


The Impact of the Physical Activity Level on Sarcopenic Obesity in Community-Dwelling Older Adults
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
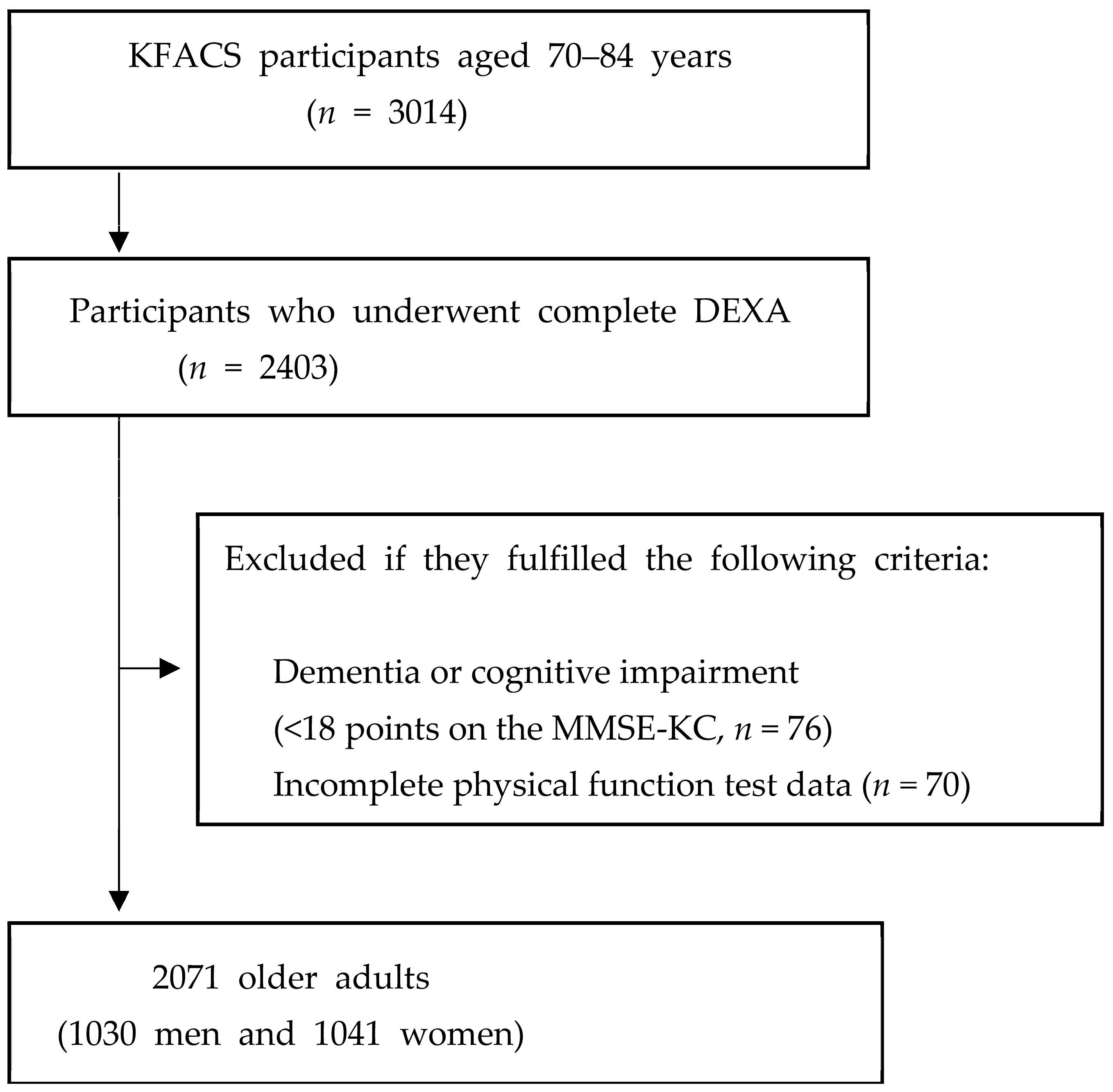
2.1. Study Population
2.2. Sarcopenic Obesity
- (1)
- Fat mass: DXA was used to measure body fat mass, and the body fat mass was adjusted to body weight (body fat mass/weight) (cut-off values, men: >29.7%, women: >37.2%) [17].
- (2)
- Appendicular lean mass: DXA was used to measure ALM, which was adjusted for body weight (ALM/weight, ALM/W) (cutoff values, men: <29.5%, women: <23.2%) [18].
- (3)
- Muscle strength: HGS was measured using a hand dynamometer (T.K.K.5401; Takei Scientific Instruments Co., Ltd., Tokyo, Japan). The participants were instructed to squeeze the handle with maximum effort, with the elbow extended in a standing position for 3 s. HGS was measured twice on both sides, and the maximum value was obtained in kilograms (cutoff values: men <28 kg, women <18 kg) [19].
- (4)
- Five-time sit-to-stand test. The five-time sit-to-stand test assesses the time it takes to rise five times from a seated position without utilizing the arms. The participants were instructed to stand up and sit down five times as quickly as possible. Time was measured to the nearest 0.01 s (cut-off value, ≥17 s) [20].
2.3. Physical Activity
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Physical Activity Category | Cut-Off Levels |
|---|---|
| Low | no activity is reported or |
| not enough to meet moderate or high activity criteria | |
| Moderate | any one of the following three criteria |
| ≥5 days of walking or moderate or vigorous intensity activities accumulating ≥600 MET-min/week | |
| ≥5 days of 30 min of moderate intensity walking per day | |
| ≥3 days of 20 min of vigorous activity per day | |
| High | any one of the following two criteria |
| 7 days of walking or moderate or vigorous intensity activities accumulating ≥3000 MET-min/week | |
| vigorous intensity activity on ≥3 days and ≥1500 MET-min/week |
References
- United Nations Department of Economic Affairs. World Population Prospects 2022: Summary of Results; United Nations: Geneva, Switzerland, 2023. [Google Scholar]
- Batsis, J.A.; Zagaria, A.B. Addressing obesity in aging patients. Med. Clin. 2018, 102, 65–85. [Google Scholar] [CrossRef] [PubMed]
- El Maghraoui, A.; Sadni, S.; El Maataoui, A.; Majjad, A.; Rezqi, A.; Ouzzif, Z.; Mounach, A. Influence of obesity on vertebral fracture prevalence and vitamin D status in postmenopausal women. Nutr. Metab. 2015, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nam, G.E.; Kim, Y.-H.; Han, K.; Jung, J.-H.; Rhee, E.-J.; Lee, W.-Y. Obesity fact sheet in Korea, 2020: Prevalence of obesity by obesity class from 2009 to 2018. J. Obes. Metab. Syndr. 2021, 30, 141. [Google Scholar] [CrossRef] [PubMed]
- Bonomini, F.; Rodella, L.F.; Rezzani, R. Metabolic syndrome, aging and involvement of oxidative stress. Aging Dis. 2015, 6, 109. [Google Scholar] [CrossRef]
- Volpi, E.; Nazemi, R.; Fujita, S. Muscle tissue changes with aging. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 405. [Google Scholar] [CrossRef]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177. [Google Scholar] [CrossRef]
- Horstman, A.M.; Dillon, E.L.; Urban, R.J.; Sheffield-Moore, M. The role of androgens and estrogens on healthy aging and longevity. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2012, 67, 1140–1152. [Google Scholar] [CrossRef]
- Tiidus, P.M.; Lowe, D.A.; Brown, M. Estrogen replacement and skeletal muscle: Mechanisms and population health. J. Appl. Physiol. 2013, 115, 569–578. [Google Scholar] [CrossRef]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- Lee, D.-C.; Shook, R.P.; Drenowatz, C.; Blair, S.N. Physical activity and sarcopenic obesity: Definition, assessment, prevalence and mechanism. Future Sci. OA 2016, 2, FSO127. [Google Scholar] [CrossRef]
- Du, Y.; Xu, T.; Yin, Z.; Espinoza, S.; Xie, Y.; Gentry, C.; Tian, Q.; Zhao, L.-J.; Shen, H.; Luo, Z. Associations of physical activity with sarcopenia and sarcopenic obesity in middle-aged and older adults: The Louisiana osteoporosis study. BMC Public Health 2022, 22, 896. [Google Scholar] [CrossRef] [PubMed]
- Aggio, D.A.; Sartini, C.; Papacosta, O.; Lennon, L.T.; Ash, S.; Whincup, P.H.; Wannamethee, S.G.; Jefferis, B.J.J.P.M. Cross-sectional associations of objectively measured physical activity and sedentary time with sarcopenia and sarcopenic obesity in older men. Prev. Med. 2016, 91, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Ryu, M.; Jo, J.; Lee, Y.; Chung, Y.-S.; Kim, K.-M.; Baek, W.-C.J.A. Association of physical activity with sarcopenia and sarcopenic obesity in community-dwelling older adults: The Fourth Korea National Health and Nutrition Examination Survey. Age Ageing 2013, 42, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Obes. Facts 2022, 15, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Won, C.W.; Lee, S.; Kim, J.; Chon, D.; Kim, S.; Kim, C.-O.; Kim, M.K.; Cho, B.; Choi, K.M.; Roh, E. Korean frailty and aging cohort study (KFACS): Cohort profile. BMJ Open 2020, 10, e035573. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Chang, C.; Tanaka, T.; Kuroda, A.; Tsuji, T.; Akishita, M.; Iijima, K. The association between sarcopenic obesity and depressive symptoms in older Japanese adults. PLoS ONE 2016, 11, e0162898. [Google Scholar] [CrossRef]
- Kim, M.K.; Baek, K.H.; Song, K.-H.; Kang, I.M.; Park, C.Y.; Lee, W.Y.; Oh, K.W. Vitamin D deficiency is associated with sarcopenia in older Koreans, regardless of obesity: The Fourth Korea National Health and Nutrition Examination Surveys (KNHANES IV) 2009. J. Clin. Endocrinol. Metab. 2011, 96, 3250–3256. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Cesari, M.; Kritchevsky, S.B.; Newman, A.B.; Simonsick, E.M.; Harris, T.B.; Penninx, B.W.; Brach, J.S.; Tylavsky, F.A.; Satterfield, S.; Bauer, D.C. Added value of physical performance measures in predicting adverse health-related events: Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2009, 57, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.J.M.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.; Grjibovski, A.M.; Hagströmer, M.; Sallis, J.F.; Sjöström, M. The association between health enhancing physical activity and neighbourhood environment among Swedish adults—A population-based cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.D.; Vaux-Bjerke, A.; Quam, J.B.; Piercy, K.L.; Troiano, R.P.; George, S.M.; Sprow, K.; Ballard, R.M.; Fulton, J.E.; Galuska, D.A. Physical Activity Guidelines for Americans. Available online: https://revistanadar.com.br/index.php/Swimming-Magazine/article/view/48/89 (accessed on 30 October 2023).
- Cauley, J.A. An overview of sarcopenic obesity. J. Clin. Densitom. 2015, 18, 499–505. [Google Scholar] [CrossRef]
- Goisser, S.; Kemmler, W.; Porzel, S.; Volkert, D.; Sieber, C.C.; Bollheimer, L.C.; Freiberger, E. Sarcopenic obesity and complex interventions with nutrition and exercise in community-dwelling older persons—A narrative review. Clin. Interv. Aging 2015, 6, 1267–1282. [Google Scholar]
- Poggiogalle, E.; Migliaccio, S.; Lenzi, A.; Donini, L.M. Treatment of body composition changes in obese and overweight older adults: Insight into the phenotype of sarcopenic obesity. Endocrine 2014, 47, 699–716. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Liatis, S.; Dalamaga, M.; Kokkinos, A.J. Sarcopenic obesity: Epidemiologic evidence, pathophysiology, and therapeutic perspectives. Curr. Obes. Rep. 2019, 8, 458–471. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; Koyanagi, A.; Olaya, B.; Ayuso-Mateos, J.L.; Miret, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Leonardi, M.; Haro, J.M. Factors associated with skeletal muscle mass, sarcopenia, and sarcopenic obesity in older adults: A multi-continent study. J. Cachexia Sarcopenia Muscle 2016, 7, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The effects of exercise and physical activity on weight loss and maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Duscha, B.D.; Slentz, C.A.; Johnson, J.L.; Houmard, J.A.; Bensimhon, D.R.; Knetzger, K.J.; Kraus, W.E. Effects of exercise training amount and intensity on peak oxygen consumption in middle-age men and women at risk for cardiovascular disease. Chest 2005, 128, 2788–2793. [Google Scholar] [CrossRef]
- Kessler, H.S.; Sisson, S.B.; Short, K.R. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. 2012, 42, 489–509. [Google Scholar] [CrossRef]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of high-intensity interval training (HIT) and continuous endurance training for VO 2max improvements: A systematic review and meta-analysis of controlled trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [PubMed]
- Hägg, S.; Fall, T.; Ploner, A.; Mägi, R.; Fischer, K.; Draisma, H.H.; Kals, M.; de Vries, P.S.; Dehghan, A.; Willems, S.M. Adiposity as a cause of cardiovascular disease: A Mendelian randomization study. Int. J. Epidemiol. 2015, 44, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Pattyn, N.; Coeckelberghs, E.; Buys, R.; Cornelissen, V.A.; Vanhees, L. Aerobic interval training vs. moderate continuous training in coronary artery disease patients: A systematic review and meta-analysis. Sports Med. 2014, 44, 687–700. [Google Scholar] [CrossRef] [PubMed]


| Men (n = 1030) | Women (n = 1041) | |||
|---|---|---|---|---|
| SO † (+) (n = 90, 8.7%) | SO (−) (n = 940, 91.3%) | SO † (+) (n = 108, 10.4%) | SO (−) (n = 933, 89.6%) | |
| Age (years) | 78.7 ± 3.9 ** | 76.1 ± 3.88 | 76.6 ± 3.9 ** | 75.3 ± 3.9 |
| Height (cm) | 163 ± 5.8 ** | 165 ± 5.5 | 150 ± 5.3 ** | 152 ± 5.2 |
| Weight (kg) | 67.8 ± 9.5 ** | 64.9 ± 8.8 | 58.6 ± 7.6 ** | 56.2 ± 7.6 |
| BMI (kg/m2) | 25.6 ± 2.6 ** | 23.7 ± 2.8 | 25.8 ± 2.7 ** | 24.2 ± 2.8 |
| Waist circumference (cm) | 94.8 ± 7.8 ** | 88.0 ± 8.2 | 89.7 ± 8.4 ** | 85.6 ± 8.0 |
| Hypertension (n, %) | 60 (66.7) ** | 485 (51.6) | 74 (68.5) * | 528 (56.6) |
| Diabetes mellitus (n, %) | 32 (35.6) ** | 220 (23.4) | 26 (24.1) | 173 (18.5) |
| Dyslipidemia (n, %) | 27 (30.0) | 223 (23.7) | 52 (44.1) | 373 (40.0) |
| Heart disease (n, %) | 11 (12.2) | 88 (9.4) | 7 (6.5) | 55 (5.9) |
| CVA (n, %) | 4 (4.4) | 56 (6.0) | 4 (3.7) | 28 (3.0) |
| Alcohol (n, %) | 46 (47.8) | 483 (51.4) | 13 (11.6) | 99 (10.6) |
| Current smoker (n, %) | 8 (9.8) | 104 (11.1) | 1 (0.9) | 10 (1.1) |
| Knee OA (n, %) | 12 (13.3) | 97 (10.3) | 33 (30.6) | 267 (28.6) |
| Osteoporosis (n, %) | 4 (4.4) | 25 (2.7) | 28 (25.9) | 225 (24.1) |
| Depression (n, %) | 4 (4.4) | 15 (1.6) | 8 (7.4) * | 26 (2.8) |
| MMSE-KC | 26.11 ± 3.01 | 26.43 ± 2.67 | 24.4 ± 3.8 ** | 25.4 ± 3.3 |
| Total physical activity (METs-min/week) ¶ | 2320 ± 1833 ** | 4319 ± 4549 | 2606 ± 2242 ** | 4158 ± 3822 |
| Total energy expenditure (Kcal/week) § | 2641 ± 2180 ** | 4635 ± 5026 | 2526 ± 2224 ** | 3851 ± 3371 |
| Biochemical variables | ||||
| Fasting glucose (mg/dL) | 109.7 ± 21.7 | 104.8 ± 24.1 | 103.7 ± 30.8 | 102.2 ± 21.1 |
| HbA1c (%) | 6.1 ± 0.7 * | 5.9 ± 0.8 | 6.1 ± 1.1 | 6.03 ± 0.76 |
| Total cholesterol (mg/dL) | 169.7 ± 33.6 | 168.1 ± 34.9 | 185.0 ± 40.3 | 181.4 ± 35.4 |
| HDL-C (mg/dL) | 46.0 ± 13.3 ** | 51.0 ± 14.3 | 57.3 ± 15.8 | 54.8 ± 13.5 |
| LDL-C (mg/dL) | 105.8 ± 30.3 | 104.1 ± 31.8 | 112.3 ± 35.2 | 113.1 ± 33.9 |
| Protein (mg/dL) | 7.0 ± 0.4 | 7.0 ± 0.4 | 6.9 ± 0.4 | 7.0 ± 0.3 |
| Albumin (mg/dL) | 4.3 ± 0.2 | 4.3 ± 0.2 | 4.3 ± 0.2 | 4.3 ± 0.2 |
| Unadjusted Model | Fully Adjusted Model | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Physical activity level | ||||
| Moderate Activity † | 0.77 (0.40–1.49) | 0.83 (0.46–1.48) | 0.89 (0.44–1.77) | 0.92 (0.50–1.70) |
| High activity †† | 0.47 (0.29–0.74) * | 0.35 (0.22–0.55) ** | 0.53 (0.33–0.87) * | 0.39 (0.24–0.62) ** |
| Physical intensity category | ||||
| 8.0 MET ¶¶ (vigorous) | 0.40 (0.16–0.98) * | 0.39 (0.07–2.24) | 0.46 (0.19–1.13) | 0.56 (0.12–2.74) |
| 4.0 MET ¶¶ (moderate) | 0.61 (0.46–0.82) * | 0.77 (0.64–0.92) * | 0.68 (0.51–0.91) * | 0.83 (0.70–0.98) * |
| 3.3 MET ¶¶ (walking) | 0.73 (0.57–0.93) * | 0.62 (0.47–0.82) | 0.74 (0.58–0.95) * | 0.66 (0.51–0.87) * |
| Unadjusted Model | Fully Adjusted Model | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| High fat mass ¶ | 0.73 (0.56–0.96) * | 0.68 (0.53–0.87) * | 0.78 (0.59–1.04) | 0.65 (0.50–0.84) * |
| Low muscle mass ¶ | 0.62 (0.49–0.80) ** | 0.53 (0.41–0.68) ** | 0.67 (0.52–0.87) * | 0.51 (0.39–0.66) * |
| Low skeletal muscle function ¶ | 0.55 (0.41–0.74) ** | 0.39 (0.28–0.52) ** | 0.63 (0.45–0.87) * | 0.44 (0.32–0.60) * |
| Unadjusted Model | Fully Adjusted Model | |||
| Men | Women | Men | Women | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Sarcopenic Obesity † | 0.39 (0.24–0.61) ** | 0.37 (0.24–0.57) ** | 0.44 (0.27–0.71) * | 0.43 (0.27–0.67) * |
| High fat mass ¶ | 0.88 (0.67–1.14) | 0.87 (0.68–1.11) | 0.90 (0.68–1.19) | 0.81 (0.62–1.05) |
| Low muscle mass ¶ | 0.73 (0.57–0.93) * | 0.61 (0.48–0.78) ** | 0.76 (0.59–0.99) * | 0.58 (0.44–0.75) * |
| Low skeletal muscle function ¶ | 0.44 (0.33–0.59) ** | 0.33 (0.25–0.45) ** | 0.52 (0.37–0.72) * | 0.40 (0.29–0.55) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Chon, J.; Yoo, M.C.; Shim, G.Y.; Kim, M.; Kim, M.; Soh, Y.; Won, C.W. The Impact of the Physical Activity Level on Sarcopenic Obesity in Community-Dwelling Older Adults. Healthcare 2024, 12, 349. https://doi.org/10.3390/healthcare12030349
Choi S, Chon J, Yoo MC, Shim GY, Kim M, Kim M, Soh Y, Won CW. The Impact of the Physical Activity Level on Sarcopenic Obesity in Community-Dwelling Older Adults. Healthcare. 2024; 12(3):349. https://doi.org/10.3390/healthcare12030349
Chicago/Turabian StyleChoi, Seongmin, Jinmann Chon, Myung Chul Yoo, Ga Yang Shim, Minjung Kim, Miji Kim, Yunsoo Soh, and Chang Won Won. 2024. "The Impact of the Physical Activity Level on Sarcopenic Obesity in Community-Dwelling Older Adults" Healthcare 12, no. 3: 349. https://doi.org/10.3390/healthcare12030349
APA StyleChoi, S., Chon, J., Yoo, M. C., Shim, G. Y., Kim, M., Kim, M., Soh, Y., & Won, C. W. (2024). The Impact of the Physical Activity Level on Sarcopenic Obesity in Community-Dwelling Older Adults. Healthcare, 12(3), 349. https://doi.org/10.3390/healthcare12030349