
Feedback for Emergency Ambulance Staff: A National Review of Current Practice Informed by Realist Evaluation Methodology


Abstract
1. Introduction
- What are the types and design elements of interventions providing feedback for EMS professionals in the UK?
- What is it about EMS feedback interventions that works, for whom, in what circumstances, how and to what extent?
2. Materials and Methods
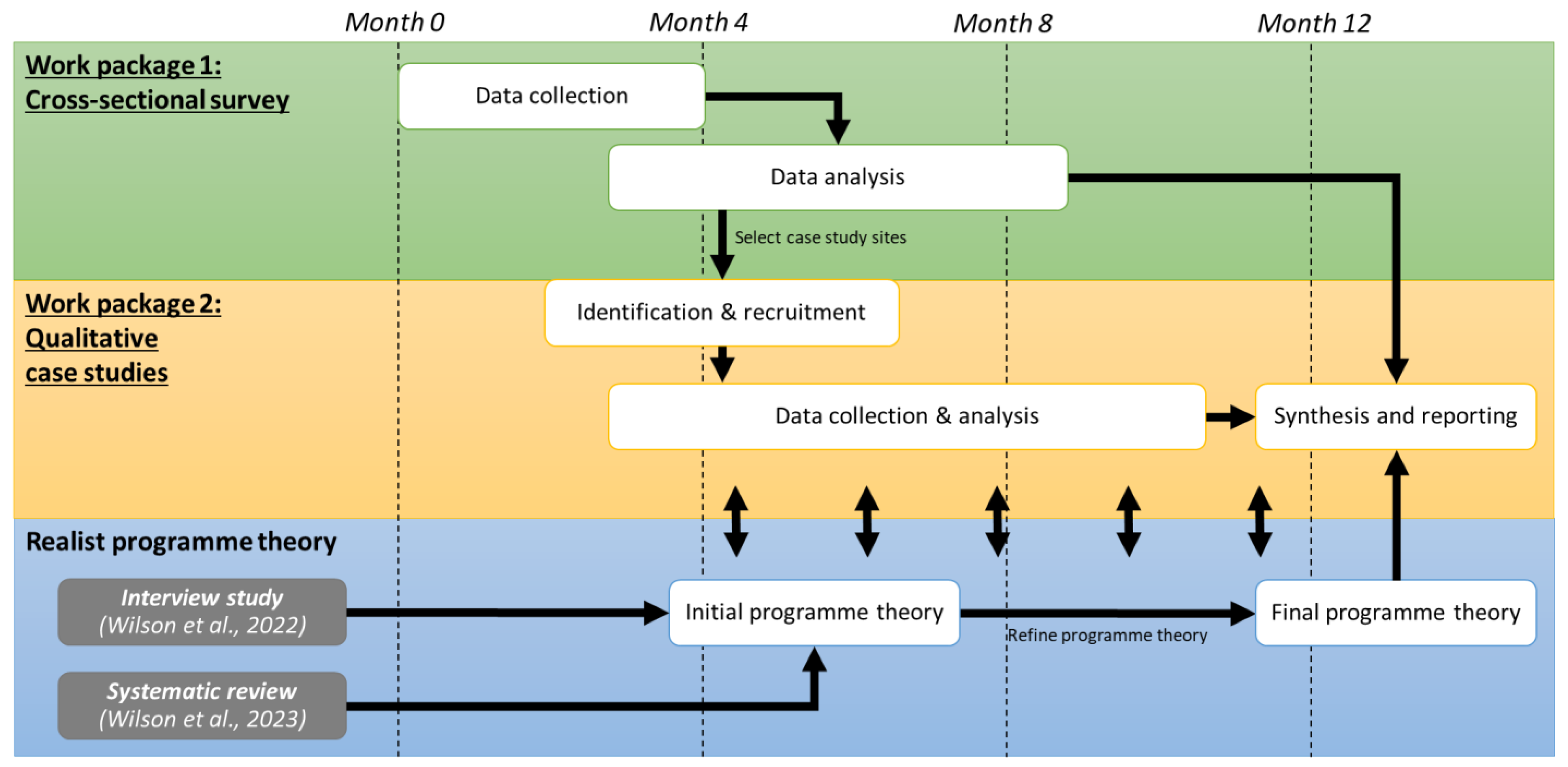
2.1. Study Design
2.2. Setting and Participants
2.3. Data Collection
2.4. Data Analysis
2.5. Development of Programme Theory
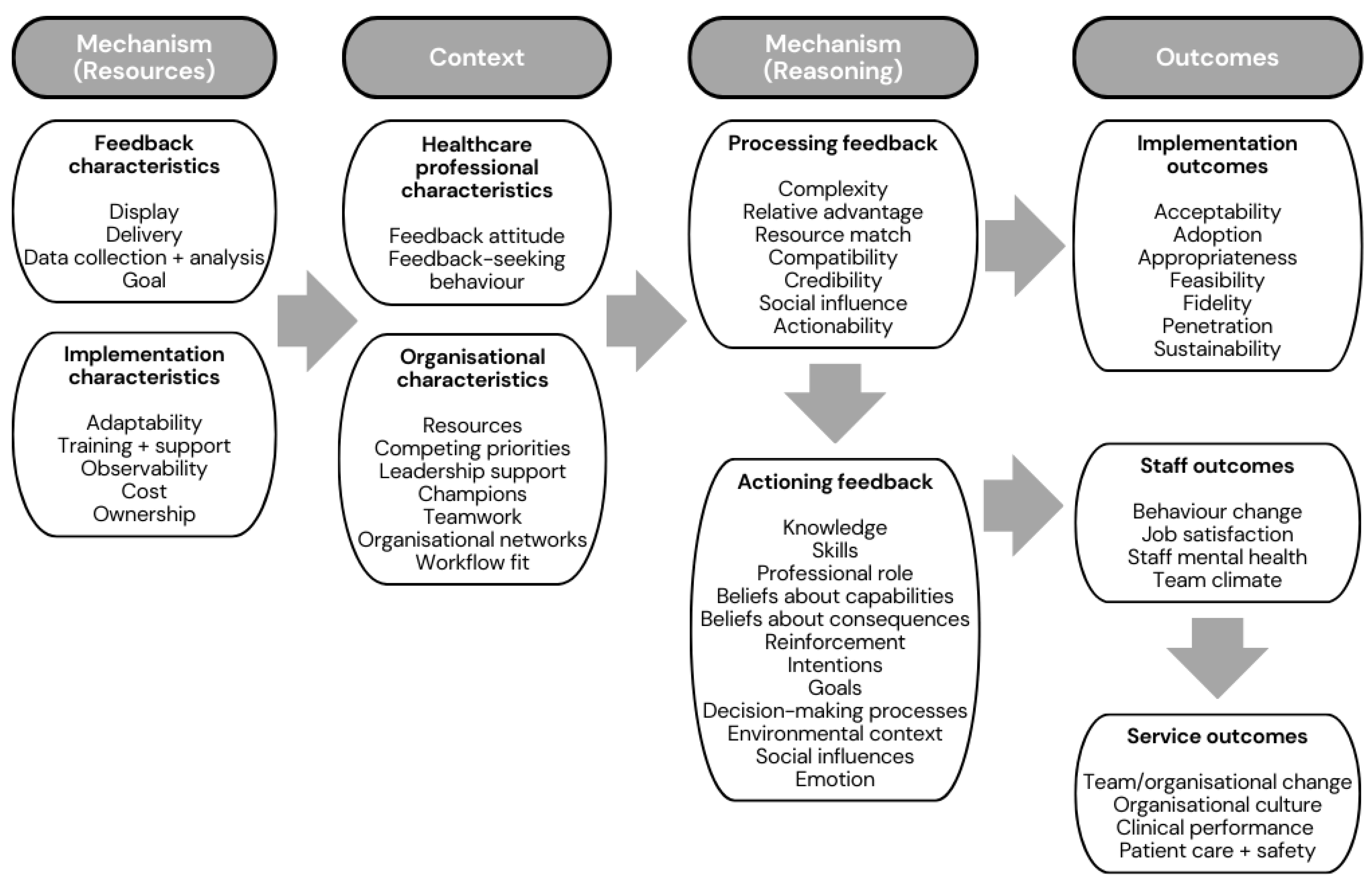
- Context: What are the barriers and facilitators to implementing feedback in EMS?
- Mechanism—Resources: What are the main characteristics of the type of feedback being provided?
- Mechanism—Reasoning: What are the psychological responses by which feedback achieves its effects?
- Outcome: What are the EMS feedback interventions’ perceived effects and impact?
3. Results
3.1. Characteristics of Survey Participants
3.2. Types and Design Elements of Interventions Providing Feedback for EMS Professionals
3.3. Characteristics of Case Study Sites
3.3.1. Case Study 1
3.3.2. Case Study 2
3.3.3. Case Study 3
3.3.4. Case Study 4
3.4. Programme Theory of Feedback within EMS
4. Discussion
4.1. Implications and Future Research
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CMOc | Context–Mechanism–Outcome Configuration |
| CP-FIT | Clinical Performance Feedback Intervention Theory |
| EMS | Emergency Medical Services |
| IQR | Interquartile Range |
| UK | United Kingdom |
| WP | Work Package |
References
- Ivers, N.M.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.D.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2012, 6, CD000259. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.; Janes, G.; Lawton, R.; Benn, J. Types and effects of feedback for emergency ambulance staff: A systematic mixed studies review and meta-analysis. BMJ Qual. Saf. 2023. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.D.; Freeman, K.; Clarke, A.; Spurgeon, P.; Smyth, M.; Perkins, G.D.; Sujan, M.A.; Cooke, M.W. Health services and delivery research. In Patient Safety in Ambulance Services: A Scoping Review; NIHR Journals Library: Southampton, UK, 2015. [Google Scholar]
- Lawn, S.; Roberts, L.; Willis, E.; Couzner, L.; Mohammadi, L.; Goble, E. The effects of emergency medical service work on the psychological, physical, and social well-being of ambulance personnel: A systematic review of qualitative research. BMC Psychiatry 2020, 20, 348. [Google Scholar] [CrossRef] [PubMed]
- Paulin, J.; Kurola, J.; Koivisto, M.; Iirola, T. Ems non-conveyance: A safe practice to decrease ed crowding or a threat to patient safety? BMC Emerg. Med. 2021, 21, 115. [Google Scholar] [CrossRef]
- Blodgett, J.M.; Robertson, D.J.; Pennington, E.; Ratcliffe, D.; Rockwood, K. Alternatives to direct emergency department conveyance of ambulance patients: A scoping review of the evidence. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 4. [Google Scholar] [CrossRef]
- Morrison, L.; Cassidy, L.; Welsford, M.; Chan, T.M. Clinical performance feedback to paramedics: What they receive and what they need. AEM Educ. Train. 2017, 1, 87–97. [Google Scholar] [CrossRef]
- Cash, R.E.; Crowe, R.P.; Rodriguez, S.A.; Panchal, A.R. Disparities in feedback provision to emergency medical services professionals. Prehospital Emerg. Care 2017, 21, 773–781. [Google Scholar] [CrossRef]
- Wilson, C.; Howell, A.-M.; Janes, G.; Benn, J. The role of feedback in emergency ambulance services: A qualitative interview study. BMC Health Serv. Res. 2022, 22, 296. [Google Scholar] [CrossRef]
- Cifra, C.L.; Sittig, D.F.; Singh, H. Bridging the feedback gap: A sociotechnical approach to informing clinicians of patients’ subsequent clinical course and outcomes. BMJ Qual. Saf. 2021, 30, 591–597. [Google Scholar] [CrossRef]
- Jamtvedt, G.; Young, J.M.; Kristoffersen, D.T.; O’Brien, M.A.; Oxman, A.D. Does telling people what they have been doing change what they do? A systematic review of the effects of audit and feedback. Qual. Saf. Health Care 2006, 15, 433–436. [Google Scholar] [CrossRef]
- Brehaut, J.C.; Colquhoun, H.L.; Eva, K.W.; Carroll, K.; Sales, A.; Michie, S.; Ivers, N.; Grimshaw, J.M. Practice feedback interventions: 15 suggestions for optimizing effectiveness. Ann. Intern. Med. 2016, 164, 435–441. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Michie, S.; Sales, A.; Ivers, N.; Grimshaw, J.M.; Carroll, K.; Chalifoux, M.; Eva, K.; Brehaut, J. Reporting and design elements of audit and feedback interventions: A secondary review. BMJ Qual. Saf. 2017, 26, 54–60. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Carroll, K.; Eva, K.W.; Grimshaw, J.M.; Ivers, N.; Michie, S.; Sales, A.; Brehaut, J.C. Advancing the literature on designing audit and feedback interventions: Identifying theory-informed hypotheses. Implement. Sci. 2017, 12, 117. [Google Scholar] [CrossRef]
- Rapin, J.; Pellet, J.; Mabire, C.; Gendron, S.; Dubois, C.-A. How does feedback shared with interprofessional health care teams shape nursing performance improvement systems? A rapid realist review protocol. Syst. Rev. 2019, 8, 182. [Google Scholar] [CrossRef]
- Brown, B.; Gude, W.T.; Blakeman, T.; van der Veer, S.N.; Ivers, N.; Francis, J.J.; Lorencatto, F.; Presseau, J.; Peek, N.; Daker-White, G. Clinical performance feedback intervention theory (cp-fit): A new theory for designing, implementing, and evaluating feedback in health care based on a systematic review and meta-synthesis of qualitative research. Implement. Sci. 2019, 14, 40. [Google Scholar] [CrossRef]
- Lyon, R.M.; Clarke, S.; Milligan, D.; Clegg, G.R. Resuscitation feedback and targeted education improves quality of pre-hospital resuscitation in scotland. Resuscitation 2012, 83, 70–75. [Google Scholar] [CrossRef]
- Sommers, N.; Evans, L.; Collingwood, T.; Dykes, L. PP29 ‘Breaking down Barriers: Experiences from the first year of an ED to EMS feedback ‘Postbox. Emerg. Med. J. 2019, 36, e13. [Google Scholar] [CrossRef]
- Snowsill, M.; Cracolici, G.; Wieder, T.; Allen, G. Facilitated hospital to pre-hospital feedback for professional development (phem feedback): A service evaluation using a self-reported questionnaire to understand the experiences of participating pre-hospital clinicians in the first year of operation. Br. Paramed. J. 2023, 8, 42–52. [Google Scholar] [CrossRef]
- Foy, R.; Skrypak, M.; Alderson, S.; Ivers, N.M.; McInerney, B.; Stoddart, J.; Ingham, J.; Keenan, D. Revitalising audit and feedback to improve patient care. BMJ 2020, 368, m213. [Google Scholar] [CrossRef]
- Davidoff, F. Understanding contexts: How explanatory theories can help. Implement. Sci. 2019, 14, 23. [Google Scholar] [CrossRef]
- Davidoff, F.; Dixon-Woods, M.; Leviton, L.; Michie, S. Demystifying theory and its use in improvement. BMJ Qual. Saf. 2015, 24, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Funnell, S.; Rogers, P. Purposeful Program Theory: Effective Use of Theories of Change and Logic Models; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar]
- Pawson, R.; Tilley, N. Realistic Evaluation; Sage: Los Angeles, CA, USA, 1997. [Google Scholar]
- Pawson, R.; Manzano-Santaella, A. A realist diagnostic workshop. Evaluation 2012, 18, 176–191. [Google Scholar] [CrossRef]
- NHS Health Research Authority. UK Policy Framework for Health and Social Care Research; NHS Health Research Authority: London, UK, 2017. [Google Scholar]
- Wong, G.; Westhorp, G.; Manzano, A.; Greenhalgh, J.; Jagosh, J.; Greenhalgh, T. Rameses ii reporting standards for realist evaluations. BMC Med. 2016, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Duc, N.T.M.; Thang, T.L.L.; Nam, N.H.; Ng, S.J.; Abbas, K.S.; Huy, N.T.; Marušić, A.; Paul, C.L.; Kwok, J.; et al. A consensus-based checklist for reporting of survey studies (cross). J. Gen. Intern. Med. 2021, 36, 3179–3187. [Google Scholar] [CrossRef]
- Manzano, A. The craft of interviewing in realist evaluation. Evaluation 2016, 22, 342–360. [Google Scholar] [CrossRef]
- Mukumbang, F.C.; Marchal, B.; Van Belle, S.; van Wyk, B. Using the realist interview approach to maintain theoretical awareness in realist studies. Qual. Res. 2019, 20, 485–515. [Google Scholar] [CrossRef]
- De Weger, E.; Van Vooren, N.J.E.; Wong, G.; Dalkin, S.; Marchal, B.; Drewes, H.W.; Baan, C.A. What’s in a realist configuration? Deciding which causal configurations to use, how, and why. Int. J. Qual. Methods 2020, 19, 1609406920938577. [Google Scholar] [CrossRef]
- De Brún, A.; McAuliffe, E. Identifying the context, mechanisms and outcomes underlying collective leadership in teams: Building a realist programme theory. BMC Health Serv. Res. 2020, 20, 261. [Google Scholar] [CrossRef]
- Greenhalgh, J.; Manzano, A. Understanding ‘context’ in realist evaluation and synthesis. Int. J. Soc. Res. Methodol. 2022, 25, 583–595. [Google Scholar] [CrossRef]
- Dalkin, S.; Greenhalgh, J.; Jones, D.; Cunningham, B.; Lhussier, M. What’s in a mechanism? Development of a key concept in realist evaluation. Implement. Sci. 2015, 10, 49. [Google Scholar] [CrossRef]
- Gilmore, B.; McAuliffe, E.; Power, J.; Vallières, F. Data analysis and synthesis within a realist evaluation: Toward more transparent methodological approaches. Int. J. Qual. Methods 2019, 18, 1609406919859754. [Google Scholar] [CrossRef]
- Jagosh, J. Retroductive theorizing in pawson and tilley’s applied scientific realism. J. Crit. Realism 2020, 19, 121–130. [Google Scholar] [CrossRef]
- Mukumbang, F.C.; Kabongo, E.M.; Eastwood, J.G. Examining the application of retroductive theorizing in realist-informed studies. Int. J. Qual. Methods 2021, 20, 16094069211053516. [Google Scholar] [CrossRef]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef]
- Carey, R.N.; Connell, L.E.; Johnston, M.; Rothman, A.J.; de Bruin, M.; Kelly, M.P.; Michie, S. Behavior change techniques and their mechanisms of action: A synthesis of links described in published intervention literature. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2019, 53, 693–707. [Google Scholar] [CrossRef]
- Porter, A.; Badshah, A.; Black, S.; Fitzpatrick, D.; Harris-Mayes, R.; Islam, S.; Jones, M.; Kingston, M.; LaFlamme-Williams, Y.; Mason, S.; et al. Electronic health records in ambulances: The era multiple-methods study. Health Serv. Deliv. Res. 2020, 8, 1–140. [Google Scholar] [CrossRef]
- Cuk, S.; Wimmer, H.; Powell, L.M. Problems associated with patient care reports and transferring data between ambulance and hospitals from the perspective of emergency medical technicians. Issues Inf. Syst. 2017, 18, 16–26. [Google Scholar]
- Eaton-Williams, P.; Mold, F.; Magnusson, C. Exploring paramedic perceptions of feedback using a phenomenological approach. Br. Paramed. J. 2020, 5, 7–14. [Google Scholar] [CrossRef]
- O’Hara, R.; Johnson, M.; Siriwardena, A.N.; Weyman, A.; Turner, J.; Shaw, D.; Mortimer, P.; Newman, C.; Hirst, E.; Storey, M.; et al. A qualitative study of systemic influences on paramedic decision making: Care transitions and patient safety. J. Health Serv. Res. Policy 2015, 20, 45–53. [Google Scholar] [CrossRef]
- NHS Improvement. Operational Productivity and Performance in English NHS Ambulance Trusts: Unwarranted Variations; NHS Improvement: London, UK, 2018. [Google Scholar]
- O’Cathain, A.; Knowles, E.; Bishop-Edwards, L.; Coster, J.; Crum, A.; Jacques, R.; James, C.; Lawson, R.; Marsh, C.; O’Hara, R.; et al. Understanding Variation in Ambulance Service Non-Conveyance Rates: A Mixed Methods Study; NIHR Journals Library: Southampton, UK, 2018. [Google Scholar]
- Ebben, R.H.A.; Vloet, L.C.M.; Speijers, R.F.; Tönjes, N.W.; Loef, J.; Pelgrim, T.; Hoogeveen, M.; Berben, S.A.A. A patient-safety and professional perspective on non-conveyance in ambulance care: A systematic review. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 71. [Google Scholar] [CrossRef]
- Weick, K.E. Theory construction as disciplined imagination. Acad. Manag. Rev. 1989, 14, 516–531. [Google Scholar] [CrossRef]
- Kislov, R.; Pope, C.; Martin, G.P.; Wilson, P.M. Harnessing the power of theorising in implementation science. Implement. Sci. 2019, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Ivers, N.M.; Sales, A.; Colquhoun, H.; Michie, S.; Foy, R.; Francis, J.J.; Grimshaw, J.M. No more ‘business as usual’ with audit and feedback interventions: Towards an agenda for a reinvigorated intervention. Implement. Sci. 2014, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Denisi, A.; Sockbeson, C.E.S. Feedback sought vs. feedback given: A tale of two literatures. Manag. Res. J. Iberoam. Acad. Manag. 2018, 16, 320–333. [Google Scholar] [CrossRef]
- Curran, G.M.; Landes, S.J.; McBain, S.A.; Pyne, J.M.; Smith, J.D.; Fernandez, M.E.; Chambers, D.A.; Mittman, B.S. Reflections on 10 years of effectiveness-implementation hybrid studies. Front. Health Serv. 2022, 2, 1053496. [Google Scholar] [CrossRef]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N | % | |
|---|---|---|---|
| Feedback type | Patient outcome feedback | 31 | 77.5 |
| Clinical performance feedback | 4 | 10.0 | |
| Clinical performance + patient outcome feedback | 5 | 12.5 | |
| Currently active | Yes | 28 | 70.0 |
| No | 12 | 30.0 | |
| Year started Median 2019 (IQR 2017–2020) | 2004–2013 | 2 | 5.0 |
| 2014–2018 | 13 | 32.5 | |
| 2019–2022 | 23 | 57.5 | |
| No response | 2 | 5.0 | |
| Instances of feedback | <10 | 1 | 2.5 |
| 10–49 | 14 | 35.0 | |
| 50–99 | 11 | 27.5 | |
| 100–199 | 4 | 10.0 | |
| 200–299 | 2 | 5.0 | |
| 300–399 | 2 | 5.0 | |
| 400–499 | 1 | 2.5 | |
| >500 | 2 | 5.0 | |
| No response | 3 | 7.5 | |
| Feedback recipient (categories are not mutually exclusive) | Frontline EMS staff | 36 | 90.0 |
| Helicopter EMS staff | 14 | 35.0 | |
| EMS managers | 9 | 22.5 | |
| Emergency operations centre staff | 2 | 5.0 | |
| EMS organisation | 3 | 7.5 | |
| Combination | 16 | 40.0 | |
| Format | Email or electronic document | 35 | 87.5 |
| Face-to-face | 3 | 7.5 | |
| Written letter | 1 | 2.5 | |
| No response | 1 | 2.5 | |
| Frequency | Daily | 2 | 5.0 |
| Weekly | 3 | 7.5 | |
| Bi-weekly | 1 | 2.5 | |
| Monthly | 3 | 7.5 | |
| Quarterly | 1 | 2.5 | |
| Ad hoc | 29 | 72.5 | |
| No response | 1 | 2.5 | |
| Lag time Median 21 days (IQR 7–30 days) | Within 24 h | 3 | 7.5 |
| Within 7 days | 8 | 20.0 | |
| 1–2 weeks | 6 | 15.0 | |
| 2–4 weeks | 14 | 35.0 | |
| 4–12 weeks | 6 | 15.0 | |
| >12 weeks | 2 | 5.0 | |
| No response | 1 | 2.5 | |
| Recipient level | Individual | 32 | 80.0 |
| Individual + team | 3 | 7.5 | |
| Individual + organisation | 1 | 2.5 | |
| Individual + team + organisation | 4 | 10.0 | |
| Patient cases | Individual | 38 | 95.0 |
| Aggregate | 2 | 5.0 | |
| Push or pull | Push | 8 | 20.0 |
| Pull | 25 | 62.5 | |
| Combination | 6 | 15.0 | |
| No response | 1 | 2.5 | |
| Stand-alone | Stand-alone | 34 | 85.0 |
| Part of an organisational or education initiative | 6 | 15.0 | |
| Action plan included | Yes | 12 | 30.0 |
| No | 28 | 70.0 | |
| Underlying theory | Yes | 15 | 37.5 |
| No | 24 | 60.0 | |
| No response | 1 | 2.5 | |
| Aim (categories are not mutually exclusive) | Aid reflection, education + learning | 21 | 52.5 |
| Provide feedback (“close the loop”) | 19 | 47.5 | |
| Improve staff wellbeing + job satisfaction | 9 | 22.5 | |
| Improve patient care | 6 | 15.0 | |
| Improve relationships between EMS + hospital staff | 6 | 15.0 | |
| Increase protocol adherence | 4 | 10.0 | |
| Satisfy EMS staff’s curiosity | 3 | 7.5 | |
| Clinical governance | 2 | 5.0 | |
| Barriers (categories are not mutually exclusive) | Information governance | 18 | 45.0 |
| Time and resources required to generate the feedback | 16 | 40.0 | |
| Technology | 7 | 17.5 | |
| No barriers | 4 | 10.0 | |
| EMS managers | 4 | 10.0 | |
| Lack of awareness from EMS staff that the initiative existed | 3 | 7.5 | |
| Identifying hospital collaborators and securing buy-in from hospital staff | 2 | 5.0 | |
| Concerns from EMS staff that errors identified in clinical practice would be used against them | 2 | 5.0 | |
| Facilitators (categories are not mutually exclusive) | Collaboration | 14 | 35.0 |
| Enthusiasm from EMS staff | 9 | 22.5 | |
| Engagement from hospital staff | 8 | 20.0 | |
| Initiative lead with time + enthusiasm | 2 | 5.0 | |
| Alignment with organisational priorities | 2 | 5.0 | |
| No existing initiative providing feedback | 1 | 2.5 | |
| Information governance | 1 | 2.5 | |
| Conducting a pilot of the initiative first | 1 | 2.5 | |
| Inclusion of specific expertise within the team (e.g., data analyst) | 1 | 2.5 | |
| Characteristics | Case Study 1 | Case Study 2 | Case Study 3 | Case Study 4 |
|---|---|---|---|---|
| Data sources | Initiative lead interview (n = 1), Feedback recipient interviews (n = 3), documents (n = 2) | Initiative lead interviews (n = 2), Feedback recipient interview (n = 1), documents (n = 1) | Initiative lead interviews (n = 2), Feedback recipient interviews (n = 3), documents (n = 3) | Initiative lead interview (n = 1), Feedback recipient interviews (n = 4) |
| Context | Rural | Urban | Rural | Rural, urban + suburban |
| Catchment area | 1 hospital | Regional | 2 hospitals | National |
| Initiative lead | EMS manager | Regional network clinician + EMS specialist clinician | EMS specialist clinician + EMS manager | EMS specialist clinician |
| Patient group | All patients | 1 condition | All patients | 1 condition |
| Feedback type | Patient outcome | Clinical performance | Patient outcome | Clinical performance + patient outcome feedback |
| Push or pull | Pull | Push | Pull | Push |
| Year started | 2018 | 2015 | 2014 | 2020 |
| Instances of feedback | 50–99 | Unknown | >500 | 10–49 |
| Feedback recipient | Frontline EMS staff | Frontline EMS staff | Frontline EMS staff | Frontline + helicopter EMS staff |
| Format | Face-to-face | Electronic dashboard | ||
| Frequency | Whenever requested | When breach occurred | Weekly | After every event |
| Lag-time | 2–4 weeks | A few weeks | Up to 7 days | 1–6 months |
| Mechanism (Resources) | Context | Outcomes | Mechanism (Reasoning) | Data Sources | ||||
|---|---|---|---|---|---|---|---|---|
| If | an initiative is co-designed | with | feedback recipients that have a positive feedback attitude and leadership support | then | acceptability is likely to be higher ↑ | because | there is a sense of ownership, understanding and credibility | CS1-P1, CS1-P3 |
| If | a senior clinician provides push feedback on protocol adherence | within | an organisation that has leadership support | then | it is likely to be accepted ↑ | because | there is a sense of credibility | CS2-P1, CS2-P2, CS4-P2, CS4-P3 |
| If | an initiative provides patient outcome feedback via a ‘pull’ initiative | to | healthcare professionals that display feedback-seeking behaviour | then | adoption and appropriateness are likely to be higher ↑ | because | there is a sense of compatibility | CS1-P2, CS1-P3, CS1-P4, CS3-P2, CS3-P3 |
| If | a feedback initiative provides patient outcome feedback | within | an organisation where informal follow-up opportunities are limited | then | adoption is likely to be higher ↑ | because | there is a relative advantage | CS1-P1, CS1-P1, CS3-P2, CS3-P3 |
| If | the initiative lead guides feedback providers on paramedics’ scope of practice | when | feedback providers do not have any experience or knowledge of EMS clinical practice | then | feedback is more likely to be appropriate ↑ | because | it is actionable | CS1-P1, CS4-P1 |
| If | feedback is meant to be generated with limited training | within | organisations that can appoint champions to generate feedback | then | it is more likely to be feasible ↑ | because | there is a resource match | CS1-P1, CS2-P1 |
| If | the number of processed feedback requests is limited by having specific eligibility criteria | within | an organisation that has limited resources ring-fenced for this initiative | then | sustainability would be better ↑ | because | there would be a better resource match | CS1-P1, CS4-P1 |
| If | patient outcome feedback does not identify which patient it relates to | within | an organisation where staff attend multiple patients per shift and feedback is delayed | then | acceptability and adoption are likely to be poor ↓ | because | it would be complex for recipients to identify whom the feedback related to | CS1-P4 CS3-P5, CS4-P1, CS4-P2 |
| If | feedback is pushed out without training, support or raising awareness | within | an organisation that traditionally has poor feedback culture | then | acceptability is likely to be poor ↓ | because | there is poor compatibility | CS2-P3, CS4-P2, CS4-P3, CS4-P4 |
| If | feedback is provided with a long lag-time | to | a staff member that can informally follow up on patients | then | adoption is likely to be poor ↓ | because | there is no relative advantage | CS4-P1, CS4-P2, CS4-P3, CS4-P4 |
| If | an ambulance trust leads a feedback initiative | without | clearly articulating how the feedback is going to be used by the trust | then | adoption may be low ↓ | because | it could be perceived as being punitive | CS1-P2, CS1-P4, CS4-P2, CS4-P4 |
| If | a feedback initiative has a high resource cost for one individual | within | an organisation where there are competing priorities | then | it is not likely to be sustainable ↓ | because | there is no resource match | CS1-P1, CS1-D2, CS4-P1 |
| Mechanism (Resources) | Context | Outcomes | Mechanism (Reasoning) | Data Sources | ||||
|---|---|---|---|---|---|---|---|---|
| If | patient outcome feedback allows comparisons between prehospital working impression and hospital diagnosis | in | an organisation that monitors this on an aggregate level | then | it is likely to improve patient safety ↑ | because | Knowledge is improved by organisations arranging additional training; the environment is changed by organisations increasing alternative pathways | CS3-D1, CS3-D2, CS3-D3, CS3-P3, CS4-P1 |
| If | patient outcome feedback is provided | to | ambulance staff interacting with patients who are anxious about what might happen at the hospital | then | it is likely to improve service quality ↑ | because | staff have a belief about consequences and can reassure patients | CS1-P2, CS3-P3 |
| If | patient outcome feedback is provided regarding patients with a difference in prehospital/hospital diagnosis, patients frequently calling the ambulance service or patients with common conditions | to | healthcare professionals that have a positive feedback attitude and within an organisation that supports autonomous decisions by staff | then | it is likely to lead to individual behaviour change and better patient care ↑ | because | it improves beliefs about consequences | CS1-P1, CS1-D1, CS3-P3, CS3-P5, CS4-P2, CS4-P5 |
| If | additional learning materials are provided alongside patient outcome feedback | to | healthcare professionals that have a positive feedback attitude | then | it is likely to lead to individual behaviour change and better patient care ↑ | because | it improves knowledge | CS4-P2, CS1-P1, CS3-P5 |
| If | an initiative provides patient outcome feedback via a ‘pull’ initiative | to | healthcare professionals that display feedback-seeking behaviour | then | it may lead to behaviour change and improved clinical performance/patient safety ↑ | because | it improves knowledge and decision-making processes | CS1-P1, CS1-P2, CS1-P3, CS3-P2 |
| If | patient outcome feedback is provided on patients whom staff have a particular interest in | to | staff who do not routinely find out what happens to their patients | then | it is likely to improve staff mental health ↑ | because | it allows an element of closure | CS1-P1, CS1-P2, CS1-P4, CS1-D1, CS3-D2 |
| If | a senior clinician sets up an initiative providing patient outcome feedback | within | an organisation that has traditionally viewed patient outcome information as an ‘add on’ | then | it is likely to lead to increased job satisfaction ↑ | because | it makes staff feel appreciated | CS3-P3, CS3-P4, CS4-P2, CS4-P3, CS4-P4, CS4-P5 |
| If | patient outcome feedback is provided only by emergency department staff | but | patients are admitted to hospital wards | then | staff behaviour change may be limited ↓ | because | there is only a partial understanding of the consequences | CS1-P1, CS1-P3, CS3-P5 |
| Mechanism (Resources) | Context | Outcomes | Mechanism (Reasoning) | Data Sources | ||||
|---|---|---|---|---|---|---|---|---|
| If | pathway adherence feedback is provided | within | an organisation that has a centralised model of care (i.e., bypassing local hospitals to attend specialist treatment centres) | then | it will lead to behaviour change and improved patient safety ↑ | because | staff will have had the pathway reinforced | CS2-P1, CS2-P2, CS4-P2, CS4-P5 |
| If | push-feedback on protocol adherence is provided | to | a healthcare professional that has a positive feedback attitude | then | it is likely to lead to behaviour change ↑ | because | it improves knowledge | CS2-P1, CS2-P2, CS3-P2, CS3-P3, CS4-P2, CS4-P4 |
| If | feedback on protocol adherence is provided | within | an organisation that prioritises the protocol topic | then | it is likely to improve clinical performance ↑ | because | it improves knowledge and skills | CS2-P1, CS2-P2, CS4-P1 |
| If | push-feedback is provided | to | a healthcare professional that has a low sense of confidence | then | it may negatively affect staff mental health ↓ | because | it reduces beliefs about capabilities | CS1-P3, CS2-P1, CS4-P2, CS4-P4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, C.; Janes, G.; Lawton, R.; Benn, J. Feedback for Emergency Ambulance Staff: A National Review of Current Practice Informed by Realist Evaluation Methodology. Healthcare 2023, 11, 2229. https://doi.org/10.3390/healthcare11162229
Wilson C, Janes G, Lawton R, Benn J. Feedback for Emergency Ambulance Staff: A National Review of Current Practice Informed by Realist Evaluation Methodology. Healthcare. 2023; 11(16):2229. https://doi.org/10.3390/healthcare11162229
Chicago/Turabian StyleWilson, Caitlin, Gillian Janes, Rebecca Lawton, and Jonathan Benn. 2023. "Feedback for Emergency Ambulance Staff: A National Review of Current Practice Informed by Realist Evaluation Methodology" Healthcare 11, no. 16: 2229. https://doi.org/10.3390/healthcare11162229
APA StyleWilson, C., Janes, G., Lawton, R., & Benn, J. (2023). Feedback for Emergency Ambulance Staff: A National Review of Current Practice Informed by Realist Evaluation Methodology. Healthcare, 11(16), 2229. https://doi.org/10.3390/healthcare11162229