

Promoting Respectful Maternity Care by Reducing Unnecessary Episiotomies: Experiences from Centers of Excellence for Breastfeeding in Vietnam

 , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
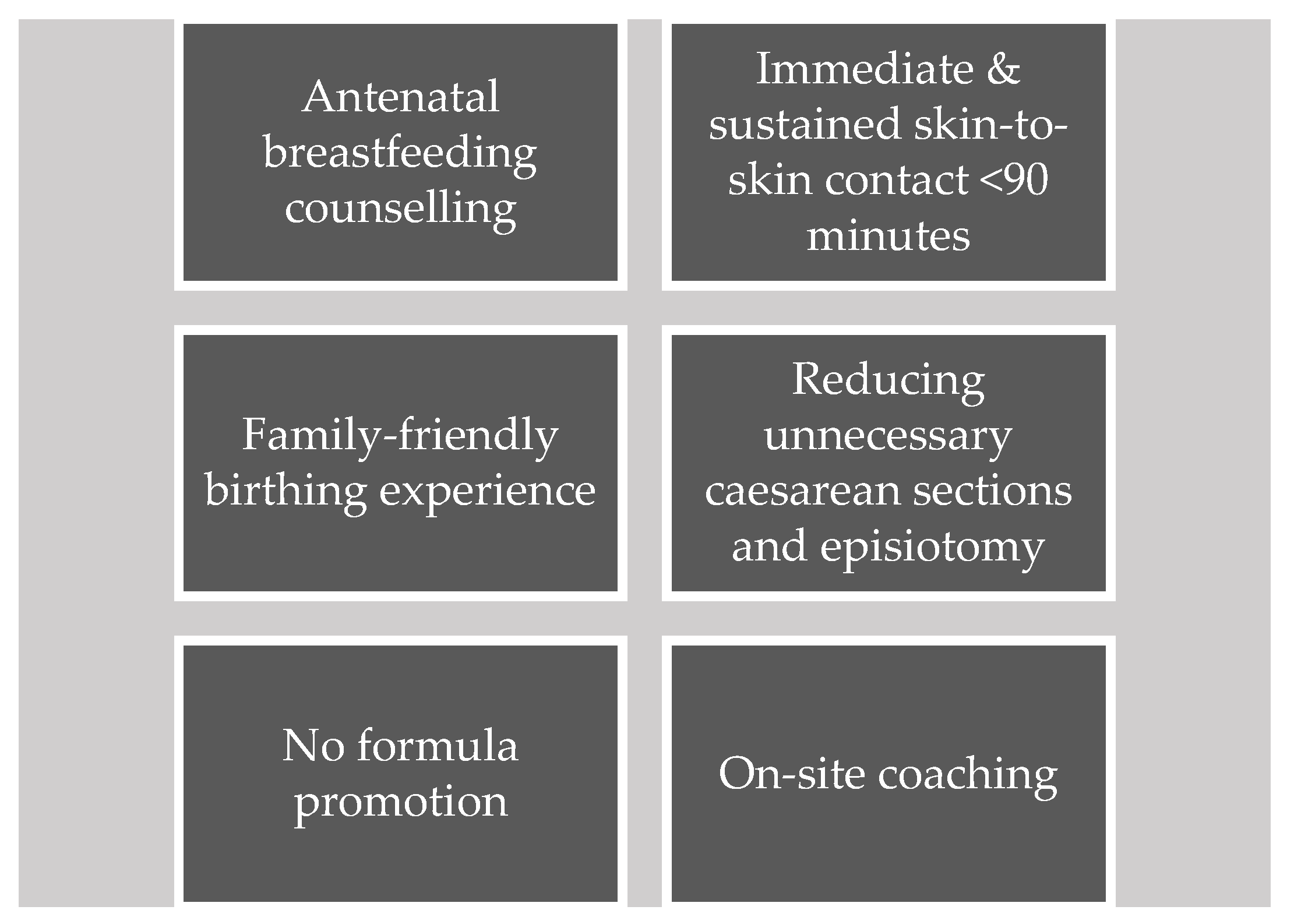
2.1. Program Description
2.2. Episiotomy Guidelines Development
2.3. Training Session Development
2.4. Recruitment
2.5. Data Collection
3. Results
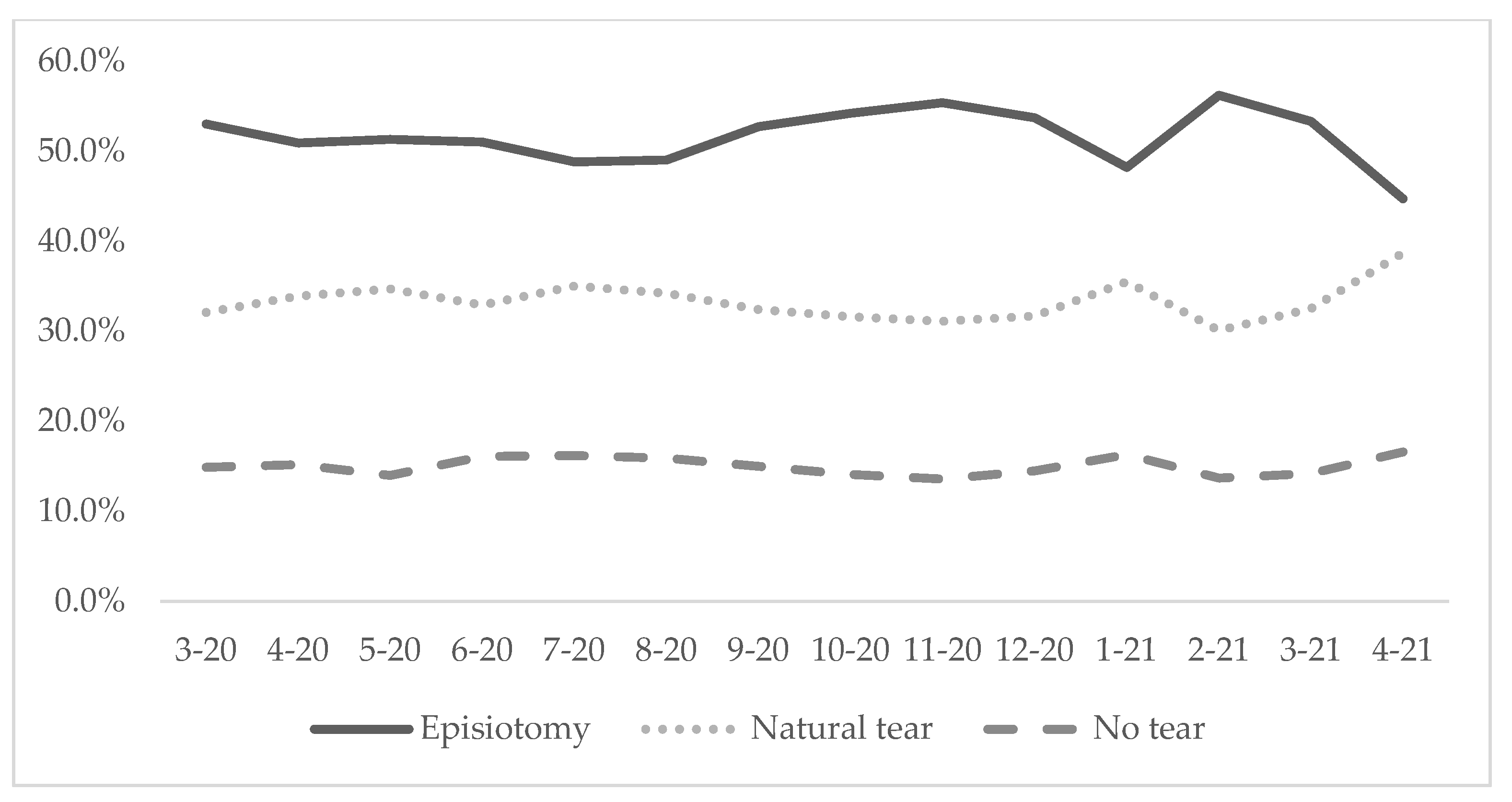
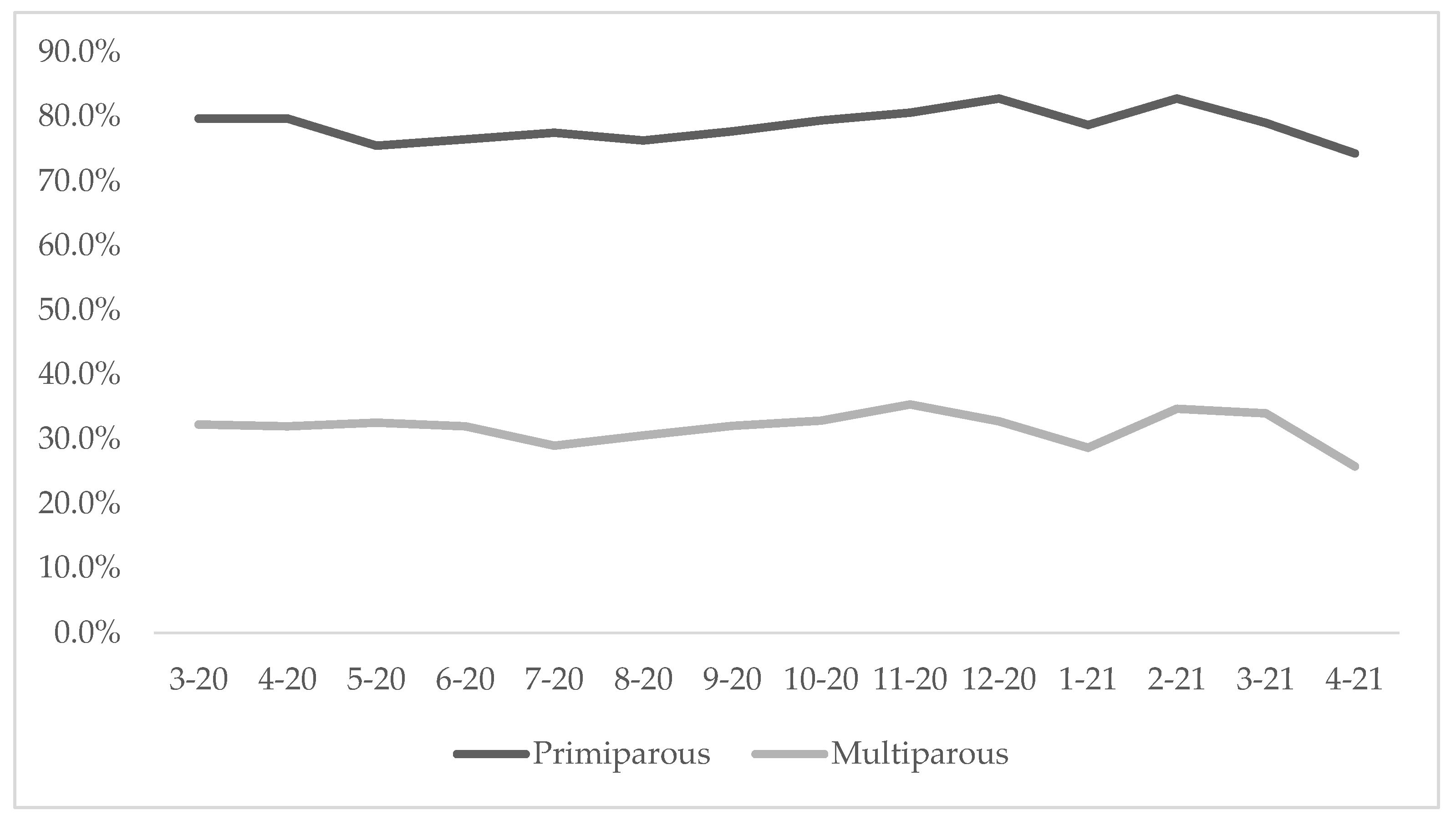
3.1. Episiotomy Usage
3.2. Facilitators to Adopting the New Episiotomy Policy into Routine Practice
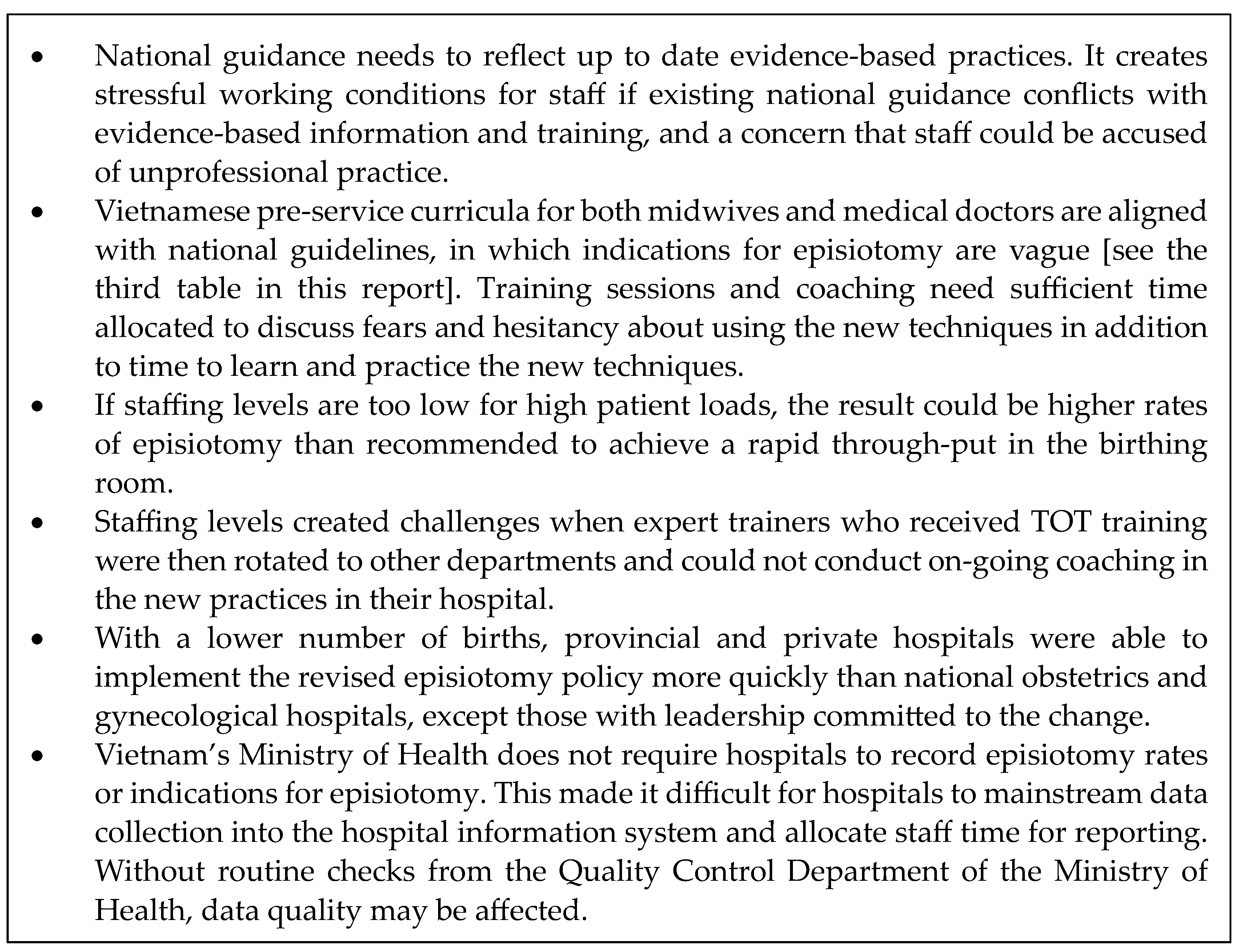
3.3. Challenges to Adopting the New Episiotomy Policy
3.4. Policy Advocacy
4. Discussion
4.1. Policy Advocacy
- Updating the national technical guideline by the Department of Maternal & Child Health to reflect evidence-based practice and clarity in its implementation.
- Allocating ongoing budget for training and coaching for trainers and staff members.
- Working with best practice and teaching hospitals, such as the ones enrolled in the COE initiative and professional organizations of midwives and medical doctors, to recognize the updated guidance as an expected standard of professional practice.
4.2. Pre- and In-Service Learning
- Reviewing and including the updated guidance in the pre-service curriculum and clinical experiences for midwives and medical doctors.
- Establishing and sustaining a core group of health workers at each maternity facility to have responsibility for in-service training and ongoing skills coaching and monitoring of practice.
4.3. Communication
- Communicating with related and collaborating organizations to use the new episiotomy guideline in their activities.
- Including the recording, monitoring, and audit of episiotomy/tears as routine obstetric data collection and in quality indicators.
- Keeping mothers and fathers and significant influencers aware of the guidance and how it affects the health and well-being of mother and baby, including through media channels.
- Ensuring antenatal information provided to pregnant women includes the guidance and time to discuss how it applies to their individual situation.
- Delivering social and behavior change communication for health workers to increase their confidence and willingness to apply new clinical guidelines.
4.4. Monitoring and Evidence Generation
- Conducting qualitative and quantitative research on mothers’ experiences of episiotomy and the impact on their lives after childbirth (e.g., quality of life assessment), using data to develop advocacy messages and materials targeted toward policy makers and service users.
- Carrying out an economic evaluation of the costs of episiotomy, including any negative outcomes, such as infection, arising from the intervention to ascertain the economic aspects of unnecessary episiotomy and savings through reducing rates in order to inform decision-making.
- Updating the health information system to include mandatory reporting on episiotomy rates to mainstream monitoring, improve data quality and compliance with the updated national technical guideline.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Province | Hospital | Average Annual Births | Type of Hospital | ||||
|---|---|---|---|---|---|---|---|---|
| National or Provincial | District | ObGyn/ObPed | Private | Data Included in This Report | ||||
| 1 | Ca Mau | Ca Mau Maternity—Pediatric Hospital | 8300 | X | X | |||
| 2 | Tran Van Thoi Area General Hospital | 2000 | X | |||||
| 3 | Hue | Phu Vang District Health Center | 1300 | X | X | |||
| 4 | Quang Nam | Vinh Duc General Hospital | 12,700 | X | X | |||
| 5 | Minh Thien General Hospital | 9500 | X | X | ||||
| 6 | Quang Nam Province General Hospital | 5000 | X | X | ||||
| 7 | Da Nang | Da Nang Hospital for Women and Children | 14,300 | X | X | |||
| 8 | Can Tho | Can Tho Obstetrics and Gynecology Hospital | 15,000 | X | X | |||
| 9 | Phuong Chau International General Hospital | 5000 | X | X | ||||
| 10 | Ho Chi Minh | Tu Du Hospital | 65,000 | X | X | |||
| 11 | Hung Vuong Hospital | 42,000 | X | X | X | |||
| 12 | Quang Ninh | Quang Ninh Obstetrics and Pediatrics Hospital | 6800 | X | X | X | ||
| Total | 186,900 | 8 | 4 | 6 | 3 | 4 | ||
References
- Jiang, H.; Qian, X.; Carroli, G.; Garner, P. Selective versus Routine Use of Episiotomy for Vaginal Birth. Cochrane Database Syst. Rev. 2017, 2017, CD000081. [Google Scholar] [CrossRef] [PubMed]
- Amorim, M.M.; Coutinho, I.C.; Melo, I.; Katz, L. Selective Episiotomy vs. Implementation of a Non-Episiotomy Protocol: A Randomized Clinical Trial. Reprod. Health 2017, 14, 55. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; United Nations Population Fund; United Nations Children’s Fund. Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors; World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/publications/i/item/9789241550215 (accessed on 21 March 2023).
- World Health Organization. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/260178/9789241550215-eng.pdf (accessed on 21 March 2023).
- World Health Organization Regional Office for the Western Pacific. Early Essential Newborn Care: Clinical Practice Pocket Guide; WHO Regional Office for the Western Pacific: Manila, Philippines, 2014; Available online: https://apps.who.int/iris/handle/10665/208158 (accessed on 21 March 2023).
- Nassar, A.H.; Visser, G.H.A.; Ayres-de-Campos, D.; Rane, A.; Gupta, S.; The FIGO Safe Motherhood and Newborn Health Committee. FIGO Statement: Restrictive Use Rather than Routine Use of Episiotomy. Int. J. Gynecol. Obstet. 2019, 146, 17–19. [Google Scholar] [CrossRef] [PubMed]
- International Confederation of Midwives. Essential Competencies for Midwifery Practice. 2019. Available online: https://www.internationalmidwives.org/assets/files/general-files/2019/10/icm-competencies-en-print-october-2019_final_18-oct-5db05248843e8.pdf (accessed on 21 March 2023).
- World Health Organization Regional Office for the Western Pacific. Meeting Report Second Biennial Meeting on Accelerating Progress in Early Essential Newborn Care (EENC) Report. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272803/9789290618492-eng.pdf?sequence=1&isAllowed=y (accessed on 21 March 2023).
- Nguyen, T.T.; Cashin, J.; Tran, H.T.; Hoang, T.A.; Mathisen, R.; Weissman, A.; Murray, J.C.S. Birth and Newborn Care Policies and Practices Limit Breastfeeding at Maternity Facilities in Vietnam. Front. Nutr. 2022, 9, 1041065. [Google Scholar] [CrossRef] [PubMed]
- Report on Maternity Web Tool—Te Whatu Ora—Health New Zealand. Available online: https://www.tewhatuora.govt.nz/our-health-system/data-and-statistics/report-on-maternity-web-tool/ (accessed on 22 February 2023).
- Australian Institute of Health and Welfare. National Core Maternity Indicators. Available online: https://www.aihw.gov.au/reports/mothers-babies/national-core-maternity-indicators/contents/about (accessed on 22 February 2023).
- Helse Nord RHF. Helseatlas: The Use of Obstetrics Healthcare Services in Norway During the Period 2015–2017. Available online: https://www.skde.no/helseatlas/v2/fodsel/ (accessed on 22 February 2023).
- Schantz, C.; Sim, K.L.; Ly, E.M.; Barennes, H.; Sudaroth, S.; Goyet, S. Reasons for Routine Episiotomy: A Mixed-Methods Study in a Large Maternity Hospital in Phnom Penh, Cambodia. Reprod. Health Matters 2015, 23, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Trinh, A.T.; Roberts, C.L.; Ampt, A.J. Knowledge, Attitude and Experience of Episiotomy Use among Obstetricians and Midwives in Viet Nam. BMC Pregnancy Childbirth 2015, 15, 101. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Petitjean, P.; Meunier, G.; Sibiude, J.; Mandelbrot, L. Evaluation of a Policy of Restrictive Episiotomy on the Incidence of Perineal Tears among Women with Spontaneous Vaginal Delivery: A Ten-Year Retrospective Study. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101870. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-J.S.; Oyama, I.A.; Hiraoka, M.; Minaglia, S.; Thomas, J.; Kaneshiro, B. Perineal Body Length Among Different Racial Groups in the First Stage of Labor. Urogynecology 2012, 18, 165. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for the Western Pacific. Third Biennial Meeting on Accelerating Progress in Early Essential Newborn Care (EENC): Synergies with Hospital Quality and Safety, Virtual Meeting, 1, 3, 4 and 9 December 2020: Meeting Report; WHO Regional Office for the Western Pacific: Manila, Philippines, 2020; Available online: https://apps.who.int/iris/handle/10665/340356 (accessed on 22 February 2023).
- Gu, S.; Pei, J.; Zhou, C.; Zhao, X.; Wan, S.; Zhang, J.; Adanlawo, A.; Luo, Z.; Wu, G.; Hua, X. Selective versus Routine Use of Episiotomy for Vaginal Births in Shanghai Hospitals, China: A Comparison of Policies. BMC Pregnancy Childbirth 2022, 22, 475. [Google Scholar] [CrossRef] [PubMed]
- Sagi-Dain, L.; Kreinin-Bleicher, I.; Bahous, R.; Gur Arye, N.; Shema, T.; Eshel, A.; Caspin, O.; Gonen, R.; Sagi, S. Is It Time to Abandon Episiotomy Use? A Randomized Controlled Trial (EPITRIAL). Int. Urogynecol. J. 2020, 31, 2377–2385. [Google Scholar] [CrossRef]
- Downe, S.; Lawrie, T.A.; Finlayson, K.; Oladapo, O.T. Effectiveness of Respectful Care Policies for Women Using Routine Intrapartum Services: A Systematic Review. Reprod. Health 2018, 15, 23. [Google Scholar] [CrossRef]
- Gadappa, S.N.; Deshpande, S.S. A Quasi-Experimental Study to Compare the Effect of Respectful Maternity Care Using Intrapartum Birth Companion of Her Choice on Maternal and Newborn Outcome in Tertiary Care Centre. J. Obs. Gynaecol. India 2021, 71 (Suppl. 2), 84–89. [Google Scholar] [CrossRef] [PubMed]
- General Statistics Office; UNICEF. Survey Measuring Viet Nam Sustainable Development Goal Indicators on Children and Women 2020–2021, Survey Findings Report. 2021. Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS6/East%20Asia%20and%20the%20Pacific/Viet%20Nam/2020-2021/Survey%20findings/Viet%20Nam%202020-21%20MICS-SDGCW_English.pdf (accessed on 1 March 2023).
- Alive & Thrive: Women and Children Benefit from Good Nutrition. Available online: https://www.aliveandthrive.org/en (accessed on 28 February 2023).
- Joyce, C.M.; Hou, S.S.-Y.; Ta, B.T.T.; Vu, D.H.; Mathisen, R.; Vincent, I.; Duc, V.N.; Nandi, A. The Association between a Novel Baby-Friendly Hospital Program and Equitable Support for Breastfeeding in Vietnam. Int. J. Environ. Res. Public Health 2021, 18, 6706. [Google Scholar] [CrossRef] [PubMed]
- Compendium of Skilled Breastfeeding Counselling Case Studies. Available online: https://www.globalbreastfeedingcollective.org/reports/compendium-skilled-breastfeeding-counselling-case-studies (accessed on 22 February 2023).
- Early Essential Newborn Care: Clinical Practice Pocket Guide. Available online: https://www.who.int/publications-detail-redirect/9789290616856 (accessed on 22 February 2023).
- Quyết Định 1377/QĐ-BYT Năm 2013 Hướng Dẫn QUY trình kỹ Thuật Khám Chữa Bệnh. Available online: https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Quyet-dinh-1377-QD-BYT-nam-2013-huong-dan-Quy-trinh-ky-thuat-kham-chua-benh-192513.aspx (accessed on 1 March 2023).
- Oanh, T.T.M.; Phuong, N.K.; Tuan, K.A. Sustainability and Resilience in the Vietnamese Health System. The Partnership for Health System Sustainability and Resilience (PHSSR). 2021. Available online: https://www3.weforum.org/docs/WEF_PHSSR_Vietnam_Report.pdf (accessed on 1 March 2023).
- Omer-Salim, A. Assessing the Effectiveness of the Center of Excellence for Breastfeeding Initiative in Viet Nam; Unpublished Program Evaluation; World Alliance for Breastfeeding Action: Uppsala, Sweden, 2021. [Google Scholar]
- De Walque, D.; Kandpal, E.; Wagstaff, A.; Friedman, J.; Neelsen, S.; Piatti-Fünfkirchen, M.; Sautmann, A.; Shapira, G.; Van de Poel, E. Improving Effective Coverage in Health: Do Financial Incentives Work? The World Bank: Washington, DC, USA, 2022. [Google Scholar] [CrossRef]




| Country | National Hospital (%) | Subnational Level Hospital (%) |
|---|---|---|
| Vietnam 2 | 71 | 70 |
| Lao PDR 3 | 36 | 30 |
| Cambodia 2 | 3 | 26 |
| China 3 | 27 | 25 |
| Mongolia 3 | 11 | 11 |
| Papua New Guinea 2 | 0 | 23 |
| Philippines 2 | 29 | 29 |
| Solomon Islands 2 | 0 | 27 |
| An episiotomy should only be performed when indicated by: |
|
| Episiotomy indications must be written in the medical record |
| * Definition of abnormal progression of labor: |
|
| Vietnam’s National Technical Guideline on Indications for Episiotomy | Analysis |
|---|---|
| 1. Maternal causes: - The perineum is thick, hard, swelling due to prolonged labor or many vaginal examinations | “The perineum is thick, hard, swelling” is a vague indication. In many cases, it is due to the limited waiting time for normal labor. A&T proposes to delete the “thick, hard, swelling perineum” indication and keep the indication of “prolonged labor”, which has been defined in the proposed practice guideline indication 1 of “abnormal progression of labor”. |
| - Maternal disease: heart failure, high blood pressure, pre-eclampsia… | Covered in indication 1 of “abnormal progression of labor”. |
| 2. Fetal causes: - Macrosomia | Macrosomia often leads to “prolonged labor” or “shoulder dystocia”, which are covered in the new indications. |
| - Abnormal presentations: occipital posterior position, face presentation, breech presentation | Occipital posterior position may be associated with caesarean, vacuum, or forceps, which are covered in indication 3. Face presentation often leads to prolonged labor, which is covered in indication 1. Breech presentation often leads to prolonged labor or fetal distress, which are covered in indication 1. |
| - Premature, fetal distress | Episiotomy is only needed in the case of fetal distress, covered in indication 2. |
| 3. Instrumental delivery (forceps, vacuum, breech presentation) | Covered in indication 3 of “vacuum or forceps childbirth”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vu, D.H.; Ta, B.T.T.; Aasen, I.L.; Le, D.Q.T.; Mathisen, R.; Becker, G.E.; Phan, H.T.; Bui, C.M.; Nguyen, T.T.K.; Hoang, S.T.T.; et al. Promoting Respectful Maternity Care by Reducing Unnecessary Episiotomies: Experiences from Centers of Excellence for Breastfeeding in Vietnam. Healthcare 2023, 11, 2520. https://doi.org/10.3390/healthcare11182520
Vu DH, Ta BTT, Aasen IL, Le DQT, Mathisen R, Becker GE, Phan HT, Bui CM, Nguyen TTK, Hoang STT, et al. Promoting Respectful Maternity Care by Reducing Unnecessary Episiotomies: Experiences from Centers of Excellence for Breastfeeding in Vietnam. Healthcare. 2023; 11(18):2520. https://doi.org/10.3390/healthcare11182520
Chicago/Turabian StyleVu, Duong Hoang, Binh T. T. Ta, Ina Landau Aasen, Dai Q. T. Le, Roger Mathisen, Genevieve E. Becker, Hang Thi Phan, Cuong Minh Bui, Trinh Thi Kieu Nguyen, Suong Thi Thu Hoang, and et al. 2023. "Promoting Respectful Maternity Care by Reducing Unnecessary Episiotomies: Experiences from Centers of Excellence for Breastfeeding in Vietnam" Healthcare 11, no. 18: 2520. https://doi.org/10.3390/healthcare11182520
APA StyleVu, D. H., Ta, B. T. T., Aasen, I. L., Le, D. Q. T., Mathisen, R., Becker, G. E., Phan, H. T., Bui, C. M., Nguyen, T. T. K., Hoang, S. T. T., & Cashin, J. (2023). Promoting Respectful Maternity Care by Reducing Unnecessary Episiotomies: Experiences from Centers of Excellence for Breastfeeding in Vietnam. Healthcare, 11(18), 2520. https://doi.org/10.3390/healthcare11182520