
COVID-19 Vaccine Acceptance Behavior among Hispanics/Latinxs in Nevada: A Theory-Based Analysis




Abstract
1. Introduction
2. Materials and Methods
2.1. Population
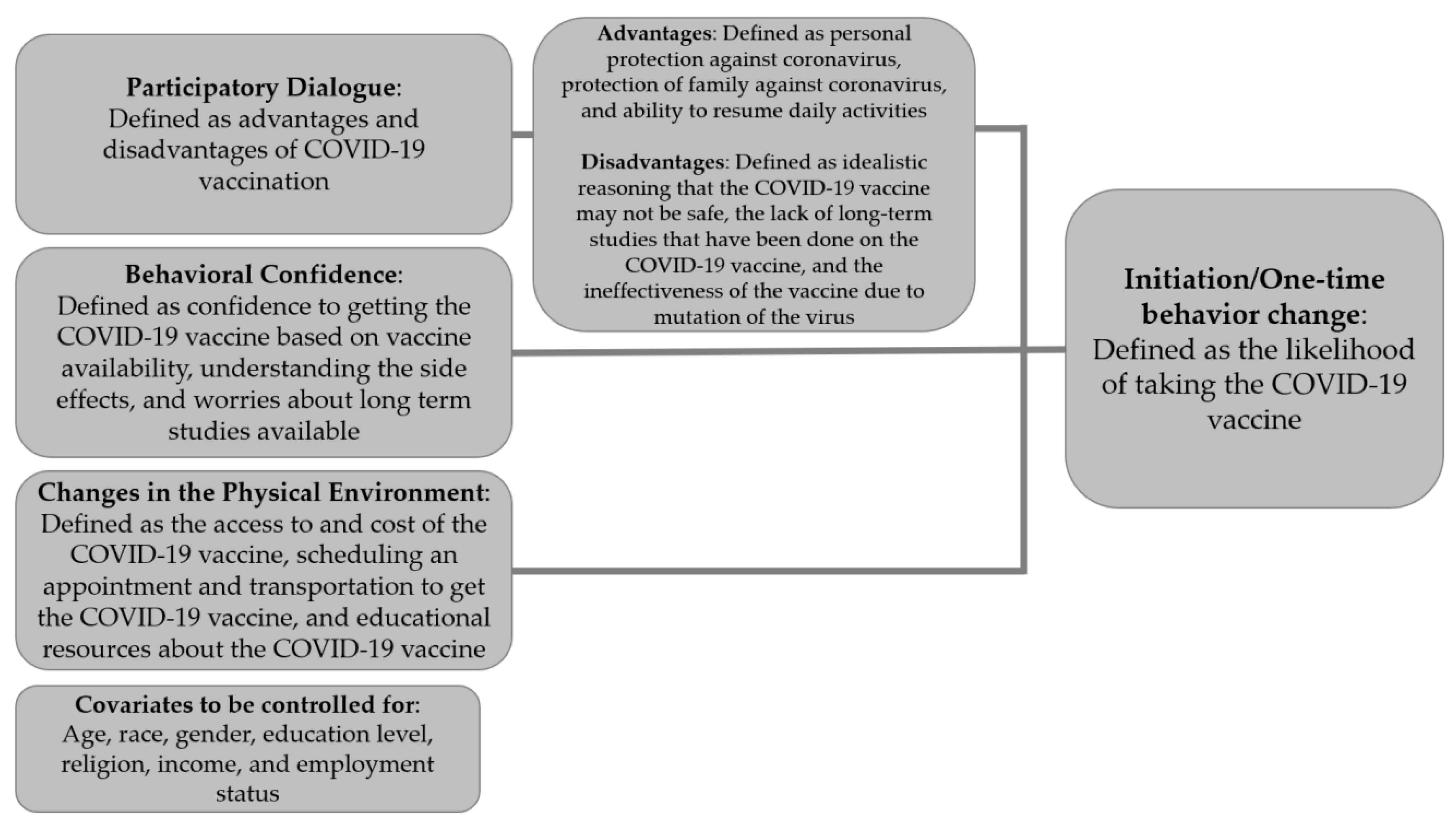
2.2. Theoretical Framework
2.3. Instrumentation
2.4. Survey Translation
2.5. Face and Content Validity
2.6. Data Collection
2.7. Construct Validity
2.8. Reliability
2.9. Data Analysis
2.10. Ethical Approval
3. Results
3.1. Confirmatory Factor Analysis for Construct Validity
3.2. Descriptive Statistics of Demographic Variables
3.3. Descriptive Statistics of Construct Variables
3.4. Zero-Order Correlation Matrix of Construct Variables
3.5. Hierarchical Multiple Regression among Construct Variables and Covariates
4. Discussion
4.1. Interpretation of Findings
4.2. Implications for Practice
4.3. Strengths of the Study
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://worldhealthorg.shinyapps.io/covid/ (accessed on 4 August 2022).
- World Health Organization. The Impact of COVID-19 on Global Health Goals. Available online: https://www.who.int/news-room/spotlight/the-impact-of-covid-19-on-global-health-goals (accessed on 1 December 2022).
- Khubchandani, J.; Macias, Y. COVID-19 vaccination hesitancy in Hispanics and African-Americans: A review and recommendations for practice. Brain Behav. Immun. Health 2021, 15, 100277. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Risk for COVID-19 Infection. Hospitalization, and Death by Race/Ethnicity. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 4 August 2022).
- Heard, M.D. The Effects of COVID-19 on America’s Hispanic and Latinx Communities. Available online: https://healthlaw.org/the-effects-of-covid-19-on-americas-hispanic-and-latinx-communities/ (accessed on 1 December 2022).
- U.S Food & Drug Administration. FDA Approves First COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 1 December 2022).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Oliver, S.E.; Gargano, J.W.; Scobie, H.; Wallace, M.; Hadler, S.C.; Leung, J.; Blain, A.E.; McClung, N.; Campos-Outcalt, D.; Morgan, R.L.; et al. The Advisory Committee on Immunization Practices’ interim recommendation for use of Janssen COVID-19 vaccine—United States, February 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- U.S Food & Drug Administration. Spikevax and Moderna COVID-19 Vaccine. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/spikevax-and-moderna-covid-19-vaccine (accessed on 1 December 2022).
- World Health Organization. Report of the Sage Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 1 December 2022).
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for COVID-19 vaccines: A rapid systematic review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunizing the Public against Misinformation. Available online: https://www.who.int/news-room/feature-stories/detail/immunizing-the-public-against-misinformation (accessed on 14 February 2023).
- Farooq, F.; Rathore, F.A. COVID-19 Vaccination and the Challenge of Infodemic and Disinformation. J. Korean Med. Sci. 2021, 36, e78. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Ghaddar, A.; Khandaqji, S.; Awad, Z.; Kansoun, R. Conspiracy beliefs and vaccination intent for COVID-19 in an infodemic. PLoS ONE 2022, 17, e0261559. [Google Scholar] [CrossRef]
- Kearney, A.; Lopes, L.; Brodie, M. Vaccine Hesitancy among Hispanic Adults. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/vaccine-hesitancy-among-hispanic-adults/ (accessed on 1 December 2022).
- Hamel, L.; Artiga, S.; Safarpour, A.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: COVID-19 Vaccine Access, Information, and Experiences among Hispanic Adults in the US. 2021. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-access-information-experiences-hispanic-adults/ (accessed on 1 December 2022).
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Gibson, D.; Agaewal, S.; Meghani, A.; Limaye, R.J.; Labrique, A. COVID-19 vaccine acceptability and inequity in the United States: Results from a nationally representative survey. Med. Lett. CDC FDA 2021, 143. [Google Scholar] [CrossRef]
- Latkin, C.; Dayton, L.A.; Yi, G.; Konstantopoulos, A.; Park, J.; Maulsby, C.; Kong, X. COVID-19 vaccine intentions in the United States, a social-ecological framework. Vaccine 2021, 39, 2288–2294. [Google Scholar] [CrossRef] [PubMed]
- Salmon, D.A.; Dudley, M.Z.; Brewer, J.; Kan, L.; Gerber, J.E.; Budigan, H.; Proveaux, T.M.; Bernier, R.; Rimal, R.; Schwartz, B. COVID-19 vaccination attitudes, values and intentions among United States adults prior to emergency use authorization. Vaccine 2021, 39, 2698–2711. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.S.; Osama, T.; McKechnie, D.G.J.; Majeed, A. Covid-19 vaccine hesitancy among ethnic minority groups. BMJ 2021, 372, n513. [Google Scholar] [CrossRef]
- Kadambari, S.; Vanderslott, S. Lessons about COVID-19 vaccine hesitancy among minority ethnic people in the UK. Lancet Infect. Dis. 2021, 21, 1204–1206. [Google Scholar] [CrossRef]
- Reid, J.A.; Mabhala, M.A. Ethnic and minority group differences in engagement with COVID-19 vaccination programmes—At Pandemic Pace; when vaccine confidence in mass rollout meets local vaccine hesitancy. Isr. J. Health Policy Res. 2021, 10, 33. [Google Scholar] [CrossRef]
- Garcia, L.L.; Yap, J.F.C. The role of religiosity in COVID-19 vaccine hesitancy. J. Public Health 2021, 43, e529–e530. [Google Scholar] [CrossRef]
- Zimmerman, R.K. Helping patients with ethical concerns about COVID-19 vaccines in light of fetal cell lines used in some COVID-19 vaccines. Vaccine 2021, 39, 4242–4244. [Google Scholar] [CrossRef]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A. Statistical power analyses using GPower 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G*Power statistical power analyses for Mac and Windows. Heinrich-Heine-Univ. Düsseldorf 2020, 39, 175–191. [Google Scholar]
- Hutcheson, G.D.; Sofroniou, N. The Multivariate Social Scientist; SAGE Publications Limited: London, UK, 1999. [Google Scholar]
- Sharma, M. Multi-theory model (MTM) for health behavior change. WebmedCentral Behav. 2015, 6, WMC004982. [Google Scholar]
- Taylor, P.; Lopez, M.; Martionez, J.; Velasco, G. When Labels Don’t Fit: Hispanics and Their Views of Identity; Pew Hispanic Center: Washington, DC, USA, 2012. [Google Scholar]
- Motel, S.; Passel, J. The 10 Largest Hispanic Origin Groups: Characteristics, Rankings, Top Counties; Pew Hispanic Center: Washington, DC, USA, 2012. [Google Scholar]
- Noe-Bustamante, L. Key Facts about U.S. Hispanics and Their Diverse Heritage; Policy File; Pew Hispanic Center: Washington, DC, USA, 2019. [Google Scholar]
- Stevens, J. Applied Multivariate Statistics for the Social Sciences; Erlbaum: Mahwah, NJ, USA, 1996. [Google Scholar]
- Sharma, M.; Petosa, R.L. Measurement and Evaluation for Health Educators; Jones & Bartlett: Burlington, MA, USA, 2014. [Google Scholar]
- UCLA. Institute for Digital Research & Education Statistical Consulting Group What Does Cronbach’s Alpha Mean? SPSS FAQ. Available online: https://stats.idre.ucla.edu/spss/faq/what-does-cronbachs-alpha-mean/ (accessed on 1 December 2022).
- IBM Total Variance Explained. Available online: https://www.ibm.com/docs/en/spss-statistics/27.0.0?topic=detection-total-variance-explained (accessed on 1 December 2022).
- Office of Research Integrity Informed Consent. Available online: https://www.unlv.edu/research/ORI-HSR/informed-consent (accessed on 1 December 2022).
- Wan, W. Coronavirus Vaccines Face Trust Gap in Black and Latino Communities, Study Finds. 2020. Available online: WashingtonPost.com (accessed on 1 December 2022).
- Reverby, S.M. Racism, disease, and vaccine refusal: People of color are dying for access to COVID-19 vaccines. PLoS Biol. 2021, 19, e3001167. [Google Scholar] [CrossRef] [PubMed]
- Salgado de Snyder, V.N.; Garcia, D.; Pineda, R.; Calderon, J.; Diaz, D.; Morales, A.; Perez, B. Exploring Why Adult Mexican Males Do Not Get Vaccinated: Implications for COVID-19 Preventive Actions. Hisp. J. Behav. Sci. 2020, 42, 515–527. [Google Scholar] [CrossRef]
- Dawson, L.; Ranji, U.; Kates, J.; Michaud, J. What Does a Multi-Dose Series Mean for the COVID-19 Vaccination Effort? Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/what-does-a-multi-dose-series-mean-for-the-covid-19-vaccination-effort/ (accessed on 1 December 2022).



{kind=link}
{kind=link}
| Characteristic | M (SD) | n (%) |
|---|---|---|
| Age (in years) | 37.83 (14.141) | |
| Gender | ||
| Male | 69 (29.9) | |
| Female | 160 (69.3) | |
| Other | 0 (0.0) | |
| Hispanic/Latinx Identity | ||
| Argentinian | 5 (2.2) | |
| Bolivian | 0 (0.0) | |
| Chilean | 2 (0.9) | |
| Colombian | 4 (1.7) | |
| Costa Rican | 2 (0.9) | |
| Cuban | 7 (3.0) | |
| Dominican | 2 (0.9) | |
| Ecuadorian | 1 (0.4) | |
| Guatemalan | 4 (1.7) | |
| Honduran | 4 (1.7) | |
| Mexican | 146 (63.2) | |
| Nicaraguan | 2 (0.9) | |
| Panamanian | 1 (0.4) | |
| Paraguayan | 0 (0.0) | |
| Peruvian | 1 (0.4) | |
| Puerto Rican | 18 (7.8) | |
| Salvadoran | 4 (1.7) | |
| Uruguayan | 0 (0.0) | |
| Venezuelan | 0 (0.0) | |
| Other Central American | 0 (0.0) | |
| Other South American | 3 (1.3) | |
| All other Hispanic or Latino | 19 (8.2) | |
| Prefer not to answer | 4 (1.7) | |
| Highest level of education | ||
| Less than high school | 5 (2.2) | |
| High school | 75 (32.5) | |
| Some college | 94 (40.7) | |
| Bachelor’s degree or higher | 53 (22.9) | |
| Religion | ||
| Buddhism | 2 (0.9) | |
| Catholicism | 79 (34.2) | |
| Judaism | 4 (1.7) | |
| Mormonism | 3 (1.3) | |
| Orthodox Christian | 7 (3.0) | |
| Other Christianity | 40 (16.9) | |
| Protestant | 8 (3.5) | |
| Unaffiliated with any religion | 69 (29.9) | |
| Other | 17 (7.4) | |
| Annual individual income | ||
| USD 0 to USD 9999 | 15 (6.5) | |
| USD 10,000 to USD 24,999 | 33 (14.3) | |
| USD 25,000 to USD 49,999 | 85 (36.8) | |
| USD 50,000 to USD 74,999 | 53 (22.9) | |
| USD 75,000 to USD 99,999 | 28 (12.1) | |
| USD 100,000 to USD 149,999 | 14 (6.1) | |
| Over USD 150,000 | 1 (0.4) | |
| Current employment status | ||
| Employed | 138 (59.7) | |
| Self-employed | 26 (11.3) | |
| Laid-off/Furloughed | 0 (0.0) | |
| Retired | 12 (5.2) | |
| Homemaker | 20 (8.7) | |
| Unreported employment | 2 (0.9) | |
| Unemployed | 27 (11.7) | |
| Other | 4 (1.7) | |
| Number of people living in household | 3.22 (1.567) | |
| Marital status | ||
| Single | 84 (36.4) | |
| Married | 74 (32.0) | |
| Divorced | 31 (13.4) | |
| Widowed | 1 (0.4) | |
| Separate | 5 (2.2) | |
| Never married | 6 (2.6) | |
| In a civil union or registered domestic partnership | 11 (4.8) | |
| A member of an unmarried couple | 17 (7.4) | |
| Possesses health insurance | ||
| Yes | 182 (78.8) | |
| No | 47 (20.3) | |
| Political affiliation (optional to answer) | ||
| Republican | 46 (19.9) | |
| Democratic | 82 (35.5) | |
| Independent | 59 (25.5) | |
| Other | 17 (7.4) | |
| Prefer not to answer | 21 (9.1) | |
| Current citizenship status (optional to answer) | ||
| Is a citizen of the United States | 206 (89.2) | |
| Not a citizen of the United States | 12 (5.2) | |
| Prefer not to answer | 6 (2.6) | |
| Expresses hesitancy to taking COVID-19 vaccine | ||
| Yes | 84 (36.4) | |
| No | 147 (63.6) | |
| Received at least one dose of the COVID-19 vaccine | ||
| Yes | 136 (58.9) | |
| No | 95 (41.1) | |
| Completed series of COVID-19 vaccine | ||
| Yes | 127 (55.0) | |
| No | 104 (45.0) | |
| Has a trusted provider provided COVID-19 vaccine information infmation | ||
| Yes | 161 (69.7) | |
| No | 68 (29.4) | |
| Has been encouraged by a medical provider to take the COVID-19 vaccine | ||
| Yes | 96 (41.6) | |
| No | 133 (57.6) |
| Variable | Vaccine-Hesitant Individuals (n = 84) | Vaccine Non-Hesitant Individuals (n = 147) | All Participants (n = 231) | |||||
|---|---|---|---|---|---|---|---|---|
| Possible Range | Observed Range | Mean (SD) | Possible Range | Observed Range | Mean (SD) | Cronbach’s Alpha | p-Value | |
| Initiation | 0–4 | 0–4 | 0.843 (1.1841) | 0–4 | 0–4 | 3.056 (1.378) | <0.001 | |
| Participatory dialogue: advantages | 0–12 | 0–9 | 3.083 (2.617) | 0–12 | 0–12 | 7.545 (3.440) | 0.960 | <0.001 |
| Participatory dialogue: disadvantages | 0–12 | 2–12 | 9.155 (2.659) | 0–12 | 0–12 | 5.124 (2.850) | 0.841 | 0.002 |
| Participatory dialogue: advantages–disadvantages | −12–+12 | −12–+7 | −6.071 (4.834) | −12–+12 | −12–+12 | 2.421 (4.785) | <0.001 | |
| Behavioral confidence | 0–12 | 0–9 | 4.361 (1.664) | 0–12 | 0–12 | 8.570 (3.351) | 0.773 | <0.001 |
| Changes in the physical environment | 0–20 | 0–20 | 12.928 (5.055) | 0–20 | 0–20 | 14.278 (5.117) | 0.870 | <0.001 |
| Sustenance | 0–4 | 0–4 | 0.634 (0.988) | 0–4 | 0–4 | 2.722 (1.465) | <0.001 | |
| Emotional transformation | 0–24 | 0–23 | 7.277 (5.315) | 0–24 | 0–24 | 16.133 (7.0653) | 0.992 | <0.001 |
| Practice for change | 0–20 | 0–20 | 7.634 (6.093) | 0–20 | 0–20 | 13.090 (5.390) | 0.901 | <0.001 |
| Changes in the social environment | 0–12 | 0–12 | 5.061 (3.923) | 0–12 | 0–12 | 8.069 (3.363) | 0.907 | <0.001 |
| Vaccine-Hesitant Individuals (n = 84) | ||||
| Construct | Initiation | Participatory Dialogue | Behavioral Confidence | Changes in the Physical Environment |
| 1. Initiation | – | 0.691 ** (p < 0.001) | 0.636 ** (p < 0.001) | −0.165 (p = 0.136) |
| 2. Participatory dialogue: advantages–disadvantages | – | 0.411 ** (p < 0.001) | −0.320 ** (p = 0.003) | |
| 3. Behavioral confidence | – | 0.202 (p = 0.067) | ||
| 4. Changes in the physical environment | – | |||
| Vaccine Non-Hesitant Individuals (n = 147) | ||||
| Construct | Initiation | Participatory Dialogue | Behavioral Confidence | Changes in the Physical Environment |
| 1. Initiation | – | 0.606 ** (p < 0.001) | 0.762 ** (p < 0.001) | 0.587 ** (p < 0.001) |
| 2. Participatory dialogue advantages–disadvantages | – | 0.568 ** (p < 0.001) | 0.361 ** (p < 0.001) | |
| 3. Behavioral confidence | – | 0.696 ** (p < 0.001) | ||
| 4. Changes in the physical environment | – | |||
| Vaccine-Hesitant Individuals (n = 84) | ||||
| Construct | Sustenance | Emotional Transformation | Practice for Change | Changes in the Social Environment |
| 1. Sustenance | – | 0.530 ** (p < 0.001) | 0.382 ** (p < 0.001) | 0.248 * (p = 0.025) |
| 2. Emotional transformation | – | 0.541 ** (p < 0.001) | 0.327 ** (p = 0.003) | |
| 3. Practice for change | – | 0.687 ** (p < 0.001) | ||
| 4. Changes in the social environment | – | |||
| Vaccine Non-Hesitant Individuals (n = 147) | ||||
| Construct | Sustenance | Emotional Transformation | Practice for Change | Changes in the Social Environment |
| 1. Sustenance | – | 0.816 ** (p < 0.001) | 0.632 ** (p < 0.001) | 0.658 ** (p < 0.001) |
| 2. Emotional transformation | – | 0.789 ** (p < 0.001) | 0.807 ** (p < 0.001) | |
| 3. Practice for change | – | 0.859 ** (p < 0.001) | ||
| 4. Changes in the social environment | – | |||
| Hesitant Participants | b | S.E. | β | p | LBCI | UBCI |
| Age | 0.003 | 0.006 | 0.035 | 0.623 | −0.009 | 0.015 |
| Mexican (reference: non-Mexican) | −0.040 | 0.164 | −0.017 | 0.807 | −0.367 | 0.287 |
| Female (reference: male) | 0.129 | 0.184 | 0.051 | 0.485 | −0.238 | 0.496 |
| Some college (reference: high school education or less, or bachelor’s degree and higher) | −0.042 | 0.172 | −0.018 | 0.809 | −0.385 | 0.302 |
| Catholicism (reference: non-Catholicism) | −0.004 | 0.192 | −0.001 | 0.985 | −0.387 | 0.379 |
| USD 25,000 to USD 49,999 (reference: lower and higher income than USD 25,000 to USD 49,999) | 0.486 | 0.175 | 0.193 | 0.007 | 0.136 | 0.835 |
| Employed (reference: other employment or non-employed) | 0.099 | 0.165 | 0.042 | 0.550 | −0.230 | 0.428 |
| Participatory dialogue advantages–disadvantages | 0.113 | 0.021 | 0.461 | <0.001 | 0.071 | 0.155 |
| Behavioral confidence | 0.358 | 0.059 | 0.503 | <0.001 | 0.241 | 0.475 |
| Changes in the physical environment | −0.032 | 0.019 | −0.135 | 0.099 | −0.069 | 0.006 |
| Model statistics including predictors of covariates, participatory dialogue, and behavioral confidence: R2 = 0.671, adjusted R2 = 0.630, F(9,73) = 16.520, p < 0.001 | ||||||
| Non-Hesitant Participants | b | S.E. | Β | p | LBCI | UBCI |
| Age | 0.017 | 0.006 | 0.172 | 0.003 | 0.006 | 0.028 |
| Mexican (reference: non-Mexican) | −0.003 | 0.159 | −0.001 | 0.983 | −0.318 | 0.311 |
| Female (reference: male) | 0.093 | 0.159 | 0.031 | 0.557 | −0.220 | 0.407 |
| Some college (reference: high school education or less, or bachelor’s degree and higher) | −0.017 | 0.159 | −0.006 | 0.915 | −0.330 | 0.297 |
| Catholicism (reference: non-Catholicism) | −0.057 | 0.152 | −0.020 | 0.707 | −0.357 | 0.243 |
| USD 25,000 to USD 49,999 (reference: lower and higher income than USD 25,000 to USD 49,999) | 0.124 | 0.149 | 0.044 | 0.408 | −0.171 | 0.419 |
| Employed (reference: other employment or non-employed) | 0.175 | 0.156 | 0.062 | 0.263 | −0.133 | 0.483 |
| Participatory dialogue advantages–disadvantages | 0.072 | 0.018 | 0.249 | <0.001 | 0.035 | 0.108 |
| Behavioral confidence | 0.206 | 0.034 | 0.502 | <0.001 | 0.139 | 0.274 |
| Changes in the physical environment | 0.031 | 0.019 | 0.116 | 0.109 | −0.007 | 0.069 |
| Model statistics including predictors of covariates, participatory dialogue, and behavioral confidence: R2 = 0.656, adjusted R2 = 0.632, F(9,132) = 27.959, p < 0.001 | ||||||
| Hesitant Participants | b | S.E. | β | p | LBCI | UBCI |
| Age | −0.019 | 0.006 | −0.275 | 0.004 | −0.032 | −0.006 |
| Mexican (reference: non-Mexican) | 0.129 | 0.185 | 0.066 | 0.487 | −0.239 | 0.497 |
| Female (reference: male) | −0.212 | 0.209 | −0.100 | 0.314 | −0.628 | 0.205 |
| Some college (reference: high school education or less, or bachelor’s degree and higher) | −0.269 | 0.181 | −0.137 | 0.140 | −0.630 | 0.091 |
| Catholicism (reference: non-Catholicism) | 0.097 | 0.211 | 0.045 | 0.646 | −0.323 | 0.518 |
| USD 25,000 to USD 49,999 (reference: lower and higher income than USD 25,000 to USD 49,999) | −0.115 | 0.194 | −0.055 | 0.554 | −0.501 | 0.271 |
| Employed (reference: other employment or non-employed) | 0.079 | 0.189 | 0.040 | 0.679 | −0.299 | 0.456 |
| Emotional transformation | 0.087 | 0.020 | 0.470 | <0.001 | 0.046 | 0.127 |
| Practice for change | 0.018 | 0.023 | 0.114 | 0.416 | −0.027 | 0.063 |
| Changes in the social environment | −0.004 | 0.032 | −0.017 | 0.890 | −0.067 | 0.058 |
| Model statistics including predictors of covariates and emotional transformation: R2 = 0.436, adjusted R2 = 0.374, F(8,73) = 7.045, p < 0.001 | ||||||
| Non-Hesitant Participants | b | S.E. | β | p | LBCI | UBCI |
| Age | 0.006 | 0.006 | 0.061 | 0.294 | −0.006 | 0.018 |
| Mexican (reference: non-Mexican) | −0.157 | 0.164 | −0.048 | 0.341 | −0.481 | 0.167 |
| Female (reference: male) | −0.111 | 0.162 | −0.035 | 0.492 | −0.432 | 0.209 |
| Some college (reference: high school education or less, or bachelor’s degree and higher) | 0.089 | 0.167 | 0.030 | 0.594 | −0.241 | 0.419 |
| Catholicism (reference: non-Catholicism) | 0.146 | 0.157 | 0.048 | 0.356 | −0.166 | 0.457 |
| USD 25,000 to USD 49,999 (reference: lower and higher income than USD 25,000 to USD 49,999) | 0.212 | 0.153 | 0.071 | 0.166 | −0.090 | 0.515 |
| Employed (reference: other employment or non-employed) | 0.129 | 0.160 | 0.043 | 0.421 | −0.187 | 0.446 |
| Emotional transformation | 0.177 | 0.019 | 0.850 | <0.001 | 0.139 | 0.215 |
| Practice for change | −0.015 | 0.028 | −0.054 | 0.606 | −0.070 | 0.041 |
| Changes in the social environment | 0.000 | 0.048 | −0.001 | 0.994 | −0.096 | 0.095 |
| Model statistics including predictors of covariates and emotional transformation: R2 = 0.683, adjusted R2 = 0.664, F(8,133) = 35.801, p =< 0.001 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nerida, T.M.; Sharma, M.; Labus, B.; Marquez, E.; Dai, C.-L. COVID-19 Vaccine Acceptance Behavior among Hispanics/Latinxs in Nevada: A Theory-Based Analysis. Healthcare 2023, 11, 688. https://doi.org/10.3390/healthcare11050688
Nerida TM, Sharma M, Labus B, Marquez E, Dai C-L. COVID-19 Vaccine Acceptance Behavior among Hispanics/Latinxs in Nevada: A Theory-Based Analysis. Healthcare. 2023; 11(5):688. https://doi.org/10.3390/healthcare11050688
Chicago/Turabian StyleNerida, Tara Marie, Manoj Sharma, Brian Labus, Erika Marquez, and Chia-Liang Dai. 2023. "COVID-19 Vaccine Acceptance Behavior among Hispanics/Latinxs in Nevada: A Theory-Based Analysis" Healthcare 11, no. 5: 688. https://doi.org/10.3390/healthcare11050688
APA StyleNerida, T. M., Sharma, M., Labus, B., Marquez, E., & Dai, C.-L. (2023). COVID-19 Vaccine Acceptance Behavior among Hispanics/Latinxs in Nevada: A Theory-Based Analysis. Healthcare, 11(5), 688. https://doi.org/10.3390/healthcare11050688