
The Synergetic Effect of Plyometric Compound Exercises and Transcranial Direct Current Stimulation on Balance and Physical Function


Abstract
:1. Introduction
2. Materials and Methods
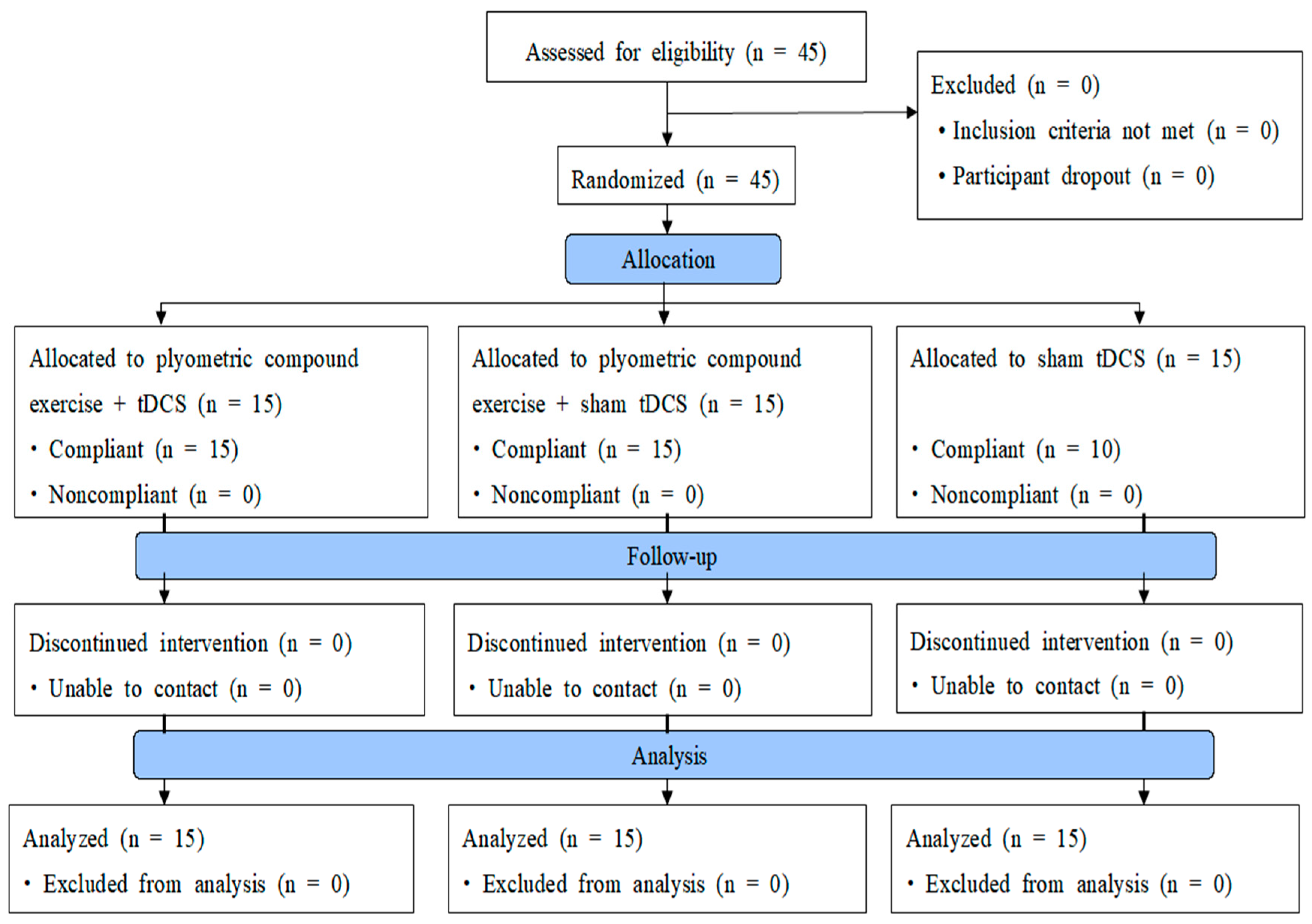
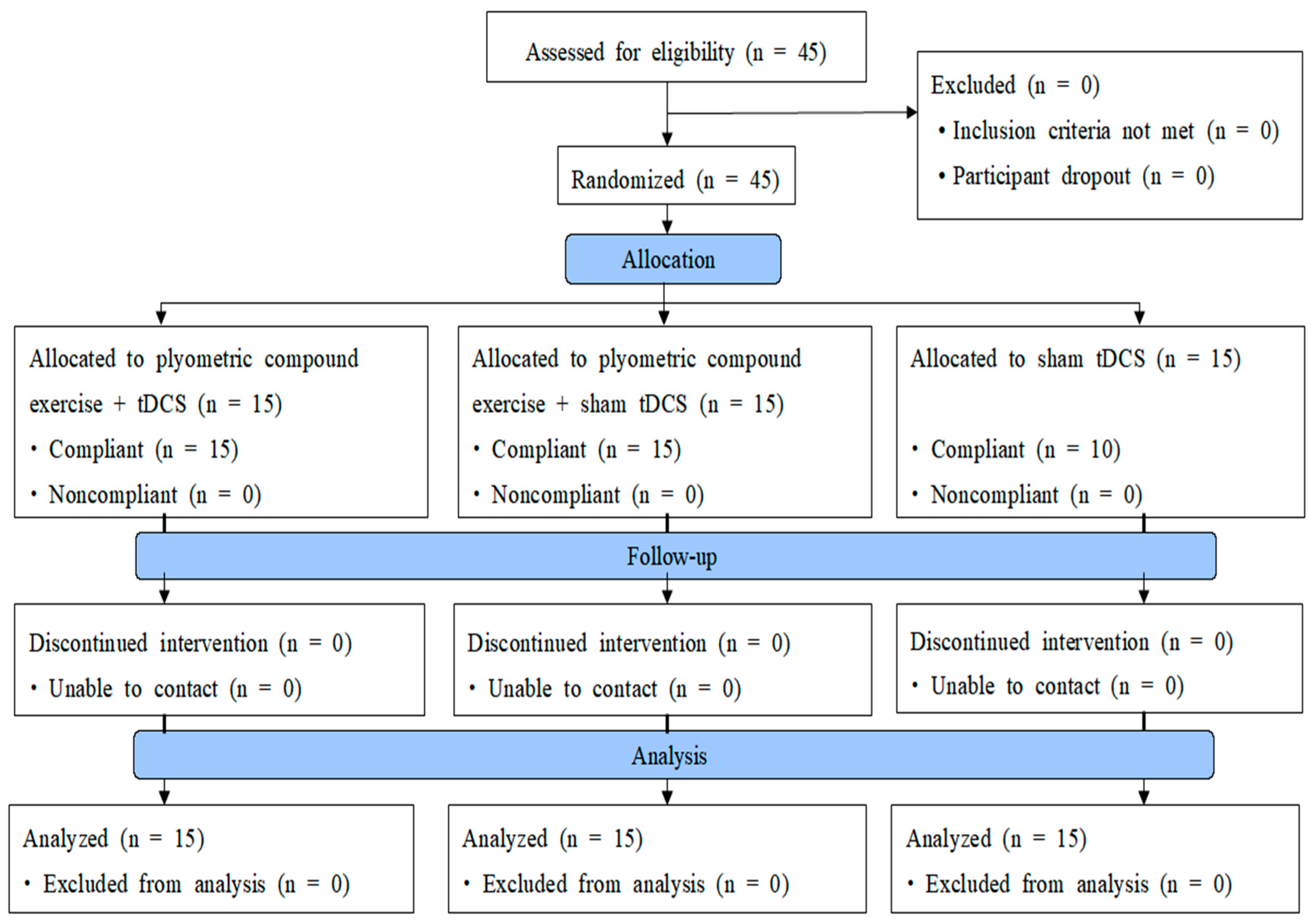
2.1. Participants
2.2. Study Design
2.3. Procedures
2.4. Outcome Measures
2.4.1. Static Balance Ability
2.4.2. Dynamic Balancing Ability
2.4.3. Power
- The vertical jump test: The participant stood 20 cm away from a wall with feet shoulder-width apart, outstretched arms as far as possible, marked the height with fingertips, jumped as high as possible without run-up, and marked the points of fingertips as the height; the distance between the first and second marks was measured in cm. The entire process was repeated twice, and the highest measurement was recorded [22].
- The long jump test: The participant stood in front of a parallel measuring board, lowered their center of body weight, bent their knees, swung their arms backward, jumped off the ground, swung their arms forward as much as possible, stretched their body, bent their abdomen and legs, and landed on the heels; the researcher measured the distance between the heels when landing on both feet on the measuring board. The entire process was repeated twice, and the highest measurement (cm) was recorded [23].
2.4.4. Agility
- t-test: A stopwatch (CASIO HS-80W, Japan) was used to measure agility. The participant quickly sprinted from point A to point B (9.14 m) following the instruction “Ready, start”. The participant then moved their body to the right to point D (4.57 m), from point D to point C, and back to point B (13.71 m), before finally returning to point A (9.14 m). The entire process was repeated twice, and the shortest time(s) was recorded [24].
- Side-step test: Three lines were marked with paper tape at the center, on the left, and on the right at an interval of 120 cm on the floor. The participant took a ready posture with both feet shoulder-width apart; as the test began, if the right foot crossed over to the right line, it was scored as 1; if the right foot, which had crossed over to the right line, quickly returned to the center line, it was 2; if the left foot crossed the left line after returning to the center line, it was 3. The whole process was repeated twice for 10 s and the maximum number of frequencies was recorded [25,26].
2.5. Intervention
2.5.1. Exercise Program
2.5.2. Transcranial Direct Current Stimulation
2.5.3. Statistical Analysis
3. Results
3.1. General Subject Characteristics
3.2. Changes in Static Balance (FRT) before and after the Intervention
3.3. Changes in Dynamic Balance (Y-BT) before and after the Intervention
3.3.1. Change in Dynamic Balance of the Left Leg before and after the Intervention
3.3.2. Change in Dynamic Balance of the Right Leg before and after the Intervention
3.4. Changes in Power before and after the Intervention
3.4.1. Vertical Jump Test
3.4.2. Long Jump Test
3.5. Changes in Agility before and after the Intervention
3.5.1. t-Test
3.5.2. Side-Step Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wojtys, E.M. Sports injury prevention. Sports Health 2017, 9, 106–107. [Google Scholar] [CrossRef]
- Kiers, H.; van Dieën, J.; Dekkers, H.; Wittink, H.; Vanhees, L. A systematic review of the relationship between physical activities in sports or daily life and postural sway in upright stance. Sports Med. 2013, 43, 1171–1189. [Google Scholar] [CrossRef]
- Han, J.; Anson, J.; Waddington, G.; Adams, R.; Liu, Y. The Role of Ankle Proprioception for Balance Control in relation to Sports Performance and Injury. BioMed Res. Int. 2015, 2015, 842804. [Google Scholar] [CrossRef]
- Sasaki, S.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Kimura, Y.; Fujita, Y.; Ishibashi, Y. Core-muscle training and neuromuscular control of the lower limb and trunk. J. Athl. Train. 2019, 54, 959–969. [Google Scholar] [CrossRef]
- Zech, A.; Hübscher, M.; Vogt, L.; Banzer, W.; Hänsel, F.; Pfeifer, K. Balance training for neuromuscular control and performance enhancement: A systematic review. J. Athl. Train. 2010, 45, 392–403. [Google Scholar] [CrossRef]
- Behm, D.G.; Sale, D.G. Intended rather than actual movement velocity determines velocity-specific training response. J. Appl. Physiol. 1993, 74, 359–368. [Google Scholar] [CrossRef]
- Davies, G.; Riemann, B.L.; Manske, R. Current concepts of plyometric exercise. Int. J. Sports Phys. Ther. 2015, 10, 760–786. [Google Scholar]
- Chmielewski, T.L.; Myer, G.D.; Kauffman, D.; Tillman, S.M. Plyometric exercise in the rehabilitation of athletes: Physiologic responses and clinical application. J. Orthop. Sports Phys. Ther. 2006, 36, 308–319. [Google Scholar] [CrossRef]
- Ramachandran, A.K.; Singh, U.; Ramirez-Campillo, R.; Clemente, F.M.; Afonso, J.; Granacher, U. Effects of plyometric jump training on balance performance in healthy participants: A systematic review with meta-analysis. Front. Physiol. 2021, 12, 730945. [Google Scholar] [CrossRef]
- Bel, L.; Mathieu, N.; Ducrest, V.; Bizzini, M. Lower limb exercise-based injury prevention programs are effective in improving sprint speed, jumping, agility and balance: An umbrella review. Int. J. Sports Phys. Ther. 2021, 16, 1396–1404. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Grosprêtre, S.; Grandperrin, Y.; Nicolier, M.; Gimenez, P.; Vidal, C.; Tio, G.; Haffen, E.; Bennabi, D. Effect of transcranial direct current stimulation on the psychomotor, cognitive, and motor performances of power athletes. Sci. Rep. 2021, 11, 9731. [Google Scholar] [CrossRef]
- Machado, S.; Jansen, P.; Almeida, V.; Veldema, J. Is tDCS an adjunct ergogenic resource for improving muscular strength and endurance performance? A systematic review. Front. Psychol. 2019, 10, 1127. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Paltamaa, J.; Sjögren, T.; Peurala, S.H.; Heinonen, A. Effects of physiotherapy interventions on balance in multiple sclerosis: A systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 2012, 44, 811–823. [Google Scholar] [CrossRef]
- Codella, R.; Alongi, R.; Filipas, L.; Luzi, L. Ergogenic effects of bihemispheric transcranial direct current stimulation on fitness: A randomized cross-over trial. Int. J. Sports. Med. 2021, 42, 66–73. [Google Scholar] [CrossRef]
- Atalag, O.; Kurt, C.; Huebner, A.; Galimba, M.; Uson, J.K. Is complex training superior to drop jumps or back squats for eliciting a post activation potentiation enhancement response? J. Phys. Educ. Sport 2021, 21, 2228–2236. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The reliability of an instrumented device for measuring components of the star excursion balance test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar]
- Shaffer, S.W.; Teyhen, D.S.; Lorenson, C.L.; Warren, R.L.; Koreerat, C.M.; Straseske, C.A.; Childs, J.D. Y-balance test: A reliability study involving multiple raters. Mil. Med. 2013, 178, 1264–1270. [Google Scholar] [CrossRef]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- Lee, M.G. Effects of Plyometric Training with Electrostimulation on Muscle Power and Fitness Variables in Soccer Players. Master’s Thesis, Korea National University of Sports, Seoul, Republic of Korea, 2018. [Google Scholar]
- Coker, C. Kinematic effects of varying adolescents’ attentional instructions for standing long jump. Percept. Mot. Ski. 2018, 125, 1093–1102. [Google Scholar] [CrossRef]
- Munro, A.G.; Herrington, L.C. Between-session reliability of four hop tests and the agility t-test. J. Strength Cond. Res. 2011, 25, 1470–1477. [Google Scholar] [CrossRef]
- Johnson, B.L.; Nelson, J.K. Practical Measurements for Evaluation in Physical Education; Burgess Publishing Company: Minneapolis, MN, USA, 1969. [Google Scholar]
- Choo, S. Effects of Tabata and Plyometric Exercises on Equilibrium, Agility, and Quickness of Elementary School Taekwondo Demonstrators. Master’s Thesis, Graduate School of General Studies, Korea University of Sports, Seoul, Republic of Korea, 2022. [Google Scholar]
- Hedrick, A. Training for hypertrophy. Strength Cond. J. 1995, 17, 22–29. [Google Scholar] [CrossRef]
- Earle, R. Weight Training Exercise Prescription. Essentials of Personal Training Symposium Workbook; NSCA Certification Commission: Lincoln, NE, USA, 1999. [Google Scholar]
- Hoffman, J.R.; Ratamess, N.A.; Klatt, M.; Faigenbaum, A.D.; Ross, R.E.; Tranchina, N.M.; McCurley, R.C.; Kang, J.; Kraemer, W.J. Comparison between different off-season resistance training programs in Division III American college football players. J. Strength Cond. Res. 2009, 23, 11–19. [Google Scholar] [CrossRef]
- Soon, M.T. Effects of Load-Dependent Plyometric Training on Jump Mechanics. Master’s Thesis, Graduate School of Kookmin, Seoul University, Seoul, Republic of Korea, 2014. [Google Scholar]
- Gandiga, P.C.; Hummel, F.C.; Cohen, L.G. Transcranial DC stimulation (tDCS): A tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 2006, 117, 845–850. [Google Scholar] [CrossRef]
- Amatachaya, A.; Jensen, M.P.; Patjanasoontorn, N.; Auvichayapat, N.; Suphakunpinyo, C.; Janjarasjitt, S.; Ngernyam, N.; Aree-uea, B.; Auvichayapat, P. The short-term effects of transcranial direct current stimulation on electroencephalography in children with autism: A randomized crossover controlled trial. Behav. Neurol. 2015, 2015, 928631. [Google Scholar] [CrossRef]
- Woods, A.J.; Antal, A.; Bikson, M.; Boggio, P.S.; Brunoni, A.R.; Celnik, P.; Cohen, L.G.; Fregni, F.; Herrmann, C.S.; Kappenman, E.S.; et al. A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin. Neurophysiol. 2016, 127, 1031–1048. [Google Scholar] [CrossRef]
- Gonçalves, C.; Bezerra, P.; Clemente, F.M.; Vila-Chã, C.; Leão, C.; Brandão, A.; Cancela, J.M. Effect of instability and bodyweight neuromuscular training on dynamic balance control in active young adults. Int. J. Environ. Res. Public Health 2020, 17, 8879. [Google Scholar] [CrossRef]
- Mahdieh, L.; Zolaktaf, V.; Karimi, M.T. Effects of dynamic neuromuscular stabilization (DNS) training on functional movements. Hum. Mov. Sci. 2020, 70, 102568. [Google Scholar] [CrossRef]
- Cherni, Y.; Jlid, M.C.; Mehrez, H.; Shephard, R.J.; Paillard, T.; Chelly, M.S.; Hermassi, S. Eight weeks of plyometric training improves ability to change direction and dynamic postural control in female basketball players. Front. Physiol. 2019, 10, 726. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, R.; Shahrjerdi, S.; Golpaigany, M.; Kazemi, M. The effect of a six-week plyometric training on dynamic balance and knee proprioception in female badminton players. J. Can. Chiropr. Assoc. 2019, 63, 144–153. [Google Scholar] [PubMed]
- Dutta, A.; Chugh, S. Effect of transcranial direct current stimulation on cortico-muscular coherence and standing postural steadiness. In Proceedings of the 2nd IASTED International Conference on Assistive Technologies, Innsbruck, Austria, 15–17 February 2012. [Google Scholar] [CrossRef]
- Kaminski, E.; Steele, C.J.; Hoff, M.; Gundlach, C.; Rjosk, V.; Sehm, B.; Villringer, A.; Ragert, P. Transcranial direct current stimulation (tDCS) over primary motor cortex leg area promotes dynamic balance task performance. Clin. Neurophysiol. 2016, 127, 2455–2462. [Google Scholar] [CrossRef] [PubMed]
- de Haart, M.; Geurts, A.C.; Huidekoper, S.C.; Fasotti, L.; van Limbeek, J. Recovery of standing balance in postacute stroke patients: A rehabilitation cohort study. Arch. Phys. Med. Rehabil. 2004, 85, 886–895. [Google Scholar] [CrossRef]
- Kim, J.; Jung, S. Effects of strength training on H/Q ratio and joint position sense in adult women with ipsilateral muscle strength imbalance of the knee joint. Korean J. Wellness 2019, 14, 363–370. [Google Scholar] [CrossRef]
- Matsunaga, K.; Nitsche, M.A.; Tsuji, S.; Rothwell, J.C. Effect of transcranial DC sensorimotor cortex stimulation on somatosensory evoked potentials in humans. Clin. Neurophysiol. 2004, 115, 456–460. [Google Scholar] [CrossRef]
- Zheng, X.; Alsop, D.C.; Schlaug, G. Effects of transcranial direct current stimulation (tDCS) on human regional cerebral blood flow. Neuroimage 2011, 58, 26–33. [Google Scholar] [CrossRef]
- Park, W. Effects of Sensorimotor Training and Transcranial Direct Current Stimulation on Improving Balance Ability of Soccer Players. Master’s Thesis, Graduate School of General Studies, Dongshin University, Naju, Republic of Korea, 2018. [Google Scholar]
- Lundy-Ekman, L. Neuroscience-E-Book: Fundamentals for Rehabilitation, 4th ed.; Elsevier Sauders: St. Louis, MO, USA, 2012. [Google Scholar]
- Meylan, C.; Malatesta, D. Effects of in-season plyometric training within soccer practice on explosive actions of young players. J. Strength Cond. Res. 2009, 23, 2605–2613. [Google Scholar] [CrossRef]
- Van Roie, E.; Walker, S.; Van Driessche, S.; Delabastita, T.; Vanwanseele, B.; Delecluse, C. An age-adapted plyometric exercise program improves dynamic strength, jump performance and functional capacity in older men either similarly or more than traditional resistance training. PLoS ONE 2020, 15, e0237921. [Google Scholar] [CrossRef]
- Chen, C.H.; Chen, Y.C.; Jiang, R.S.; Lo, L.Y.; Wang, I.L.; Chiu, C.H. Transcranial direct current stimulation decreases the decline of speed during repeated sprinting in basketball athletes. Int. J. Environ. Res. Public Health 2021, 18, 6967. [Google Scholar] [CrossRef]
- Wilk, K.E.; Voight, M.L.; Keirns, M.A.; Gambetta, V.; Andrews, J.R.; Dillman, C.J. Stretch-shortening drills for the upper extremities: Theory and clinical application. J. Orthop. Sports Phys. Ther. 1993, 17, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Zouhal, H.; Abderrahman, A.B.; Dupont, G.; Truptin, P.; Le Bris, R.; Le Postec, E.; Sghaeir, Z.; Brughelli, M.; Granacher, U.; Bideau, B. Effects of neuromuscular training on agility performance in elite soccer players. Front. Physiol. 2019, 10, 947. [Google Scholar] [CrossRef] [PubMed]
- Kamali, A.M.; Saadi, Z.K.; Yahyavi, S.S.; Zarifkar, A.; Aligholi, H.; Nami, M. Transcranial direct current stimulation to enhance athletic performance outcome in experienced bodybuilders. PLoS ONE 2019, 14, e0220363. [Google Scholar] [CrossRef] [PubMed]
- Kidgell, D.J.; Goodwill, A.M.; Frazer, A.K.; Daly, R.M. Induction of cortical plasticity and improved motor performance following unilateral and bilateral transcranial direct current stimulation of the primary motor cortex. BMC Neurosci. 2013, 14, 64. [Google Scholar] [CrossRef]
- Dumel, G.; Bourassa, M.E.; Desjardins, M.; Voarino, N.; Charlebois-Plante, C.; Doyon, J.; De Beaumont, L. Multisession anodal tDCS protocol improves motor system function in an aging population. Neural Plast. 2016, 2016, 5961362. [Google Scholar] [CrossRef]

{kind=link}
| Type of Exercise | Reps | Sets | |
|---|---|---|---|
| Week 1 | Squat Jump, Side Short Pitch, Lateral Barrier Hop, Skip | 10 | 3 |
| Week 2 | Squat Jump, Two Foot Ankle Hop, Ice Skater Jump, Lunge Hop | 10 | 3 |
| Week 3 | Two Foot Ankle Hop, Ice Skater Jump, Squat Box Jump, Lunge Hop | 12 | 3 |
| Week 4 | Two Foot Ankle Hop, Squat Box Jump, Burpee Box Jump, Leap Frogs Jump | 15 | 4 |
| Experimental Group I (n = 15) | Experimental Group II (n = 15) | Control Group (n = 15) | p | |
|---|---|---|---|---|
| Age (years) | 33.06 ± 4.60 a | 33.26 ± 4.80 | 33.00 ± 3.22 | 0.984 |
| Height (cm) | 174.60 ± 2.82 | 174.8 ± 3.27 | 176.4 ± 4.32 | 0.293 |
| Weight (kg) | 75.40 ± 3.85 | 74.86 ± 4.06 | 75.66 ± 4.59 | 0.868 |
| Experimental Group I (n = 15) | Experimental Group II (n = 15) | Control Group (n = 15) | Group X Time F (p) | ||
|---|---|---|---|---|---|
| FRT (cm) | Before | 42.00 ± 2.13 a | 41.86 ± 2.32 | 41.86 ± 2.77 | 46.214 (<0.001) |
| After | 46.66 ± 2.58 | 44.40 ± 1.91 | 42.06 ± 2.60 | ||
| Difference | 4.66 ± 1.49 | 2.53 ± 1.18 | 0.26 ± 1.03 | ||
| t(p) | −12.081 (0.000) | −8.264 (0.000) | −0.823 (0.424) |
| Experimental Group I (n = 15) | Experimental Group II (n = 15) | Control Group (n = 15) | Group X Time | ||
|---|---|---|---|---|---|
| F (p) | |||||
| Y-Balance Test (Rt score) | Before | 90.83 ± 1.77 a | 91.37 ± 3.04 | 92.02 ± 2.29 | 55.131 (<0.001) |
| After | 94.25 ± 1.93 | 93.75 ± 2.83 | 92.03 ± 2.42 | ||
| Difference | 3.42 ± 1.17 | 2.38 ± 0.77 | 0.00 ± 0.72 | ||
| t (p) | −11.290 (0.000) | −12.003 (0.000) | −0.045 (0.965) | ||
| Y-Balance Test (Lt score) | Before | 91.62 ± 1.41 a | 91.42 ± 2.58 | 91.95 ± 2.35 | 85.703 (<0.001) |
| After | 95.03 ± 1.49 | 94.09 ± 2.71 | 92.01 ± 2.32 | ||
| Difference | 3.40 ± 0.52 | 2.67 ± 0.90 | 0.06 ± 0.73 | ||
| t (p) | −25.197 (0.000) | −11.475 (0.000) | −0.321 (0.753) |
| Experimental Group I (n = 15) | Experimental Group II (n = 15) | Control Group (n = 15) | Group X Time | ||
|---|---|---|---|---|---|
| F (p) | |||||
| Vertical Jump Test (cm) | Before | 40.20 ± 2.00 a | 40.46 ± 1.76 | 40.26 ± 2.25 | 57.512 (<0.001) |
| After | 45.20 ± 1.97 | 42.93 ± 2.84 | 40.33 ± 2.09 | ||
| Difference | 5.00 ± 1.25 | 2.46 ± 1.59 | 0.03 ± 0.79 | ||
| t (p) | −15.448 (0.000) | −5.980 (0.000) | −0.323 (0.751) | ||
| Long Jump Test (cm) | Before | 229.60 ± 4.59 a | 230.13 ± 3.94 | 230.73 ± 4.62 | 107.043 (<0.001) |
| After | 235.00 ± 4.47 | 234.20 ± 4.00 | 230.93 ± 4.72 | ||
| Difference | 5.40 ± 1.18 | 4.06 ± 0.88 | 0.20 ± 0.94 | ||
| t (p) | −17.676 (0.000) | −17.823 (0.000) | −0.823 (0.424) |
| Experimental Group I (n = 15) | Experimental Group II (n = 15) | Control Group (n = 15) | Group X Time | ||
|---|---|---|---|---|---|
| F (p) | |||||
| t-Test (second) | Before | 13.22 ± 0.40 a | 13.16 ± 0.47 | 13.30 ± 0.38 | 35.942 (<0.001) |
| After | 12.17 ± 0.40 | 12.47 ± 0.56 | 13.32 ± 0.52 | ||
| Difference | −1.05 ± 0.31 | −0.68 ± 0.35 | 0.01 ± 0.37 | ||
| t (p) | 12.926 (0.000) | 7.502 (0.000) | −0.171 (0.867) | ||
| Side-Step Test (frequency) | Before | 12.06 ± 1.27 a | 12.00 ± 1.30 | 10.86 ± 2.13 | 73.082 (<0.001) |
| After | 17.26 ± 2.15 | 15.73 ± 1.57 | 10.93 ± 2.12 | ||
| Difference | 5.20 ± 1.42 | 3.73 ± 1.38 | 0.06 ± 0.59 | ||
| t (p) | −14.140 (0.000) | −10.425 (0.000) | −0.435 (0.670) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.-H.; Yim, J.-E. The Synergetic Effect of Plyometric Compound Exercises and Transcranial Direct Current Stimulation on Balance and Physical Function. Healthcare 2023, 11, 2774. https://doi.org/10.3390/healthcare11202774
Song J-H, Yim J-E. The Synergetic Effect of Plyometric Compound Exercises and Transcranial Direct Current Stimulation on Balance and Physical Function. Healthcare. 2023; 11(20):2774. https://doi.org/10.3390/healthcare11202774
Chicago/Turabian StyleSong, Jeong-Hyeok, and Jong-Eun Yim. 2023. "The Synergetic Effect of Plyometric Compound Exercises and Transcranial Direct Current Stimulation on Balance and Physical Function" Healthcare 11, no. 20: 2774. https://doi.org/10.3390/healthcare11202774
APA StyleSong, J.-H., & Yim, J.-E. (2023). The Synergetic Effect of Plyometric Compound Exercises and Transcranial Direct Current Stimulation on Balance and Physical Function. Healthcare, 11(20), 2774. https://doi.org/10.3390/healthcare11202774