


Hidden and Understaffed: Exploring Canadian Medical Laboratory Technologists’ Pandemic Stressors and Lessons Learned

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participant Recruitment
2.3. Ethical Considerations
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Participant Demographic
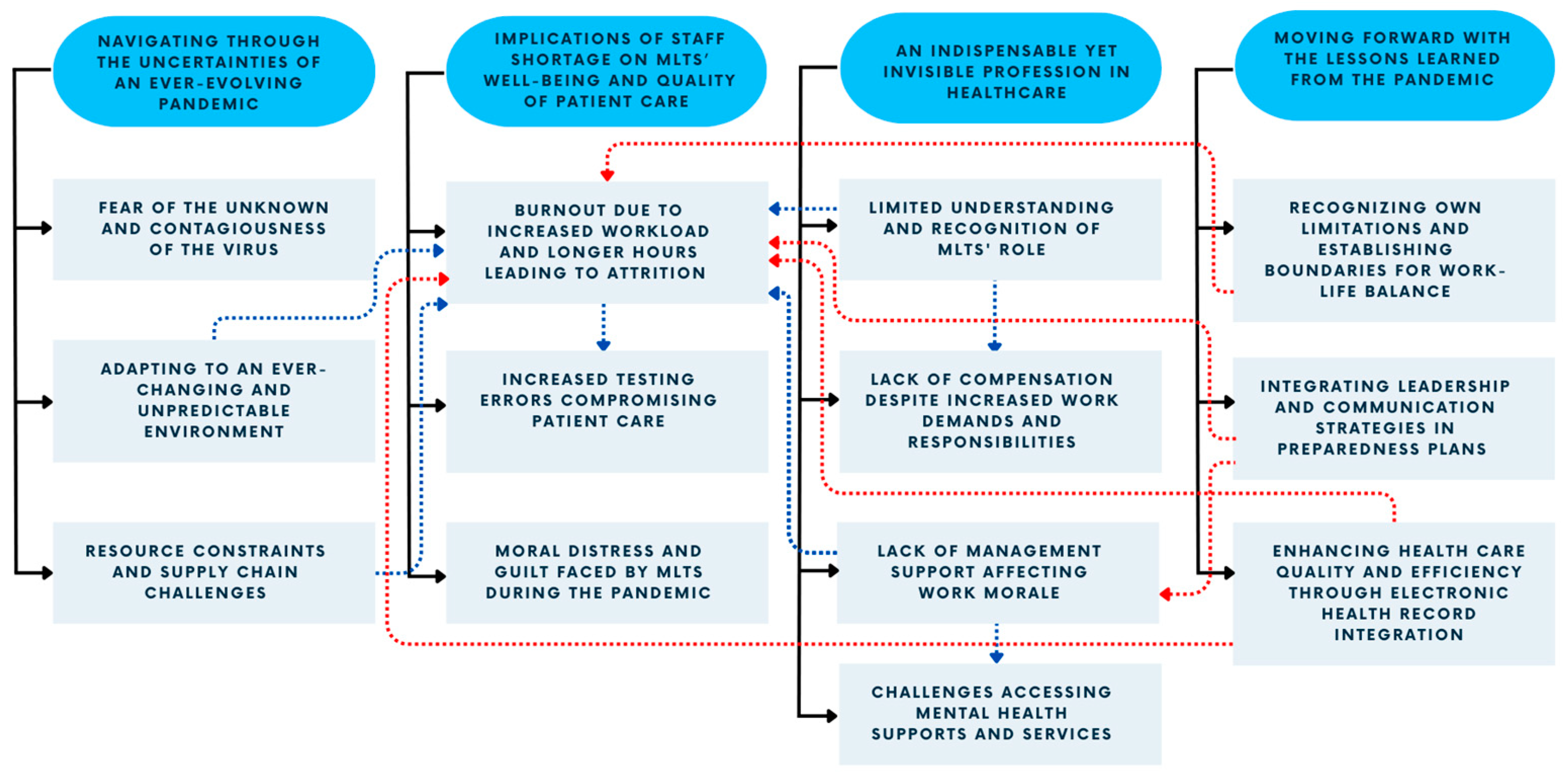
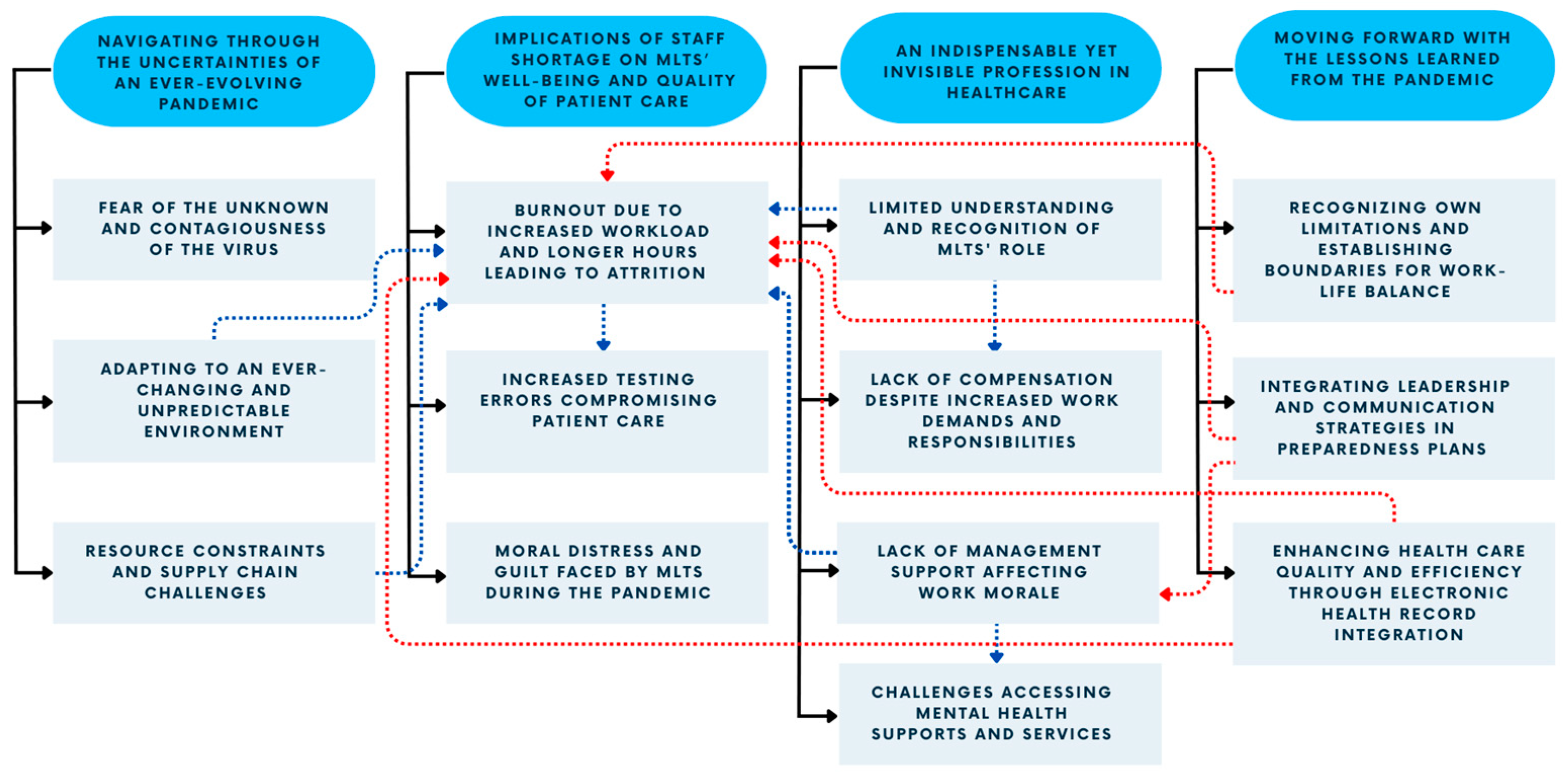
3.2. Unexpected Challenges Navigating through the Uncertainties of an Ever-Evolving Pandemic
3.2.1. Fear of the Unknown and Contagiousness of the Virus
FG-80: “So, I found the, the biggest stressor for me at least, like for, for the first wave, when it first started, was the unknown. So, you sort of like, everyone in the public had we don’t know what the effect of this is, we don’t know how contagious it is. We don’t really know what’s going on.”
FG-89: “Uh, I think in the beginning it was, it was really the uncertainty of the pandemic like, um, yeah, just you don’t know what’s gonna happen next.”
FG-104: “…just anxiety about catching COVID and going to work and having to put myself at risk while this maximum workload was still being placed upon us, so like my own health and safety.”
FG-79: “…there was a shortage of masks and we wanted to reserve the masks to the nurses and doctors or other professionals who interacted with the patients directly.”
FG-53: “…in the first wave and especially at the beginning was, was the fear of infection and the fear of, worse, the fear of bringing it home. I, I, I don’t know many people who in, in health care, who weren’t experiencing that, the fear of bringing it home… especially in the beginning when we didn’t have enough information about transmission and modes of contact and means of managing containment. We didn’t have any of that.”
FG-85: “Like for me, I had a brand-new baby at home and I had a, a child in school and coming home and not like, trying not to bring it home. I was like scrubbing down and showering, going straight down, stripping my scrubs off and putting them in the, um, wash… And so, then I was changing at work and then coming home and so, it was a lot of that stress and just not knowing, and trying to keep your, your family safe. Even knowing that you’re, you’ve just walked into a, a positive room and like, “How do I not bring this home to my brand-new baby? How do I not bring this home to my, my husband and, and little son?”
FG-80: “My husband is also exposed to patients and, and my kids go to school so, there was also, you know, that. And I have, you know, my mom’s in her 70s and we’re worried about her and, you know that kind of stuff?… And you know, when you go to work and then you worry about bringing it home.”
FG-82: “I also live with someone who’s immunocompromised, and our lab was right beside the intensive care unit, so I was a bit concerned about bringing anything home.”
FG-79: “Because we didn’t know much about COVID such that how it’s spread, etcetera, I was hoping that I will, I was not spreading the virus to patients by coming to work.”
3.2.2. Adapting to an Ever-Changing and Unpredictable Environment
FG-80: “And then just every time we went to work, there was a change. So, one day it would be like, okay, well, you have to wear a mask all the time, well, you do this, and now it’s you have to wear an N-95 and now it’s, okay well, we want you to wear an N-95 and a face shield and then, oh, well, you don’t really need any of that. So, every day when we went to work, there was something new, there was a new procedure to learn, there was a new protocol to follow, and it’s just, we sort of had these, like, debriefings every day.”
FG-97: “Um, I will say for us one of the biggest stressors would be a heavy workload which increased exponentially for us, especially during COVID because our lab was very much involved in the COVID testing. And with that, the need to adapt to change very quickly and then like, to learn new processes and new testing methods in a very short period of time.”
FG-11: “…I found during COVID there was a need for a lot of, um, adaptability and there was a lot of changing just kind of happening in a very short time scale and a lot of lab[s] just weren’t prepared to take that on.”
3.2.3. Resource Constraints and Supply-Chain Challenges
FG-105: “I just wanted to also add the strain of supply chain, um, where our current, like most common supplies are often running out with no alternative to replace. Um, and for the lab, it means a lot because we actually have to validate new reagent, new test tubes. And this is just increasing workload to already stretched workforce, um, and we’ve never seen this in the past.”
FG-96: “And then the final stressor that I thought of that was touched on was just supply issues, but not only COVID-specific supplies but even things like our gold top tubes. At one point, we were very near to the point of sending our patients to another location because we had to save the very few (saline) tubes that we had in case we had stats, in case we had emergencies, that sort of thing, um, because we just could not source it. We’re a small clinic. We were not on the top priority list for the supplier. So, it took a lot to be able to get a hold of the supplies that we needed, even for things that weren’t COVID-related.”
FG-107: “There’s a lack of equipment required to do our, our job with, you know, sometimes a lot of the instruments are getting older.”
3.3. Implications of Staff Shortage for the Well-Being of MLTs and the Quality of Patient Care
3.3.1. Burnout due to Increased Workload and Prolonged Hours Leading to Attrition
FG-104: “…you know, you had three night shifts, then one day off then had to work seven day shifts in a row and you never got to see your spouse or you had to work stat holidays.”
FG-94: “There’s been injuries at work and with how we have staff shortages and increased load, people are trying to push harder, work faster so those injuries are happening more often.”
FG-107: “It was a, a big stress on me because I, I needed to get everything up and running because people’s lives were, um, on the line. So, that was, it was so bad that I actually ended up in the hospital with a cardiac event. And stupid me thought, okay, well, uh, I should just go back, I’m okay now, I’m gonna go back. So, I tried for a few more months and the stress, it just didn’t, it didn’t stop, like it just kept actually rising. So, I ended up going on medical leave.”
FG-89: “Like my experience in my workplace was that a lot of the staff burnt out during the pandemic… Uh, our sample load increased dramatically and there was a lot of people that weren’t adjusted to that to, um, that kind of workload…they ended up retiring early because they couldn’t take the, they couldn’t take the workload… because it was just, like it was just too much work. And then so that, that caused our staff to be in a little bit of a crisis because suddenly there was many people leaving our lab.”
FG-104: “Before COVID, we didn’t necessarily ever have staffing shortages because it would be like one tech got hired and one tech would retire and it was sort of this ongoing trade off and it wasn’t too bad, but we found with COVID we had a lot of techs, uh, for about halfway through 2021, we had a lot of retirees and a lot of people leaving permanently due to stress leave, so we were really running out of people because so many people were leaving.”
FG-105: “For me, I often had to re-evaluate if I wanted to retire because I’m actually at an age where I can retire. Uh, so I did have quite a few times where I would just wanted to give up because on a daily basis, I just deal with problems, like everyone was so negative, and problem-solving all the time and having to find all the solutions.”
FG-89: “I actually like reconsidered my profession many, many times. I would think it was such a mistake to get into healthcare, that I just wanted out, that I wouldn’t recommend this health -, this profession to anyone…”
FG-51: “Even before the pandemic. I think we had maybe half a year or a year when I first started where we were fully staffed, and it was, uh, sort of a steady decline from there on out and it got much, much worse to the point where I actually left that lab and moved to a different lab because it was too short staffed and the demands were still the same or a little bit more, and it ended up putting a little too much strain on people who are left.”
FG-89: “…since we had, um, uh, since it was so stressful at our lab, people would come and be trained and then leave immediately after finding a new job just because, just the workload that they were thrown into was so, was so high that they just looked for, for a new job.”
FG-49: “…it’s stressful and I can’t imagine being a new person and having expectations … You don’t wanna make mistakes and there’s a lot of pressure to make sure that what you’re putting out is accurate and correct and, on both sides, I think from our new hires, and that’s why we’ve actually had a lot of new hires leave because it’s so chaotic, they, they just can’t take the environment.”
3.3.2. Increased Testing Errors due to Workload Pressures and Inadequate Training Compromising Patient Care
FG-39: “I feel that when you are constantly under stress, sometimes I, I might have and I, I might have and so many other MLT’s when they were under so much stress, they might have accidentally made any transcriptional errors in the reporting the critical results. Some results might have been missed to call, which could affect the patient care, because those patients are waiting for those results so that they, their, their treatment could begin and stuff like that, but there were there were situation where the sample was too old to be loaded onto the analyzer. But we were told to cut corners and not to reject the specimen and just continue processing them, which directly implements the patient care. Because if the patient was actually a positive but now that the specimen integrity has lost, that patient might come out as a negative. So, there, there were so many cut corners from the management.”
FG-95: “Just to add on, I want to say that I feel that, that training, the training period was inadequate for a lot of the processes that were being implemented just because due to COVID, it needs to be implemented very fast and very soon. So, not only is the training inadequate, but staff wasn’t- staff weren’t sure what they were doing and there’s a lot of corrective reports that went out. So, I think it added on to a lot of stress that was in my workforce…”
FG-98: “So, if we are, yeah, um, so if we’re putting out like grads who are not fully trained or they may not know certain things, then when we put them out to the workforce and they have the, the employer has these expectations like you have to x, y, z and they don’t know those things, it may require like a recollection from a patient if they collect the wrong tube, whether that be like blood or if it’s a microbiology sample if they plate the, if they inoculate the plates incorrectly, stuff like that. And we have seen cases like this pop up, so it requires a recollection from a patient, which will just ultimately delay patient care.”
FG-95: “Uh, I know that there was a lot more mistakes that were made. And then, there was a lot of corrective reports just because of the burnout and it was just small mistakes that were missed that ended up being reported out. And then we’d have to phone and correct it. So, there was implications at the end of it.”
3.3.3. Moral Distress and Guilt Faced by MLTs during the Pandemic
FG-53: “And so, you ended up with this backlog or you were having conversations about whether or not to do this test this month and whether or not the patient could wait a month or the next month for the test and there was conversations that should never be had that were being had and it left me as a professional feeling inadequate, which I think really wore on all of us. And that was through start to finish. There wasn’t a time where that wasn’t a problem.”
FG-53: “…during the 2nd and the 3rd wave, some of the testing panels we were performing in my particular area were looked at as a possible means of determining who would be ventilated and who would not be ventilated, in the case where a lack of ventilators became possible. And both in the 2nd and the 3rd waves, those conversations were definitely happening. And knowing that the numbers you were generating would literally determine the fate of a human being, was incredibly stressful, way more than I had ever signed up for in my career.”
FG-39: “We also needed a break but you can’t. You badly want to go on your coffee break, but when you actually go on your coffee break, you cannot enjoy your coffee break, because now you’re constantly thinking about going back and calling all those critical results. You could imagine how you must be feeling at 3:00 AM in the, in your night shift, where you have so much work to do. And sometimes we were even asked to handle the bacteriology side as well when there was no support of a lab assistant during night.”
FG-95: “When you’re, when, during our testing, we finish, we usually try to finish the whole process and not leave it to someone else because it’s just very difficult to hand off sometimes. So, um, unpaid overtime, meaning that a lot of times to finish it before the shift ended, we wouldn’t take our break times. So, we would just skip our breaks entirely or we would just take an extra 10 min to finish resulting the samples. And it wasn’t something that was forced, it was just that a lot of people, it was just so busy that you just want to finish your work and go home and have no conscious about it and not take that work home. And then you just didn’t want to leave thinking that, um, you know, that you didn’t hand off properly, it was rushed, and it was just a lot of just emotional kind of, you didn’t want to leave home thinking about work.”
FG-89: “…You would see on the schedule, um, that they’re working short that day and then yeah so, I had uh, yeah, even, even myself like, I would, I would always like triple think even, even trying for one, because you just know that it wouldn’t be possible. Yeah, and even some people who are genuinely sick, like they would feel so guilty about calling in sick to work because they just know it’s, it’s just gonna mean like, an even worse day for everyone.”
FG-101: “People that had like their retirement plan, like planned out, they had their dinner ready they were like, “yeah, I’m gone.” COVID kind of hit, and they were like, “I’ll stay. I will, like, stay, until this is all figured out.” We had people come back, like it was the opposite here, people that were retiring stayed on to see us through. They’re still working to make sure that we, like, get through this.”
3.4. Revealing the Realities of the Hidden, yet Indispensable Role of MLTs in Predominantly Non-Patient-Facing Roles
3.4.1. Limited Understanding and Recognition of the Importance and Roles of MLTs in Healthcare
FG-53: “Some of the stressors that I’ve experienced in this profession, for the 27 odd years, primarily boils down to a lack of either understanding and or respect for the work that actually is accomplished within the laboratory. People outside of the lab kind of view us as that magic black box, samples will go, come, go in. Magic happens. Numbers come out, values come out, but what happens in between is magic… I think that’s the single biggest challenge I’ve experienced in my long career…We’re not in the front, to, for the world to see… we’re hidden, and I think that has a lot to do with why we’re not funded to the levels required to achieve the staffing that’s required to make it possible for us to feel not spread thin.”
FG-96: “I would say our common stressor is, uh, communication and dealing with other health care professionals who may or may not understand, um, really how our profession works and the, the sort of rules the, um, standards that we need to follow.”
3.4.2. Lack of Compensation despite Increased Work Demands and Responsibilities
FG-49: “…you’re asked to take on more responsibilities without actually any additional compensation.”
FG-84: “And then, um, I know then in Ontario, one of the stressors was they did like a pandemic pay for like nurses and people that work in the, like the dietary people, the secretaries, they were getting a pandemic pay, but then the MLTs and respiratory technologist and diagnostic imaging, they didn’t get that cause they weren’t first, first line workers…Like, we were like right there, but it was never acknowledged.”
FG-53: “And then, the lack of pandemic pay hit. And I am sorry, every lab tech in this thing has cried during this pandemic. And then to have that pandemic pay slap in the face hurt. It was like, so it really doesn’t matter what we do, so maybe we should just stop doing it. So, there was that.”
3.4.3. Lack of Management Support
FG-51: “There was also that sense of management not hearing us where we were constantly banging on the fact that we were really short [and] we need to hire more people. We need to do something about this and, uh, almost the feeling like the concerns with being brushed off they weren’t even really being acknowledged. Um, and then sometimes even if management can’t do anything, if they say, ‘But our, our hands are tied, we can’t really do anything about it, but we see you, we’ll do what we can.’ Sometimes even hearing that helps, but our hospital didn’t really do that. So that kind of also affected morale.”
FG-56: “I also had a family emergency during, I think, wave three of the pandemic and I wasn’t allowed to take time off work to deal with that. So, what, management is fully aware of what I was going through, but I was told we’re short-staffed.”
3.4.4. Challenges Accessing Mental Health Supports and Services for MLTs
FG-99: “…it’s usually really difficult, like, given like how short we are, not everyone actually has the time outside the work to attend these, uh, sessions on their personal time.”
3.5. Leveraging Insights from the COVID-19 Pandemic to Enhance Healthcare Practices and Preparedness
3.5.1. Recognizing One’s Own Limitations and Establishing Boundaries for a Healthy Work-Life Balance
FG-99: “Um, just knowing what my own limits are and just really know how I am and what I can take on is that, you know, as a medical lab tech. And also, how to handle the various stressors either at work or at home, so that, that’s really became, um, I would say the highlight of what I’ve learned throughout this whole pandemic period, to figure out, uh, more of my own, uh, yeah, mental capacities.”
FG-94: “…I learned to set up boundaries for myself. I was more of like a yes person before, and even if there were things I wouldn’t [be] uncomfortable with or I didn’t agree with, I would just kind of think of it as a compromise and just let things be. But to me this was a really big deal and I learned to kind of stand up for myself and my family and set up boundaries which, uh, some people were not used to, but it was, uh, it was kind of like, uh, I got a little stronger in a sense, I guess. So, that was, that was kind of the lesson I learned in kind of the good thing that came out of it.”
FG-107: “And also, you know, in order to serve the citizens of Manitoba, you know, I, I need, I needed to, to remember that I need to place myself, ensure that I’m placing myself first and I wasn’t doing that… I was just always thinking about somebody else, but it got to the point where I was putting other people first and then it was having its toll on me.”
3.5.2. Integrating Leadership and Communication Strategies in Preparedness Plans for Effective Public-Health Emergency Response
FG-82: “I think a major thing and it’s a tough thing to be able to do, given that, you know, responding to a pandemic is ever-changing but consistent messaging and consistent, um, like a consistent approach from leadership, uh, in enforcing rules or even determining what the rules are, and very clearly and consistently communicating those rules would have reduced some stress.”
FG-81: “…in terms of preparedness, having a plan for future pandemics, I think it’d also be important to emphasize the role of leadership. Who is doing what and where? Who’s taking care of these staff? Who’s taking care of this patient, for that patient? During the pandemic in my region, everybody was their own leader. We were left to a lot of our own devices… So, in the future, knowing that we have certain people we can look up to, and knowing that we can go to them to find what our roles are, know what their roles are, know what we need to do as individuals would better help not just us understand things, help our morale, help our stress, but give the patients better care.”
FG-80: “…communication was probably the number one thing that, sort of, wasn’t wonderful for this pandemic and, and also just leadership in general. Like, I think people need to feel like they’re a part of a team, but also that they have someone leading them who actually, I mean, I don’t know what one knew what was going on, but it was, it was, everything was so uncertain. And if they could, like, make clear plans…I think if leadership really made stronger protocols and actually stood behind them, it, it gives you sort of a feeling of where you’re supposed to be because everything was really up in the air, and we didn’t have sort of any kind of leg to stand on.”
3.5.3. Enhancing Healthcare Quality and Efficiency through Electronic Health-Record Integration
FG-82: “So, I think, kind of a foundational piece that could be improved across the board is the electronic health record. Um, if that was really seamless with our test results going in and, um, being accessible as soon as they’re ready and, and all of that, I feel like communication between healthcare providers could be improved, patient care could be improved, you know, our workload could be reduced if that was really seamless, just across the board, that would be an improvement. And that could be, you know, a great source of data for epidemiology that would be a little bit more consistent if it was, uh, yeah, more cohesive across Canada or even within provinces, um, between health authorities and between the private and public healthcare, um, like, uh, private lab companies, results being able to come into the EHR in a hospital setting in a simple way would make things simpler.”
4. Discussion
4.1. Pandemic Stressors
4.2. Staff Shortage: The Root of All Evil
4.3. Recommendations
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koontalay, A.; Suksatan, W.; Prabsangob, K.; Sadang, J.M. Healthcare Workers’ Burdens During the COVID-19 Pandemic: A Qualitative Systematic Review. J. Multidiscip. Healthc. 2021, 14, 3015–3025. [Google Scholar] [CrossRef]
- Vindrola-Padros, C.; Andrews, L.; Dowrick, A.; Djellouli, N.; Fillmore, H.; Bautista Gonzalez, E.; Javadi, D.; Lewis-Jackson, S.; Manby, L.; Mitchinson, L.; et al. Perceptions and Experiences of Healthcare Workers during the COVID-19 Pandemic in the UK. BMJ Open 2020, 10, e040503. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/220603/dq220603a-eng.htm (accessed on 31 July 2023).
- Gómez-Urquiza, J.L.; De la Fuente-Solana, E.I.; Albendín-García, L.; Vargas-Pecino, C.; Ortega-Campos, E.M.; Cañadas-De la Fuente, G.A. Prevalence of Burnout Syndrome in Emergency Nurses: A Meta-Analysis. Crit. Care Nurse 2017, 37, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Sexton, J.B.; Adair, K.C.; Proulx, J.; Profit, J.; Cui, X.; Bae, J.; Frankel, A. Emotional Exhaustion Among US Health Care Workers Before and During the COVID-19 Pandemic, 2019–2021. JAMA Netw. Open 2022, 5, e2232748. [Google Scholar] [CrossRef] [PubMed]
- Eftekhar Ardebili, M.; Naserbakht, M.; Bernstein, C.; Alazmani-Noodeh, F.; Hakimi, H.; Ranjbar, H. Healthcare Providers Experience of Working during the COVID-19 Pandemic: A Qualitative Study. Am. J. Infect. Control 2021, 49, 547–554. [Google Scholar] [CrossRef]
- Maunder, R.G.; Heeney, N.D.; Hunter, J.J.; Strudwick, G.; Jeffs, L.P.; Ginty, L.; Johnstone, J.; Kiss, A.; Loftus, C.A.; Wiesenfeld, L.A. Trends in Burnout and Psychological Distress in Hospital Staff over 12 Months of the COVID-19 Pandemic: A Prospective Longitudinal Survey. J. Occup. Med. Toxicol. 2022, 17, 11. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, J.; Geng, Y.; Fang, Z.; Zhu, L.; Chen, Y.; Yao, Y. Meta-Analysis of the Prevalence of Anxiety and Depression among Frontline Healthcare Workers during the COVID-19 Pandemic. Front. Public Health 2022, 10, 984630. [Google Scholar] [CrossRef]
- D’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef]
- Saragih, I.D.; Tonapa, S.I.; Saragih, I.S.; Advani, S.; Batubara, S.O.; Suarilah, I.; Lin, C.-J. Global Prevalence of Mental Health Problems among Healthcare Workers during the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2021, 121, 104002. [Google Scholar] [CrossRef]
- Sultana, A.; Sharma, R.; Hossain, M.M.; Bhattacharya, S.; Purohit, N. Burnout among Healthcare Providers during COVID-19: Challenges and Evidence-Based Interventions. Indian J. Med. Ethics 2020, 5, 308–311. [Google Scholar] [CrossRef]
- Tong, J.; Zhang, J.; Zhu, N.; Pei, Y.; Liu, W.; Yu, W.; Hu, C.; Sun, X. Effects of COVID-19 Pandemic on Mental Health among Frontline Healthcare Workers: A Systematic Review and Meta-Analysis. Front. Psychol. 2023, 13, 1096857. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ Burnout and Associated Risk Factors during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Bayot, M.L.; Lopes, J.E.; Naidoo, P. Clinical Laboratory. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Canadian Institute for Health Information. Medical Laboratory Technologists in Canada, 2010; CIHI: Ottawa, ON, Canada, 2012; p. 33. [Google Scholar]
- Lippi, G.; Plebani, M. The Critical Role of Laboratory Medicine during Coronavirus Disease 2019 (COVID-19) and Other Viral Outbreaks. Clin. Chem. Lab. Med. (CCLM) 2020, 58, 1063–1069. [Google Scholar] [CrossRef]
- Nowrouzi-Kia, B.; Dong, J.; Gohar, B.; Hoad, M. Factors Associated with Burnout among Medical Laboratory Professionals in Ontario, Canada: An Exploratory Study during the Second Wave of the COVID-19 Pandemic. Health Plan. Manag. 2022, 37, 2183–2197. [Google Scholar] [CrossRef]
- Canadian Society for Medical Laboratory Science. Available online: https://csmls.org/About-Us/Society-News/Media-Releases/MEDICAL-LABORATORY-PROFESSIONALS-CONCERNED-WITH-O.aspx (accessed on 5 August 2023).
- Canadian Institute for Health Information. Health Workforce in Canada, 2017 to 2021: Overview—Data Tables 2022; CIHI: Ottawa, ON, Canada, 2022. [Google Scholar]
- Canadian Society for Medical Laboratory Science. Available online: https://www.csmls.org/Research/Research-Reports/The-Canadian-Medical-Laboratory-Profession-s-Call.aspx (accessed on 20 July 2023).
- Nowrouzi-Kia, B.; Dong, J.; Gohar, B.; Hoad, M. Examining the Mental Health, Wellbeing, Work Participation and Engagement of Medical Laboratory Professionals in Ontario, Canada: An Exploratory Study. Front. Public Health 2022, 10, 876883. [Google Scholar] [CrossRef]
- Djukic, B.; Nielsen, C. Mental Health Status of Medical Laboratory Professionals. Healthc. Manag. Forum 2022, 35, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.; Fayyaz, Y.; Jaswal, S.; Gohar, B.; Yazdani, A.; Chattu, V.K.; Nowrouzi-Kia, B. Factors Associated with Job Satisfaction in Medical Laboratory Professionals during the COVID-19 Pandemic: An Exploratory Study in Ontario, Canada. Eur. J. Investig. Health Psychol. Educ. 2022, 13, 54–66. [Google Scholar] [CrossRef]
- Fernández-Castillo, R.-J.; González-Caro, M.-D.; Fernández-García, E.; Porcel-Gálvez, A.-M.; Garnacho-Montero, J. Intensive Care Nurses’ Experiences during the COVID-19 Pandemic: A Qualitative Study. Nurs. Crit. Care 2021, 26, 397–406. [Google Scholar] [CrossRef]
- Gohar, B.; Nowrouzi-Kia, B. The Forgotten (Invisible) Healthcare Heroes: Experiences of Canadian Medical Laboratory Employees Working During the Pandemic. Front. Psychiatry 2022, 13, 854507. [Google Scholar] [CrossRef] [PubMed]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of Data Collection in Qualitative Research: Interviews and Focus Groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Microsoft. Microsoft Teams 22.08.1; Microsoft: Redmond, WA, USA, 2017. [Google Scholar]
- Almujlli, G.; Alrabah, R.; Al-Ghosen, A.; Munshi, F. Conducting Virtual Focus Groups During the COVID-19 Epidemic Utilizing Videoconferencing Technology: A Feasibility Study. Cureus 2022, 14, e23540. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.; Rafinejad-Farahani, B.; Moodie, S.; O’Hagan, R.; Glista, D. A Scoping Review of Virtual Focus Group Methods Used in Rehabilitation Sciences. Int. J. Qual. Methods 2021, 20, 160940692110422. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Quirkos. Quirkos Software 2.5.3; Quirkos: Edinburgh, UK, 2021. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Arnetz, J.E.; Goetz, C.M.; Arnetz, B.B.; Arble, E. Nurse Reports of Stressful Situations during the COVID-19 Pandemic: Qualitative Analysis of Survey Responses. Int. J. Environ. Res. Public Health 2020, 17, 8126. [Google Scholar] [CrossRef]
- Berkhout, S.G.; Sheehan, K.A.; Abbey, S.E. Individual- and Institutional-Level Concerns of Health Care Workers in Canada During the COVID-19 Pandemic: A Qualitative Analysis. JAMA Netw. Open 2021, 4, e2118425. [Google Scholar] [CrossRef]
- Brophy, J.T.; Keith, M.M.; Hurley, M.; McArthur, J.E. Sacrificed: Ontario Healthcare Workers in the Time of COVID-19. New Solut. A J. Environ. Occup. Health Policy 2021, 30, 267–281. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among Front-Line Health-Care Workers and the General Community: A Prospective Cohort Study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Schwartz, K.L.; Achonu, C.; Buchan, S.A.; Brown, K.A.; Lee, B.; Whelan, M.; Wu, J.H.; Garber, G. Epidemiology, Clinical Characteristics, Household Transmission, and Lethality of Severe Acute Respiratory Syndrome Coronavirus-2 Infection among Healthcare Workers in Ontario, Canada. PLoS ONE 2020, 15, e0244477. [Google Scholar] [CrossRef] [PubMed]
- Hoernke, K.; Djellouli, N.; Andrews, L.; Lewis-Jackson, S.; Manby, L.; Martin, S.; Vanderslott, S.; Vindrola-Padros, C. Frontline Healthcare Workers’ Experiences with Personal Protective Equipment during the COVID-19 Pandemic in the UK: A Rapid Qualitative Appraisal. BMJ Open 2021, 11, e046199. [Google Scholar] [CrossRef] [PubMed]
- Lau, Y.-Y.; Dulebenets, M.A.; Yip, H.-T.; Tang, Y.-M. Healthcare Supply Chain Management under COVID-19 Settings: The Existing Practices in Hong Kong and the United States. Healthcare 2022, 10, 1549. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and Somatic Symptoms among Frontline Healthcare Professionals at the Peak of the Italian COVID-19 Pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef]
- Fiabane, E.; Gabanelli, P.; La Rovere, M.T.; Tremoli, E.; Pistarini, C.; Gorini, A. Psychological and Work-Related Factors Associated with Emotional Exhaustion among Healthcare Professionals during the COVID-19 Outbreak in Italian Hospitals. Nurs. Health Sci. 2021, 23, 670–675. [Google Scholar] [CrossRef]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of Covid-19 Lockdown on Mental Health and Sleep Disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef] [PubMed]
- Jalili, M.; Niroomand, M.; Hadavand, F.; Zeinali, K.; Fotouhi, A. Burnout among Healthcare Professionals during COVID-19 Pandemic: A Cross-Sectional Study. Int. Arch. Occup. Environ. Health 2021, 94, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Menon, G.R.; Yadav, J.; Aggarwal, S.; Singh, R.; Kaur, S.; Chakma, T.; Periyasamy, M.; Venkateswaran, C.; Singh, P.K.; Balachandar, R.; et al. Psychological Distress and Burnout among Healthcare Worker during COVID-19 Pandemic in India-A Cross-Sectional Study. PLoS ONE 2022, 17, e0264956. [Google Scholar] [CrossRef] [PubMed]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]
- Ślusarz, R.; Cwiekala-Lewis, K.; Wysokiński, M.; Filipska-Blejder, K.; Fidecki, W.; Biercewicz, M. Characteristics of Occupational Burnout among Nurses of Various Specialties and in the Time of the COVID-19 Pandemic—Review. Int. J. Environ. Res. Public Health 2022, 19, 13775. [Google Scholar] [CrossRef]
- Abbas, A.; Al-Otaibi, T.; Gheith, O.A.; Nagib, A.M.; Farid, M.M.; Walaa, M. Sleep Quality Among Healthcare Workers During the COVID-19 Pandemic and Its Impact on Medical Errors: Kuwait Experience. Turk. Thorac. J. 2021, 22, 142–148. [Google Scholar] [CrossRef]
- Bannai, A.; Tamakoshi, A. The Association between Long Working Hours and Health: A Systematic Review of Epidemiological Evidence. Scand. J. Work Environ. Health 2014, 40, 5–18. [Google Scholar] [CrossRef]
- Bondagji, D.; Fakeerh, M.; Alwafi, H.; Khan, A.A. The Effects of Long Working Hours on Mental Health Among Resident Physicians in Saudi Arabia. Psychol. Res. Behav. Manag. 2022, 15, 1545–1557. [Google Scholar] [CrossRef] [PubMed]
- Ervasti, J.; Pentti, J.; Nyberg, S.T.; Shipley, M.J.; Leineweber, C.; Sørensen, J.K.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Long Working Hours and Risk of 50 Health Conditions and Mortality Outcomes: A Multicohort Study in Four European Countries. Lancet Reg. Health Eur. 2021, 11, 100212. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.; Chan, A.H.S.; Ngan, S.C. The Effect of Long Working Hours and Overtime on Occupational Health: A Meta-Analysis of Evidence from 1998 to 2018. Int. J. Environ. Res. Public Health 2019, 16, 2102. [Google Scholar] [CrossRef]
- Statistics Canada. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/220427/dq220427a-eng.htm (accessed on 3 August 2023).
- Martin, B.; Kaminski-Ozturk, N.; O’Hara, C.; Smiley, R. Examining the Impact of the COVID-19 Pandemic on Burnout and Stress Among U.S. Nurses. J. Nurs. Regul. 2023, 14, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Tabur, A.; Elkefi, S.; Emhan, A.; Mengenci, C.; Bez, Y.; Asan, O. Anxiety, Burnout and Depression, Psychological Well-Being as Predictor of Healthcare Professionals’ Turnover during the COVID-19 Pandemic: Study in a Pandemic Hospital. Healthcare 2022, 10, 525. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Brown, R.; Sinsky, C.; Linzer, M. The Association of Work Overload with Burnout and Intent to Leave the Job Across the Healthcare Workforce During COVID-19. J. Gen. Intern. Med. 2023, 38, 1920–1927. [Google Scholar] [CrossRef]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Bradley, K.A.; Wipf, J.E.; Back, A.L. Burnout and Self-Reported Patient Care in an Internal Medicine Residency Program. Ann. Intern. Med. 2002, 136, 358–367. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J. Burnout and Medical Errors among American Surgeons. Ann. Surg. 2010, 251, 995–1000. [Google Scholar] [CrossRef]
- Karakachian, A.; Colbert, A. Nurses’ Moral Distress, Burnout, and Intentions to Leave: An Integrative Review. J. Forensic Nurs. 2019, 15, 133–142. [Google Scholar] [CrossRef]
- Sheppard, K.N.; Runk, B.G.; Maduro, R.S.; Fancher, M.; Mayo, A.N.; Wilmoth, D.D.; Morgan, M.K.; Zimbro, K.S. Nursing Moral Distress and Intent to Leave Employment During the COVID-19 Pandemic. J. Nurs. Care Qual. 2022, 37, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Lui, J.N.M.; Andres, E.B.; Johnston, J.M. Presenteeism Exposures and Outcomes amongst Hospital Doctors and Nurses: A Systematic Review. BMC Health Serv. Res. 2018, 18, 985. [Google Scholar] [CrossRef] [PubMed]
- Shan, G.; Wang, S.; Wang, W.; Guo, S.; Li, Y. Presenteeism in Nurses: Prevalence, Consequences, and Causes From the Perspectives of Nurses and Chief Nurses. Front. Psychiatry 2021, 11, 584040. [Google Scholar] [CrossRef]
- Letvak, S.A.; Ruhm, C.J.; Gupta, S.N. Nurses’ Presenteeism and Its Effects on Self-Reported Quality of Care and Costs. Am. J. Nurs. 2012, 112, 30–38, quiz 48, 39. [Google Scholar] [CrossRef]
- Niven, K.; Ciborowska, N. The Hidden Dangers of Attending Work While Unwell: A Survey Study of Presenteeism among Pharmacists. Int. J. Stress Manag. 2015, 22, 207–221. [Google Scholar] [CrossRef]
- Rainbow, J.G.; Drake, D.A.; Steege, L.M. Nurse Health, Work Environment, Presenteeism and Patient Safety. West. J. Nurs. Res. 2020, 42, 332–339. [Google Scholar] [CrossRef]
- Alahiane, L.; Zaam, Y.; Abouqal, R.; Belayachi, J. Factors Associated with Recognition at Work among Nurses and the Impact of Recognition at Work on Health-Related Quality of Life, Job Satisfaction and Psychological Health: A Single-Centre, Cross-Sectional Study in Morocco. BMJ Open 2023, 13, e051933. [Google Scholar] [CrossRef] [PubMed]
- Deressa, B.; Adugna, K.; Bezane, B.; Jabessa, M.; Wayessa, G.; Kebede, A.; Tefera, G.; Demissie, Y. The Relationship Between Organizational Commitment and Organizational Justice Among Health Care Workers in Ethiopian Jimma Zone Public Health Facilities. J. Healthc. Leadersh. 2022, 14, 5–16. [Google Scholar] [CrossRef]
- Mengstie, M.M. Perceived Organizational Justice and Turnover Intention among Hospital Healthcare Workers. BMC Psychol. 2020, 8, 19. [Google Scholar] [CrossRef]
- Al-Qathmi, A.; Zedan, H. The Effect of Incentive Management System on Turnover Rate, Job Satisfaction and Motivation of Medical Laboratory Technologists. Health Serv. Res. Manag. Epidemiol. 2021, 8, 2333392820988404. [Google Scholar] [CrossRef]
- Hussain, M.K.; Khayat, R.A.M. The Impact of Transformational Leadership on Job Satisfaction and Organisational Commitment Among Hospital Staff: A Systematic Review. J. Health Manag. 2021, 23, 614–630. [Google Scholar] [CrossRef]
- Labrague, L.J.; Nwafor, C.E.; Tsaras, K. Influence of Toxic and Transformational Leadership Practices on Nurses’ Job Satisfaction, Job Stress, Absenteeism and Turnover Intention: A Cross-sectional Study. J. Nurs. Manag. 2020, 28, 1104–1113. [Google Scholar] [CrossRef]
- Musinguzi, C.; Namale, L.; Rutebemberwa, E.; Dahal, A.; Nahirya-Ntege, P.; Kekitiinwa, A. The Relationship between Leadership Style and Health Worker Motivation, Job Satisfaction and Teamwork in Uganda. J. Healthc. Leadersh. 2018, 10, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Gohar, B.; Larivière, M.; Lightfoot, N.; Wenghofer, E.; Larivière, C.; Nowrouzi-Kia, B. Meta-Analysis of Nursing-Related Organizational and Psychosocial Predictors of Sickness Absence. Occup. Med. 2020, 70, 593–601. [Google Scholar] [CrossRef]
- Vroom, V.H.; Jago, A.G. The New Leadership: Managing Participation in Organizations; Prentice Hall: Hoboken, NJ, USA, 1988. [Google Scholar]
- Specchia, M.L.; Cozzolino, M.R.; Carini, E.; Di Pilla, A.; Galletti, C.; Ricciardi, W.; Damiani, G. Leadership Styles and Nurses’ Job Satisfaction. Results of a Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1552. [Google Scholar] [CrossRef] [PubMed]
- Gohar, B.; Larivière, M.; Nowrouzi-Kia, B. Sickness Absence in Healthcare Workers during the COVID-19 Pandemic. Occup. Med. 2020, 70, 338–342. [Google Scholar] [CrossRef]
- Statistics Canada. Available online: https://www.statcan.gc.ca/en/subjects-start/population_and_demography/40-million (accessed on 3 August 2023).
- Medical Laboratory Professionals’ Association of Ontario. Available online: https://www.mlpao.org/post/media-release-new-skills-development-fund-program-will-train-50-iemlts-to-support-shortage (accessed on 3 August 2023).
- The Michener Institute of Education at UHN. Available online: https://michener.ca/nova-scotia-training-more-medical-laboratory-technologists-through-innovative-partnership-with-michener/ (accessed on 3 August 2023).
- Azeem, S.M.; Akhtar, N. The Influence of Work Life Balance and Job Satisfaction on Organizational Commitment of Healthcare Employees. Int. J. Hum. Resour. Stud. 2014, 4, 18. [Google Scholar] [CrossRef]
- Reitz, K.M.; Terhorst, L.; Smith, C.N.; Campwala, I.K.; Owoc, M.S.; Downs-Canner, S.M.; Diego, E.J.; Switzer, G.E.; Rosengart, M.R.; Myers, S.P. Healthcare Providers’ Perceived Support from Their Organization Is Associated with Lower Burnout and Anxiety amid the COVID-19 Pandemic. PLoS ONE 2021, 16, e0259858. [Google Scholar] [CrossRef] [PubMed]
- Giusino, D.; De Angelis, M.; Mazzetti, G.; Christensen, M.; Innstrand, S.T.; Faiulo, I.R.; Chiesa, R. “We All Held Our Own”: Job Demands and Resources at Individual, Leader, Group, and Organizational Levels During COVID-19 Outbreak in Health Care. A Multi-Source Qualitative Study. Workplace Health Saf. 2022, 70, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Sangal, R.B.; Bray, A.; Reid, E.; Ulrich, A.; Liebhardt, B.; Venkatesh, A.K.; King, M. Leadership Communication, Stress, and Burnout among Frontline Emergency Department Staff amid the COVID-19 Pandemic: A Mixed Methods Approach. Healthcare 2021, 9, 100577. [Google Scholar] [CrossRef]
- Shah, M.; Roggenkamp, M.; Ferrer, L.; Burger, V.; Brassil, K.J. Mental Health and COVID-19: The Psychological Implications of a Pandemic for Nurses. Clin. J. Oncol. Nurs. 2021, 25, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.L.; Goh, C.F.; Adam, M.B.H.; Tan, O.K. Transformational Leadership, Empowerment, and Job Satisfaction: The Mediating Role of Employee Empowerment. Hum. Resour. Health 2016, 14, 73. [Google Scholar] [CrossRef] [PubMed]
- Zaresani, A.; Scott, A. Does Digital Health Technology Improve Physicians’ Job Satisfaction and Work–Life Balance? A Cross-Sectional National Survey and Regression Analysis Using an Instrumental Variable. BMJ Open 2020, 10, e041690. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Gender | Age (Years) | Province | Marital Status | Location | Work Setting | Total Length of Practice | Length of Practice at Current Location |
|---|---|---|---|---|---|---|---|
| Men = 4 Women = 23 | 21–25 = 3 26–30 = 4 31–35 = 5 36–40 = 8 41–45 = 2 46–50 = 1 51–55 = 4 (M = 37, SD = 9.3) | Ontario = 9 British Columbia = 8 Alberta = 6 Nova Scotia = 2 Manitoba = 1 Newfoundland and Labrador = 1 | Single = 11 Common-Law = 4 Married = 12 | Urban = 19 Rural = 4 Mixed = 4 | Hospital = 19 Private laboratories = 2 Provincial laboratory = 1 Clinic = 1 Community center = 1 Non-profit organization = 1 Manufacturing/distribution = 2 | Min. = 2 years Max. = 35 years (M = 10, SD = 8.7) | Min. = 2 months Max. = 26 years (M = 6, SD = 6.6) |
| Themes | Subthemes |
|---|---|
| Theme 1: Unexpected challenges navigating through the uncertainties of an ever-evolving pandemic | Subtheme 1: Fear of the unknown and contagiousness of the virus Subtheme 2: Adapting to an ever-changing and unpredictable environment Subtheme 3: Resource constraints and supply chain challenges |
| Theme 2: Implications of staff shortage for the well-being of MLTs and the quality of patient care | Subtheme 1: Burnout due to increased workload and prolonged work hours leading to attrition Subtheme 2: Increased testing errors compromising patient care Subtheme 3: Moral distress and guilt faced by MLTs during the pandemic |
| Theme 3: Revealing the realities of the hidden, yet indispensable MLTs in predominantly non-patient-facing roles | Subtheme 1: Limited understanding and recognition of the importance and role of MLTs in healthcare Subtheme 2: Lack of compensation despite increased work demands and responsibilities Subtheme 3: Lack of management affecting work morale Subtheme 4: Lack of available mental health supports and services for MLTs |
| Theme 4: Leveraging insights from the COVID-19 pandemic to enhance healthcare practices and preparedness | Subtheme 1: Recognizing one’s own limitations and establishing boundaries for a healthy work-life balance Subtheme 2: Integrating leadership and communication strategies in preparedness plans for effective public health emergency response Subtheme 3: Enhancing healthcare quality and efficiency through electronic health record integration |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dignos, P.N.; Khan, A.; Gardiner-Davis, M.; Papadopoulos, A.; Nowrouzi-Kia, B.; Sivanthan, M.; Gohar, B. Hidden and Understaffed: Exploring Canadian Medical Laboratory Technologists’ Pandemic Stressors and Lessons Learned. Healthcare 2023, 11, 2736. https://doi.org/10.3390/healthcare11202736
Dignos PN, Khan A, Gardiner-Davis M, Papadopoulos A, Nowrouzi-Kia B, Sivanthan M, Gohar B. Hidden and Understaffed: Exploring Canadian Medical Laboratory Technologists’ Pandemic Stressors and Lessons Learned. Healthcare. 2023; 11(20):2736. https://doi.org/10.3390/healthcare11202736
Chicago/Turabian StyleDignos, Patricia Nicole, Ayesha Khan, Michael Gardiner-Davis, Andrew Papadopoulos, Behdin Nowrouzi-Kia, Myuri Sivanthan, and Basem Gohar. 2023. "Hidden and Understaffed: Exploring Canadian Medical Laboratory Technologists’ Pandemic Stressors and Lessons Learned" Healthcare 11, no. 20: 2736. https://doi.org/10.3390/healthcare11202736
APA StyleDignos, P. N., Khan, A., Gardiner-Davis, M., Papadopoulos, A., Nowrouzi-Kia, B., Sivanthan, M., & Gohar, B. (2023). Hidden and Understaffed: Exploring Canadian Medical Laboratory Technologists’ Pandemic Stressors and Lessons Learned. Healthcare, 11(20), 2736. https://doi.org/10.3390/healthcare11202736