
Circadian Lighting Was Associated with a Reduction in the Number of Hospitalized Patients Experiencing Falls: A Retrospective Observational Study

Abstract
1. Introduction
2. Materials and Methods
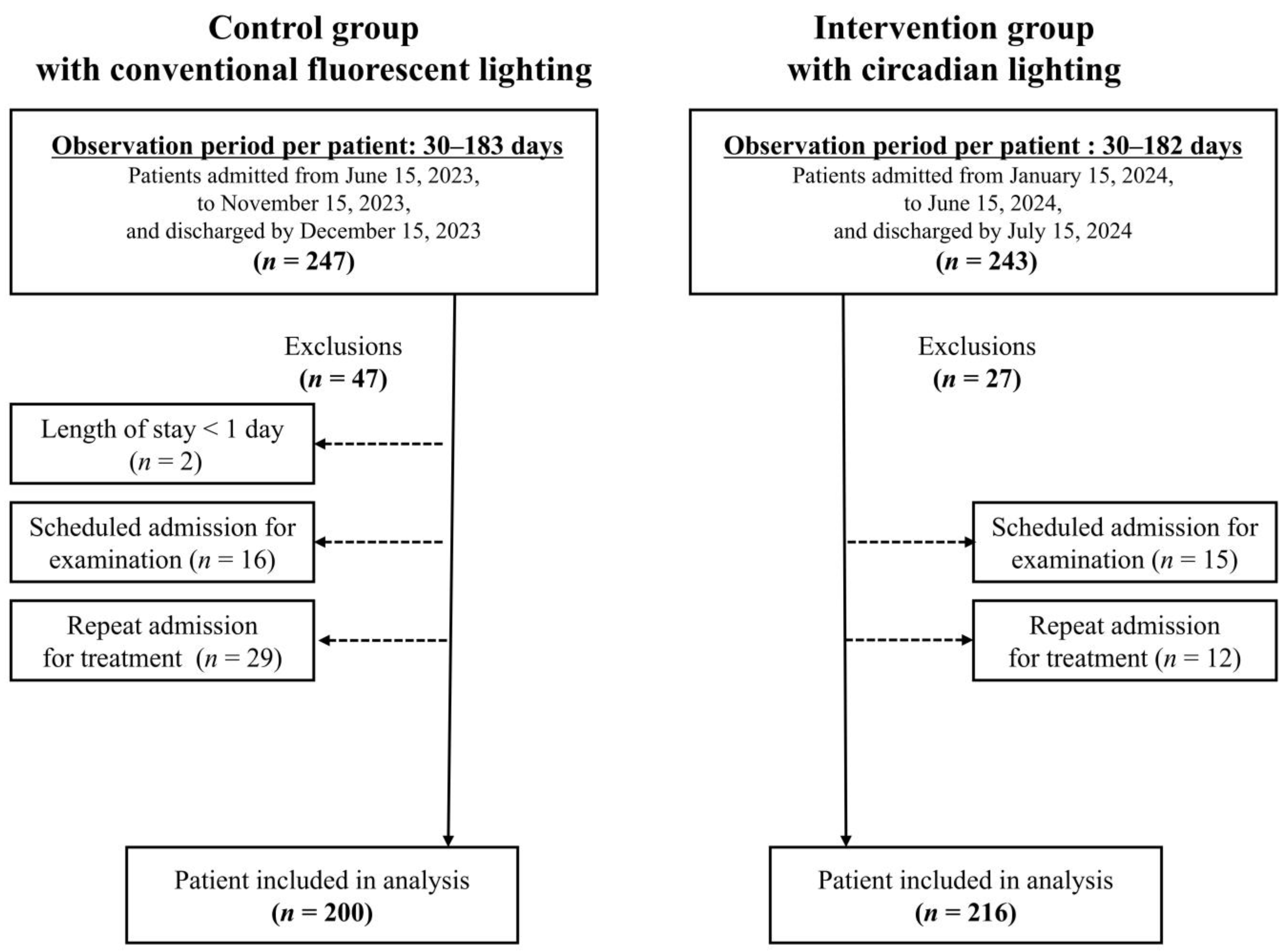
2.1. Study Design
2.2. Participants
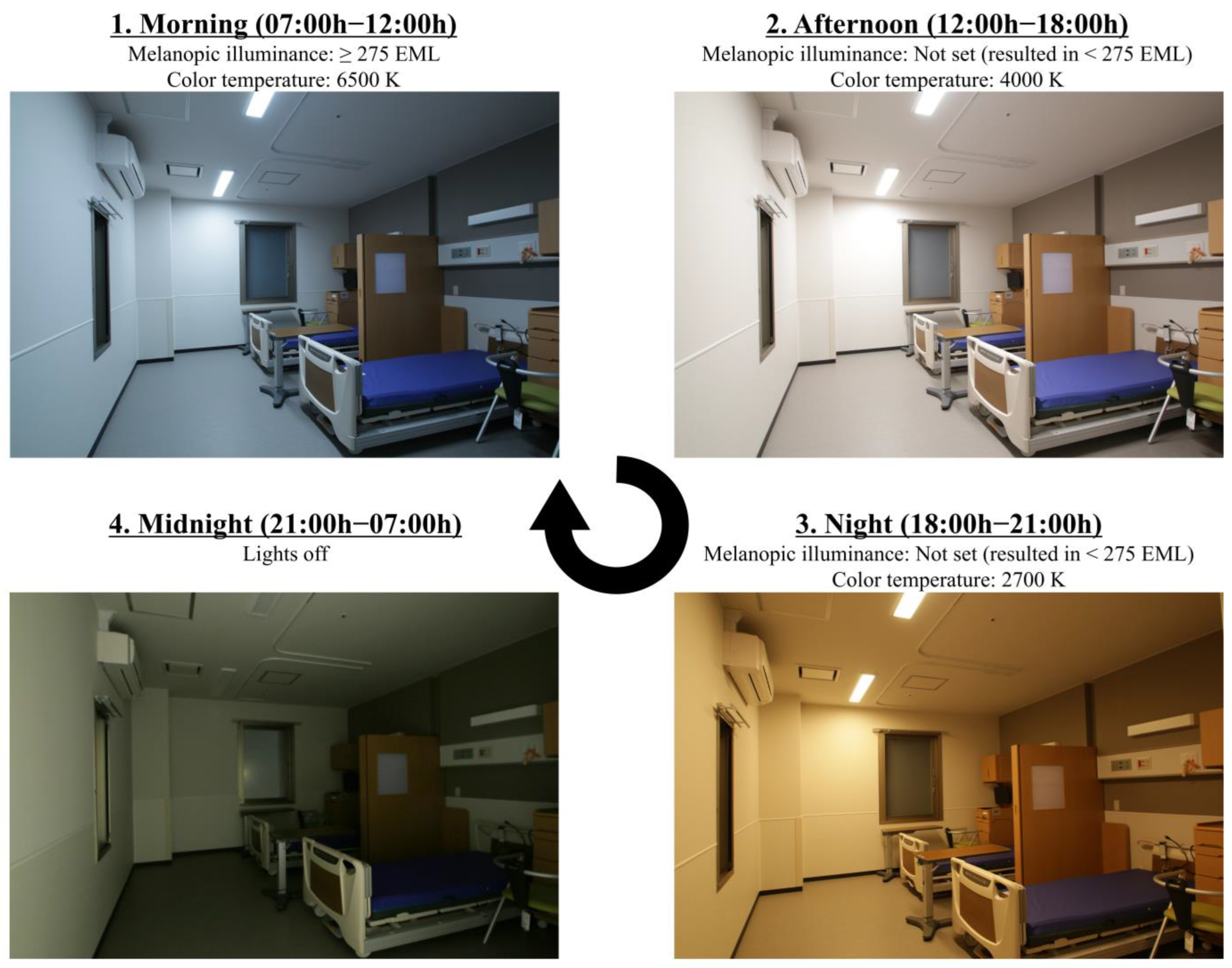
2.3. Lighting Setting
2.4. Light Environment
2.5. Variables
2.6. Study Procedure
2.7. Statistical Analysis
3. Results
3.1. Participant Demographics
3.2. Comparison of the Number of Fallers and Falls
3.3. Risk Factors for Fallers
4. Discussion
4.1. Study Strength
4.2. Lighting Environment
4.3. Mechanisms Underlying the Reduction in the Number of Fallers
4.4. Fall Prevention
4.5. Future Prospects
4.6. Limitations
- Reliability of nursing records: As fall documentation depended on nursing records, it is possible that some falls were not recorded if the nursing staff was unaware of them.
- Adherence to the lighting environment: In the control group, patients could freely operate their room lights, whereas in the intervention group, the circadian lighting was generally not user-adjustable. However, patients in both groups could control their bedside lights, which may have influenced the outcome.
- Changes in hospital facilities from renovation: Environmental changes beyond lighting, resulting from the hospital renovation, are another source of confounding. The renovation involved changes to room entrances, toilet access, and corridors. However, due to building regulations, there were no major changes to the surface area of the rooms. Considering that the majority of falls (81.5%) occurred within patient rooms, we concluded that structural changes outside the rooms were unlikely to have had a significant impact on the fall incidence rate.
- Organizational factors: Because the two groups were studied during different periods, differences in the attending healthcare staff could be a confounding factor. As reported by Kim et al., the likelihood of patient falls is significantly lower in hospitals with lower nurse-to-patient ratios and longer care times, whereas the risk is markedly higher in hospitals with a greater proportion of novice nurses with less than one year of clinical experience [38]. This suggests that organizational-level factors may influence fall risk. However, the medical functions of the ward remained consistent throughout both study periods, the attending physicians did not change, and only a few nurses were different between the periods.
- Seasonal factors: The different seasons during which the two groups were studied could also act as a confounder. Fall events can fluctuate seasonally, and a prior study has reported fewer falls in autumn than in spring [39]. Given the composition of our study—the control group was hospitalized during a season with typically fewer falls, while the intervention group was hospitalized during a season with more falls—it is possible that an even more favorable fall prevention effect would have been observed in the intervention group if the seasonal factor had been controlled.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| aOR | adjusted odds ratio |
| CI | confidence interval |
| ipRGCs | intrinsically photosensitive retinal ganglion cells |
| EML | equivalent melanopic lux |
| LEDs | light-emitting diodes |
| BMI | body mass index |
| FIM | Functional Independence Measure |
| ADLs | activities of daily living |
| MMSE | Mini-Mental State Examination |
| BZDs | benzodiazepines |
| LASSO | least absolute shrinkage and selection operator) |
| EPV | events per variable |
| VIF | variance inflation factor |
| IQR | interquartile range |
| SD | standard deviation |
References
- Morris, R.; O’Riordan, S. Prevention of Falls in Hospital. Clin. Med. 2017, 17, 360–362. [Google Scholar] [CrossRef]
- Cameron, I.D.; Dyer, S.M.; Panagoda, C.E.; Murray, G.R.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for Preventing Falls in Older People in Care Facilities and Hospitals. Cochrane Database Syst. 2018, 9, CD005465. [Google Scholar] [CrossRef]
- Oliver, D.; Healey, F.; Haines, T.P. Preventing Falls and Fall-Related Injuries in Hospitals. Clin. Geriatr. Med. 2010, 26, 645–692. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Ganz, D.A.; Shekelle, P.G. Inpatient Fall Prevention Programs as a Patient Safety Strategy: A Systematic Review. Ann. Intern. Med. 2013, 158, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Morello, R.T.; Barker, A.L.; Watts, J.J.; Haines, T.; Zavarsek, S.S.; Hill, K.D.; Brand, C.; Sherrington, C.; Wolfe, R.; Bohensky, M.A.; et al. The Extra Resource Burden of In-Hospital Falls: A Cost of Falls Study. Med. J. Aust. 2015, 203, 367. [Google Scholar] [CrossRef] [PubMed]
- Dykes, P.C.; Curtin-Bowen, M.; Lipsitz, S.; Franz, C.; Adelman, J.; Adkison, L.; Bogaisky, M.; Carroll, D.; Carter, E.; Herlihy, L.; et al. Cost of Inpatient Falls and Cost-Benefit Analysis of Implementation of an Evidence-Based Fall Prevention Program. JAMA Health Forum 2023, 4, e225125. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.M.; Kamkar, N.; Pieruccini-Faria, F.; Osman, A.; Sarquis-Adamson, Y.; Close, J.; Hogan, D.B.; Hunter, S.W.; Kenny, R.A.; Lipsitz, L.A.; et al. Evaluation of Clinical Practice Guidelines on Fall Prevention and Management for Older Adults: A Systematic Review. JAMA Netw. Open 2021, 4, e2138911. [Google Scholar] [CrossRef]
- Morris, M.E.; Webster, K.; Jones, C.; Hill, A.M.; Haines, T.; McPhail, S.; Kiegaldie, D.; Slade, S.; Jazayeri, D.; Heng, H.; et al. Interventions to Reduce Falls in Hospitals: A Systematic Review and Meta-Analysis. Age Ageing 2022, 51, 1–12. [Google Scholar] [CrossRef]
- Heng, H.; Jazayeri, D.; Shaw, L.; Kiegaldie, D.; Hill, A.M.; Morris, M.E. Hospital Falls Prevention with Patient Education: A Scoping Review. BMC Geriatr. 2020, 20, 140. [Google Scholar] [CrossRef]
- Fitzgerald, J.M.; Adamis, D.; Trzepacz, P.T.; O’Regan, N.; Timmons, S.; Dunne, C.; Meagher, D.J. Delirium: A Disturbance of Circadian Integrity? Med. Hypotheses 2013, 81, 568–576. [Google Scholar] [CrossRef]
- Birder, L.A.; Van Kerrebroeck, P.E.V. Pathophysiological Mechanisms of Nocturia and Nocturnal Polyuria: The Contribution of Cellular Function, the Urinary Bladder Urothelium, and Circadian Rhythm. Urology 2019, 133, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Leng, Y.; Musiek, E.S.; Hu, K.; Cappuccio, F.P.; Yaffe, K. Association between Circadian Rhythms and Neurodegenerative Diseases. Lancet Neurol. 2019, 18, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Legates, T.A.; Fernandez, D.C.; Hattar, S. Light as a Central Modulator of Circadian Rhythms, Sleep and Affect. Nat. Rev. Neurosci. 2014, 15, 443. [Google Scholar] [CrossRef]
- Vasey, C.; McBride, J.; Penta, K. Circadian Rhythm Dysregulation and Restoration: The Role of Melatonin. Nutrients 2021, 13, 3480. [Google Scholar] [CrossRef]
- Al Enezi, J.; Revell, V.; Brown, T.; Wynne, J.; Schlangen, L.; Lucas, R. A “Melanopic” Spectral Efficiency Function Predicts the Sensitivity of Melanopsin Photoreceptors to Polychromatic Lights. J. Biol. Rhythm. 2011, 26, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Circadian Lighting Design. Available online: https://v2.wellcertified.com/en/wellv2/light/feature/3 (accessed on 31 March 2025).
- Lucas, R.J.; Peirson, S.N.; Berson, D.M.; Brown, T.M.; Cooper, H.M.; Czeisler, C.A.; Figueiro, M.G.; Gamlin, P.D.; Lockley, S.W.; O’Hagan, J.B.; et al. Measuring and Using Light in the Melanopsin Age. Trends Neurosci. 2014, 37, 1–9. [Google Scholar] [CrossRef]
- Measuring Melanopic Illuminance and Melanopic Irradiance. Available online: https://lucasgroup.lab.manchester.ac.uk/measuringmelanopicilluminance/ (accessed on 31 March 2025).
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The Reliability of the Functional Independence Measure: A Quantitative Review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Najafpour, Z.; Godarzi, Z.; Arab, M.; Yaseri, M. Risk Factors for Falls in Hospital In-Patients: A Prospective Nested Case Control Study. Int. J. Health Policy Manag. 2019, 8, 300. [Google Scholar] [CrossRef]
- Czernuszenko, A.; Czlonkowska, A. Risk Factors for Falls in Stroke Patients during Inpatient Rehabilitation. Clin. Rehabil. 2009, 23, 176–188. [Google Scholar] [CrossRef]
- Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 31 March 2025).
- Hitcho, E.B.; Krauss, M.J.; Birge, S.; Dunagan, W.C.; Fischer, I.; Johnson, S.; Nast, P.A.; Costantinou, E.; Fraser, V.J. Characteristics and Circumstances of Falls in a Hospital Setting. J. Gen. Intern. Med. 2004, 19, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software ‘EZR’ for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Callis, N. Falls Prevention: Identification of Predictive Fall Risk Factors. Appl. Nurs. Res. 2016, 29, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.; Hodgkinson, B.; Lambert, L.; Wood, J. Falls Risk Factors in the Hospital Setting: A Systematic Review. Int. J. Nurs. Pract. 2001, 7, 38–45. [Google Scholar] [CrossRef]
- Kolla, B.P.; Lovely, J.K.; Mansukhani, M.P.; Morgenthaler, T.I. Zolpidem Is Independently Associated with Increased Risk of Inpatient Falls. J. Hosp. Med. 2013, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in Older People: Epidemiology, Risk Factors and Strategies for Prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef]
- Song, Q.X.; Suadicani, S.O.; Negoro, H.; Jiang, H.H.; Jabr, R.; Fry, C.; Xue, W.; Damaser, M.S. Disruption of Circadian Rhythm as a Potential Pathogenesis of Nocturia. Nat. Rev. Urol. 2025, 22, 276–293. [Google Scholar] [CrossRef]
- Nava Zisapel, C.; Zisapel, N. New Perspectives on the Role of Melatonin in Human Sleep, Circadian Rhythms and Their Regulation. Br. J. Pharmacol. 2018, 175, 3190–3199. [Google Scholar] [CrossRef]
- Díaz-Gutiérrez, M.J.; Martínez-Cengotitabengoa, M.; Sáez de Adana, E.; Cano, A.I.; Martínez-Cengotitabengoa, M.T.; Besga, A.; Segarra, R.; González-Pinto, A. Relationship between the Use of Benzodiazepines and Falls in Older Adults: A Systematic Review. Maturitas 2017, 101, 17–22. [Google Scholar] [CrossRef]
- Karlsson, M.K.; Vonschewelov, T.; Karlsson, C.; CÃster, M.; Rosengen, B.E. Prevention of Falls in the Elderly: A Review. Scand. J. Public Health 2013, 41, 442–454. [Google Scholar] [CrossRef]
- Haines, T.P.; Hill, A.M.; Hill, K.D.; McPhail, S.; Oliver, D.; Brauer, S.; Hoffmann, T.; Beer, C. Patient Education to Prevent Falls Among Older Hospital Inpatients: A Randomized Controlled Trial. Arch. Intern. Med. 2011, 171, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Pati, D.; Valipoor, S.; Lorusso, L.; Mihandoust, S.; Jamshidi, S. The Impact of the Built Environment on Patient Falls in Hospital Rooms: An Integrative Review. J. Patient Saf. 2021, 17, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Benloucif, S.; Burgess, H.J.; Klerman, E.B.; Lewy, A.J.; Middleton, B.; Murphy, P.J.; Parry, B.L.; Revell, V.L. Measuring Melatonin in Humans. J. Clin. Sleep Med. 2008, 4, 66–69. [Google Scholar] [CrossRef] [PubMed]
- de Zambotti, M.; Goldstein, C.; Cook, J.; Menghini, L.; Altini, M.; Cheng, P.; Robillard, R. State of the Science and Recommendations for Using Wearable Technology in Sleep and Circadian Research. Sleep 2024, 47, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, E.; Jung, Y.; Kwon, H.; Lee, S. Patient-Level and Organizational-Level Factors Influencing in-Hospital Falls. J. Adv. Nurs. 2022, 78, 3641–3651. [Google Scholar] [CrossRef]
- López-Soto, P.J.; Smolensky, M.H.; Sackett-Lundeen, L.L.; De Giorgi, A.; Rodríguez-Borrego, M.A.; Manfredini, R.; Pelati, C.; Fabbian, F. Temporal Patterns of In-Hospital Falls of Elderly Patients. Nurs. Res. 2016, 65, 435–445. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Melanopic Illuminance (EML) | Color Temperature (K) | Illuminance (lx) | Number of Rooms | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Median | IQR | ||||
| Reduced ambient light exposure (shade condition) | |||||||||
| Control group | South-facing room | p.m. | 57.7 | [51.1–94.0] | 3630 | [3456–3715] | 128.7 | [113.7–159.2] | 5 |
| North-facing room | 51.4 | [36.3–66.5] | 3687 | [3618–3755] | 104.6 | [74.8–134.4] | 2 | ||
| Intervention group | a.m. | 315.7 | [245.3–323.9] | 6497 | [6460–6511] | 279.4 | [217.1–286.6] | 17 | |
| p.m. | 151.7 | [132.7–207.3] | 4348 | [4121–4395] | 189.7 | [165.8–259.1] | 17 | ||
| night | 54.0 | [49.5–68.2] | 2627 | [2615–2656] | 120.0 | [109.9–151.6] | 17 | ||
| Actual ambient light exposure (normal use) | |||||||||
| Control group | South-facing room | a.m. | 526.3 | [470.8–722.4] | 5268 * | [5131–5674] | 634.9 | [585.4–882.2] | 5 |
| p.m. | 1794.9 | [1056.2–1913.8] | 4514 * | [4404–5432] | 1929.3 | [1236.7–2407.5] | 5 | ||
| North-facing room | a.m. | 60.4 | [60.1–60.7] | 4070 * | [3822–4317] | 105.1 | [95.3–114.9] | 2 | |
| p.m. | 59.3 | [58.0–60.6] | 3901 * | [3693–4108] | 95.8 | [90.7–101.0] | 2 | ||
| Intervention group | a.m. | 383.4 | [245.9–565.7] | 6015 | [5548–6203] | 372.0 | [222.0–514.0] | 17 | |
| p.m. | 271.5 | [201.8–647.2] | 4323 | [4056–4702] | 316.0 | [253.0–649.0] | 17 | ||
| night | 39.9 | [26.9–81.1] | 2606 | [2543–2634] | 94.0 | [70.0–183.0] | 17 | ||
| Control Group | Intervention Group | p Value | ||
|---|---|---|---|---|
| Factors | Number of Cases | 200 | 216 | |
| Age, median [range] | 82.00 [37.00–97.00] | 83.00 [35.00–99.00] | 0.314 | |
| Sex, n (%) | Men | 83 (41.5) | 80 (37.0) | 0.367 |
| Women | 117 (58.5) | 136 (63.0) | ||
| Ethnicity, n (%) | Japanese | 200 (100.0) | 216 (100.0) | 1 |
| Body mass index (kg/m2), median [range] * | 20.28 [11.60–35.28] | 19.97 [11.89–38.14] | 0.662 | |
| FIM motor items score, median [range] * | 23.00 [13.00–72.00] | 20.00 [13.00–77.00] | 0.612 | |
| MMSE score, median [range] * | 20.50 [4.00–30.00] | 21.00 [1.00–30.00] | 0.547 | |
| Primary illness, n (%) | Orthopedics or dermatology | 55 (27.5) | 66 (30.6) | 0.142 |
| Various internal diseases ** | 110 (55.0) | 113 (52.3) | ||
| Neurological disorder | 26 (13.0) | 18 (8.3) | ||
| Malignancy | 9 (4.5) | 19 (8.8) | ||
| Past history, n (%) | Stroke | 53 (26.5) | 49 (22.7) | 0.425 |
| Parkinson’s disease | 27 (13.5) | 25 (11.6) | 0.557 | |
| Other neurological disease | 23 (11.5) | 16 (7.4) | 0.179 | |
| Diabetes mellitus | 55 (27.5) | 55 (25.5) | 0.658 | |
| Malignancy | 16 (8.0) | 29 (13.4) | 0.083 | |
| Medication within 7 days of hospitalization, n (%) | Diuretics | 53 (26.5) | 57 (26.4) | 1 |
| Antihypertensives except diuretics | 85 (42.5) | 105 (48.6) | 0.237 | |
| Anti-coagulants | 63 (31.5) | 66 (30.6) | 0.916 | |
| Diabetes medication | 39 (19.5) | 38 (17.6) | 0.705 | |
| BZD/Z-drugs | 36 (18.0) | 35 (16.2) | 0.696 | |
| Other hypnotics *** | 65 (32.5) | 71 (32.9) | 1 | |
| Anti-depressants | 17 (8.5) | 21 (9.7) | 0.735 | |
| Anti-dementia medication | 30 (15.0) | 27 (12.5) | 0.479 | |
| Anticonvulsants | 13 (6.5) | 15 (6.9) | 1 | |
| Antipsychotics | 44 (22.0) | 56 (25.9) | 0.361 | |
| Antihistamines | 18 (9.0) | 14 (6.5) | 0.362 | |
| Non-narcotic analgesics | 5 (2.5) | 10 (4.6) | 0.298 | |
| Narcotic analgesics | 7 (3.5) | 8 (3.7) | 1 | |
| Length of stay, days | median [IQR] | 17.50 [9.00–36.25] | 18.50 [8.00–39.25] | 0.699 |
| mean (SD) | 27.33 (24.40) | 27.15 (24.83) | ||
| Outcome | Discharge | 107 (53.5) | 128 (59.3) | 0.241 |
| Transfer to a different ward | 64 (32.0) | 57 (26.4) | ||
| Transfer to a different hospital | 19 (9.5) | 14 (6.5) | ||
| Death | 10 (5.0) | 17 (7.9) | ||
| Control Group | Intervention Group | ||
|---|---|---|---|
| Patients, n | 200 | 216 | |
| Patient days | 5465 | 5864 | |
| Fallers, n (%) | 30 (15.0%) | 16 (7.4%) | p = 0.0182 |
| Falls, n (per 1000 patient-days) | 39 (7.14) | 26 (4.43) | |
| Falls with serious complications, n (per 1000 patient-days) | 3 (0.55) * | 0 (0) |
| Non-Faller | Faller | p Value | ||
|---|---|---|---|---|
| Factors | Number of Cases | 370 | 46 | |
| Age in years, n (%) | ≤79 | 149 (40.3) | 11 (23.9) | 0.036 |
| ≥80 | 221 (59.7) | 35 (76.1) | ||
| Sex, n (%) | Men | 144 (38.9) | 19 (41.3) | 0.751 |
| Women | 226 (61.1) | 27 (58.7) | ||
| Body mass index in kg/m2, n (%) * | <18.5 (underweight) | 123 (35.8) | 15 (35.7) | 1 |
| ≥18.5 | 221 (64.2) | 27 (64.3) | ||
| FIM motor items score (%) * | ≤26 (poor motor ADL) | 209 (59.5) | 22 (50.0) | 0.257 |
| ≥27 | 142 (40.5) | 22 (50.0) | ||
| MMSE score (%) * | ≤23 (cognitive decline) | 109 (64.5) | 25 (78.1) | 0.156 |
| ≥24 | 60 (35.5) | 7 (21.9) | 0.156 | |
| Lighting, n (%) | Conventional fluorescent light | 170 (45.9) | 30 (65.2) | 0.018 |
| Circadian LED light | 200 (54.1) | 16 (34.8) | ||
| Primary illness, n (%) | Orthopedics or dermatology | 110 (29.7) | 11 (23.9) | 0.858 |
| Various internal diseases ** | 196 (53.0) | 27 (58.7) | ||
| Neurological disorder | 39 (10.5) | 5 (10.9) | ||
| Malignancy | 25 (6.8) | 3 (6.5) | ||
| Past history, n (%) | Stroke | 91 (24.6) | 11 (23.9) | 1 |
| Parkinson’s disease | 49 (13.2) | 3 (6.5) | 0.242 | |
| Other neurological disease | 33 (8.9) | 6 (13.0) | 0.417 | |
| Diabetes mellitus | 96 (25.9) | 14 (30.4) | 0.595 | |
| Malignancy | 41 (11.1) | 4 (8.7) | 0.803 | |
| Medication within 7 days of hospitalization, n (%) | Diuretics | 95 (25.7) | 15 (32.6) | 0.375 |
| Antihypertensives except diuretics | 174 (47.0) | 16 (34.8) | 0.142 | |
| Anti-coagulants | 117 (31.6) | 12 (26.1) | 0.502 | |
| Diabetes medication | 66 (17.8) | 11 (23.9) | 0.317 | |
| BZD/Z-drugs | 61 (16.5) | 10 (21.7) | 0.405 | |
| Other hypnotics *** | 118 (31.9) | 18 (39.1) | 0.322 | |
| Anti-depressants | 36 (9.7) | 2 (4.3) | 0.411 | |
| Anti-dementia medication | 46 (12.4) | 11 (23.9) | 0.041 | |
| Anticonvulsants | 21 (5.7) | 7 (15.2) | 0.025 | |
| Antipsychotics | 85 (23.0) | 15 (32.6) | 0.148 | |
| Antihistamines | 31 (8.4) | 1 (2.2) | 0.235 | |
| Non-narcotic analgesics | 13 (3.5) | 2 (4.3) | 0.676 | |
| Narcotic analgesics | 13 (3.5) | 2 (4.3) | 0.676 | |
| Length of stay, n (%) | ≤29 days | 252 (68.1) | 25 (54.3) | 0.069 |
| ≥30 days | 118 (31.9) | 21 (45.7) | ||
| Outcome, n (%) | Discharge | 207 (55.9) | 28 (60.9) | 0.703 |
| Transfer to a different ward | 107 (28.9) | 14 (30.4) | ||
| Transfer to a different hospital | 30 (8.1) | 3 (6.5) | ||
| Death | 26 (7.0) | 1 (2.2) |
| Faller | |||
|---|---|---|---|
| Factors | Adjusted Odds Ratio | 95% Confidence Interval | p Value |
| Circadian lighting | 0.558 | 0.351–0.887 | 0.0137 |
| Age ≥ 80 years | 2.48 | 1.18–5.21 | 0.0167 |
| Anticonvulsant medication | 3.68 | 1.39–9.72 | 0.0087 |
| Anti-dementia medication | 2.07 | 0.954–4.48 | 0.0657 |
| BZDs/Z-drugs | 1.46 | 0.667–3.19 | 0.344 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okinami, T.; Suzuki, T.; Nishikawa, N.; Negoro, H. Circadian Lighting Was Associated with a Reduction in the Number of Hospitalized Patients Experiencing Falls: A Retrospective Observational Study. Healthcare 2025, 13, 1692. https://doi.org/10.3390/healthcare13141692
Okinami T, Suzuki T, Nishikawa N, Negoro H. Circadian Lighting Was Associated with a Reduction in the Number of Hospitalized Patients Experiencing Falls: A Retrospective Observational Study. Healthcare. 2025; 13(14):1692. https://doi.org/10.3390/healthcare13141692
Chicago/Turabian StyleOkinami, Takeshi, Toshihiro Suzuki, Nobuyuki Nishikawa, and Hiromitsu Negoro. 2025. "Circadian Lighting Was Associated with a Reduction in the Number of Hospitalized Patients Experiencing Falls: A Retrospective Observational Study" Healthcare 13, no. 14: 1692. https://doi.org/10.3390/healthcare13141692
APA StyleOkinami, T., Suzuki, T., Nishikawa, N., & Negoro, H. (2025). Circadian Lighting Was Associated with a Reduction in the Number of Hospitalized Patients Experiencing Falls: A Retrospective Observational Study. Healthcare, 13(14), 1692. https://doi.org/10.3390/healthcare13141692