
Cost–Effectiveness Analysis of Pharmacist Adherence Interventions in People Living with HIV/AIDS in Pakistan

 ,
,  ,
,  , , , and
, , , and
Abstract
1. Background
2. Methods
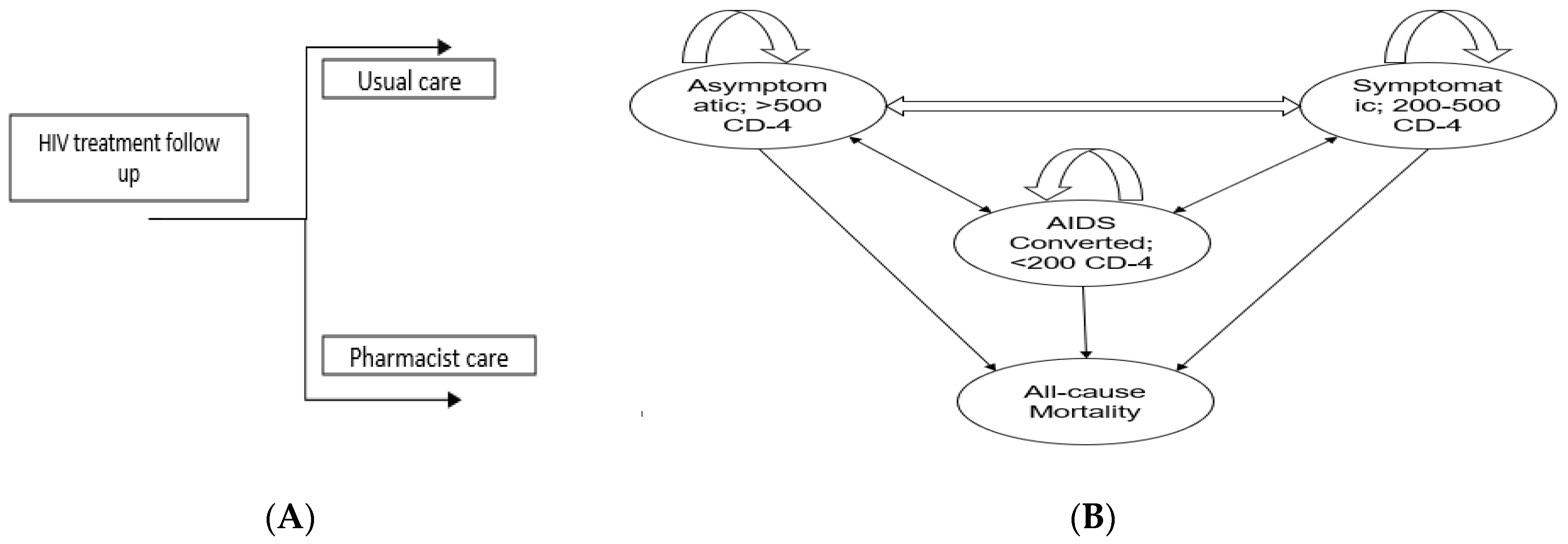
2.1. Intervention Trial
2.2. Model Structure
2.3. Model Inputs and Data Sources
2.4. Willingness to Pay
2.5. Statistical Analysis
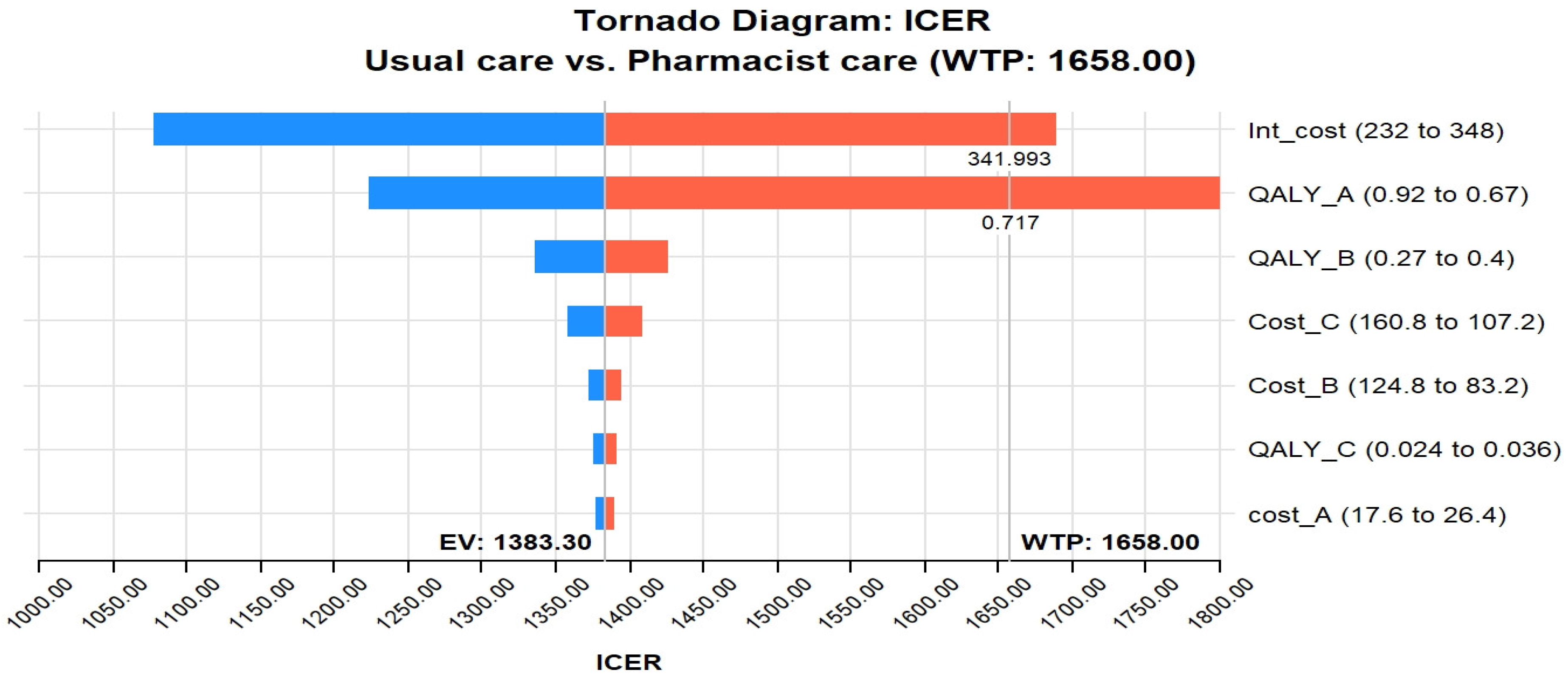
2.6. Sensitivity Analysis
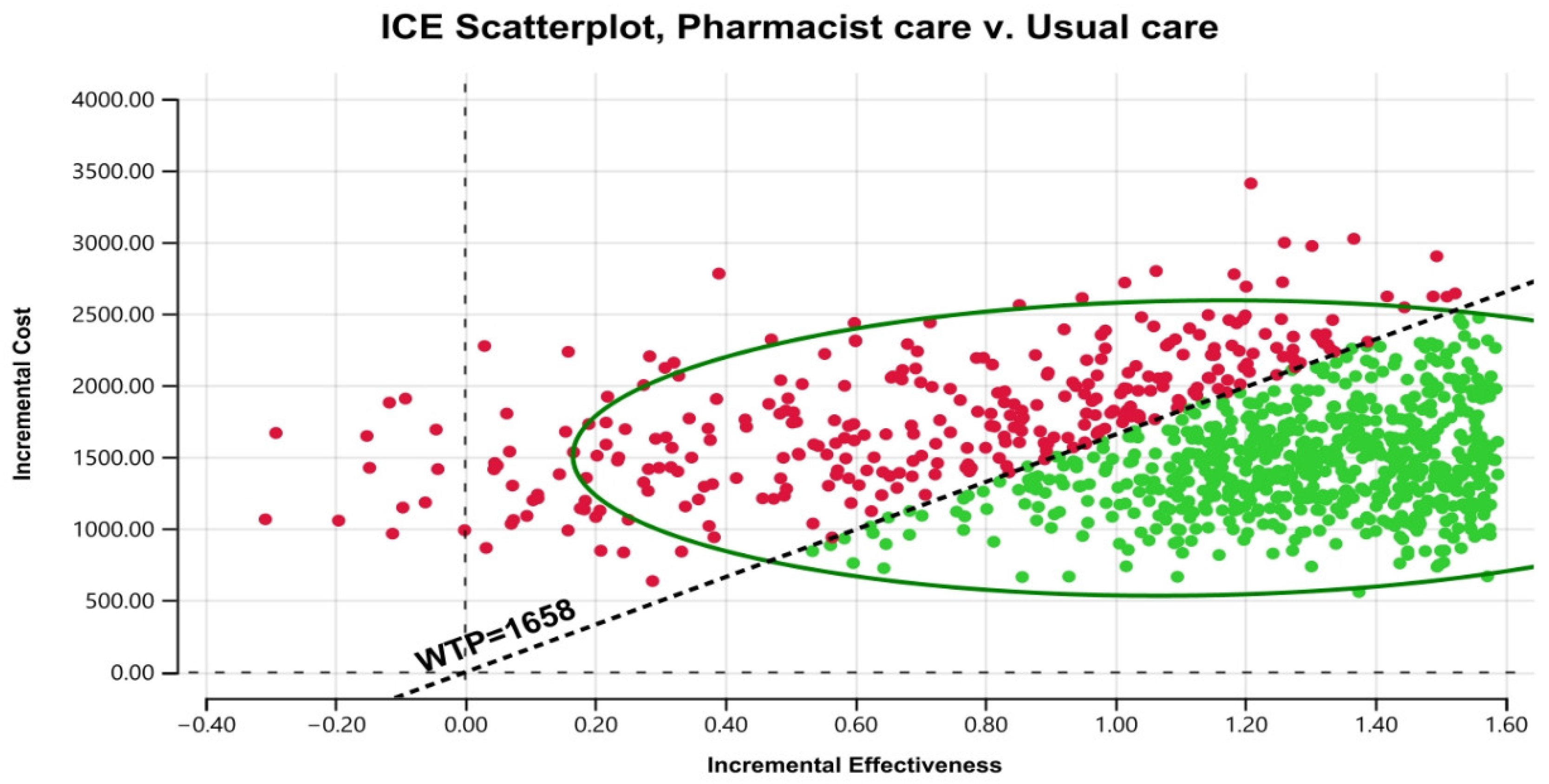
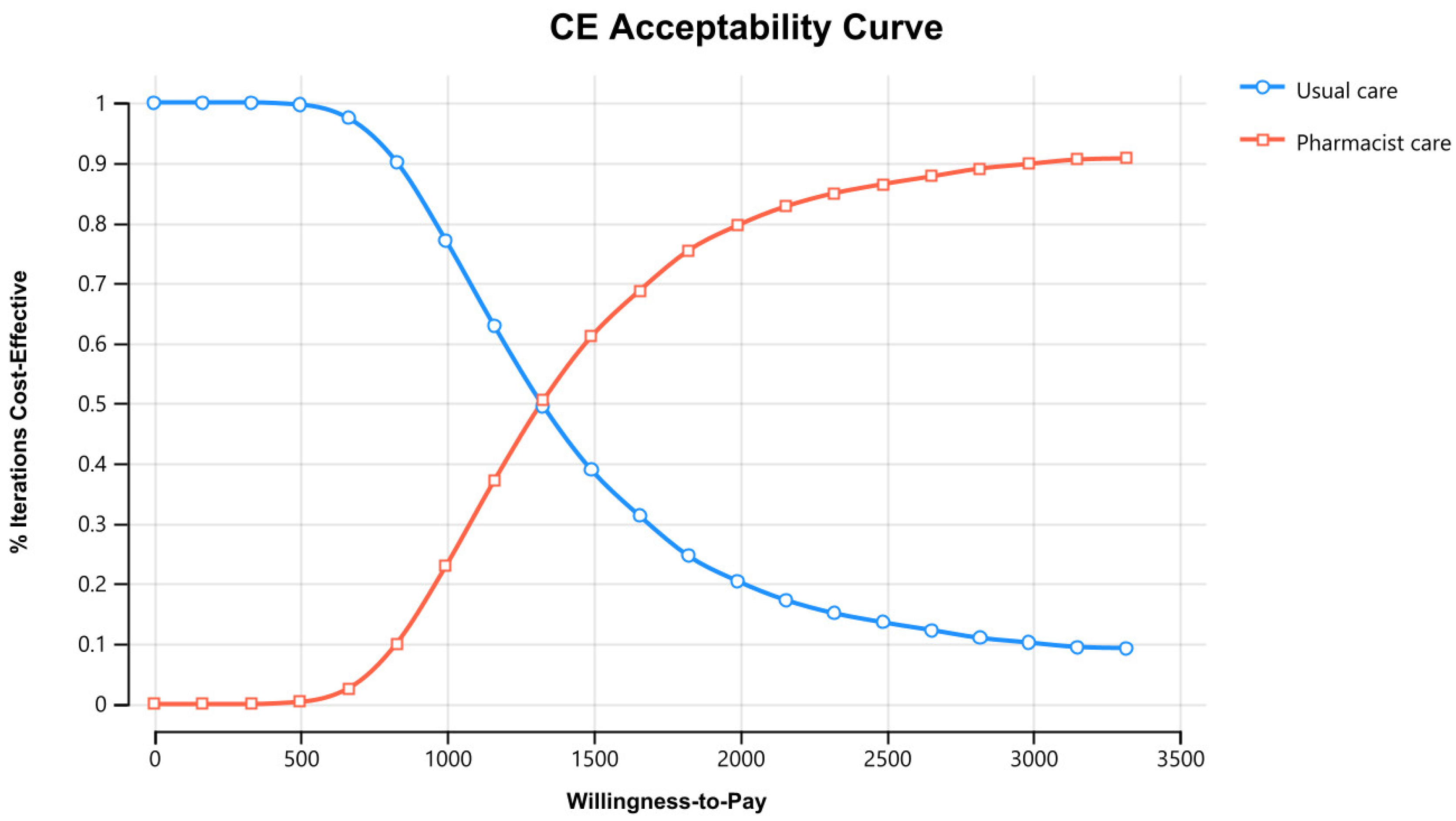
2.7. Probabilistic Sensitivity Analysis (PSA)
3. Results
3.1. Base Case Analysis
3.2. Sensitivity Analysis
3.3. Probabilistic Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV & AIDS Statistics Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 7 February 2023).
- Ahmed, A.; Saqlain, M.; Akhtar, N.; Hashmi, F.; Blebil, A.; Dujaili, J.; Umair, M.M.; Bukhsh, A. Translation and cross-cultural adaptation of WHOQOL-HIV Bref among people living with HIV/AIDS in Pakistan. Health Qual. Life Outcomes 2021, 19, 48. [Google Scholar] [CrossRef]
- NACP. National AIDS Control Programme of Pakistan, Ministry of National Health Services Regulation and Coordination, Govt of Pakistan. Available online: https://nacp.gov.pk/ (accessed on 22 August 2022).
- Ahmed, A.; Hashmi, F.K.; Khan, G.M. HIV outbreaks in Pakistan. Lancet HIV 2019, 6, e418. [Google Scholar] [CrossRef]
- Ahmed, A. Barriers and Facilitators of Antiretrovirals Adherence and Evaluation of Cost Effectiveness of Pharmaceutical Care Interventions to Improve the Health Outcomes of People Living with HIV/AIDS. Ph.D. Thesis, Monash University, Jaya, Malaysia, 2023. [Google Scholar]
- Ahmed, A.; Saqlain, M.; Bashir, N.; Dujaili, J.; Hashmi, F.; Mazhar, F.; Khan, A.; Jabeen, M.; Blebil, A.; Awaisu, A. Health-related quality of life and its predictors among adults living with HIV/AIDS and receiving antiretroviral therapy in Pakistan. Qual. Life Res. 2021, 30, 1653–1664. [Google Scholar] [CrossRef]
- Nurwijayanti, N.; Rias, Y.A.; Nasution, N.; Samsudin, R.R.; Priyono, D.; Rosyad, Y.S. Synergist effect of antiretroviral therapy adherence and viral load suppression on quality of life of people with HIV/AIDS. Br. J. Nurs. 2023, 32, S12–S18. [Google Scholar] [CrossRef] [PubMed]
- Forsythe, S.S.; McGreevey, W.; Whiteside, A.; Shah, M.; Cohen, J.; Hecht, R.; Bollinger, L.A.; Kinghorn, A. Twenty years of antiretroviral therapy for people living with HIV: Global costs, health achievements, economic benefits. Health Aff. 2019, 38, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Dujaili, J.A.; Jabeen, M.; Umair, M.M.; Chuah, L.-H.; Hashmi, F.K.; Awaisu, A.; Chaiyakunapruk, N. Barriers and enablers for adherence to antiretroviral therapy among people living with HIV/AIDS in the era of COVID-19: A qualitative study from Pakistan. Front. Pharmacol. 2022, 12, 3968. [Google Scholar] [CrossRef] [PubMed]
- Azmach, N.N.; Hamza, T.A.; Husen, A.A. Socioeconomic and demographic statuses as determinants of adherence to antiretroviral treatment in HIV infected patients: A systematic review of the literature. Curr. HIV Res. 2019, 17, 161–172. [Google Scholar] [CrossRef]
- Jackson, S.D.; Wagner, K.R.; Yepes, M.; Harvey, T.D.; Higginbottom, J.; Pachankis, J.E. A pilot test of a treatment to address intersectional stigma, mental health, and HIV risk among gay and bisexual men of color. Psychotherapy 2022, 59, 96. [Google Scholar] [CrossRef]
- Jones, D.; Cook, R.; Cecchini, D.; Sued, O.; Bofill, L.; Weiss, S.; Waldrop-Valverde, D.; Lopez, M.R.; Spence, A. Examining adherence among challenging patients in public and private HIV care in Argentina. AIDS Behav. 2015, 19, 1619–1629. [Google Scholar] [CrossRef][Green Version]
- Wasti, S.P.; Simkhada, P.; Randall, J.; Freeman, J.V.; van Teijlingen, E. Factors influencing adherence to antiretroviral treatment in Nepal: A mixed-methods study. PLoS ONE 2012, 7, e35547. [Google Scholar] [CrossRef]
- Tessema, B.T.; Bune, G.T.; Mamo, Z.B. Non-Disclosure of HIV-Positive Serostatus: Unmatched Case–Control Study in People Living with HIV in Public Health Facilities of Gedeo Zone, Southern Ethiopia. HIV/AIDS-Res. Palliat. Care 2023, 15, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.; Lavoie, M.-C.; Bashorun, A.; Dalhatu, I.; Jahun, I.; Agbakwuru, C.; Boyd, M.; Stafford, K.; Swaminathan, M.; Aliyu, G. Individual and household factors associated with non-disclosure of positive HIV status in a population-based HIV serosurvey. AIDS 2023, 37, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Saqlain, M.; Umair, M.M.; Hashmi, F.K.; Saeed, H.; Amer, M.; Blebil, A.Q.; Dujaili, J.A. Stigma, Social Support, Illicit Drug Use, and Other Predictors of Anxiety and Depression Among HIV/AIDS Patients in Pakistan: A Cross-Sectional Study. Front. Public Health 2021, 9, 745545. [Google Scholar] [CrossRef]
- Ahmed, A.; Rehman, I.U.; Hong, A.C.L.; Hashmi, F.K.; Awaisu, A.; Chaiyakunapruk, N. Effect of pharmacist care on clinical outcomes among people living with HIV/AIDS: A systematic review and meta-analysis. Res. Soc. Adm. Pharm. 2022, 18, 2962–2980. [Google Scholar] [CrossRef]
- Cernasev, A.; Veve, M.P.; Hohmeier, K.C.; Summers, N.A.; Kumar, S. Importance of pharmacist-patient relationship in people living with HIV and concomitant opioid use disorder. Explor. Res. Clin. Soc. Pharm. 2021, 3, 100052. [Google Scholar] [CrossRef]
- Schafer, J.J.; Gill, T.K.; Sherman, E.M.; McNicholl, I.R.; Hawkins, B. ASHP guidelines on pharmacist involvement in HIV care. Am. J. Health-Syst. Pharm. 2016, 73, 468–494. [Google Scholar] [CrossRef]
- McNicholl, I.R.; Gandhi, M.; Hare, C.B.; Greene, M.; Pierluissi, E. A pharmacist-led program to evaluate and reduce polypharmacy and potentially inappropriate prescribing in older HIV-positive patients. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 1498–1506. [Google Scholar] [CrossRef]
- Dilworth, T.J.; Klein, P.W.; Mercier, R.-C.; Borrego, M.E.; Jakeman, B.; Pinkerton, S.D. Clinical and economic effects of a pharmacist-administered antiretroviral therapy adherence clinic for patients living with HIV. J. Manag. Care Spec. Pharm. 2018, 24, 165–172. [Google Scholar] [CrossRef]
- Ahmed, A.; Dujaili, J.; Hashmi, F.K.; Awaisu, A.; Chaiyakunapruk, N.; Hasan, S.S. The economic impact of pharmacist care for people living with HIV/AIDS: A systematic review. Explor. Res. Clin. Soc. Pharm. 2021, 3, 100066. [Google Scholar] [CrossRef]
- Ahmed, A.; Tanveer, M.; Dujaili, J.A.; Chuah, L.H.; Hashmi, F.K.; Awaisu, A. Pharmacist-Involved Antiretroviral Stewardship Programs in People Living with HIV/AIDS: A Systematic Review. AIDS Patient Care STDs 2023, 37, 31–52. [Google Scholar] [CrossRef]
- Lutz, S.; Heberling, M.; Goodlet, K.J. Patient perspectives of pharmacists prescribing HIV pre-exposure prophylaxis: A survey of patients receiving antiretroviral therapy. J. Am. Pharm. Assoc. 2021, 61, e75–e79. [Google Scholar] [CrossRef] [PubMed]
- Jackson, I.L.; Ukwe, C.V. Clinical outcomes of pharmaceutical care intervention in HIV positive patients with hypertension: A randomized controlled study. J. Clin. Pharm. Ther. 2021, 46, 1083–1094. [Google Scholar] [CrossRef] [PubMed]
- Crawford, N.D.; Myers, S.; Young, H.; Klepser, D.; Tung, E. The Role of Pharmacies in the HIV Prevention and Care Continuums: A Systematic Review. AIDS Behav. 2021, 25, 1819–1828. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Orjuela, C.; García-Molina, M.; De la Hoz-Restrepo, F. Is there something else beyond cost-effectiveness analysis for public health decision making? Value Health Reg. Issues 2020, 23, 1–5. [Google Scholar] [CrossRef]
- Bertram, M.Y.; Lauer, J.A.; Stenberg, K.; Edejer, T.T.T. Methods for the economic evaluation of health care interventions for priority setting in the health system: An update from WHO CHOICE. Int. J. Health Policy Manag. 2021, 10, 673. [Google Scholar] [CrossRef]
- Avanceña, A.L.; Prosser, L.A. Innovations in cost-effectiveness analysis that advance equity can expand its use in health policy. BMJ Glob. Health 2022, 7, e008140. [Google Scholar] [CrossRef]
- Ahmed, A.; Dujaili, J.A.; Chuah, L.H.; Hashmi, F.K.; Le, L.K.-D.; Khanal, S.; Awaisu, A.; Chaiyakunapruk, N. Cost-Effectiveness of Anti-retroviral Adherence Interventions for People Living with HIV: A Systematic Review of Decision Analytical Models. Appl. Health Econ. Health Policy 2023, 21, 731–750. [Google Scholar] [CrossRef]
- Sanders, G.D.; Maciejewski, M.L.; Basu, A. Overview of cost-effectiveness analysis. JAMA 2019, 321, 1400–1401. [Google Scholar] [CrossRef]
- Bilinski, A.; MacKay, E.; Salomon, J.A.; Pandya, A. Affordability and value in decision rules for cost-effectiveness: A survey of health economists. Value Health 2022, 25, 1141–1147. [Google Scholar] [CrossRef]
- Chatha, Z.F.; Rashid, U.; Olsen, S.; ud Din, F.; Khan, A.; Nawaz, K.; Gan, S.H.; Khan, G.M. Pharmacist-led counselling intervention to improve antiretroviral drug adherence in Pakistan: A randomized controlled trial. BMC Infect. Dis. 2020, 20, 874. [Google Scholar] [CrossRef]
- Sanders, G.D.; Neumann, P.J.; Basu, A.; Brock, D.W.; Feeny, D.; Krahn, M.; Kuntz, K.M.; Meltzer, D.O.; Owens, D.K.; Prosser, L.A. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: Second panel on cost-effectiveness in health and medicine. JAMA 2016, 316, 1093–1103. [Google Scholar] [CrossRef] [PubMed]
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: Updated reporting guidance for health economic evaluations. Int. J. Technol. Assess. Health Care 2022, 38, e13. [Google Scholar] [CrossRef] [PubMed]
- Pauker, S.G.; Kassirer, J.P. Decision analysis. In Medical Uses of Statistics; CRC Press: Boca Raton, FL, USA, 2019; pp. 159–179. [Google Scholar]
- Hiatt, J.; Hultquist, J.F.; McGregor, M.J.; Bouhaddou, M.; Leenay, R.T.; Simons, L.M.; Young, J.M.; Haas, P.; Roth, T.L.; Tobin, V. A functional map of HIV-host interactions in primary human T cells. Nat. Commun. 2022, 13, 1752. [Google Scholar] [CrossRef] [PubMed]
- Simmons, R.; Ciancio, B.; Kall, M.; Rice, B.; Delpech, V. Ten-year mortality trends among persons diagnosed with HIV infection in E ngland and W ales in the era of antiretroviral therapy: AIDS remains a silent killer. HIV Med. 2013, 14, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Xe Currency Converter. Available online: https://www.xe.com/currencyconverter/convert/?Amount=1&From=USD&To=PKR (accessed on 9 February 2023).
- Bertram, M.Y.; Lauer, J.A.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.-P.; Hill, S.R. Cost–effectiveness thresholds: Pros and cons. Bull. World Health Organ. 2016, 94, 925. [Google Scholar] [CrossRef]
- Ivinson, A.J. Macroeconomics and health: Investing in health for economic development. Nat. Med. 2002, 8, 551–552. [Google Scholar] [CrossRef]
- Statista. Pakistan: Gross Domestic Product (GDP) per Capita in Current Prices from 1986 to 2022. Available online: https://www.statista.com/statistics/383750/gross-domestic-product-gdp-per-capita-in-pakistan/#:~:text=The%20gross%20domestic%20product%20per,1%2C658.36%20U.S.%20dollars%20in%202022 (accessed on 14 February 2023).
- Criss, S.D.; Cao, P.; Bastani, M.; Ten Haaf, K.; Chen, Y.; Sheehan, D.F.; Blom, E.F.; Toumazis, I.; Jeon, J.; de Koning, H.J. Cost-effectiveness analysis of lung cancer screening in the United States: A comparative modeling study. Ann. Intern. Med. 2019, 171, 796–804. [Google Scholar] [CrossRef]
- Briggs, A.; Sculpher, M.; Buxton, M. Uncertainty in the economic evaluation of health care technologies: The role of sensitivity analysis. Health Econ. 1994, 3, 95–104. [Google Scholar] [CrossRef]
- Vreman, R.A.; Geenen, J.W.; Knies, S.; Mantel-Teeuwisse, A.K.; Leufkens, H.G.; Goettsch, W.G. The application and implications of novel deterministic sensitivity analysis methods. Pharmacoeconomics 2021, 39, 1–17. [Google Scholar] [CrossRef]
- Baio, G.; Dawid, A.P. Probabilistic sensitivity analysis in health economics. Stat. Methods Med. Res. 2015, 24, 615–634. [Google Scholar] [CrossRef]
- Hatswell, A.J.; Bullement, A.; Briggs, A.; Paulden, M.; Stevenson, M.D. Probabilistic sensitivity analysis in cost-effectiveness models: Determining model convergence in cohort models. Pharmacoeconomics 2018, 36, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Shahi, A.; Shrestha, S.; Bardi, K.C.; Acharya, K.; Pradhan, S.K. Potential roles of pharmacists in HIV/AIDS care delivery in Nepal: A qualitative study. PLoS ONE 2023, 18, e0280160. [Google Scholar] [CrossRef] [PubMed]
- Tarfa, A.; Pecanac, K.; Shiyanbola, O.O. A qualitative inquiry into the patient-related barriers to linkage and retention in HIV care within the community setting. Explor. Res. Clin. Soc. Pharm. 2023, 9, 100207. [Google Scholar] [CrossRef] [PubMed]
- Barnes, E.; Zhao, J.; Giumenta, A.; Johnson, M. The effect of an integrated health system specialty pharmacy on HIV antiretroviral therapy adherence, viral suppression, and CD4 count in an outpatient infectious disease clinic. J. Manag. Care Spec. Pharm. 2020, 26, 95–102. [Google Scholar] [CrossRef]
- Kelly, D.V.; Kielly, J.; Hughes, C.; Gahagan, J.; Asghari, S.; Hancock, S.; Burt, K.; Smyczek, P.; Charlton, C.; Nguyen, H. Expanding access to HIV testing through Canadian community pharmacies: Findings from the APPROACH study. BMC Public Health 2020, 20, 639. [Google Scholar] [CrossRef]
- Asieba, I.O.; Oqua, D.A.; Wutoh, A.A.; Agu, K.A.; Omeh, O.I.; Adeyanju, Z.A.; Adesina, A.; Agu, F.; Agada, P.; Achanya, A. Antiretroviral therapy in community pharmacies-Implementation and outcomes of a differentiated drug delivery model in Nigeria. Res. Soc. Adm. Pharm. 2021, 17, 842–849. [Google Scholar] [CrossRef]
- Crawford, N.D.; Lewis, C.F.; Moore, R.; Pietradoni, G.; Weidle, P. Examining the multilevel barriers to pharmacy-based HIV prevention and treatment services. Sex. Transm. Dis. 2022, 49, S22–S25. [Google Scholar] [CrossRef]
- Shrestha, R.K.; Schommer, J.C.; Taitel, M.S.; Garza, O.W.; Camp, N.M.; Akinbosoye, O.E.; Clay, P.G.; Byrd, K.K. Costs and Cost-Effectiveness of the Patient-Centered HIV Care Model: A Collaboration Between Community-Based Pharmacists and Primary Medical Providers. J. Acquir. Immune Defic. Syndr. 2020, 85, e48–e54. [Google Scholar] [CrossRef]
- Ahmed, A.; Saqlain, M.; Tanveer, M.; Blebil, A.Q.; Dujaili, J.A.; Hasan, S.S. The impact of clinical pharmacist services on patient health outcomes in Pakistan: A systematic review. BMC Health Serv. Res. 2021, 21, 859. [Google Scholar] [CrossRef]
- Ahmed, A.; Tanveer, M.; Siddiqui, A.; Khan, G.M. Bridging the gap for clinical pharmacist in developing countries like Pakistan. J. Coll. Phys. Surg. Pak. 2018, 28, 229–232. [Google Scholar] [CrossRef]
- Hasan, S.S.; Mustafa, Z.U.; Kow, C.S.; Merchant, H.A. “Sehat Sahulat Program”: A Leap into the Universal Health Coverage in Pakistan. Int. J. Environ. Res. Public Health 2022, 19, 6998. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Distribution | Base Case | Plausible Range | Sources |
|---|---|---|---|---|
| Transition Probabilities | Beta | Trial data | Trial data | Chatha et al. [33] Simmons et al. [38] NACP et al. [3] |
| Utilities | ||||
| Asymptomatic (>500 CD-4) | Beta | 0.83 | 0.67–0.99 | Ahmed et al. [6] |
| Symptomatic (200–500 CD-4) | Beta | 0.34 | 0.27–0.40 | Ahmed et al. [6] |
| AIDS Converted (<200 CD-4) | Beta | 0.03 | 0.024–0.036 | Ahmed et al. [6] |
| Cost (2023 USD) | ||||
| Intervention cost | Gamma | 290 | 232–348 | Assumptions |
| Stage A, Asymptomatic | Gamma | 22 | 17.6–26.4 | NACP et al. [3] |
| Stage B, Symptomatic | Gamma | 104 | 83.2–124.8 | NACP et al. [3] |
| Stage C, AIDS converted | Gamma | 134 | 107.2–160.8 | NACP et al. [3] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, A.; Dujaili, J.A.; Chuah, L.H.; Hashmi, F.K.; Le, L.K.D.; Chatha, Z.F.; Khanal, S.; Awaisu, A.; Chaiyakunapruk, N. Cost–Effectiveness Analysis of Pharmacist Adherence Interventions in People Living with HIV/AIDS in Pakistan. Healthcare 2023, 11, 2453. https://doi.org/10.3390/healthcare11172453
Ahmed A, Dujaili JA, Chuah LH, Hashmi FK, Le LKD, Chatha ZF, Khanal S, Awaisu A, Chaiyakunapruk N. Cost–Effectiveness Analysis of Pharmacist Adherence Interventions in People Living with HIV/AIDS in Pakistan. Healthcare. 2023; 11(17):2453. https://doi.org/10.3390/healthcare11172453
Chicago/Turabian StyleAhmed, Ali, Juman Abdulelah Dujaili, Lay Hong Chuah, Furqan Khurshid Hashmi, Long Khanh Dao Le, Zeenat Fatima Chatha, Saval Khanal, Ahmed Awaisu, and Nathorn Chaiyakunapruk. 2023. "Cost–Effectiveness Analysis of Pharmacist Adherence Interventions in People Living with HIV/AIDS in Pakistan" Healthcare 11, no. 17: 2453. https://doi.org/10.3390/healthcare11172453
APA StyleAhmed, A., Dujaili, J. A., Chuah, L. H., Hashmi, F. K., Le, L. K. D., Chatha, Z. F., Khanal, S., Awaisu, A., & Chaiyakunapruk, N. (2023). Cost–Effectiveness Analysis of Pharmacist Adherence Interventions in People Living with HIV/AIDS in Pakistan. Healthcare, 11(17), 2453. https://doi.org/10.3390/healthcare11172453