
Intensity Differences of Resistance Training for Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Retrieval Strategies
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Extraction and Literature Quality Assessment
2.4. Subgroup Division
2.5. Data Analysis
3. Results
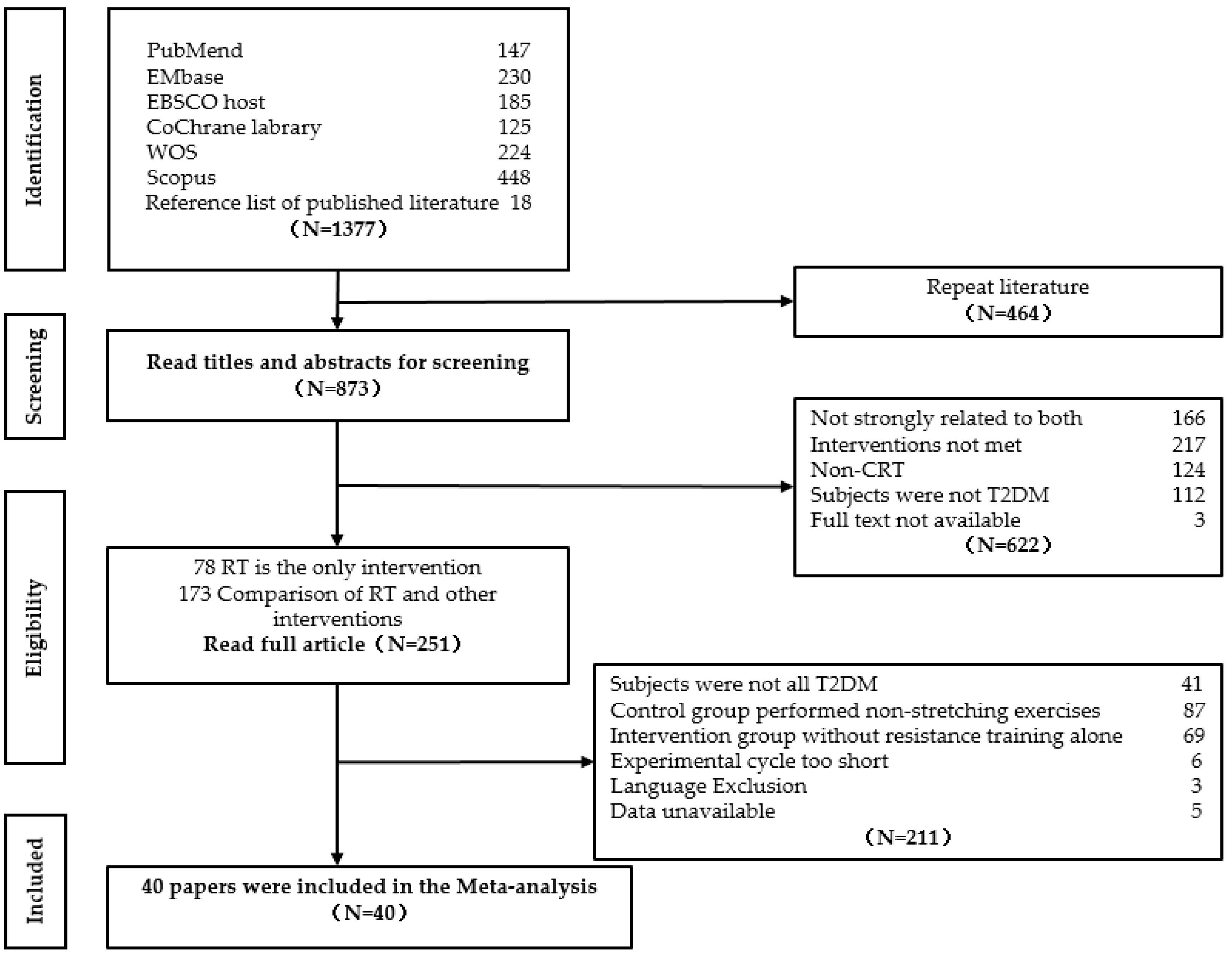
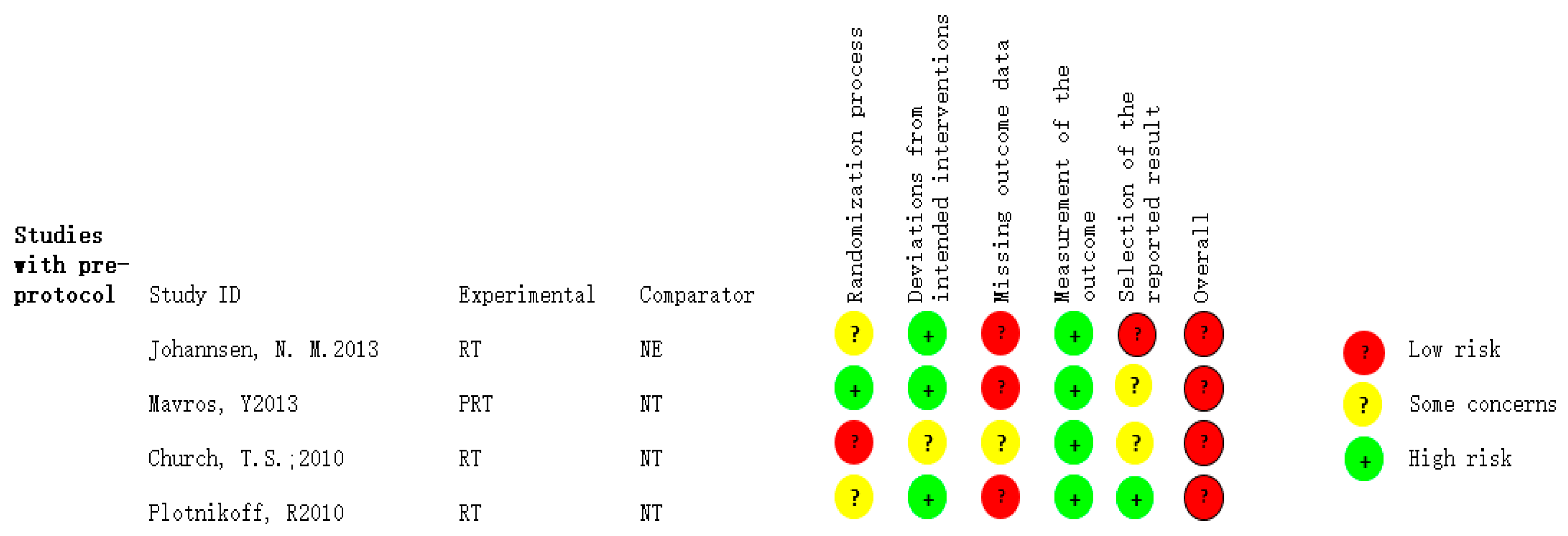
3.1. Literature Screening and Quality Assessment
3.2. Effect of Different Intensities of Resistance Training on the Adjunctive Therapy of Type 2 Diabetes Patients
3.2.1. Blood Glucose Indicators
3.2.2. Blood Lipid Indicators
3.2.3. Blood Pressure
3.2.4. Cardiopulmonary Function Indicators
3.2.5. Anthropometrical Indicators
3.2.6. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
| Search Strategy | Number | |
| #1 | “Diabetes Mellitus, Type 2”[Mesh] OR (Diabetes Mellitus, Noninsulin-Dependent[Title/Abstract]) OR (Diabetes Mellitus, Ketosis-Resistant[Title/Abstract]) OR (Diabetes Mellitus, Ketosis Resistant[Title/Abstract]) OR (Ketosis-Resistant Diabetes Mellitus[Title/Abstract]) OR (Diabetes Mellitus, Non Insulin Dependent[Title/Abstract]) OR (Diabetes Mellitus, Non-Insulin-Dependent[Title/Abstract]) OR (Non-Insulin-Dependent Diabetes Mellitus[Title/Abstract]) OR (Diabetes Mellitus, Stable[Title/Abstract]) OR (Stable Diabetes Mellitus[Title/Abstract]) OR (Diabetes Mellitus, Type II[Title/Abstract]) OR (NIDDM[Title/Abstract]) OR (Diabetes Mellitus, Noninsulin Dependent[Title/Abstract]) OR (Diabetes Mellitus, Maturity-Onset[Title/Abstract]) OR (Diabetes Mellitus, Maturity Onset[Title/Abstract]) OR (Maturity-Onset Diabetes Mellitus[Title/Abstract]) OR (Maturity Onset Diabetes Mellitus[Title/Abstract]) OR (MODY[Title/Abstract]) OR (Diabetes Mellitus, Slow-Onset[Title/Abstract]) OR (Diabetes Mellitus, Slow Onset[Title/Abstract]) OR (Slow-Onset Diabetes Mellitus[Title/Abstract]) OR (Type 2 Diabetes Mellitus[Title/Abstract]) OR (Noninsulin-Dependent Diabetes Mellitus[Title/Abstract]) OR (Noninsulin Dependent Diabetes Mellitus[Title/Abstract]) OR (Maturity-Onset Diabetes[Title/Abstract]) OR (Diabetes, Maturity-Onset[Title/Abstract]) OR (Maturity Onset Diabetes[Title/Abstract]) OR (Type 2 Diabetes[Title/Abstract]) OR (Diabetes, Type 2[Title/Abstract]) OR (Diabetes Mellitus, Adult-Onset[Title/Abstract]) OR (Adult-Onset Diabetes Mellitus[Title/Abstract]) OR (Diabetes Mellitus, Adult Onset[Title/Abstract]) | 212,413 |
| #2 | (“Resistance Training”[Mesh] OR (Training, Resistance[Title/Abstract]) OR (Strength Training[Title/Abstract]) OR (Training, Strength[Title/Abstract]) OR (Weight-Lifting Strengthening Program[Title/Abstract]) OR (Strengthening Program, Weight-Lifting[Title/Abstract]) OR (Strengthening Programs, Weight-Lifting[Title/Abstract]) OR (Weight Lifting Strengthening Program[Title/Abstract]) OR (Weight-Lifting Strengthening Programs[Title/Abstract]) OR (Weight-Lifting Exercise Program[Title/Abstract]) OR (Exercise Program, Weight-Lifting[Title/Abstract]) OR (Exercise Programs, Weight-Lifting[Title/Abstract]) OR (Weight Lifting Exercise Program[Title/Abstract]) OR (Weight-Lifting Exercise Programs[Title/Abstract]) OR (Weight-Bearing Strengthening Program[Title/Abstract]) OR (Strengthening Program, Weight-Bearing[Title/Abstract]) OR (Strengthening Programs, Weight-Bearing[Title/Abstract]) OR (Weight Bearing Strengthening Program[Title/Abstract]) OR (Weight-Bearing Strengthening Programs[Title/Abstract]) OR (Weight-Bearing Exercise Program[Title/Abstract]) OR (Exercise Program, Weight-Bearing[Title/Abstract]) OR (Exercise Programs, Weight-Bearing[Title/Abstract]) OR (Weight Bearing Exercise Program[Title/Abstract]) OR (Weight-Bearing Exercise Programs[Title/Abstract]) | 15,575 |
| #3 | #1 AND #2 | 391 |
| #4 | #3 Filters: Randomized Controlled Trial | 147 |
| Search Strategy | Number | |
| #1 | ‘non insulin dependent diabetes mellitus’/exp | 299,169 |
| #2 | ‘resistance training’/exp | 23,271 |
| #3 | #1 AND #2 | 994 |
| #4 | #3 AND ‘randomized controlled trial’/de | 230 |
| Search Strategy | Number | |
| S1 | DE “Exercise” OR DE “Physical Activity” OR DE “Aerobic Exercise” OR DE “Weightlifting” OR DE “Yoga” OR DE “Exercise Dependence” OR DE “Health Behavior” OR DE “Kinesiology” OR DE “Movement Therapy” OR DE “Physical Fitness” OR DE “Sport and Exercise Measures” OR DE “Sport Psychology” OR DE “Wearable Devices” OR DE “Weight Control” | 1,021,010 |
| S2 | DE “Type 2 Diabetes” OR DE “Blood Sugar” | 135,774 |
| S3 | S1 AND S2 | 7472 |
| S4 | randomized controlled trials→Update | 185 |
| Search Strategy | Number | |
| #1 | MeSH descriptor: [Resistance Training] explode all trees | 4073 |
| #2 | MeSH descriptor: [Diabetes Mellitus, Type 2] explode all trees | 19,666 |
| #3 | #1 AND #2 | 125 |
| #4 | Trials | 125 |
| Search Strategy | Number | |
| (1) | TS = (non insulin dependent diabetes mellitus) OR TS = (Diabetes Mellitus Type 2) | 16,147 |
| (2) | TS = (resistance training)OR TS = (resistance exercise) | 7122 |
| (3) | (TS = (non insulin dependent diabetes mellitus) OR TS = (Diabetes Mellitus Type 2)) AND (TS = (resistance training)OR TS = (resistance exercise)) AND TS = (randomized controlled trials) | 335 |
| (4) | Refine:(Article) | 224 |
| Search Strategy | Number |
| TITLE-ABS-KEY(‘non insulin dependent diabetes mellitus’ OR ‘Diabetes Mellitus Type 2’) | 174,313 |
| TITLE-ABS-KEY(‘resistance training’ OR ‘resistance exercise’) | 50,934 |
| TITLE-ABS-KEY((‘resistance training’ OR ‘resistance exercise’) AND (‘non insulin dependent diabetes mellitus’ OR ‘diabetes mellitus type 2’)) | 3246 |
| TITLE-ABS-KEY((‘resistance training’ OR ‘resistance exercise’) AND (‘non insulin dependent diabetes mellitus’ OR ‘Diabetes Mellitus Type 2’)) AND (LIMIT-TO (EXACTKEYWORD,”Randomized Controlled Trial” ) ) | 448 |
References
- Dagenais, G.R.; Gerstein, H.C.; Zhang, X.; McQueen, M.; Lear, S.; Lopez-Jaramillo, P.; Mohan, V.; Mony, P.; Gupta, R.; Kutty, V.R. Variations in diabetes prevalence in low-, middle-, and high-income countries: Results from the prospective urban and rural epidemiological study. Diabetes Care 2016, 39, 780–787. [Google Scholar]
- COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 28 July 2022).
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar]
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Myers, J.; Atwood, J.E.; Froelicher, V. Active lifestyle and diabetes. Am. Heart Assoc. 2003, 107, 2392–2394. [Google Scholar] [CrossRef]
- Chudyk, A.; Petrella, R.J. Effects of exercise on cardiovascular risk factors in type 2 diabetes: A meta-analysis. Diabetes Care 2011, 34, 1228–1237. [Google Scholar]
- Thomas, D.; Elliott, E.J.; Naughton, G.A. Exercise for type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2006, 2006, CD002968. [Google Scholar]
- Liu, Y.; Ye, W.; Chen, Q.; Zhang, Y.; Kuo, C.-H.; Korivi, M. Resistance exercise intensity is correlated with attenuation of HbA1c and insulin in patients with type 2 diabetes: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 140. [Google Scholar] [CrossRef]
- Ishiguro, H.; Kodama, S.; Horikawa, C.; Fujihara, K.; Hirose, A.S.; Hirasawa, R.; Yachi, Y.; Ohara, N.; Shimano, H.; Hanyu, O. In search of the ideal resistance training program to improve glycemic control and its indication for patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Sport. Med. 2016, 46, 67–77. [Google Scholar] [CrossRef]
- Hirano, T. Pathophysiology of diabetic dyslipidemia. J. Atheroscler. Thromb. 2018, 25, RV17023. [Google Scholar] [CrossRef]
- Yang, Z.; Scott, C.A.; Mao, C.; Tang, J.; Farmer, A.J. Resistance exercise versus aerobic exercise for type 2 diabetes: A systematic review and meta-analysis. Sport. Med. 2014, 44, 487–499. [Google Scholar] [CrossRef]
- Reaven, G.M.; Greenfield, M.S. Diabetic hypertriglyceridemia: Evidence for three clinical syndromes. Diabetes 1981, 30, 66–75. [Google Scholar]
- Ratamess, N. ACSM’s Foundations of Strength Training and Conditioning; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2021. [Google Scholar]
- One Rep Max Calculator. Available online: https://strengthlevel.com/one-rep-max-calculator (accessed on 30 July 2022).
- Johannsen, N.M.; Swift, D.L.; Lavie, C.J.; Earnest, C.P.; Blair, S.N.; Church, T.S. Categorical analysis of the impact of aerobic and resistance exercise training, alone and in combination, on cardiorespiratory fitness levels in patients with type 2 diabetes: Results from the HART-D study. Diabetes Care 2013, 36, 3305–3312. [Google Scholar]
- Plotnikoff, R.; Eves, N.; Jung, M.; Sigal, R.; Padwal, R.; Karunamuni, N. Multicomponent, home-based resistance training for obese adults with type 2 diabetes: A randomized controlled trial. Int. J. Obes. 2010, 34, 1733–1741. [Google Scholar]
- Mavros, Y.; Kay, S.; Anderberg, K.A.; Baker, M.K.; Wang, Y.; Zhao, R.; Meiklejohn, J.; Climstein, M.; O’Sullivan, A.; De Vos, N. Changes in insulin resistance and HbA1c are related to exercise-mediated changes in body composition in older adults with type 2 diabetes: Interim outcomes from the GREAT2DO trial. Diabetes Care 2013, 36, 2372–2379. [Google Scholar]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Mikus, C.R.; Myers, V.; Nauta, M.; Rodarte, R.Q. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: A randomized controlled trial. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef]
- Ramachandran, S.; Paul, J.; Sundaram, M.; Varalakshmi, S.; Sudhakar, S. Effects of whole-body Vibration therapy among Type II Diabetes Mellitus-A Pilot single blind randomized clinical trial. Res. J. Pharm. Technol. 2021, 14, 1465–1468. [Google Scholar]
- Sabouri, M.; Hatami, E.; Pournemati, P.; Shabkhiz, F. Inflammatory, antioxidant and glycemic status to different mode of high-intensity training in type 2 diabetes mellitus. Mol. Biol. Rep. 2021, 48, 5291–5304. [Google Scholar]
- Ranasinghe, C.; Devage, S.; Constantine, G.R.; Katulanda, P.; Hills, A.P.; King, N.A. Glycemic and cardiometabolic effects of exercise in South Asian Sri Lankans with type 2 diabetes mellitus: A randomized controlled trial Sri Lanka diabetes aerobic and resistance training study (SL-DARTS). Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 77–85. [Google Scholar] [CrossRef]
- Gholami, F.; Khaki, R.; Mirzaei, B.; Howatson, G. Resistance training improves nerve conduction and arterial stiffness in older adults with diabetic distal symmetrical polyneuropathy: A randomized controlled trial. Exp. Gerontol. 2021, 153, 111481. [Google Scholar] [CrossRef]
- Rezaeeshirazi, R. Aerobic versus resistance training: Leptin and metabolic parameters improvement in type 2 diabetes obese men. Res. Q. Exerc. Sport 2021, 93, 537–547. [Google Scholar] [CrossRef]
- Rad, M.M.; Bijeh, N.; Hosseini, S.R.A.; Saeb, A.R. The effect of two concurrent exercise modalities on serum concentrations of FGF21, irisin, follistatin, and myostatin in men with type 2 diabetes mellitus. Arch. Physiol. Biochem. 2020, 1–10. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Nagai, Y.; Kawanabe, S.; Hishida, Y.; Hiraki, K.; Sone, M.; Tanaka, Y. Effects of resistance training using elastic bands on muscle strength with or without a leucine supplement for 48 weeks in elderly patients with type 2 diabetes. Endocr. J. 2021, 68, 291–298. [Google Scholar]
- Mogharnasi, M.; TajiTabas, A.; Tashakorizadeh, M.; Nayebifar, S. The Effects of resistance and endurance training on levels of nesfatin-1, HSP70, insulin resistance and body composition in women with type 2 diabetes mellitus. Sci. Sport. 2019, 34, e15–e23. [Google Scholar]
- Hsieh, P.-L.; Tseng, C.-H.; Tseng, Y.J.; Yang, W.-S. Resistance training improves muscle function and cardiometabolic risks but not quality of life in older people with type 2 diabetes mellitus: A randomized controlled trial. J. Geriatr. Phys. Ther. 2018, 41, 65–76. [Google Scholar] [CrossRef]
- Botton, C.E.; Umpierre, D.; Rech, A.; Pfeifer, L.O.; Machado, C.L.; Teodoro, J.L.; Dias, A.S.; Pinto, R.S. Effects of resistance training on neuromuscular parameters in elderly with type 2 diabetes mellitus: A randomized clinical trial. Exp. Gerontol. 2018, 113, 141–149. [Google Scholar] [CrossRef]
- AminiLari, Z.; Fararouei, M.; Amanat, S.; Sinaei, E.; Dianatinasab, S.; AminiLari, M.; Daneshi, N.; Dianatinasab, M. The effect of 12 weeks aerobic, resistance, and combined exercises on omentin-1 levels and insulin resistance among type 2 diabetic middle-aged women. Diabetes Metab. J. 2017, 41, 205. [Google Scholar] [CrossRef]
- Shabani, R.; Nazari, M.; Dalili, S.; Rad, A.H. Effect of circuit resistance training on glycemic control of females with diabetes Type II. Int. J. Prev. Med. 2015, 6, 34. [Google Scholar]
- Mahdirejei, H.A.; Abadei, S.F.R.; Seidi, A.A.; Gorji, N.E.; Kafshgari, H.R.; Pour, M.E.; Khalili, H.B.; Hajeizad, F.; Khayeri, M. Effects of an eight-week resistance training on plasma vaspin concentrations, metabolic parameters levels and physical fitness in patients with type 2 diabetes. Cell J. 2014, 16, 367. [Google Scholar]
- Kadoglou, N.; Fotiadis, G.; Kapelouzou, A.; Kostakis, A.; Liapis, C.; Vrabas, I. The differential anti-inflammatory effects of exercise modalities and their association with early carotid atherosclerosis progression in patients with type 2 diabetes. Diabet. Med. 2013, 30, e41–e50. [Google Scholar]
- Oliveira, V.N.D.; Bessa, A.; Jorge, M.L.M.P.; Oliveira, R.J.D.S.; de Mello, M.T.; De Agostini, G.G.; Jorge, P.T.; Espindola, F.S. The effect of different training programs on antioxidant status, oxidative stress, and metabolic control in type 2 diabetes. Appl. Physiol. Nutr. Metab. 2012, 37, 334–344. [Google Scholar]
- Kadoglou, N.P.; Fotiadis, G.; Athanasiadou, Z.; Vitta, I.; Lampropoulos, S.; Vrabas, I.S. The effects of resistance training on ApoB/ApoA-I ratio, Lp (a) and inflammatory markers in patients with type 2 diabetes. Endocrine 2012, 42, 561–569. [Google Scholar] [CrossRef]
- Hameed, U.A.; Manzar, D.; Raza, S.; Shareef, M.Y.; Hussain, M.E. Resistance training leads to clinically meaningful improvements in control of glycemia and muscular strength in untrained middle-aged patients with type 2 diabetes mellitus. N. Am. J. Med. Sci. 2012, 4, 336. [Google Scholar]
- Yavari, A.; Najafipoor, F.; Aliasgarzadeh, A.; Niafar, M.; Mobasseri, M. Effect of aerobic exercise, resistance training or combined training on glycaemic control and cardio-vascular risk factors in patients with type 2 diabetes. Biol. Sport 2012, 29, 135–143. [Google Scholar]
- Jorge, M.L.M.P.; de Oliveira, V.N.; Resende, N.M.; Paraiso, L.F.; Calixto, A.; Diniz, A.L.D.; Resende, E.S.; Ropelle, E.R.; Carvalheira, J.B.; Espindola, F.S. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adipocytokines, and muscle insulin signaling in patients with type 2 diabetes mellitus. Metabolism 2011, 60, 1244–1252. [Google Scholar]
- Larose, J.; Sigal, R.J.; Khandwala, F.; Prud’homme, D.; Boulé, N.; Kenny, G.P. Associations between physical fitness and HbA1c in type 2 diabetes mellitus. Diabetologia 2011, 54, 93–102. [Google Scholar]
- Kwon, H.R.; Min, K.W.; Ahn, H.J.; Seok, H.G.; Lee, J.H.; Park, G.S.; Han, K.A. Effects of aerobic exercise vs. resistance training on endothelial function in women with type 2 diabetes mellitus. Diabetes Metab. J. 2011, 35, 364–373. [Google Scholar]
- Hazley, L.; Ingle, L.; Tsakirides, C.; Carroll, S.; Nagi, D. Impact of a short-term, moderate intensity, lower volume circuit resistance training programme on metabolic risk factors in overweight/obese type 2 diabetics. Res. Sport. Med. 2010, 18, 251–262. [Google Scholar] [CrossRef]
- Ku, Y.; Han, K.; Ahn, H.; Kwon, H.; Koo, B.; Kim, H.; Min, K. Resistance exercise did not alter intramuscular adipose tissue but reduced retinol-binding protein-4 concentration in individuals with type 2 diabetes mellitus. J. Int. Med. Res. 2010, 38, 782–791. [Google Scholar] [CrossRef]
- Gavin, C.; Sigal, R.J.; Cousins, M.; Menard, M.L.; Atkinson, M.; Khandwala, F.; Kenny, G.P.; Proctor, S.; Ooi, T.C. Resistance exercise but not aerobic exercise lowers remnant-like lipoprotein particle cholesterol in type 2 diabetes: A randomized controlled trial. Atherosclerosis 2010, 213, 552–557. [Google Scholar]
- Wycherley, T.P.; Noakes, M.; Clifton, P.M.; Cleanthous, X.; Keogh, J.B.; Brinkworth, G.D. A high-protein diet with resistance exercise training improves weight loss and body composition in overweight and obese patients with type 2 diabetes. Diabetes Care 2010, 33, 969–976. [Google Scholar]
- Arora, E.; Shenoy, S.; Sandhu, J. Effects of resistance training on metabolic profile of adults with type 2 diabetes. Indian J. Med. Res. 2009, 129, 515. [Google Scholar]
- Cheung, N.; Cinnadaio, N.; Russo, M.; Marek, S. A pilot randomised controlled trial of resistance exercise bands in the management of sedentary subjects with type 2 diabetes. Diabetes Res. Clin. Pract. 2009, 83, e68–e71. [Google Scholar] [CrossRef]
- Larose, J. The Effect of Exercise Training on Physical Fitness in type 2 Diabetes Mellitus. Master’s Thesis, University of Ottawa, Ottawa, ON, Canada, 2009. [Google Scholar]
- Shenoy, S.; Arora, E.; Jaspal, S. Effects of progressive resistance training and aerobic exercise on type 2 diabetics in Indian population. Int. J. Diabetes Metab. 2009, 17, 27–30. [Google Scholar]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 357–369. [Google Scholar]
- Baum, K.; Votteler, T.; Schiab, J. Efficiency of vibration exercise for glycemic control in type 2 diabetes patients. Int. J. Med. Sci. 2007, 4, 159. [Google Scholar] [CrossRef]
- Brooks, N.; Layne, J.E.; Gordon, P.L.; Roubenoff, R.; Nelson, M.E.; Castaneda-Sceppa, C. Strength training improves muscle quality and insulin sensitivity in Hispanic older adults with type 2 diabetes. Int. J. Med. Sci. 2007, 4, 19. [Google Scholar] [CrossRef]
- Castaneda, C.; Layne, J.E.; Munoz-Orians, L.; Gordon, P.L.; Walsmith, J.; Foldvari, M.; Roubenoff, R.; Tucker, K.L.; Nelson, M.E. A randomized controlled trial of resistance exercise training to improve glycemic control in older adults with type 2 diabetes. Diabetes Care 2002, 25, 2335–2341. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Puddey, I.B.; Beilin, L.J.; Burke, V.; Morton, A.R.; Stanton, K. Effects of a short-term circuit weight training program on glycaemic control in NIDDM. Diabetes Res. Clin. Pract. 1998, 40, 53–61. [Google Scholar]
- Ishii, T.; Yamakita, T.; Sato, T.; Tanaka, S.; Fujii, S. Resistance training improves insulin sensitivity in NIDDM subjects without altering maximal oxygen uptake. Diabetes Care 1998, 21, 1353–1355. [Google Scholar] [CrossRef]
- Honkola, A.; Forsen, T.; Eriksson, J. Resistance training improves the metabolic profile in individuals with type 2 diabetes. Acta Diabetol. 1997, 34, 245–248. [Google Scholar]
- Reid, R.; Tulloch, H.; Sigal, R.; Kenny, G.; Fortier, M.; McDonnell, L.; Wells, G.; Boule, N.; Phillips, P.; Coyle, D. Effects of aerobic exercise, resistance exercise or both, on patient-reported health status and well-being in type 2 diabetes mellitus: A randomised trial. Diabetologia 2010, 53, 632–640. [Google Scholar]
- Gordon, P.; Vannier, E.; Hamada, K.; Layne, J.; Hurley, B.; Roubenoff, R.; Castaneda-Sceppa, C. Resistance training alters cytokine gene expression in skeletal muscle of adults with type 2 diabetes. Int. J. Immunopathol. Pharmacol. 2006, 19, 739–749. [Google Scholar] [CrossRef]
- Holten, M.K.; Zacho, M.; Gaster, M.; Juel, C.; Wojtaszewski, J.F.; Dela, F. Strength training increases insulin-mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes. Diabetes 2004, 53, 294–305. [Google Scholar] [CrossRef]
- Wang, L. Genetic and Dietary Effects on Physical Properties, Assembly and Secretion of apoB-Containing Lipoproteins; Texas A&M University: College Station, TX, USA, 2003. [Google Scholar]
- Pastor-Barriuso, R.; Banegas, J.R.; Damin, J.; Appel, L.J.; Guallar, E. Systolic blood pressure, diastolic blood pressure, and pulse pressure: An evaluation of their joint effect on mortality. Ann. Intern. Med. 2003, 139, 731–739. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Country | RT /CN | Female % | Age (Year) | HbA1C (%) | Intensity %1RM | Repetition (Times) | Set | Frequency (t/wk) | Duration (k) | Outcome Indicators |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ramachandran et al. [21] | India | 12/12 | - | 51.4 ± 2.2 | 8.34 ± 0.67 | 70–80↑ | 12 | 2 | 3 | 12 | a.e.g.h. |
| Sabouri et al. [22] | Iran | 15/13 | 53.6 | 51.76 ± 3.92 | 7.52 ± 0.88 | 80↑ | 8 | 3 | 3 | 12 | n.s.m.k.i.j.d.b.c.a.e.f.g.h. |
| Ranasinghe et al. [23] | Sri Lanka | 27/28 | 50 | 49.16 ± 8.13 | 8.27 ± 1.7 | 81↑ | 8 | 3 | 2 | 12 | d.a.b.c.e.f.g.h.i.j.n.s.o.q.r. |
| Gholami et al. [24] | Iran | 15/14 | 0 | 63.48 ± 3 | 9.51 ± 1.82 | ≥50↓ | 10–15 | 1–3 | 2–3 | 12 | a. |
| Rezaeeshirazi et al. [25] | Iran | 14/15 | 0 | 21.9 ± 1.97 | ≥2 years | 50–70↓ | 8–15 ii | 3 | 4 | 8 | d.b.c.m.s.r.q.o.n. |
| Motahari et al. [26] | Iran | 15/13 | - | 44.33 ± 2.81 | 8.1 ± 0.8 | 40–80↓ | 8–18 ii | 3 | 3 | 12 | n.s.m.r.c.a. |
| Yamamoto et al. [27] | Japan | 18/17 | 45.7 | 73.25 ± 2.55 | 7.21 ± 0.81 | Medium-low↓ | 20 | 15 Min | 7 | 48 | a.s. |
| Mogharnasi et al. [28] | Iran | 10/8 | 100 | 48.52 ± 7.06 | ≥3 years | 30–80↓ | 10–18 ii | 3 | 3 | 10 | n.s.p.r.m.d.b.c. |
| Hsieh et al. [29] | China | 14/15 | 63.3 | 71.2 ± 4.4 | 7.25 ± 0.76 | 40–75↓ | 8–12 | 3 | 3 | 12 | m.l.i.j.n.r.o.d.a.e.f.g.h. |
| Botton et al. [30] | Brazil | 13/13 | 40.9 | 69.6 ± 6.9 | 7.07 ± 0.67 | 67 i↓ | 12 | 3 | 3 | 12 | a.d.e.f.g.h. |
| AminiLari et al. [31] | Iran | 12/15 | 100 | 45–60 | ≥2 years | 50–55↓ | 8 | 3 | 3 | 12 | n.s.r.d.b. |
| Shabani et al. [32] | Iran | 10/10 | 100 | 50.75 ± 5.83 | 7.45 ± 1.43 | 40–65↓ | 8–12 | 1–3 iii | 3 | 8 | n.s.p.a.d. |
| Mahdirejei et al. [33] | Iran | 9/9 | 0 | 48.61 ± 7.88 | 7.96 ± 1.62 | 50–80↓ | 8–15 ii | 3 | 3 | 8 | n.s.r.p.m.e.f.g.h.d.a.b.c |
| Kadoglou et al. [34] | Greece | 23/24 | 70.2 | 57 ± 6.3 | 7.9 ± 0.75 | 60–80↓ | 8–10 | 2–3 | 4 | 24 | s.p.i.j.m.d.a.e.f.g.h.b.c.r |
| Oliveira et al. [35] | Brazil | 10/12 | 63.6 | 53.7 ± 9.4 | 7.71 ± 1.73 | ≥50↓ | 8–12 | 4 | 3 | 12 | d.a.e.f.g.h.n.q.o.p.m.i.j.r. |
| Kadoglou et al. [36] | Greece | 23/24 | 74.5 | 63.08 ± 4.87 | 7.45 ± 0.45 | 60–80↓ | 6–8 | 2–3 | 3 | 12 | s.p.i.j.a.d.e.f.g.h.b.c.m.r. |
| Hameed et al. [37] | India | 24/24 | 27.08 | 44.7 ± 4.9 | 8.4 ± 0.8 | 65–70↓ | 10 | 3 | 2–3 | 8 | a.n.o.e.f.g.h.i.j. |
| Yavari et al. [38] | Iran | 20/20 | 53.75 | 51.5 ± 7.48 | 7.5 ± 0.89 | 75–80↑ | 8–10 | 3 | 3 | 52 | a.d.e.f.g.h.n.s.r.i.j.l.m. |
| Jorge et al. [39] | Brazil | 12/12 | 62.5 | 53.8 ± 9.4 | 7.63 ± 1.79 | 89–94↑ | 10 | 2 | 3 | 12 | s.p.m.i.j.a.d.f.g.c.e. |
| Larose et al. [40] | Canada | 64/63 | 36.2 | 54.75 ± 58.6 | 7.69 ± 6.97 | 80 i↑ | 8 | 2 | 2–3 | 22 | a.n.s.m. |
| Kwon et al. [41] | Seoul, Korea | 12/15 | - | 57.74 ± 5.88 | 7.23 ± 0.79 | 40–50↓ | 10–15 ii | 3 | 3 | 12 | n.a.b.e.f.g.h. |
| Hazley et al. [42] | Britain | 6/6 | 41.7 | 54 ± 9 | 7.3 ± 0.95 | 50–60↓ | 15 | 3 | 2 | 8 | s.o.p.l.d.a.e.f.g.h.b.c.i.j. |
| Ku et al. [43] | Korea | 13/16 | 100 | 56.86 ± 7.32 | 7.3 ± 0.8 | 40–50↓ | 15–20 ii | 3 | 5 | 12 | n.s.o.a.d. |
| Gavin et.al. [44] | Canada | 64/63 | 34.6 | 54.75 ± 7.35 | 7.69 ± 0.88 | 80 i↑ | 8 | 2 | 2–3 | 22 | e.a.g.h. |
| Wycherley et al. [45] | Australia | 17/16 | - | 55.0 ± 8.4 | 7.45 ± 1.2 | 70–85↑ | 12 | 2 | 3 | 16 | n.s.q.o.i.j.d.a.b.e.f.g.h. |
| Arora et al. [46] | India | 9/10 | 50 | 54 ± 3.9 | 7.67 ± 1.18 | 70–80↑ | 10 | 3 | 2 | 8 | a.g.e.f.i.j.l.s. |
| Cheung et al. [47] | Australia | 20/17 | 67.6 | 60.38 ± 7.85 | 7.31 ± 1.36 | 67 i↓ | 12 | 2 | 5 | 16 | a.s.o. |
| Larose et al. [48] | Canada | 64/63 | 36.2 | 54.75 ± 7.35 | 7.69 ± 0.88 | 80 i↑ | 8 | 2 | 2–3 | 22 | k. |
| Shenoy et al. [49] | India | 10/10 | 40 | 54 ± 3.89 | 7.67 ± 0.41 | 60–100↑ | 10 | 3 | 2 | 16 | a.d.i.j.l. |
| Sigal et al. [50] | Canada | 56/59 | 37.5 | 54.75 ± 7.35 | 7.69 ± 0.88 | 81↑ | 8 | 2–3 | 3 | 22 | a.i.j.e.f.g.h.n.o.q.r.s. |
| Baum et al. [51] | Germany | 13/13 | 40 | 63.1 ± 6.64 | - | 70–80↑ | 12 | 3 | 3 | 36 | d. |
| Brooks et al. [52] | USA | 31/31 | 35.48 | 66 ± 1.58 | 8.55 ± 0.3 | 70–80↑ | 8 | 3 | 3 | 16 | a. |
| Castaneda et al. [53] | USA | 29/31 | 64.5 | 66 ± 1.58 | 8.55 ± 0.3 | 60–80↓ | 8 | 3 | 3 | 16 | a.d.f.g.h.i.j.l |
| Dunstan et al. [54] | Australia | 11/10 | 38 | 50.68 ± 6.79 | 4.8 years | 50–55↓ | 10–15 | 2–3 | 3 | 8 | n.s.p.b.d.i.j.l.a. |
| Ishii et al. [55] | Japan | 9/8 | 0 | 49.2 ± 8.58 | 9.22 ± 2.5 | 40–50↓ | 10–20 | 2 | 5 | 6 | s.r. |
| Honkola et al. [56] | Finland | 18/20 | 55 | 64.63 ± 2 | 7.61 ± 1.31 | medium↓ | 12–15 | 2 | 2 | 20 | i.j.e.f.g.h.n.a. |
| Outcome | Participants RT/NT | Merger Effect Value MD 95%CI | Quantifying Heterogeneity | Test for Overall Effect | Between Groups | |
|---|---|---|---|---|---|---|
| I2 (%) | p | p | p | |||
| HbA1c (%) (30) | 616/624 | −0.41 [−0.64, −0.18] | 67 | <0.01 | <0.01 | |
| H | 377/377 | −0.49 [−0.73, −0.02] | 75 | <0.01 | 0.02 | 0.5268 |
| L-M | 239/247 | −0.33 [−0.75, −0.13] | 56 | <0.01 | 0.01 | |
| Insulin (ng/mL) (12) | 180/185 | −1.27 [−2.79, 0.26] | 77 | <0.01 | 0.10 | |
| H | 60/59 | −1.05 [−3.26, 1.15] | 0 | 0.68 | 0.35 | 0.8680 |
| L-M | 120/126 | −1.30 [−3.14, 0.55] | 83 | <0.01 | 0.17 | |
| HOMA-IR (10) | 155/154 | −0.82 [−1.46, −0.18] | 85 | <0.01 | 0.01 | |
| H | 55/55 | 0.11 [−0.40, −0.63] | 0 | 0.85 | 0.66 | 0.0085 |
| L-M | 100/99 | −1.09 [−1.83, −0.36] | 87 | <0.01 | <0.01 | |
| FBG (mmol/L) (21) | 307/317 | −0.52 [−1.00, −0.04] | 71 | 0.053 | 0.03 | |
| H | 119/121 | −0.23 [−1.37, 0.91] | 76 | <0.01 | 0.69 | 0.4958 |
| L-M | 188/196 | −0.66 [−1.18, −0.15] | 66 | <0.01 | 0.01 | |
| TG (mmol/L) (19) | 379/390 | −0.20 [−0.32, −0.08] | 30 | 0.10 | <0.01 | |
| H | 227/228 | −0.28 [−0.44, −0.12] | 0 | 0.88 | <0.01 | 0.1917 |
| L-M | 152/162 | −0.06 [−0.35, 0.22] | 55 | 0.02 | 0.67 | |
| TC (mmol/L) (17) | 274/286 | −0.26 [−0.42, −0.09] | 0 | 0.49 | <0.01 | |
| H | 108/107 | −0.32 [−0.56, −0.08] | 22 | 0.26 | <0.01 | 0.5884 |
| L-M | 166/179 | −0.20 [−0.43, 0.03] | 0 | 0.62 | 0.09 | |
| HDL-c (mmol/L) (20) | 406/420 | −0.02 [−0.06, 0.02] | 10 | 0.33 | 0.38 | |
| H | 240/241 | −0.01 [−0.06, 0.05] | 34 | 0.14 | 0.81 | 0.5243 |
| L-M | 166/179 | −0.03 [−0.09, 0.03] | 0 | 0.63 | 0.30 | |
| LDL-c (mmol/L) (18) | 386/399 | −0.18 [−0.30, −0.05] | 0 | 0.64 | <0.01 | |
| H | 206/206 | −0.19 [−0.35, −0.03] | 6 | 0.38 | 0.02 | 0.8697 |
| L-M | 180/193 | −0.16 [−0.34, 0.03] | 0 | 0.63 | 0.10 | |
| DBP (mmHg) (17) | 320/331 | −1.81 [−4.80, 1.19] | 81 | <0.01 | 0.24 | |
| H | 161/165 | −2.16 [−5.99, 1.66] | 81 | <0.01 | 0.27 | 0.7956 |
| L-M | 159/166 | −1.33 [−6.39, 3.74] | 83 | <0.01 | 0.61 | |
| SBP (mmHg) (17) | 320/331 | −6.83 [−11.50, −2.61] | 72 | <0.01 | <0.01 | |
| H | 161/165 | −4.36 [−9.74, 1.02] | 71 | <0.01 | 0.11 | 0.2350 |
| L-M | 159/166 | −9.53 [−16.15, −2.91] | 71 | <0.01 | <0.01 | |
| Rest HR (bpm) (6) | 88/91 | −3.42 [−8.92, 2.09] | 71 | <0.01 | 0.22 | |
| H | 33/35 | −3.42 [−8.92, 2.09] | 87 | <0.01 | 0.43 | 0.8661 |
| L-M | 55/56 | −2.71 [−8.05, 2.63] | 0 | 0.97 | 0.32 | |
| HRmax (bpm) (2) | 79/76 | −0.10 [−0.83, 0.63] | 0 | 0.81 | 0.80 | |
| H | 79/76 | −0.10 [−0.83, 0.63] | 0 | 0.81 | 0.80 | |
| L-M | ||||||
| VO2max (ml/kg) (12) | 225/221 | 0.62 [−0.99, 2.23] | 81 | <0.01 | 0.45 | |
| H | 121/116 | −0.25 [−3.00, 2.49] | 69 | 0.01 | 0.86 | 0.4154 |
| L-M | 104/105 | 1.13 [−0.77, 3.04] | 83 | <0.01 | 0.24 | |
| Weight (kg) (19) | 368/380 | 0.39 [−1.19, 1.97] | 0 | 0.64 | 0.63 | |
| H | 195/196 | 4.25 [0.27, 8.22] | 0 | 0.75 | 0.04 | 0.0382 |
| L-M | 173/184 | −0.33 [−2.05, 1.39] | 0 | 0.76 | 0.70 | |
| WC (cm) (10) | 202/208 | −0.75 [−2.24, 0.75] | 0 | 0.85 | 0.33 | |
| H | 100/103 | −1.49 [−5.55, 2.58] | 0 | 0.82 | 0.47 | 0.7006 |
| L-M | 102/105 | −0.63 [−2.24, 0.98] | 0 | 0.64 | 0.44 | |
| WHR (9) | 114/115 | −0.02 [−0.03, 0.01] | 0 | 0.43 | 0.21 | |
| H | 12/12 | 0.01 [−0.06, 0.08] | 0.4213 | |||
| L-M | 102/103 | −0.02 [−0.04, 0.01] | 5 | 0.39 | 0.14 | |
| FM (kg) (6) | 147/152 | −1.18 [−3.75, 1.39] | 51 | 0.07 | 0.37 | |
| H | 115/119 | −2.12 [−7.25, 3.01] | 64 | 0.04 | 0.42 | 0.7281 |
| L-M | 32/33 | −1.57 [−3.03, −0.11] | 43 | 0.18 | 0.03 | |
| PFM (%) (13) | 243/251 | −1.38 [−2.64, −0.12] | 52 | 0.01 | 0.03 | |
| H | 103/108 | −2.61 [−7.98, 2.75] | 76 | 0.02 | 0.34 | 0.6455 |
| L-M | 140/143 | −0.94 [−1.52, −0.36] | 46 | 0.05 | <0.01 | |
| BMI (22) | 409/410 | −0.29 [−0.70, 0.11] | 0 | 0.92 | 0.15 | |
| H | 216/218 | 0.18 [−1.05, 1.41] | 0 | 0.86 | 0.77 | 0.4223 |
| L-M | 193/192 | −0.35 [−0.78, 0.08] | 0 | 0.80 | 0.11 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, T.; Lin, M.-H.; Kim, K. Intensity Differences of Resistance Training for Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 440. https://doi.org/10.3390/healthcare11030440
Fan T, Lin M-H, Kim K. Intensity Differences of Resistance Training for Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(3):440. https://doi.org/10.3390/healthcare11030440
Chicago/Turabian StyleFan, Tenglong, Man-Hsu Lin, and Kijin Kim. 2023. "Intensity Differences of Resistance Training for Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis" Healthcare 11, no. 3: 440. https://doi.org/10.3390/healthcare11030440
APA StyleFan, T., Lin, M.-H., & Kim, K. (2023). Intensity Differences of Resistance Training for Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis. Healthcare, 11(3), 440. https://doi.org/10.3390/healthcare11030440