Abstract
Background: Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that affects social interaction, communication, and behavior. Traditional interventions such as Applied Behavior Analysis and sensory integration therapy often lack a person-centered approach. Art therapy offers a creative and holistic alternative for supporting children and adolescents with ASD. Objectives: This study systematically reviewed and evaluated the effectiveness, modalities, formats, and methodological quality of randomized controlled trials (RCTs) involving art therapy interventions for children and adolescents with ASD. Methods: A systematic search of eight databases identified 12 RCTs involving art therapy for children and adolescents with ASD. Intervention outcomes, formats, and methodological rigor were assessed through this systematic review. Methodological rigor was assessed using the Cochrane ROB 2.0 tool, and the Delphi list with four additional items. Results: Art therapy showed promise in reducing ASD symptoms and stress-related symptoms, and in improving social communication, motor skills, language, and neurodevelopment. Most studies had limitations, including small sample sizes, short durations, a high risk of bias, and low methodological quality. Conclusions: Although existing studies suggest that art therapy may benefit children and adolescents with ASD, further rigorously designed studies are required to establish its efficacy and inform evidence-based practice.
1. Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition characterized by persistent deficits in social communication and restricted, repetitive patterns of behavior [1]. Children and adolescents with ASD may experience difficulties in understanding social-emotional reciprocity, as well as in verbal and nonverbal communication. They often have impaired abilities to develop, maintain, and comprehend relationships, alongside ritualized behavior patterns, abnormal intensity or focus of interests, and hypersensitivity or hyperreactivity to sensory input [1,2,3,4]. ASD affects approximately 0.6% to 0.72% of children and adolescents worldwide from an early age, with recent meta-analyses indicating an increasing prevalence over recent decades [1,2,3,4]. ASD can lead to functional impairments in various settings, thus qualifying it as a disability. In school, children and adolescents with ASD frequently struggle with adhering to rules, achieving academic success, and interacting with peers, placing them at a higher risk of being bullied [5,6]. In community settings, they may encounter challenges in organizing or planning their daily activities [7]. These discrepancies between the external environment and the characteristics of ASD can result in frustration and anxiety among them, negatively impacting their and their caregivers’ psychological well-being [8].
Intervention for ASDs encompasses a variety of approaches targeting different socio-behavioral symptoms. These treatments include Applied Behavior Analysis (ABA), Cognitive Behavioral Therapy (CBT), Sensory Integration Therapy (SIT), Early Start Denver Model (ESDM), and therapies focusing on social and professional skills [9]. While these interventions have demonstrated effectiveness, each comes with its own limitations. ABA, despite its widespread use and evidence-based success, has been criticized for being too rigid and overly focused on compliance rather than fostering intrinsic motivation and personal autonomy [10]. Therapies focusing on social skills and occupational training can be highly effective but may fall short if not tailored to the individual’s needs and often struggle with generalization to real-world settings [11]. Sensory integration therapy is criticized for focusing on symptoms rather than the holistic needs [12]. Overall, while these approaches show benefits, their effectiveness can be limited in generalizing to real-life situations, and a lack of emphasis on empowerment and holistic health. In response, practitioners have increasingly adopted more person-centered and developmentally appropriate approaches, such as art therapy. However, empirical evidence supporting the effectiveness of art therapy for children and adolescents with ASD remains limited [13,14,15,16]. To address this gap, the present study investigates the impact of art therapy on the psychological, social, and behavioral outcomes of children under the age of 18 diagnosed with ASD.
1.1. Benefits of Art Therapy on Children and Adolescents with ASD
Art therapy is a holistic therapeutic approach that integrates principles from mental health, human development, and psychological theory with various art modalities—such as visual art, music, movement, drama, and creative writing—to promote individual and community well-being [17,18]. Art therapy adopts approaches from psychodynamic therapy, humanistic approaches, and family therapy, and its key features include using art (e.g., drawing, music, drama) to facilitate psychological healing; symbolic expression; client-centered and strength-based practice; and nonverbal and multisensory experience [18]. With these features, art therapy can effectively promote emotional expression by externalizing inner experiences in a safe and symbolic form; facilitate self-discovery and strengthen self-efficacy; alleviate stress and anxiety; and encourage positive coping strategies support. It can also foster interpersonal interaction and communication, particularly in group settings [19].
Art therapy may support children and adolescents with ASD in sensory processing, attention abilities, flexibility, motor skills, social learning, and emotional expression [20]. In art therapy, therapists create safe, rich and supportive sensory experiences for children to facilitate sensory integration and processing [21]. By “looking together”, during the art-making process, art therapy enhances joint attention ability and further fosters social learning and attachment [22]. In art therapy, children and adolescents are typically encouraged to create artwork freely by themselves, which can increase behavioral flexibility, strengthen their motor skills, and promote relaxation in daily environments [20]. As children and adolescents with ASD often struggle to identify and verbally express emotions, art therapy can serve as a safe medium for emotional expression and support mental well-being [20,23].
1.2. A Theoretical Framework for Art Therapy in ASD
Beyond the potential benefits described above, and considering the psychoanalytic and humanistic foundations of art therapy [17,18,24], this paper proposes Self-Determination Theory (SDT) as a conceptual framework to better understand the mechanisms underlying the effectiveness of art therapy for individuals with ASD [25,26,27,28].
SDT posits that psychological well-being is supported by the fulfillment of three fundamental needs: autonomy, competence, and relatedness. Autonomy—the experience of acting with volition and self-endorsement—is considered the central psychological need within SDT. Research indicates that environments fostering autonomy, such as classrooms and therapeutic settings, are associated with increased engagement, reduced anxiety, improved emotional regulation, and enhanced social and academic outcomes [26,28,29]. Competence refers to the sense of effectiveness and mastery in one’s activities, while relatedness involves forming meaningful interpersonal connections. A growing body of evidence supports positive associations between competence, relatedness, and psychosocial well-being in both neurotypical children and those with ASD [28,30,31].
Art therapy establishes conditions that support the fulfillment of psychological needs, thereby enhancing the psychological, social, and behavioral outcomes of children with ASD. Its defining characteristics include: (a) freedom and choice, which foster autonomy; (b) non-directive art-making, which supports competence through self-paced exploration; and (c) non-verbal, sensory-rich activities, which promote relatedness and emotional expression, particularly for children and adolescents with limited verbal communication. These elements are illustrated in Figure 1, which conceptualizes the relationship between art therapy and the fulfillment of psychological needs in children and adolescents with ASD.
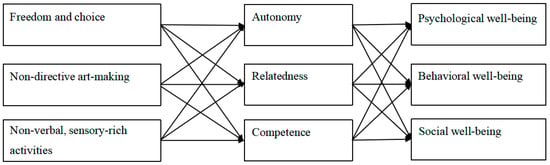
Figure 1.
Art Therapy, Self Determination Theory and Psychosocial and Behavioral Outcomes.
Freedom and Choice. Art therapy provides a compelling avenue for fostering autonomy by offering children opportunities to make choices and exercise personal agency [32]. Within these therapeutic settings, children are encouraged to engage in art-making that reflects their individual preferences, interests, and emotional needs, free from rigid expectations or predetermined outcomes. This open-ended structure enables spontaneous, self-directed expression, particularly evident in multimodal arts activities, where children can choose among various mediums—such as painting, music, or movement—and transition between them as they wish [18].
Such autonomy-supportive environments not only enhance children’s sense of control but also contribute to feelings of competence, thereby promoting positive psychosocial and behavioral outcomes [25]. The inherently enjoyable and self-directed nature of art-making further facilitates relatedness, as children and therapists collaboratively explore the deeper meanings embedded in the creative process, fostering trust and emotional connection [18,32]. Moreover, completing a personally meaningful art product reinforces competence by empowering children to take ownership of the entire creative process—from inception to final realization—thereby strengthening their confidence and sense of achievement [18,32].
Non-directive Arts-Making. A defining feature of art therapy is its non-directive and facilitative approach, in which therapists adopt a supportive rather than prescriptive role [18,20]. Therapists honor each child’s pace and preferences, offering gentle guidance and constructive feedback that nurture both autonomy and competence. This respectful dynamic fosters a genuine therapeutic alliance, which may serve as a model for broader social engagement and connection [33].
In addition to supporting individual expression, collaborative arts-based projects—such as group murals or ensemble music-making—offer opportunities for children with ASD to practice and develop social relatedness [34,35]. The non-directive nature of these group activities encourages spontaneous social interaction, enabling children to engage in authentic communication and relationship-building within a relaxed, low-pressure environment. Such settings support the development of perspective-taking, empathy, and cooperation—skills that are often challenging for children on the spectrum [20,32,35,36].
Non-verbal and Sensory-Rich Activities. The non-verbal and sensory-rich nature of art therapy makes it particularly well-suited for children with ASD who experience sensory over-responsiveness and limited verbal communication abilities [37,38]. By engaging in the expressive and non-cognitive domains of the brain, arts-based activities provide alternative pathways for self-expression and interpersonal communication [20,32]. For example, in family therapy sessions, children may use movement, singing, or visual art to express affection—bypassing the need for verbal articulation and enabling more authentic emotional expression.
The sensory-rich qualities of art therapy—such as the tactile experience of sculpting, the visual stimulation of colors, and the auditory engagement of music—can support sensory integration and emotional regulation in children with ASD [20]. These structured therapeutic experiences help children become more familiar with sensory stimuli and learn to manage hypersensitive responses within a safe and supportive environment. Over time, such engagement may lead to improvements in social behavior, emotional flexibility, and adaptive functioning.
Moreover, effective sensory integration lays the foundation for emotional self-regulation, which is essential for developing social competence and behavioral self-management. As children become more confident in managing sensory input, they are more likely to experience a sense of autonomy and competence in navigating the often unpredictable and overstimulating social environment [39,40,41].
1.3. Research Gap and Research Questions
Despite growing interest in art therapy for children with ASD, the academic community continues to grapple with clarifying its overall effectiveness. Existing review studies frequently focus on single-case designs, isolated art modalities, or narrowly defined outcome categories, which limits the generalizability and applicability of findings [13,14,15,16,20,42]. Moreover, there is a lack of comprehensive synthesis evaluating both the methodological rigor and multidimensional outcomes of art therapy for children with ASD. To address this gap, the present study conducts a systematic review to assess the effectiveness and methodological quality of art therapy interventions for children with ASD. This study is guided by the following research questions:
- What outcomes have been identified in art therapy for children and adolescents with ASD?
- How effective is art therapy in promoting positive developmental outcomes in children and adolescents with ASD?
- What theoretical frameworks have guided the design of art therapy for children and adolescents with ASD?
- What intervention strategies—regarding art modality and format (e.g., individual vs. group)—are associated with positive outcomes?
- What is the methodological rigor of existing art therapy studies for children and adolescents with ASD?
2. Methods
This systematic review was conducted in accordance with the PRISMA 2020 guidelines, ensuring transparency and methodological rigor [43]. This review was registered on the Open Science Framework (OSF). Registration DOI: https://doi.org/10.17605/OSF.IO/XAG58 (accessed on 1 November 2025).
2.1. Search Strategy
To evaluate the effectiveness of various forms of art therapy for children and adolescents with ASD, a comprehensive search was conducted across eight electronic databases: PsycINFO, PsycARTICLES, PubMed, Web of Science, Scopus, EMBASE, CINAHL, and Medline. The search was conducted with a cutoff date of 1 November 2024, and included only articles published prior to this date. A detailed list of search terms is provided in Appendix A.
2.2. Study Selection
All studies were manually screened and data were independently extracted by two reviewers. At each stage, each reviewer conducted the initial screening independently and resolved the discrepancies through subsequent discussion. Studies were included based on the following criteria: (a) randomized controlled trials (RCTs); (b) participants aged 18 years or younger diagnosed with ASD; (c) interventions employing art therapy approaches. In this study, art therapy refers to interventions using visual art, music, dance/movement, drama, poetry/writing, and intermodal or multimodal approaches as the primary intervention modality (See definitions in Appendix B); (d) sample size of more than 15 participants per experimental or control group to ensure adequate statistical power and reduce the risk of bias; (e) publication in peer-reviewed journals; and (f) written in English to ensure language consistency and facilitate access to a broad and internationally recognized body of scholarly work. Studies were excluded if they: (a) did not report quantitative results; or (b) focused on parents rather than children and adolescents.
2.3. Data Synthesis and Analysis
Information from each identified study was synthesized based on study background, participant characteristics, research aims or hypotheses, intervention details, outcomes, and significance of outcome variables. Data were extracted manually without the guidance of formal guidelines. Two independent reviewers conducted data extraction and cross-checking to ensure accuracy, and regular meetings were held to discuss study progress and emerging findings.
2.4. Assessment of Methodological Rigor
To assess methodological rigor, two separate rating scales were employed. The first was the Cochrane Risk of Bias tool (ROB 2.0) [44], and the second was the Delphi List [45], supplemented with four additional self-designed items. In this review, the score of methodological rigor will not be considered as an inclusion criterion. To ensure inter-rater reliability, two independent reviewers conducted the rating process using both scales.
2.4.1. Cochrane Risk of Bias Tool (ROB 2.0)
The ROB 2.0 tool is a widely recognized instrument designed to assist reviewers in assessing the risk of bias in RCTs due to methodological shortcomings. It includes 22 structured items grouped into five domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in outcome measurement, and (5) bias in the selection of the reported result. Each item is evaluated using one of five response options: Yes, Probably yes, Probably no, No, or No information. Based on these responses, each domain is rated as having a low risk, some concerns, or high risk of bias. A low-risk rating indicates strong confidence that the study results are unlikely to be affected by bias. A rating of some concerns reflects uncertainty regarding the validity of the findings due to potential methodological limitations. A high-risk rating suggests serious methodological flaws in at least one domain, which are likely to substantially compromise the credibility of the study outcomes [44].
2.4.2. Delphi List with Four Additional Items
To complement the ROB 2.0 tool, the Delphi List [45] was also employed to assess the methodological quality of the included studies. The Delphi List is a widely accepted instrument for appraising the quality of RCTs and consists of nine items. The assessed criteria include: (1) reporting of randomization, (2) allocation concealment, (3) baseline comparability, (4) specification of eligibility criteria, (5) blinding of participants, (6) blinding of service providers, (7) blinding of outcome assessors, (8) reporting of point estimates and measures of variability, and (9) use of intention-to-treat analysis [45]. To enhance the comprehensiveness of the quality assessment, four additional items were incorporated to reflect contemporary methodological standards, based on the Consolidated Standards of Reporting Trials (CONSORT) guidelines [46]. The assessed criteria include: (10) Sample size justification and power calculation, (11) Follow-up sufficiency and reporting, (12) Trial registration, (13) Statistical appropriateness. The complete list of quality assessment items is presented in Appendix C. Overall, the 13 items encompass four key domains of methodological quality: (i) research design (item 1, 2, 3, 5, 6, 7, 9), (ii) participant recruitment (item 4, 10), (iii) intervention protocol and follow-up (item 11, 12), and (iv) statistical appropriateness and outcome reporting (item 8, 13).
The 13 items was evaluated using a dichotomous scoring system (Yes = 1; No/Unclear = 0), resulting in a maximum possible score of 13 points. Higher total scores indicated greater methodological quality. As the Delphi List does not specify a cut-off score, tertile-based classification was applied to align with the three-level evaluation framework of the ROB 2.0 tool. Specifically, scores above 8 (i.e., >66.6% of the maximum) were categorized as high methodological quality; scores between 5 and 8 were considered moderate quality; and scores below 5 (i.e., <33.3% of the maximum) were classified as low quality.
3. Results
As shown in the PRISMA flow diagram (Figure 2), the initial search yielded a total of 851 articles across eight electronic databases. Both reviewers conducted an initial screening based on titles and abstracts, removing duplicates and ineligible records. Following this screening, 43 articles remained for full-text review. Additionally, four systematic reviews were screened to supplement the search [13,14,15,16], resulting in four additional articles being included. After a thorough full-text review, 12 articles were selected, which were published between 2017 and 2024 and encompassed a total of 899 participants aged 5 to 11 years diagnosed with ASD (see Table 1).
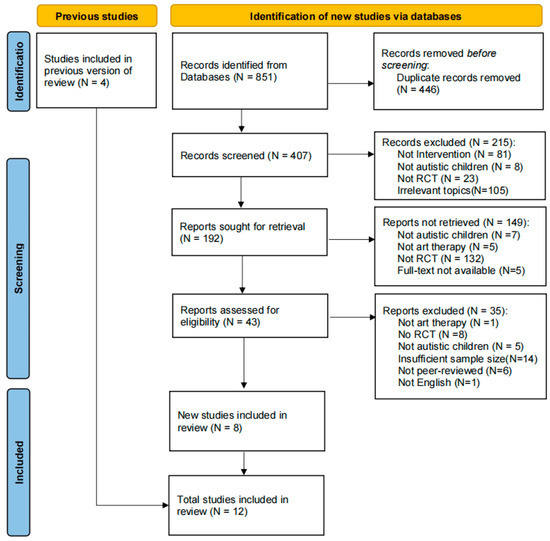
Figure 2.
Flow diagram for systematic reviews which included searches of databases.

Table 1.
Characteristics of included studies.
The studies demonstrated broad international representation: three were conducted in China [49,50,53], two in the United States [48,52], and two in Iran [56,57]. Additional studies were conducted in Iraq [51], France [55], and Canada [58]. Two studies included participants from multiple countries [47,54].
3.1. Effectiveness of Art Therapy
Overall ASD Symptoms. Among the 12 studies included in this review, three evaluated changes in overall ASD symptoms [50,53,55]. These studies assessed all core domains of ASD, including impairments in social communication and interaction, repetitive behaviors, and atypical sensory processing. Standardized assessment tools were employed, such as the Autism Diagnostic Observation Schedule [59], the Autism Behavior Checklist [60], the Childhood Autism Rating Scale [61], and the Clinical Global Impression scale [62]. All three studies reported a statistically significant reduction in overall ASD symptom scores among participants in the experimental groups compared to those in the control groups.
Social communication and social interaction. Among the 12 studies reviewed, seven reported outcomes related to social communication and interaction [47,48,52,53,54,56,58]. These outcomes were assessed using standardized instruments, including the Social Responsiveness Scale [63], Peer Interaction Paradigm [64], Matson Social Skills Questionnaire [65], and the Children’s Communication Checklist—Second Edition [66]. Of the seven studies, five reported statistically significant improvements in social communication and interaction following arts-based interventions in the experimental groups [48,52,53,56,58], while two studies observed improvements that were not statistically significant [47,54]. Collectively, these findings suggest that arts-based interventions may positively influence social communication skills in children and adolescents with ASD.
Psychological outcomes. Among the 12 studies reviewed, two reported psychological outcomes [49,52], specifically stress-related symptoms such as perceived pressure [49] and anxiety [52]. Ding [49] found significant reductions in perceived pressure following art therapy. Ioannou et al. [52] observed notable improvements in trait anxiety—defined as a general tendency to experience anxiety—over time. However, no significant changes were reported in state anxiety, which refers to anxiety triggered by specific situational stressors [67]. Overall, these findings suggest that art therapy may be effective in alleviating general stress-related symptoms in children and adolescents with ASD.
Behavioral outcomes. Of the 12 studies reviewed, two reported behavioral outcomes, specifically sleep habits and maladaptive behaviors [49,58]. These outcomes were assessed using the Children’s Sleep Habits Questionnaire [68] and the Maladaptive Behavior Subscale of the Vineland Adaptive Behavior Scales [69]. Ding [49] reported significant improvements in sleep habits following art therapy, whereas Sharda et al. [58] found no significant changes in maladaptive behaviors. Overall, the evidence regarding the effectiveness of art therapy in improving behavioral outcomes remains limited and warrants further investigation.
Other outcomes. Other outcomes reported in the reviewed studies included motor skills [51,57], neurologically related development [53,58], and language ability [47,53,58]. Two studies evaluated motor skills [51,57], both utilizing the Lincoln–Oseretsky Motor Development Scale [70]. Imankhah et al. [51] reported significant improvements in overall motor skills, and Sabet and Abadi [57] observed notable enhancements in fine motor skills, balance, and physical flexibility. These findings suggest that arts-based therapies may be effective in enhancing motor functioning in children and adolescents with ASD.
Two studies assessed neurologically related development [53,58]. Liu et al. [53] reported that participants in the experimental group demonstrated significantly greater improvements in neural development scores, as measured by the Gesell Developmental Schedules [71]. Similarly, Sharda et al. [58] observed significant enhancements in functional brain connectivity using resting-state functional magnetic resonance imaging (rs-fMRI). These findings provide preliminary evidence that art therapy may promote positive neurological development in children and adolescents with ASD.
Three studies assessed language-related outcomes [48,53,58]. Sharda et al. [58] found no significant changes in receptive vocabulary, as measured by the Peabody Picture Vocabulary Test, Fourth Edition [72]. In contrast, Corbett et al. [48] reported significant improvements in verbal ability, assessed using the Theory of Mind–Verbal Interactions test. Similarly, Liu et al. [53] observed improvements in language ability, measured by the Psycho-Educational Profile, Third Edition [73].
3.2. Intervention Format
Arts modalities. The reviewed studies employed various arts modalities as intervention approaches, including music, drama, painting, and multimodal arts. Among the 12 studies, six utilized music-based interventions [47,50,53,54,55,58].
Of these, five incorporated improvised activities such as singing, dancing, playing musical instruments, joint musical engagement with a therapist (e.g., singing or instrumental play), improvisational performance, instrument selection, personalized music listening sessions, and both instrumental and vocal improvisation [47,50,54,55,58]. One study applied the TOMATIS method, which targets neurosensory stimulation through auditory training [53].
Four studies employed drama-based interventions [48,49,52,56]. These interventions included theater games, role-playing exercises, protagonist character development, puppet shows, small group activities, and live performances [48,49,52,56].
Additionally, one study utilized an intermodal arts approach, combining music with body movement [51]. Another study implemented a visual arts-based intervention, incorporating activities such as painting, paper tearing, pottery, and handicraft making [57].
In terms of modality-specific effectiveness, music therapy demonstrated efficacy in improving core ASD symptoms [50,53,55], as well as outcomes related to social communication and interaction, language ability, and neurological development [53,58]. Drama therapy was effective in enhancing social communication and interaction [48,52,56], reducing anxiety [48,49,52], improving behavioral regulation [50], and supporting language development [48]. The single study employing painting therapy reported improvements in fine motor skills, balance, and flexibility [57]. Additionally, the study utilizing a mixed-modality approach combining music therapy with dance and movement also demonstrated effectiveness in enhancing motor skills [51].
Group versus one-on-one format. Six studies employed a group-based intervention format [48,49,51,52,55,56], including four that utilized drama therapy [48,49,52,56], one used music therapy [55], and one that combined music therapy with dance and movement [51]. Six studies adopted an individual (one-on-one) format [47,50,53,54,57,58], comprising five that implemented music therapy [47,50,53,54,58] and one that used painting therapy [57].
Overall, individual therapy was more frequently applied in music-based interventions. Group therapy was predominantly used in drama-based interventions.
Duration and frequency. The majority of the reviewed studies (N = 8) had intervention durations of three months or less [48,49,50,51,52,56,57,58], while interventions were conducted once a week [48,52,55,56,58], twice a week [51], or three or more times per week [53,54].
3.3. Theoretical Underpinnings Guiding Intervention
Among the 12 reviewed studies, five explicitly referenced theoretical frameworks [48,49,50,53,58], while seven did not discuss their theoretical underpinnings [47,51,52,54,55,56,57]. Sharda et al. [58] employed a reward-based cortical modulation and sensorimotor integration framework to guide the design of music therapy. Two studies cited auditory integration theory [50,53] as the basis for music therapy interventions. Social learning theory [48] and analytical psychology [49] were used to offer grounding for drama therapy.
3.4. Methodological Rigor
The Cohen’s kappa value for the assessment of methodological rigor was 0.803, indicating a high level of inter-rater reliability.
3.4.1. Risk of Bias
Risk of bias was assessed for all included studies using the ROB 2.0 tool (see Figure 3). Of the 12 studies reviewed, only one employed an intention-to-treat (ITT) analysis [47], which includes all participants as originally allocated after randomization, regardless of adherence to the intervention protocol. The remaining 11 studies utilized per-protocol (PP) analysis, which includes only participants who completed the study in accordance with the protocol [74]. The study that used ITT was rated as having “some concerns” [47]. Among the 11 studies that employed PP analysis, eight were assessed as having a high overall risk of bias [48,49,51,52,53,54,56,57], two studies were rated as having “some concerns [50,55]” and one study was rated as having a “low risk of bias [58]”. Overall, the included studies exhibited a relatively high risk of bias, highlighting the need for cautious interpretation of their findings within the context of this systematic review.
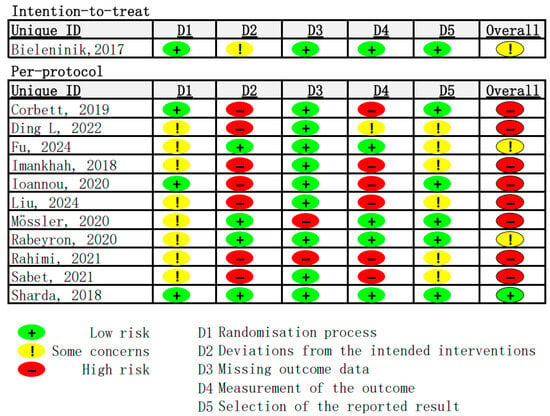
Figure 3.
Results of risk of bias assessment (N = 12) [47,48,49,50,51,52,53,54,55,56,57,58].
3.4.2. Methodological Quality
The methodological quality of the included studies was assessed using a 13-item checklist comprising the Delphi List [45], supplemented with four additional items (see Appendix C). The mean quality score was 5.92 (SD = 2.72), with a median score of 7, out of a maximum possible score of 13. Based on the predefined cut-off criteria, two studies scored above the 66.6th percentile (≥9), indicating high methodological quality. Six studies scored between 5 and 8, representing moderate quality, while four studies fell within the lowest 33.3rd percentile (≤4), indicating low methodological quality (see Appendix D).
(i) Research design. All the studies included were RCTs. Allocation concealment during the randomization process was reported in five studies [47,48,52,54,58], typically involving third-party procedures, while the remaining seven did not provide sufficient information regarding this aspect. Baseline comparability was confirmed in seven studies [47,48,50,52,53,54,58], supporting the validity of the randomization process; however, five studies did not report baseline equivalence. Regarding blinding procedures, two studies reported that participants were blinded to group allocation [50,55]. None of the studies reported blinding of intervention providers, and four studies indicated that outcome assessors were blinded [47,50,54,58].
(ii) Participants recruitment. Most of the included studies (N = 11) clearly defined and operationalized eligibility criteria for participation in the intervention. However, in terms of sample size, 11 studies recruited participants that were fewer than the recommended minimum of 64 per group, except for Bieleninik et al. (2017) [47]. Furthermore, only two studies reported a formal sample size justification [50,55].
(iii) Intervention protocol and follow-up. Regarding intervention protocols, six studies reported clinical trial registration [47,48,52,54,55,58], while the remaining studies did not provide any information on this aspect. In terms of follow-up procedures, only three studies conducted follow-up assessments and reported corresponding results [47,54,56].
(iv) Statistical appropriateness and outcome reporting. In terms of statistical analysis, four studies utilized statistically inappropriate approaches, such as independent t-tests and one-way ANCOVA [49,51,53,57]. Most of the included studies (N = 10) reported outcome variability, typically presenting results with means and standard deviations. Two studies did not report these descriptive statistics [49,53].
4. Discussion
This study evaluated the effectiveness of art therapy for children and adolescents with ASD and reviewed the implementation strategies and methodological quality of existing intervention studies. A total of 12 RCTs were included, encompassing various forms of art therapy: music therapy (N = 6), drama therapy (N = 4), painting therapy (N = 1), and therapy using mixed modalities (N = 1). All studies included at least 15 participants per group. The findings of this systematic review suggest that art therapy shows promise in reducing overall ASD symptoms and stress-related psychological outcomes, as well as in enhancing social communication, motor skills, language ability, and neurodevelopmental functioning in children with ASD. However, the review also identified a generally high risk of bias and low methodological rigor among the included studies.
A key contribution of this study is that, among existing reviews on the effectiveness of art therapy for children and adolescents with ASD, it is the first systematic review to include only RCTs with adequate sample sizes, thereby providing more reliable and generalizable findings. In addition, the study offers a thorough and systematic evaluation of the methodological rigor of current RCTs, including assessment of risk of bias, intervention dosage, follow-up procedures, and statistical analyses, and highlights important directions for future research.
4.1. Effectiveness of Art Therapy for Children and Adolescents with ASD
Regarding outcome variables, this review found that social communication and interaction was the most frequently reported outcome among the included studies [47,48,52,53,54,56,58]. Other commonly reported outcomes included overall ASD symptoms [50,53,55], language ability [48,53,58], stress-related psychological outcomes [50,61] and behavioral outcomes [49,58], motor skills [51,57], and neurologically related development [53,58].
In terms of the effectiveness of art therapy for children and adolescents with ASD, results of this systematic review revealed that, among the studies reporting the outcomes above, more than half demonstrated significant improvements in social communication and interaction (5 out of 7, 5/7), overall ASD symptoms(3/3), anxiety/stress reduction (2/2), motor skills (2/2), language ability (2/3), and neurologically related development (2/2), suggesting a positive effect of art therapy in these domains. However, evidence regarding behavioral outcomes—including sleep habits (1/1) and maladaptive behaviors (0/1)—remains inconclusive.
The current findings align with several previous reviews on the effectiveness of art therapy for individuals with ASD. For example, Bololia et al. [14] reported that dramatherapy can foster social skills and promote emotional well-being, and Vogel et al. [16] observed improvements in both social and motor skills. Notably, although there are some consistent findings across certain variables, the number of RCTs examining these outcomes remains relatively small, and the positive results may, in part, be influenced by publication bias. Therefore, more empirical studies are needed to further verify the effectiveness of art therapy.
4.2. Theoretical Frameworks Have Guided the Design of Art Therapy
Among the 12 reviewed studies, only five explicitly referenced theoretical frameworks [48,49,50,53,58]. Of these five studies, three were music therapy interventions, all of which mentioned auditory integration theory as their theoretical basis [50,53,58]. The remaining two studies were drama therapy, which drew on social learning theory [48] and analytical psychology [49] to provide a theoretical foundation for their interventions.
These results reveal a trend toward using auditory integration theory to explain the effects of music therapy, with intervention designs emphasizing sensory processing and auditory experience. In addition, this result also shows that intervention designs based on behavioral theory and psychoanalytic theory emphasize social learning and social participation, reinforcing the imitation of social behaviors and the development of mastery in social experiences. Analytical psychology offers a holistic approach that supports the integration of the unconscious and conscious self with the external world and releases emotional tension on an unconscious level within a safe therapeutic context.
However, it can also be observed that current studies lack emphasis on humanistic and positive psychology theories, even though art therapy inherently highlights client-centered and strength-based practice. Based on this, we propose incorporating SDT into the theoretical frameworks of future studies. The arts-based therapies reviewed in this study draw upon various theoretical frameworks aligned with SDT [25,26,27,28], for example, creating a therapeutic environment that encouraged participants to explore personal preferences and share personal experiences to connect their inner world with the external world through artwork [53]. This approach supports the SDT principles of autonomy and relatedness. Similarly, drama therapy promotes interpersonal connection and competence development through peer interaction and performance-based activities. These elements resonate with SDT’s emphasis on intrinsic motivation and psychological growth. By engaging participants in expressive modalities that affirm their agency and sense of social belonging, these therapies exemplify how SDT can be applied within creative mental health interventions.
Furthermore, this result also reveals a considerable inconsistency in the theoretical foundations of current art therapy research. Since most studies (7/12) did not explain the theoretical basis of their intervention design, we strongly recommend that future research pay greater attention to this aspect.
4.3. Intervention Formats of Art Therapy for Children and Adolescents with ASD
Regarding the format and modality of interventions, music therapy (N = 6) and drama therapy (N = 4) were the most frequently employed approaches. Music-based interventions incorporated improvised activities such as singing, dancing, playing musical instruments, joint musical engagement with a therapist, improvisational performance, and personalized music listening sessions. In contrast, drama-based interventions included components such as role-playing, rehearsals, and performance, which offer specific therapeutic benefits by actively engaging participants in social scenarios. An interesting finding of this study is that music therapy reported more benefits for overall ASD symptoms [50,55], while drama therapy showed promising effects on social skills [48,52,56]. Although this study cannot examine this in depth, considering the differences in activities and theoretical foundations, it is worthwhile to explore whether music therapy and drama therapy benefit individuals with ASD in different aspects.
Six studies utilized individual interventions, while six implemented group-based formats. Individual therapy was more frequently applied in music-based interventions, whereas group therapy was predominantly used in drama-based interventions.
The majority of the reviewed studies had intervention durations of less than three months (N = 8), and majority of sessions were conducted two or less a week (N = 6). Compared with the recommendations of Brentani et al. [9], which suggest intensive treatment—five days a week for a minimum of five hours per day, the interventions included in the current review appear to be low in dosage.
4.4. Methodological Rigor of Existing Art Therapy Studies for Children and Adolescents with ASD
Across the reviewed studies, a high risk of bias and generally low methodological rigor were identified. The results of ROB 2.0 show that most studies (N = 8) were rated as having a high overall risk of bias, suggesting serious flaws in study design. One major limitation is that, although all studies employed RCT designs, most relied on PP analyses rather than ITT approaches, introducing potential bias by excluding participants who deviated from the study protocol—PP analyses often exclude participants who drop out or deviate from the protocol, removing less favorable outcomes and potentially inflating treatment effects [74]. When combined with publication bias, which favors the reporting of positive results [75,76], the literature may overestimate the true effectiveness of art therapy. This convergence of biases highlights the need for future studies to employ ITT analyses and preregistered protocols to ensure more accurate and transparent evaluations of therapeutic outcomes [77].
Another major limitation was the inadequate sample size. The majority of the included studies (N = 8) enrolled between 15 and 30 participants per group, which falls below the recommended sample size of 64 per group for adequate statistical power, raising concerns about the increased risk of Type II errors. As a result, some studies might have failed to detect significant effects not because the interventions were ineffective, but rather due to insufficient statistical power.
Other limitations on methodology include the randomization process, blinding procedures, trial registration, and sample size calculations—were largely overlooked among the included studies. These limitations collectively reduce confidence in the reported findings and underscore the need for more rigorously designed trials in future research.
4.5. Implications for Research and Practice
This systematic review has several important implications for both future research and clinical practice regarding art therapy on ASD. First of all, while art therapy demonstrates potential as a complementary approach for promoting positive outcomes in children with ASD, the current evidence base is constrained by low methodological rigor. Many studies rely on small sample sizes, increasing the likelihood of Type II errors, and frequently employ PP analyses rather than ITT approaches, despite utilizing RCT designs. This review provides a strong emphasis on the necessity of robust methodological practices to enhance confidence in reported outcomes. Generating evidence-based insights is essential for the development and broader application of arts therapies for neurodiverse populations, thereby advancing the field of applied psychology through innovative and inclusive approaches.
Secondly, a promising direction for future research involves the integration of technology to more precisely measure therapeutic change. The present review found that most studies relied on self-report measures. Due to the client-centered and improvisational nature of art therapy and the specific characteristics of the ASD population, conducting large-scale quantitative studies may be challenging. One possible direction is to understand neural changes during art therapy. Notably, we identified one study that employed neuroimaging techniques and demonstrated enhanced brain connectivity following music therapy [58]. Future research could further explore the potential impact of art therapy on brain development.
Thirdly, to establish best practices, further implementation studies are needed to identify components that may influence the effectiveness of art therapy—such as optimal session frequency, modality selection, therapeutic settings, and ASD severity. Future research could also investigate hypothesized process variables grounded in SDT [26,27], including autonomy, relatedness, and competence.
From a practical standpoint, practitioners are encouraged to design intervention sessions informed by theoretical frameworks and structured formats, incorporating diverse art modalities and considering the appropriateness of group versus individual settings. Given the unique challenges associated with working with neurodiverse children, facilitators must remain attuned to their individual needs and preferences. Rather than viewing these children through a deficit-based lens, a more constructive approach involves creating autonomous, creative, and enjoyable environments—such as those offered by art therapy—that affirm their identities and foster meaningful engagement.
4.6. Limitations
The findings of this study should be interpreted in light of several limitations. First, only 12 studies met the inclusion criteria, which limits the available evidence regarding the effectiveness of art therapy in improving various outcomes.
Second, due to the limited number of studies and difficulties in obtaining datasets, despite efforts to contact authors, the available data were ultimately insufficient to conduct a convinced meta-analysis (only 4 studies for social communication outcomes and 3 for overall ASD symptoms). Consequently, the conclusions of this review are based on qualitative synthesis and cannot indicate statistical significance and may be influenced by the researchers’ training and interpretive stance.
Third, the exclusion of non-English publications may have inadvertently omitted relevant research, limiting the representativeness and cultural diversity of the findings. Furthermore, the exclusion of interventions targeting caregivers limited the review’s ability to assess the effectiveness of family-involved interventions, which may represent an important component of therapy [9].
Fourth, during the article screening process, reviewers conducted initial screening at each stage and resolved discrepancies through discussion. Therefore, inter-rater reliability for the entire screening process is not available. Future research could implement independent screening procedures and report inter-rater reliability to enhance methodological rigor and ensure objectivity.
5. Conclusions
This systematic review synthesized evidence from 12 RCTs to evaluate the effectiveness of art therapy for children and adolescents with ASD. The findings indicate that art therapy, particularly music and drama therapy, can enhance social communication, language ability, motor skills, and neurodevelopment, while also reducing stress-related symptoms and overall ASD severity. However, most studies demonstrated small sample sizes, brief intervention durations, and low methodological rigor, limiting the generalizability of current evidence. Only a few studies reported theoretical underpinnings, revealing a lack of consistent frameworks to guide intervention design. Future research should prioritize methodological improvements, such as larger sample sizes, trial registration, intention-to-treat analyses, and longitudinal follow-ups, to strengthen the evidence base. Moreover, incorporating theoretical perspectives like SDT could better explain the mechanisms of change and emphasize autonomy, competence, and relatedness within creative interventions. Overall, art therapy represents a promising, person-centered, and holistic approach for supporting the developmental and psychological needs of children and adolescents with ASD, but further rigorously designed studies are required to establish its efficacy and inform evidence-based practice.
Author Contributions
Conceptualization: S.W., A.H.Y.L. and H.W.H.H.; Writing—original draft preparation: S.W. and A.H.Y.L.; Writing—review and editing: A.H.Y.L.; Methodology, software, and data analysis: S.W.; Data collection and evaluation: S.W. and H.W.H.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. This review was registered on the Open Science Framework (OSF). Registration DOI: https://doi.org/10.17605/OSF.IO/XAG58 (accessed on 1 November 2025).
Acknowledgments
Gratitude is extended to all researchers whose studies were included in this systematic review.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Search Terms
(“expressive arts therapy” OR “expressive art therapy” OR “creative arts therapy” OR “multimedia arts therapy” OR “multimedia art therapy” OR “music therapy” OR “drama therapy” OR “dance therapy” OR “dance and movement therapy” OR “behavioral music therapy” OR “art therapy” OR “arts therapy” OR “theater education” OR “drama education” OR “visual art therapy” OR “visual arts therapy” OR “fine art therapy” OR “fine arts therapy”)
AND
(“intervention” OR “reduction” OR “management” OR “managing” OR “coping” OR “program” OR “programme” OR “training” OR “skills” OR “techniques” OR “counseling” OR “development” OR “modification” OR “modifying” OR “treatment”)
AND
(“autistic children” OR “autism” OR “ASD” OR “Autistic Spectrum Disorder” OR “autistic student” OR “developmental disorder” OR “autism spectrum disorder” OR “Asperger”)
AND
(“RCT” OR “randomized control trial” OR “randomized controlled trial” OR “randomized clinical trial” OR “randomised control trial” OR “randomised clinical trial” OR “randomised controlled trial”) [Abstract]
NOT
(protocol OR pilot) [Title]
AND
(filtered by peer-reviewed journal, human, English)
Appendix B. Definitions of Different Types of Art Therapy
Table A1.
Definitions of Different Types of Art Therapy.
Table A1.
Definitions of Different Types of Art Therapy.
| Terms | Definition |
|---|---|
| Art therapy | Art therapy is a holistic therapeutic approach that integrates principles from mental health, human development, and psychological theory with various art modalities—such as visual art, music, movement, drama, and creative writing—to promote individual and community well-being [18]. |
| Visual art therapy | Visual art therapy is defined as a “therapeutic process based on spontaneous or prompted creative expression using various art materials and art techniques such as painting, drawing, sculpture, clay modeling and collage” [78]. |
| Music therapy | Music Therapy is the clinical & evidence-based use of music interventions to accomplish individualized goals within a therapeutic relationship by a credentialed professional who has completed an approved music therapy program [79]. |
| Dance/movement therapy | The psychotherapeutic use of dance, movement, body awareness, and embodied communication to foster healing and well-being for all individuals, families, and communities [80]. |
| Drama therapy | Drama therapy is one form of art therapy, which utilizes methods and techniques from the performing arts with principles of psychotherapy that promote transformation and evolution. Drama therapists employ a range of artistic techniques through methods such as storytelling, Greek myths, play scripts, puppetry, masks, and improvisation [81]. |
| Poetry/writing therapy | Poetry therapy is the use of language, symbol, and story in therapeutic, educational, growth, and community-building capacities. It relies upon the use of poems, stories, song lyrics, imagery, and metaphor to facilitate personal growth, healing, and greater self-awareness. Bibliotherapy, narrative, journal writing, metaphor, storytelling, and ritual are all within the realm of poetry therapy [82]. |
| Intermodal or Multimodal approaches | Intermodal expressive arts therapy involves the intentional use and integration of multiple artistic modalities within a therapeutic or growth-oriented process. These modalities may include visual arts (such as painting, photography, and crafts), movement and dance, voice, rhythm, sound, and music, as well as drama, enactment, and various forms of writing including poetry and storytelling. Additionally, intermodal practice may incorporate guided meditation, imaginative processes, and nature-based activities to facilitate self-expression, healing, and transformation [83]. |
Appendix C. List of Quality Rating Items
Table A2.
List of Quality Rating Items (The Delphi List and 4 Additional Items).
Table A2.
List of Quality Rating Items (The Delphi List and 4 Additional Items).
| Items | Yes | No | Don’t Know |
|---|---|---|---|
| 1. Was a method of randomization performed? | □ | □ | □ |
| 2. Was the treatment allocation concealed? | □ | □ | □ |
| 3. Were the groups similar at baseline regarding the most important prognostic indicators? | □ | □ | □ |
| 4. Were the eligibility criteria specified? | □ | □ | □ |
| 5. Was the outcome assessor blinded? | □ | □ | □ |
| 6. Was the care provider blinded? | □ | □ | □ |
| 7. Was the clients blinded? | □ | □ | □ |
| 8. Were point estimates and measures of variability presented for the primary outcome measures? | □ | □ | □ |
| 9. Did the analysis include an intention-to-treat analysis? | □ | □ | □ |
| 10. Was a sample size justification or power calculation provided? | □ | □ | □ |
| 11. Was the follow-up period sufficiently long (i.e., >3 months) and adequately reported? | □ | □ | □ |
| 12. Was the trial registered? | □ | □ | □ |
| 13. Were the statistical analysis methods clearly described, justified, and appropriate? | □ | □ | □ |
Appendix D. The Results of Quality Rating Scale
Table A3.
The Results of Quality Rating Scale (The Delphi List and 4 Additional Items).
Table A3.
The Results of Quality Rating Scale (The Delphi List and 4 Additional Items).
| (i) Research Design | (ii) Participants Recruitment | (iii) Intervention Protocol and Follow-Up | (iv) Statistical Appropriateness and Outcome Reporting | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 5 | Item 6 | Item 7 | Item 9 | Item 4 | Item 10 | Item 11 | Item 12 | Item 8 | Item 13 | |||
| No. | Study | Randomization Reported | Allocation Concealment | Baseline Comparability | Participants Blinding | Providers Blinding | Assessors Blinding | ITT Analysis | Eligibility Criteria | Sample Size Justification | Follow-Up Reported | Trial Registration | Variability Reported | Statistical Appropriateness | |
| 1 | Bieleninik, 2017 [47] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 |
| 2 | Corbett, 2019 [48] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 7 |
| 3 | Ding, 2022 [49] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 4 | Fu, 2024 [50] | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 8 |
| 5 | Imankhah, 2018 [51] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 3 |
| 6 | Ioannou, 2020 [52] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 7 |
| 7 | Liu, 2024 [53] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 3 |
| 8 | Mössler, 2020 [54] | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 9 |
| 9 | Rabeyron, 2020 [55] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| 10 | Rahimi, 2021 [56] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 5 |
| 11 | Sabet, 2021 [57] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 3 |
| 12 | Sharda, 2018 [58] | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 8 |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Hirota, T.; King, B.H. Autism Spectrum Disorder. JAMA 2023, 329, 157. [Google Scholar] [CrossRef]
- Salari, N.; Rasoulpoor, S.; Rasoulpoor, S.; Shohaimi, S.; Jafarpour, S.; Abdoli, N.; Khaledi-Paveh, B.; Mohammadi, M. The global prevalence of autism spectrum disorder: A comprehensive systematic review and meta-analysis. Ital. J. Pediatr. 2022, 48, 112. [Google Scholar] [CrossRef]
- Talantseva, O.I.; Romanova, R.S.; Shurdova, E.M.; Dolgorukova, T.A.; Sologub, P.S.; Titova, O.S.; Kleeva, D.F.; Grigorenko, E.L. The global prevalence of autism spectrum disorder: A three-level meta-analysis. Front. Psychiatry 2023, 14, 1071181. [Google Scholar] [CrossRef]
- Di Blasi, F.D.; Costanzo, A.A.; Finocchiaro, M.; Stimoli, M.A.; Zuccarello, R.; Buono, S.; Ferri, R.; Zoccolotti, P. Academic Skills in Students with Autism Spectrum Disorder and Intellectual Disability: A Systematic Review and Meta-Analysis. Educ. Sci. 2023, 13, 1026. [Google Scholar] [CrossRef]
- Rowley, E.; Chandler, S.; Baird, G.; Simonoff, E.; Pickles, A.; Loucas, T.; Charman, T. The experience of friendship, victimization and bullying in children with an autism spectrum disorder: Associations with child characteristics and school placement. Res. Autism Spectr. Disord. 2012, 6, 1126–1134. [Google Scholar] [CrossRef]
- Ghanouni, P.; Quirke, S.; Blok, J.; Casey, A. Independent living in adults with autism spectrum disorder: Stakeholders’ perspectives and experiences. Res. Dev. Disabil. 2021, 119, 104085. [Google Scholar] [CrossRef]
- Ault, S.; Breitenstein, S.M.; Tucker, S.; Havercamp, S.M.; Ford, J.L. Caregivers of Children with Autism Spectrum Disorder in Rural Areas: A Literature Review of Mental Health and Social Support. J. Pediatr. Nurs. 2021, 61, 229–239. [Google Scholar] [CrossRef]
- Brentani, H.; de Paula, C.S.; Bordini, D.; Rolim, D.; Sato, F.; Portolese, J.; Pacifico, M.C.; McCracken, J.T. Autism spectrum disorders: An overview on diagnosis and treatment. Rev. Bras. Psiquiatr. 2013, 35, S62–S72. [Google Scholar] [CrossRef]
- Sandoval-Norton, A.H.; Shkedy, G.; Shkedy, D. How much compliance is too much compliance: Is long-term ABA therapy abuse? Cogent Psychol. 2019, 6, 1641258. [Google Scholar] [CrossRef]
- Bellini, S.; Peters, J.K.; Benner, L.; Hopf, A. A Meta-Analysis of School-Based Social Skills Interventions for Children With Autism Spectrum Disorders. Remedial Spec. Educ. 2007, 28, 153–162. [Google Scholar] [CrossRef]
- Sandbank, M.; Bottema-Beutel, K.; Crowley LaPoint, S.; Feldman, J.I.; Barrett, D.J.; Caldwell, N.; Dunham, K.; Crank, J.; Albarran, S.; Woynaroski, T. Autism intervention meta-analysis of early childhood studies (Project AIM): Updated systematic review and secondary analysis. BMJ 2023, 383, e076733. [Google Scholar] [CrossRef]
- Bernier, A.; Ratcliff, K.; Hilton, C.; Fingerhut, P.; Li, C.-Y. Art Interventions for Children With Autism Spectrum Disorder: A Scoping Review. Am. J. Occup. Ther. 2022, 76, 7605205030. [Google Scholar] [CrossRef]
- Bololia, L.; Williams, J.; Macmahon, K.; Goodall, K. Dramatherapy for children and adolescents with autism spectrum disorder: A systematic integrative review. Arts Psychother. 2022, 80, 101918. [Google Scholar] [CrossRef]
- López-Escribano, C.; Orío-Aparicio, C. Creative arts therapy for autistic children: A systematic review. Arts Psychother. 2024, 91, 102224. [Google Scholar] [CrossRef]
- Vogel, S.W.; Mullins, K.L.; Kumar, S. Art therapy for children and adolescents with autism: A systematic review. Int. J. Art. Ther. 2025, 30, 113–122. [Google Scholar] [CrossRef]
- Rogers, N. The Creative Connection: Expressive Arts as Healing; Science & Behavior Books: Mountain View, CA, USA, 1993. [Google Scholar]
- Malchiodi, C.A. Expressive arts therapy and multimodal approaches. In Handbook of Art Therapy, 6th ed.; Guilford Press: New York, NY, USA, 2003; pp. 106–119. [Google Scholar]
- Versitano, S.; Tesson, S.; Lee, C.-W.; Linnell, S.; Perkes, I. Art therapy with children and adolescents experiencing acute or severe mental health conditions: A systematic review. Aust. N. Z. J. Psychiatry 2025, 59, 863–887. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, C.; Knorth, E.J.; Spreen, M. Art therapy with children with Autism Spectrum Disorders: A review of clinical case descriptions on ‘what works’. Arts Psychother. 2014, 41, 577–593. [Google Scholar] [CrossRef]
- Ke, X.; Song, W.; Yang, M.; Li, J.; Liu, W. Effectiveness of music therapy in children with autism spectrum disorder: A systematic review and meta-analysis. Front. Psychiatry 2022, 13, 905113. [Google Scholar] [CrossRef]
- Isserow, J. Looking together: Joint attention in art therapy. Int. J. Art. Ther. 2008, 13, 34–42. [Google Scholar] [CrossRef]
- Ho, R.; Chiu, W.C. Joint Painting for Understanding the Development of Emotional Regulation and Adjustment Between Mother and Son in Expressive Arts Therapy. In Arts-Based Research, Resilience and Well-Being Across the Lifespan; Springer International Publishing: Cham, Switzerland, 2020; pp. 127–146. [Google Scholar]
- Van Lith, T. Art therapy in mental health: A systematic review of approaches and practices. Arts Psychother. 2016, 47, 9–22. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L.; Grolnick, W.S.; La Guardia, J.G. The Significance of Autonomy and Autonomy Support in Psychological Development and Psychopathology. In Developmental Psychopathology; Wiley: Hoboken, NJ, USA, 2015; pp. 795–849. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Deci, E.L.; Ryan, R.M. The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Roth, G.; Vansteenkiste, M.; Ryan, R.M. Integrative emotion regulation: Process and development from a self-determination theory perspective. Dev. Psychopathol. 2019, 31, 945–956. [Google Scholar] [CrossRef]
- Yu, C.; Li, X.; Wang, S.; Zhang, W. Teacher autonomy support reduces adolescent anxiety and depression: An 18-month longitudinal study. J. Adolesc. 2016, 49, 115–123. [Google Scholar] [CrossRef] [PubMed]
- López-Pérez, B.; Zuffianò, A. Children’s and Adolescents’ Happiness Conceptualizations at School and their Link with Autonomy Competence, and Relatedness. J. Happiness Stud. 2021, 22, 1141–1163. [Google Scholar] [CrossRef]
- Orkibi, H.; Ronen, T. Basic Psychological Needs Satisfaction Mediates the Association between Self-Control Skills and Subjective Well-Being. Front. Psychol. 2017, 8, 936. [Google Scholar] [CrossRef]
- Schweizer, C.; Spreen, M.; Knorth, E.J. Exploring What Works in Art Therapy With Children With Autism: Tacit Knowledge of Art Therapists. Art. Therapy 2017, 34, 183–191. [Google Scholar] [CrossRef]
- Pilkington, P.D.; Spicer, L.; Wilson, M. Schema therapists’ perceptions of the influence of their early maladaptive schemas on therapy. Psychother. Res. 2022, 32, 833–846. [Google Scholar] [CrossRef]
- Hartley, C.; Fisher, S. Do Children with Autism Spectrum Disorder Share Fairly and Reciprocally? J. Autism. Dev. Disord. 2018, 48, 2714–2726. [Google Scholar] [CrossRef]
- Epp, K.M. Outcome-Based Evaluation of a Social Skills Program Using Art Therapy and Group Therapy for Children on the Autism Spectrum. Child. Sch. 2008, 30, 27–36. [Google Scholar] [CrossRef]
- Vaisvaser, S. Moving Along and Beyond the Spectrum: Creative Group Therapy for Children With Autism. Front. Psychol. 2019, 10, 417. [Google Scholar] [CrossRef]
- Vogindroukas, I.; Stankova, M.; Chelas, E.-N.; Proedrou, A. Language and Speech Characteristics in Autism. Neuropsychiatr. Dis. Treat. Volume 2022, 18, 2367–2377. [Google Scholar] [CrossRef]
- Ben-Sasson, A.; Gal, E.; Fluss, R.; Katz-Zetler, N.; Cermak, S.A. Update of a Meta-analysis of Sensory Symptoms in ASD: A New Decade of Research. J. Autism Dev. Disord. 2019, 49, 4974–4996. [Google Scholar] [CrossRef] [PubMed]
- Sung, Y.-S.; Lin, C.-Y.; Chu, S.Y.; Lin, L.-Y. Emotion Dysregulation Mediates the Relationship Between Sensory Processing Behavior Problems in Young Children with Autism Spectrum Disorder: A Preliminary Study. J. Autism Dev. Disord. 2024, 54, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Jia, Z.; Huang, X.; Lui, S.; Kuang, W.; Sweeney, J.A.; Gong, Q. Brain structural abnormalities in emotional regulation and sensory processing regions associated with anxious depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 94, 109676. [Google Scholar] [CrossRef] [PubMed]
- Brindle, K.; Moulding, R.; Bakker, K.; Nedeljkovic, M. Is the relationship between sensory-processing sensitivity and negative affect mediated by emotional regulation? Aust. J. Psychol. 2015, 67, 214–221. [Google Scholar] [CrossRef]
- Gao, X.; Xu, G.; Fu, N.; Ben, Q.; Wang, L.; Bu, X. The effectiveness of music therapy in improving behavioral symptoms among children with autism spectrum disorders: A systematic review and meta-analysis. Front. Psychiatry 2025, 15, 1511920. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.W.; de Bie, R.A.; Kessels, A.G.H.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]
- Hopewell, S.; Chan, A.-W.; Collins, G.S.; Hróbjartsson, A.; Moher, D.; Schulz, K.F.; Tunn, R.; Aggarwal, R.; Berkwits, M.; Berlin, J.A.; et al. CONSORT 2025 statement: Updated guideline for reporting randomised trials. Lancet 2025, 405, 1633–1640. [Google Scholar] [CrossRef]
- Bieleninik, L.; Geretsegger, M.; Mössler, K.; Assmus, J.; Thompson, G.; Gattino, G.; Elefant, C.; Gottfried, T.; Igliozzi, R.; Muratori, F.; et al. Effects of Improvisational Music Therapy vs Enhanced Standard Care on Symptom Severity Among Children With Autism Spectrum Disorder. JAMA 2017, 318, 525. [Google Scholar] [CrossRef]
- Corbett, B.A.; Ioannou, S.; Key, A.P.; Coke, C.; Muscatello, R.; Vandekar, S.; Muse, I. Treatment Effects in Social Cognition and Behavior following a Theater-based Intervention for Youth with Autism. Dev. Neuropsychol. 2019, 44, 481–494. [Google Scholar] [CrossRef]
- Ding, L. Application of drama performance in intervention of children with autism spectrum disorders. Psychiatr Danub. 2022, 34, 909–913. [Google Scholar]
- Fu, Y.; Tian, M.; Chen, J.; Chen, W.; Li, H. Improvement of symptoms in children with autism by TOMATIS training: A cross-sectional and longitudinal study. Front. Behav. Neurosci. 2024, 18, 1357453. [Google Scholar] [CrossRef] [PubMed]
- Imankhah, F.; Hossein Khanzadeh, A.A.; Hasirchaman, A. The Effectiveness of Combined Music Therapy and Physical Activity on Motor Coordination in Children With Autism. Iran. Rehabil. J. 2018, 16, 405–412. [Google Scholar] [CrossRef]
- Ioannou, S.; Key, A.P.; Muscatello, R.A.; Klemencic, M.; Corbett, B.A. Peer Actors and Theater Techniques Play Pivotal Roles in Improving Social Play and Anxiety for Children With Autism. Front. Psychol. 2020, 11, 908. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, Q.; He, C.; Yao, C.; Ying, F. Effects of Auditory Integration Training Combined with Music Therapy on Children with Autism Spectrum Disorder; IOS Press Ebooks: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Mössler, K.; Schmid, W.; Aßmus, J.; Fusar-Poli, L.; Gold, C. Attunement in Music Therapy for Young Children with Autism: Revisiting Qualities of Relationship as Mechanisms of Change. J. Autism Dev. Disord. 2020, 50, 3921–3934. [Google Scholar] [CrossRef]
- Rabeyron, T.; Robledo del Canto, J.-P.; Carasco, E.; Bisson, V.; Bodeau, N.; Vrait, F.-X.; Berna, F.; Bonnot, O. A randomized controlled trial of 25 sessions comparing music therapy and music listening for children with autism spectrum disorder. Psychiatry Res. 2020, 293, 113377. [Google Scholar] [CrossRef]
- Pordanjani, S.R. Effectiveness of Drama Therapy on Social Skills of Autistic Children. Pract. Clin. Psychol. 2021, 9, 9–18. [Google Scholar] [CrossRef]
- Sabet, S.; Gholami, H.A.Z. The effect of art therapy on motor skills of children with autism. Int. J. Appl. Behav. Sci. 2021, 8, 27–34. [Google Scholar]
- Sharda, M.; Tuerk, C.; Chowdhury, R.; Jamey, K.; Foster, N.; Custo-Blanch, M.; Tan, M.; Nadig, A.; Hyde, K. Music improves social communication and auditory–motor connectivity in children with autism. Transl. Psychiatry 2018, 8, 231. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Goode, S.; Heemsbergen, J.; Jordan, H.; Mawhood, L.; Schopler, E. Autism Diagnostic Observation Schedule. In PsycTESTS Dataset; APA PsycNet: Washington, DC, USA, 2016. [Google Scholar]
- Krug, D.A.; Arick, J.; Almond, P. Behavior Checklist for Identifying Severely Handicapped Individuals with High Levels of Autistic Behavior. Child Psychol. Psychiatry 1980, 21, 221–229. [Google Scholar] [CrossRef]
- Schopler, E.; Reichler, R.J.; DeVellis, R.F.; Daly, K. Childhood Autism Rating Scale. In PsycTESTS Dataset; APA PsycNet: Washington, DC, USA, 2016. [Google Scholar]
- Kessler, M.; Petersen, G.; Vu, H.M.; Baudry, M.; Lynch, G. L-phenylalanyl-L-glutamate-stimulated, chloride-dependent glutamate binding represents glutamate sequestration mediated by an exchange system. J. Neurochem. 1987, 48, 1191–1200. [Google Scholar] [CrossRef]
- Constantino, J.N.; Davis, S.A.; Todd, R.D.; Schindler, M.K.; Gross, M.M.; Brophy, S.L.; Metzger, L.M.; Shoushtari, C.S.; Splinter, R.; Reich, W. Social Responsiveness Scale. In PsycTESTS Dataset; APA PsycNet: Washington, DC, USA, 2021. [Google Scholar]
- Corbett, B.A.; Schupp, C.W.; Simon, D.; Ryan, N.; Mendoza, S. Elevated cortisol during play is associated with age and social engagement in children with autism. Mol. Autism 2010, 1, 13. [Google Scholar] [CrossRef]
- Matson, J.L.; Rotatori, A.F.; Helsel, W.J. Development of a rating scale to measure social skills in children: The matson evaluation of social skills with youngsters (MESSY). Behav. Res. Ther. 1983, 21, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.V.M. The Children’s Communication Checklist—2; The Psychological Corporation: London, UK, 2003. [Google Scholar]
- Leal, P.C.; Goes, T.C.; da Silva, L.C.F.; Teixeira-Silva, F. Trait vs. state anxiety in different threatening situations. Trends Psychiatry Psychother 2017, 39, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Spirito, A.; McGuinn, M. The Children’s Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep 2000, 23, 1043–1051. [Google Scholar] [CrossRef]
- Sparrow, S.S. Vineland adaptive behavior scales. In Encyclopedia of Clinical Neuropsychology; Springer: New York, NY, USA, 2011; pp. 2618–2621. [Google Scholar]
- Sloan, W. The Lincoln-Oseretsky Motor Development Scale. Genet. Psychol. Monogr. 1955, 51, 183–252. [Google Scholar] [PubMed]
- Gesell, A. Developmental schedules. In The Mental Growth of the Pre-School Child: A Psychological Outline of Normal Development from Birth to the Sixth Year, Including a System of Developmental Diagnosis; MacMillan Co.: New York, NY, USA, 1925; pp. 362–375. [Google Scholar]
- Dunn, L.M.; Dunn, D.M. Peabody Picture Vocabulary Test, 4th ed.; (PPVT-4); Pearson: London, UK, 2007. [Google Scholar]
- Schopler, E.; Lansing, M.D.; Reichler, R.J.; Marcus, L.M. Psychoeducational Profile: PEP-3: TEACCH Individualized Psychoeducational Assessment for Children with Autism Spectrum Disorders; Pro-Ed: Austin, TX, USA, 2005. [Google Scholar]
- Gupta, S. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. Why Most Published Research Findings Are False. PLoS Med. 2005, 2, e124. [Google Scholar] [CrossRef]
- Song, F.; Parekh, S.; Hooper, L.; Loke, Y.; Ryder, J.; Sutton, A.; Hing, C.; Kwok, C.; Pang, C.; Harvey, I. Dissemination and publication of research findings: An updated review of related biases. Health Technol. Assess. 2010, 14, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.-W.; Song, F.; Vickers, A.; Jefferson, T.; Dickersin, K.; Gøtzsche, P.C.; Krumholz, H.M.; Ghersi, D.; van der Worp, H.B. Increasing value and reducing waste: Addressing inaccessible research. Lancet 2014, 383, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Avrahami, D. Visual Art Therapy’s Unique Contribution in the Treatment of Post-Traumatic Stress Disorders. J. Trauma. Dissociation 2006, 6, 5–38. [Google Scholar] [CrossRef] [PubMed]
- American Music Therapy Association. What is Music Therapy? 2005. Available online: https://www.musictherapy.org/about/musictherapy/ (accessed on 31 October 2025).
- American Dance Therapy Association. What is Dance Therapy? 2025. Available online: https://www.adta.org/ (accessed on 31 October 2025).
- Leather, J.; Kewley, S. Assessing Drama Therapy as an Intervention for Recovering Substance Users: A Systematic Review. J. Drug Issues 2019, 49, 545–558. [Google Scholar] [CrossRef]
- National Association for Poetry Therapy. Promoting Growth and Healing Through Language, Symbol, and Story. Available online: https://poetrytherapy.org/ (accessed on 1 November 2025).
- International Expressive Arts Therapy Association. What is Intermodal Expressive Arts? Available online: https://www.ieata.org/what-is-intermodal-expressive-arts/ (accessed on 1 November 2025).



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).