix A.6. CHECKPOINT #6: Sounds Meditation
Appendix A.7. Self-Compassion
Appendix A.8. CHECKPOINT #8: Closure & Review
Appendix B. Word List for Occurrences and Theme Analysis
References
- Lin, Y.; Fan, Z. The Relationship between Rejection Sensitivity and Social Anxiety among Chinese College Students: The Mediating Roles of Loneliness and Self-Esteem. Curr. Psychol. 2022, 42, 12439–12448. [Google Scholar] [CrossRef]
- Heimberg, R.G.; Brozovich, F.A.; Rapee, R.M. Chapter 15—A Cognitive Behavioral Model of Social Anxiety Disorder: Update and Extension. In Social Anxiety Clinical, Developmental, and Social Perspectives; Elsevier Academic Press: Amsterdam, The Netherlands, 2010; pp. 395–422. [Google Scholar]
- Stein, M.B.; Stein, D.J. Social Anxiety Disorder. Lancet 2008, 371, 1115–1125. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Kean, Y.M. Disability and Quality of Life in Social Phobia: Epidemiologic Findings. Am. J. Psychiatry 2000, 157, 1606–1613. [Google Scholar] [CrossRef]
- Kimbrel, N.A. A Model of the Development and Maintenance of Generalized Social Phobia. Clin. Psychol. Rev. 2008, 28, 592–612. [Google Scholar] [CrossRef] [PubMed]
- Elzinga, B.M.; Spinhoven, P.; Berretty, E.; de Jong, P.; Roelofs, K. The Role of Childhood Abuse in HPA-Axis Reactivity in Social Anxiety Disorder: A Pilot Study. Biol. Psychol. 2010, 83, 1–6. [Google Scholar] [CrossRef]
- Goldin, P.R.; Manber, T.; Hakimi, S.; Canli, T.; Gross, J.J. Neural Bases of Social Anxiety Disorder: Emotional Reactivity and Cognitive Regulation during Social and Physical Threat: Emotional Reactivity and Cognitive Regulation during Social and Physical Threat. Arch. Gen. Psychiatry 2009, 66, 170–180. [Google Scholar] [CrossRef]
- Hofmann, S.G. Cognitive Mediation of Treatment Change in Social Phobia. J. Consult. Clin. Psychol. 2004, 72, 392–399. [Google Scholar] [CrossRef]
- Straube, T.; Kolassa, I.-T.; Glauer, M.; Mentzel, H.-J.; Miltner, W.H.R. Effect of Task Conditions on Brain Responses to Threatening Faces in Social Phobics: An Event-Related Functional Magnetic Resonance Imaging Study. Biol. Psychiatry 2004, 56, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Goldin, P.R.; Sareen, J.; Zorrilla, L.T.E.; Brown, G.G. Increased Amygdala Activation to Angry and Contemptuous Faces in Generalized Social Phobia. Arch. Gen. Psychiatry 2002, 59, 1027–1034. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Harris, M.G.; Kazdin, A.E.; Vigo, D.V.; Sampson, N.A.; Chiu, W.T.; Al-Hamzawi, A.; Alonso, J.; Altwaijri, Y.A.; Andrade, L.; et al. Perceived Helpfulness of Treatment for Social Anxiety Disorder: Findings from the WHO World Mental Health Surveys. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 2079–2095. [Google Scholar] [CrossRef]
- Chavira, D.A.; Stein, M.B. Childhood Social Anxiety Disorder: From Understanding to Treatment. Child. Adolesc. Psychiatr. Clin. N. Am. 2005, 14, 797–818. [Google Scholar] [CrossRef]
- Grant, B.F.; Hasin, D.S.; Blanco, C.; Stinson, F.S.; Chou, S.P.; Goldstein, R.B.; Dawson, D.A.; Smith, S.; Saha, T.D.; Huang, B. The Epidemiology of Social Anxiety Disorder in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2005, 66, 1351–1361. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, Severity, and Comorbidity of 12-Month DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef]
- MacKenzie, M.B.; Fowler, K.F. Social Anxiety Disorder in the Canadian Population: Exploring Gender Differences in Sociodemographic Profile. J. Anxiety Disord. 2013, 27, 427–434. [Google Scholar] [CrossRef]
- Single, A.; Bilevicius, E.; Ho, V.; Theule, J.; Buckner, J.D.; Mota, N.; Keough, M.T. Cannabis Use and Social Anxiety in Young Adulthood: A Meta-Analysis. Addict. Behav. 2022, 129, 107275. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Shaw, S. A Study to Investigate the Prevalence of Social Anxiety in a Sample of Higher Education Students in the United Kingdom. J. Ment. Health 2009, 18, 198–206. [Google Scholar] [CrossRef]
- Jefferies, P.; Ungar, M. Social Anxiety in Young People: A Prevalence Study in Seven Countries. PLoS ONE 2020, 15, e0239133. [Google Scholar] [CrossRef]
- Rodebaugh, T.L.; Holaway, R.M.; Heimberg, R.G. The Treatment of Social Anxiety Disorder. Clin. Psychol. Rev. 2004, 24, 883–908. [Google Scholar] [CrossRef]
- Carlton, C.N.; Sullivan-Toole, H.; Strege, M.V.; Ollendick, T.H.; Richey, J.A. Mindfulness-Based Interventions for Adolescent Social Anxiety: A Unique Convergence of Factors. Front. Psychol. 2020, 11, 1783. [Google Scholar] [CrossRef]
- Hjeltnes, A.; Molde, H.; Schanche, E.; Vøllestad, J.; Lillebostad Svendsen, J.; Moltu, C.; Binder, P.-E. An Open Trial of Mindfulness-Based Stress Reduction for Young Adults with Social Anxiety Disorder. Scand. J. Psychol. 2017, 58, 80–90. [Google Scholar] [CrossRef]
- Liu, X.; Yi, P.; Ma, L.; Liu, W.; Deng, W.; Yang, X.; Liang, M.; Luo, J.; Li, N.; Li, X. Mindfulness-Based Interventions for Social Anxiety Disorder: A Systematic Review and Meta-Analysis. Psychiatry Res. 2021, 300, 113935. [Google Scholar] [CrossRef]
- Norton, A.R.; Abbott, M.J.; Norberg, M.M.; Hunt, C. A Systematic Review of Mindfulness and Acceptance-Based Treatments for Social Anxiety Disorder. J. Clin. Psychol. 2015, 71, 283–301. [Google Scholar] [CrossRef]
- Goldin, P.R.; Morrison, A.; Jazaieri, H.; Brozovich, F.; Heimberg, R.; Gross, J.J. Group CBT versus MBSR for Social Anxiety Disorder: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2016, 84, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Chapdelaine, A.; Carrier, J.-D.; Fournier, L.; Duhoux, A.; Roberge, P. Treatment Adequacy for Social Anxiety Disorder in Primary Care Patients. PLoS ONE 2018, 13, e0206357. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Michaelis, S. Epidemiology of Anxiety Disorders in the 21st Century. Dialogues Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Goetter, E.M.; Frumkin, M.R.; Palitz, S.A.; Swee, M.B.; Baker, A.W.; Bui, E.; Simon, N.M. Barriers to Mental Health Treatment among Individuals with Social Anxiety Disorder and Generalized Anxiety Disorder. Psychol. Serv. 2020, 17, 5–12. [Google Scholar] [CrossRef]
- Chartier-Otis, M.; Perreault, M.; Bélanger, C. Determinants of Barriers to Treatment for Anxiety Disorders. Psychiatr. Q. 2010, 81, 127–138. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health (UK). Social Anxiety Disorder: Recognition, Assessment and Treatment; British Psychological Society (UK): Leicester, UK, 2013; ISBN 9781909726031. [Google Scholar]
- Ranta, K.; Kaltiala-Heino, R.; Rantanen, P.; Marttunen, M. Social Phobia in Finnish General Adolescent Population: Prevalence, Comorbidity, Individual and Family Correlates, and Service Use. Depress. Anxiety 2009, 26, 528–536. [Google Scholar] [CrossRef]
- Wolitzky-Taylor, K.; LeBeau, R. Recent Advances in the Understanding and Psychological Treatment of Social Anxiety Disorder. Fac. Rev. 2023, 12, 8. [Google Scholar] [CrossRef]
- Alyami, M.; Giri, B.; Alyami, H.; Sundram, F. Social Anxiety Apps: A Systematic Review and Assessment of App Descriptors across Mobile Store Platforms. Evid. Based. Ment. Health 2017, 20, 65–70. [Google Scholar] [CrossRef]
- Gaekwad, J.S.; Sal Moslehian, A.; Roös, P.B.; Walker, A. A Meta-Analysis of Emotional Evidence for the Biophilia Hypothesis and Implications for Biophilic Design. Front. Psychol. 2022, 13, 750245. [Google Scholar] [CrossRef]
- Clemente, D.; Romano, L.; Zamboni, E.; Carrus, G.; Panno, A. Forest Therapy Using Virtual Reality in the Older Population: A Systematic Review. Front. Psychol. 2023, 14, 1323758. [Google Scholar] [CrossRef] [PubMed]
- Reese, G.; Stahlberg, J.; Menzel, C. Digital Shinrin-Yoku: Do Nature Experiences in Virtual Reality Reduce Stress and Increase Well-Being as Strongly as Similar Experiences in a Physical Forest? Virtual Real. 2022, 26, 1245–1255. [Google Scholar] [CrossRef]
- Syed Abdullah, S.S.; Awang Rambli, D.R.; Sulaiman, S.; Alyan, E.; Merienne, F.; Diyana, N. The Impact of Virtual Nature Therapy on Stress Responses: A Systematic Qualitative Review. For. Trees Livelihoods 2021, 12, 1776. [Google Scholar] [CrossRef]
- Lee, M.; Kim, E.; Choe, J.; Choi, S.; Ha, S.; Kim, G. Psychological Effects of Green Experiences in a Virtual Environment: A Systematic Review. Forests 2022, 13, 1625. [Google Scholar] [CrossRef]
- Browning, M.H.E.M.; Shin, S.; Drong, G.; McAnirlin, O.; Gagnon, R.J.; Ranganathan, S.; Sindelar, K.; Hoptman, D.; Bratman, G.N.; Yuan, S.; et al. Daily Exposure to Virtual Nature Reduces Symptoms of Anxiety in College Students. Sci. Rep. 2023, 13, 1239. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Cervera-Martínez, J. Lifestyle Prescription for Depression with a Focus on Nature Exposure and Screen Time: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 5094. [Google Scholar] [CrossRef]
- Farrow, M.R.; Washburn, K. A Review of Field Experiments on the Effect of Forest Bathing on Anxiety and Heart Rate Variability. Glob. Adv. Health Med. 2019, 8, 2164956119848654. [Google Scholar] [CrossRef]
- Li, H.; Dong, W.; Wang, Z.; Chen, N.; Wu, J.; Wang, G.; Jiang, T. Effect of a Virtual Reality-Based Restorative Environment on the Emotional and Cognitive Recovery of Individuals with Mild-to-Moderate Anxiety and Depression. Int. J. Environ. Res. Public Health 2021, 18, 9053. [Google Scholar] [CrossRef]
- Zeng, N.; Pope, Z.; Lee, J.E.; Gao, Z. Virtual Reality Exercise for Anxiety and Depression: A Preliminary Review of Current Research in an Emerging Field. J. Clin. Med. Res. 2018, 7, 42. [Google Scholar] [CrossRef]
- Kim, C.M.; van Rompay, T.J.L.; Louwers, G.L.M.; Yoon, J.; Ludden, G.D.S. From a Morning Forest to a Sunset Beach: Understanding Visual Experiences and the Roles of Personal Characteristics for Designing Relaxing Digital Nature. Int. J. Hum. Comput. Interact. 2024, 40, 8535–8552. [Google Scholar] [CrossRef]
- Tsunetsugu, Y.; Park, B.-J.; Miyazaki, Y. Trends in Research Related to “Shinrin-Yoku” (taking in the Forest Atmosphere or Forest Bathing) in Japan. Environ. Health Prev. Med. 2010, 15, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef]
- Chun, M.H.; Chang, M.C.; Lee, S.-J. The Effects of Forest Therapy on Depression and Anxiety in Patients with Chronic Stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Yeon, P.-S.; Jeon, J.-Y.; Jung, M.-S.; Min, G.-M.; Kim, G.-Y.; Han, K.-M.; Shin, M.-J.; Jo, S.-H.; Kim, J.-G.; Shin, W.-S. Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12685. [Google Scholar] [CrossRef]
- Alyan, E.; Combe, T.; Awang Rambli, D.R.; Sulaiman, S.; Merienne, F.; Diyana, N. The Influence of Virtual Forest Walk on Physiological and Psychological Responses. Int. J. Environ. Res. Public Health 2021, 18, 11420. [Google Scholar] [CrossRef]
- Mohamad Yahaya, N.A.; Awang Rambli, D.R.; Sulaiman, S.; Merienne, F.; Alyan, E. Design of Game-Based Virtual Forests for Psychological Stress Therapy. For. Trees Livelihoods 2023, 14, 288. [Google Scholar] [CrossRef]
- Reese, G.; Kohler, E.; Menzel, C. Restore or Get Restored: The Effect of Control on Stress Reduction and Restoration in Virtual Nature Settings. Sustain. Sci. Pract. Policy 2021, 13, 1995. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Y.; An, J.; Dong, W.; Li, H.; Ma, H.; Wang, J.; Wu, J.; Jiang, T.; Wang, G. Effects of Restorative Environment and Presence on Anxiety and Depression Based on Interactive Virtual Reality Scenarios. Int. J. Environ. Res. Public Health 2022, 19, 7878. [Google Scholar] [CrossRef]
- Damen, K.H.B.; van der Spek, E.D. Virtual Reality as E-Mental Health to Support Starting with Mindfulness-Based Cognitive Therapy. In Proceedings of the Entertainment Computing—ICEC 2018, Poznan, Poland, 17–20 September 2018; Springer International Publishing: Cham, Switzerland, 2018; pp. 241–247. [Google Scholar]
- Kirschner, P.A. Cognitive Load Theory: Implications of Cognitive Load Theory on the Design of Learning. Learn. Instr. 2002, 12, 1–10. [Google Scholar] [CrossRef]
- Sari, R.C.; Pranesti, A.; Solikhatun, I.; Nurbaiti, N.; Yuniarti, N. Cognitive Overload in Immersive Virtual Reality in Education: More Presence but Less Learnt? Educ. Inf. Technol. 2024, 29, 12887–12909. [Google Scholar] [CrossRef]
- Souchet, A.D.; Philippe, S.; Lourdeaux, D.; Leroy, L. Measuring Visual Fatigue and Cognitive Load via Eye Tracking While Learning with Virtual Reality Head-Mounted Displays: A Review. Int. J. Hum. Comput. Interact. 2022, 38, 801–824. [Google Scholar] [CrossRef]
- Mattick, R.P.; Clarke, J.C. Development and Validation of Measures of Social Phobia Scrutiny Fear and Social Interaction Anxiety. Behav. Res. Ther. 1998, 36, 455–470. [Google Scholar] [CrossRef] [PubMed]
- Heimberg, R.G.; Mueller, G.P.; Holt, C.S.; Hope, D.A.; Liebowitz, M.R. Assessment of Anxiety in Social Interaction and Being Observed by Others: The Social Interaction Anxiety Scale and the Social Phobia Scale. Behav. Ther. 1992, 23, 53–73. [Google Scholar] [CrossRef]
- Korpela, K.M.; Ylén, M.; Tyrväinen, L.; Silvennoinen, H. Determinants of Restorative Experiences in Everyday Favorite Places. Health Place 2008, 14, 636–652. [Google Scholar] [CrossRef]
- Mattila, O.; Korhonen, A.; Pöyry, E.; Hauru, K.; Holopainen, J.; Parvinen, P. Restoration in a Virtual Reality Forest Environment. Comput. Hum. Behav. 2020, 107, 106295. [Google Scholar] [CrossRef]
- Staats, H.; Kieviet, A.; Hartig, T. Where to Recover from Attentional Fatigue: An Expectancy-Value Analysis of Environmental Preference. J. Environ. Psychol. 2003, 23, 147–157. [Google Scholar] [CrossRef]
- Takayama, N.; Korpela, K.; Lee, J.; Morikawa, T.; Tsunetsugu, Y.; Park, B.-J.; Li, Q.; Tyrväinen, L.; Miyazaki, Y.; Kagawa, T. Emotional, Restorative and Vitalizing Effects of Forest and Urban Environments at Four Sites in Japan. Int. J. Environ. Res. Public Health 2014, 11, 7207–7230. [Google Scholar] [CrossRef]
- Koivisto, M.; Koskinen, J.; Jokiaho, S.; Vahanne, T.; Pohjola, M.; Kontio, E. A Short Simulated Nature Experience as an Effective Way to Promote Restoration from Work-Related Stress. Scand. J. Psychol. 2024, 65, 954–965. [Google Scholar] [CrossRef]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Validation of the Virtual Reality Neuroscience Questionnaire: Maximum Duration of Immersive Virtual Reality Sessions Without the Presence of Pertinent Adverse Symptomatology. Front. Hum. Neurosci. 2019, 13, 417. [Google Scholar] [CrossRef]
- Sarkhel, S.; Singh, O.P.; Arora, M. Clinical Practice Guidelines for Psychoeducation in Psychiatric Disorders General Principles of Psychoeducation. Indian J. Psychiatry 2020, 62, S319–S323. [Google Scholar] [CrossRef]
- Andrews, G. The Treatment of Anxiety Disorders: Clinician Guides and Patient Manuals; Cambridge University Press: Cambridge, UK, 2003; ISBN 9780521788779. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living (Revised Edition): Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Random House Publishing Group: New York, NY, USA, 2013; ISBN 9780345536938. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression, First Edition: A New Approach to Preventing Relapse; Guilford Publications: New York, NY, USA, 2001; ISBN 9781572307063. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-Based Interventions in Context: Past, Present, and Future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Hachette Books: New York, NY, USA, 2009; ISBN 9781401394677. [Google Scholar]
- Hofmann, S.G.; Grossman, P.; Hinton, D.E. Loving-Kindness and Compassion Meditation: Potential for Psychological Interventions. Clin. Psychol. Rev. 2011, 31, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Spector, P.E. Summated Rating Scale Construction: An Introduction; SAGE: Thousand Oaks, CA, USA, 1992; ISBN 9780803943414. [Google Scholar]
- Peters, L.; Sunderland, M.; Andrews, G.; Rapee, R.M.; Mattick, R.P. Development of a Short Form Social Interaction Anxiety (SIAS) and Social Phobia Scale (SPS) Using Nonparametric Item Response Theory: The SIAS-6 and the SPS-6. Psychol. Assess. 2012, 24, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Korcz, N.; Janeczko, E.; Bielinis, E.; Urban, D.; Koba, J.; Szabat, P.; Małecki, M. Influence of Informal Education in the Forest Stand Redevelopment Area on the Psychological Restoration of Working Adults. Forests 2021, 12, 993. [Google Scholar] [CrossRef]
- Ch, N.A.N.; Ansah, A.A.; Katrahmani, A.; Burmeister, J.; Kun, A.L.; Mills, C.; Shaer, O.; Lee, J.D. Virtual Nature Experiences and Mindfulness Practices While Working from Home during COVID-19: Effects on Stress, Focus, and Creativity. Int. J. Hum. Comput. Stud. 2023, 171, 102982. [Google Scholar] [CrossRef]
- Gao, N.; Xie, T.; Liu, G. A Learning Engagement Model of Educational Games Based on Virtual Reality. In Proceedings of the 2018 International Joint Conference on Information, Media and Engineering (ICIME), Osaka, Japan, 12–14 December 2018; IEEE: Piscataway, NJ, USA. [Google Scholar]
- Lasekan, O.A.; Pachava, V.; Godoy Pena, M.T.; Golla, S.K.; Raje, M.S. Investigating Factors Influencing Students’ Engagement in Sustainable Online Education. Sustainability 2024, 16, 689. [Google Scholar] [CrossRef]
- Ma, S.; Varley, M.; Shark, L.-K.; Richards, J. Overcoming the Information Overload Problem in a Multiform Feedback-Based Virtual Reality System for Hand Motion Rehabilitation: Healthy Subject Case Study. Virtual Real. 2012, 16, 325–334. [Google Scholar] [CrossRef]
- Naef, A.C.; Gerber, S.M.; Single, M.; Müri, R.M.; Haenggi, M.; Jakob, S.M.; Jeitziner, M.-M.; Nef, T. Effects of Immersive Virtual Reality on Sensory Overload in a Random Sample of Critically Ill Patients. Front. Med. 2023, 10, 1268659. [Google Scholar] [CrossRef]
- Jo, H.; Song, C.; Ikei, H.; Enomoto, S.; Kobayashi, H.; Miyazaki, Y. Physiological and Psychological Effects of Forest and Urban Sounds Using High-Resolution Sound Sources. Int. J. Environ. Res. Public Health 2019, 16, 2649. [Google Scholar] [CrossRef]
- Ochiai, H.; Song, C.; Jo, H.; Oishi, M.; Imai, M.; Miyazaki, Y. Relaxing Effect Induced by Forest Sound in Patients with Gambling Disorder. Sustain. Sci. Pract. Policy 2020, 12, 5969. [Google Scholar] [CrossRef]
- Annerstedt, M.; Jönsson, P.; Wallergård, M.; Johansson, G.; Karlson, B.; Grahn, P.; Hansen, A.M.; Währborg, P. Inducing Physiological Stress Recovery with Sounds of Nature in a Virtual Reality Forest--Results from a Pilot Study. Physiol. Behav. 2013, 118, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, A.; Ross, E.; Nikles, D.; De Cesare, E.; Tran, C.; Pensini, P. Nature Guided Imagery: An Intervention to Increase Connectedness to Nature. J. Environ. Psychol. 2022, 80, 101759. [Google Scholar] [CrossRef]
- Felix, M.M.D.S.; Ferreira, M.B.G.; da Cruz, L.F.; Barbosa, M.H. Relaxation Therapy with Guided Imagery for Postoperative Pain Management: An Integrative Review. Pain Manag. Nurs. 2019, 20, 3–9. [Google Scholar] [CrossRef]
- Butler, R.M.; O’Day, E.B.; Heimberg, R.G. The Benefits of a Longer Course of Cognitive Behavioral Therapy for Some Patients with Social Anxiety Disorder. Cogn. Behav. Ther. 2021, 50, 351–365. [Google Scholar] [CrossRef]
- Clark, D.M.; Wild, J.; Warnock-Parkes, E.; Stott, R.; Grey, N.; Thew, G.; Ehlers, A. More than Doubling the Clinical Benefit of Each Hour of Therapist Time: A Randomised Controlled Trial of Internet Cognitive Therapy for Social Anxiety Disorder. Psychol. Med. 2023, 53, 5022–5032. [Google Scholar] [CrossRef]
- Letamendi, A.M.; Chavira, D.A.; Stein, M.B. Issues in the Assessment of Social Phobia: A Review. Isr. J. Psychiatry Relat. Sci. 2009, 46, 13–24. [Google Scholar]
- Malhotra, M. Reducing Cybersickness in VR Locomotion with Compatible Physical Movement Input. Master’s Thesis, University of Toronto, Toronto, ON, Canada, 2024. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session | A | B | Non-VR |
|---|---|---|---|
| 1 | 18 | 22 | 18 |
| 2 | 5 | 4 |
| SIAS Items | Factor Loadings |
|---|---|
| 1. I get nervous if I have to speak with someone in authority (teacher, boss, etc.). | 0.637 |
| 2. I have difficulty making eye contact with others. | 0.509 |
| 3. I become tense if I have to talk about myself or my feelings. | 0.472 |
| 4. I find it difficult to mix comfortably with the people I work with. | 0.803 |
| 5. I find it difficult to make friends my own age. | 0.359 |
| 6. I tense up if I meet an acquaintance in the street. | 0.606 |
| 7. When mixing socially, I am uncomfortable. | 0.768 |
| 8. I feel tense if I am alone with just one other person. | 0.380 |
| 9. I have difficulty meeting people at parties, etc. | 0.371 |
| 10. I have difficulty talking with other people. | 0.707 |
| 11. I find it difficult to think of things to talk about. | 0.433 |
| 12. I worry about expressing myself in case I appear awkward. | 0.749 |
| 13. I find it difficult to disagree with another’s point of view. | 0.529 |
| 14. I have difficulty talking to people I am attracted to. | 0.184 |
| 15. I find myself worrying that I won’t know what to say in social situations. | 0.722 |
| 16. I am nervous mixing with people I don’t know well. | 0.692 |
| 17. I feel I’ll say something embarrassing when talking. | 0.814 |
| 18. When mixing in a group, I find myself worrying I will be ignored. | 0.601 |
| 19. I am tense mixing in a group. | 0.771 |
| 20. I am unsure whether to greet someone I know only slightly. | 0.539 |
| Phase and Cronbach’s Alpha | SIAS Items |
|---|---|
| S1 Pre = 0.87 S1 Post = 0.93 | 7. When mixing socially, I am uncomfortable. 12. I worry about expressing myself in case I appear awkward. 15. I find myself worrying that I won’t know what to say in social situations. 17. I feel I’ll say something embarrassing when talking. 19. I am tense mixing in a group. |
| Checkpoint | Condition | Correct | Incorrect |
|---|---|---|---|
| 1 | B | 41 | 1 |
| Non-VR | 35 | 1 | |
| 2 | B | 19 | 2 |
| Non-VR | 17 | 1 | |
| 3 | B | 40 | 2 |
| Non-VR | 12 | 18 |
| Condition | Comments | Sentiment Score |
|---|---|---|
| Comments with highest three sentiment scores across three conditions | ||
| A | I found the sounds and relaxing graphics to be of great stress relief. i also found that it was easy to become immersed into and feel a great sense of calm. The structures were nice as they were all different and invoked a sense of interest and wonder. I enjoyed the experience thoroughly. | 0.98 |
| B | I like how there are cute animals included in there, but it’ll be better if they are all pushable (pushing animals is satisfying idk why). Also, when I was exploring the river I was expecting something under the surface (maybe fish) but turns out there’s none, which makes me feel kind of disappointed… But overall the experience is good, the forest is pretty and the sound effect is really realistic. I’ll come back if I have time. Thank you for the experiment! | 0.95 |
| Non-VR | I enjoyed the modules, very helpful, thank you. | 0.85 |
| Comments with lowest three sentiment scores across three conditions | ||
| A | I loved the environment that was created with the headset and I found myself immersed in the VR world but the feeling of nausea I had took me out of the experience and was the only thing that made me uncomfortable and what I didn’t like. | −0.33 |
| B | I liked some of the images like the clouds, river, and flowers, but i also found it a bit distracting since i did feel i was in a virtual reality that was not real. It also made me nauseous, which made it harder to concentrate. | −0.04 |
| Non-VR | Great experience but for module 4, I found it very boring and long so I may have lost focus there. | −0.64 |
| Condition | Comments |
|---|---|
| A | “sound was very calming” |
| “I really enjoyed the sounds and the graphics” | |
| “The sound and visual images made me feel like I am actually in the forest, so I felt calm.” | |
| “I feel like the visuals and the sounds were realistic enough to make my experience similar to a real-life experience.” | |
| “I think the environment that it built was really nice, but the soundtrack was the part that made it more alive.” | |
| B | “An aspect that particularly stood out to me was the sound quality, which was really good (both the forest background noises and the checkpoint narrator’s voice).” |
| “The aspect of the application that stood out to me was the sound quality. There was a lot of richness to the forest sounds, and the sound quality of the male narrator’s voice was also really good. It felt like it was coming from everywhere and nowhere at once.” | |
| “The forest is pretty and the sound effect is really realistic.” | |
| Non-VR | “The background sounds were very relaxing and helped me visualize that I was in a forest.” |
| “The sound effects were quite vivid which help immerse quickly.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.Z.; Beggs, M.; Xue, Y.; Gao, S.; Seok, J.; Xiao, Y.; Zhou, Z.; Zhou, Y.; Mariakakis, A.; Chignell, M. Are Virtual Forests Just for Relaxation, or Can They Enhance the Benefits of Therapy? Healthcare 2025, 13, 621. https://doi.org/10.3390/healthcare13060621
Hu YZ, Beggs M, Xue Y, Gao S, Seok J, Xiao Y, Zhou Z, Zhou Y, Mariakakis A, Chignell M. Are Virtual Forests Just for Relaxation, or Can They Enhance the Benefits of Therapy? Healthcare. 2025; 13(6):621. https://doi.org/10.3390/healthcare13060621
Chicago/Turabian StyleHu, You Zhi, Max Beggs, Yu Xue, Sinuo Gao, Junyoung Seok, Yawen Xiao, Ziqi Zhou, Yifei Zhou, Alex Mariakakis, and Mark Chignell. 2025. "Are Virtual Forests Just for Relaxation, or Can They Enhance the Benefits of Therapy?" Healthcare 13, no. 6: 621. https://doi.org/10.3390/healthcare13060621
APA StyleHu, Y. Z., Beggs, M., Xue, Y., Gao, S., Seok, J., Xiao, Y., Zhou, Z., Zhou, Y., Mariakakis, A., & Chignell, M. (2025). Are Virtual Forests Just for Relaxation, or Can They Enhance the Benefits of Therapy? Healthcare, 13(6), 621. https://doi.org/10.3390/healthcare13060621