
Effects of Music on the Quality of Life of Family Caregivers of Terminal Cancer Patients: A Randomised Controlled Trial


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
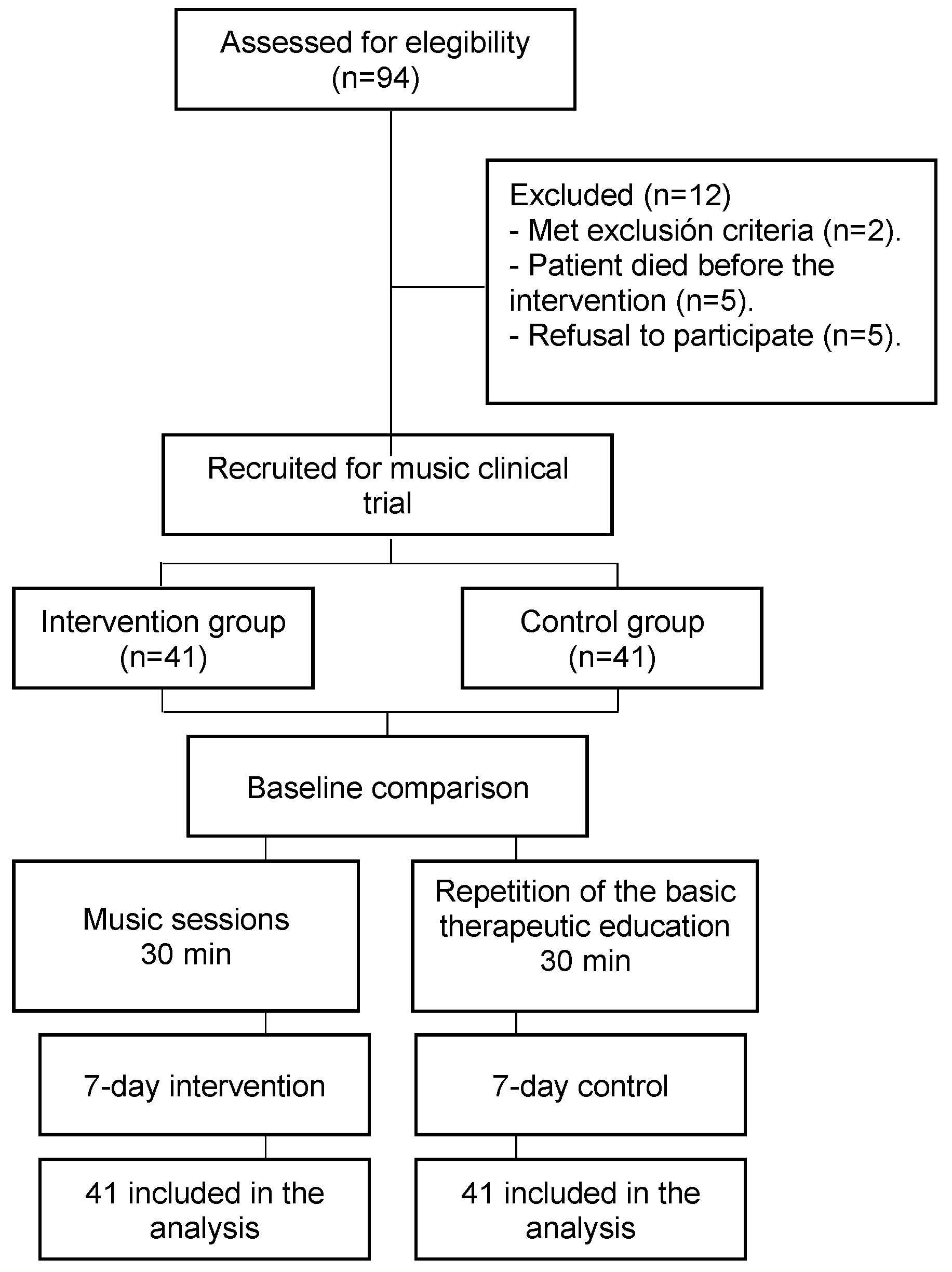
2.1. Design
2.2. Participants
2.3. Research Ethics
2.4. Measures
- -
- The Quality of Life Family Version (QOL-FV) 14, validated in Spanish [33], which measures the quality of life of family caregivers for patients with cancer, consists of thirty-seven items, scored on a scale ranging from 0 = worst result to 10 = best result (although several are coded by means of an inverse score). The instrument has four sub-scales or domains: physical well-being, psychological well-being, social concerns, and spiritual well-being;
- -
- The European Quality of Life—5 dimensions (EuroQol-5D-5L) questionnaire was developed in the United Kingdom and in Spain [34]. The questionnaire score is obtained using a visual analogue scale, ranging from 0 to 100, representing “worst imaginable state of health” to “best imaginable state of health”, respectively.
2.5. Sample Size and Randomisation
2.6. Intervention, Control Group, and Masking
2.7. Data Collection and Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| B | Standard Error | β | p-Value | |
|---|---|---|---|---|
| VAS of the EuroQol-5D-5L | −0.082 | 0.020 | −0.401 | 0.001 |
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 10 February 2022).
- Kaasa, S.; Loge, J.H.; Aapro, M.; Albreht, T.; Anderson, R.; Bruera, E.; Brunelli, C.; Caraceni, A.; Cervantes, A.; Currow, D.C.; et al. Integration of oncology and palliative care: A Lancet Oncology Commission. Lancet Oncol. 2018, 19, e588–e653. [Google Scholar] [CrossRef] [PubMed]
- Shepperd, S.; Gonçalves-Bradley, D.C.; Straus, S.E.; Wee, B. Hospital at home: Home-based end-of-life care. Cochrane Database Syst. Rev. 2021, 2021, CD009231. [Google Scholar] [CrossRef]
- Woodman, C.; Baillie, J.; Sivell, S. The preferences and perspectives of family caregivers towards place of care for their relatives at the end-of-life. A systematic review and thematic synthesis of the qualitative evidence. BMJ Support. Palliat. Care 2016, 6, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Kelly, E.P.; Meara, A.; Hyer, M.; Payne, N.; Pawlik, T.M. Understanding the Type of Support Offered Within the Caregiver, Family, and Spiritual/Religious Contexts of Cancer Patients. J. Pain Symptom Manag. 2019, 58, 56–64. [Google Scholar] [CrossRef]
- Alvariza, A.; Häger-Tibell, L.; Holm, M.; Steineck, G.; Kreicbergs, U. Increasing preparedness for caregiving and death in family caregivers of patients with severe illness who are cared for at home—Study protocol for a web-based intervention. BMC Palliat. Care 2020, 19, 33–38. [Google Scholar] [CrossRef]
- Perpiñá-Galvañ, J.; Orts-Beneito, N.; Fernández-Alcántara, M.; García-Sanjuán, S.; García-Caro, M.P.; Cabañero-Martínez, M.J. Level of Burden and Health-Related Quality of Life in Caregivers of Palliative Care Patients. Int. J. Environ. Res. Public Health 2019, 16, 4806. [Google Scholar] [CrossRef]
- Lv, X.-Q.; Liu, J.-J.; Feng, Y.; Li, S.-W.; Qiu, H.; Hong, J.-F. Predictive model of psychological distress in family caregivers of patients with cancer: A cross-sectional study. Support. Care Cancer 2021, 29, 5091–5101. [Google Scholar] [CrossRef]
- El-Jawahri, A.; Greer, J.A.; Park, E.R.; Jackson, V.A.; Kamdar, M.; Rinaldi, S.P.; Gallagher, E.R.; Jagielo, A.D.; Topping, C.E.; Elyze, M.; et al. Psychological Distress in Bereaved Caregivers of Patients With Advanced Cancer. J. Pain Symptom Manag. 2021, 61, 488–494. [Google Scholar] [CrossRef]
- Govina, O.; Vlachou, E.; Kalemikerakis, I.; Papageorgiou, D.; Kavga, A.; Konstantinidis, T. Factors Associated with Anxiety and Depression among Family Caregivers of Patients Undergoing Palliative Radiotherapy. Asia-Pac. J. Oncol. Nurs. 2019, 6, 283–291. [Google Scholar] [CrossRef]
- Valero-Cantero, I.; Wärnberg, J.; Carrión-Velasco, Y.; Martínez-Valero, F.J.; Casals, C.; Vázquez-Sánchez, M. Predictors of sleep disturbances in caregivers of patients with advanced cancer receiving home palliative care: A descriptive cross-sectional study. Eur. J. Oncol. Nurs. 2021, 51, 101907. [Google Scholar] [CrossRef]
- Oechsle, K.; Ullrich, A.; Marx, G.; Benze, G.; Wowretzko, F.; Zhang, Y.; Dickel, L.-M.; Heine, J.; Wendt, K.N.; Nauck, F.; et al. Prevalence and Predictors of Distress, Anxiety, Depression, and Quality of Life in Bereaved Family Caregivers of Patients With Advanced Cancer. Am. J. Hosp. Palliat. Med. 2019, 37, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Norinder, M.; Årestedt, K.; Lind, S.; Axelsson, L.; Grande, G.; Ewing, G.; Holm, M.; Öhlén, J.; Benkel, I.; Alvariza, A. Higher levels of unmet support needs in spouses are associated with poorer quality of life—A descriptive cross-sectional study in the context of palliative home care. BMC Palliat. Care 2021, 20, 132. [Google Scholar] [CrossRef] [PubMed]
- Ferrell, B.R.; Wisdom, C.; Wenzl, C. Quality of life as an outcome variable in the management of cancer pain. Cancer 1989, 63, 2321–2327. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.-Y.; Molassiotis, A.; Lloyd-Williams, M.; Yorke, J. Burden, emotional distress and quality of life among informal caregivers of lung cancer patients: An exploratory study. Eur. J. Cancer Care 2018, 27, e12691. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Health Services, Quality of Care. Quality Health Services and Palliative Care: Practical Approaches and Resources to Support Policy, Strategy and Practice; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-003516-4. Available online: https://www.who.int/publications/i/item/9789240035164 (accessed on 10 February 2022).
- Sun, V.; Raz, D.J.; Kim, J.Y. Caring for the informal cancer caregiver. Curr. Opin. Support. Palliat. Care 2019, 13, 238–242. [Google Scholar] [CrossRef]
- Litzelman, K.; Kent, E.E.; Mollica, M.; Rowland, J.H. How Does Caregiver Well-Being Relate to Perceived Quality of Care in Patients With Cancer? Exploring Associations and Pathways. J. Clin. Oncol. 2016, 34, 3554–3561. [Google Scholar] [CrossRef]
- Treanor, C.J. Psychosocial support interventions for cancer caregivers: Reducing caregiver burden. Curr. Opin. Support. Palliat. Care 2020, 14, 247–262. [Google Scholar] [CrossRef] [PubMed]
- Dileo, C. A classification model for music and medicine. In Applications of Music in Medicine; National Association of Music Therapy: Washington, DC, USA, 1999; pp. 1–6. [Google Scholar]
- National Center for Complementary and Integrative Health (NCCIH). Complementary, Alternative, or Integrative Health: What’s in A Name? 2021. Available online: http://nccam.nih.gov/health/whatiscam (accessed on 10 February 2022).
- Koelsch, S. A coordinate-based meta-analysis of music-evoked emotions. Neuroimage 2020, 223, 117350. [Google Scholar] [CrossRef] [PubMed]
- Koelsch, S. Brain correlates of music-evoked emotions. Nat. Rev. Neurosci. 2014, 15, 170–180. [Google Scholar] [CrossRef]
- Chen, S.-C.; Yeh, M.-L.; Chang, H.-J.; Lin, M.-F. Music, heart rate variability, and symptom clusters: A comparative study. Support. Care Cancer 2019, 28, 351–360. [Google Scholar] [CrossRef]
- Pedersen, M.; Dam, C.; Rafaelsen, S. Music and pain during endorectal ultrasonography examination: A prospective questionnaire study and literature review. Radiography 2020, 26, e164–e169. [Google Scholar] [CrossRef] [PubMed]
- Wren, A.A.; Shelby, R.A.; Soo, M.S.; Huysmans, Z.; Jarosz, J.A.; Keefe, F.J. Preliminary efficacy of a lovingkindness meditation intervention for patients undergoing biopsy and breast cancer surgery: A randomized controlled pilot study. Support. Care Cancer 2019, 27, 3583–3592. [Google Scholar] [CrossRef]
- Bradt, J.; Dileo, C.; Myers-Coffman, K.; Biondo, J. Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst. Rev. 2021, 2022, CD006911. [Google Scholar] [CrossRef]
- Choi, Y.K. The effect of music and progressive muscle relaxation on anxiety, fatigue, and quality of life in family caregivers of hospice patients. J. Music. Ther. 2010, 47, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.-L.; Li, Y.-M.; Lee, L.-H. Effects of music intervention with nursing presence and recorded music on psycho-physiological indices of cancer patient caregivers. J. Clin. Nurs. 2011, 21, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Dingley, C.; Ruckdeschel, A.; Kotula, K.; Lekhak, N. Implementation and outcomes of complementary therapies in hospice care: An integrative review. Palliat. Care Soc. Pract. 2021, 15, 26323524211051753. [Google Scholar] [CrossRef]
- Valero-Cantero, I.; Martínez-Valero, F.J.; Espinar-Toledo, M.; Casals, C.; Barón-López, F.J.; Vázquez, M. Complementary music therapy for cancer patients in at-home palliative care and their caregivers: Protocol for a multicentre randomised controlled trial. BMC Palliat. Care 2020, 19, 61. [Google Scholar] [CrossRef]
- Valero-Cantero, I.; Casals, C.; Espinar-Toledo, M.; Barón-López, F.J.; Martínez-Valero, F.J.; Soler, N.G.-A.; Vázquez-Sánchez, M. Effect of Self-Chosen Music in Alleviating the Burden on Family Caregivers of Patients with Advanced Cancer: A Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 4662. [Google Scholar] [CrossRef]
- Ortiz, L.B.; González, G.M.C.; Chaparro-Diaz, L.; Herrera, B.S.; Rosero, E.V.; Carreño, S.P. Validez de constructo y confiabilidad del instrumento calidad de vida versión familiar en español. Enfermería Glob. 2015, 14, 227–249. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Larsen, D.L.; Attkisson, C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of client/patient satisfaction: Development of a general scale. Eval. Program Plan. 1979, 2, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Attkisson, C. Assessing client satisfaction among hispanics. Evaluation Program Plan. 1983, 6, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Hanser, S.B.; Butterfield-Whitcomb, J.; Kawata, M.; Collins, B.E. Home-based music strategies with individuals who have dementia and their family caregivers. J. Music. Ther. 2011, 48, 2–27. [Google Scholar] [CrossRef] [PubMed]
- Butow, P.N.; The Australian Ovarian Cancer Study Group; Price, M.A.; Bell, M.L.; Webb, P.M.; Defazio, A.; Friedlander, M.; The Australian Ovarian Cancer Study Quality of Life Study Investigators. Caring for women with ovarian cancer in the last year of life: A longitudinal study of caregiver quality of life, distress and unmet needs. Gynecol. Oncol. 2014, 132, 690–697. [Google Scholar] [CrossRef]
- Ito, E.; Tadaka, E. Effectiveness of the Online Daily Diary (ONDIARY) program on family caregivers of advanced cancer patients: A home-based palliative care trial. Complement. Ther. Clin. Pract. 2021, 46, 101508. [Google Scholar] [CrossRef]
- Gabriel, I.; Creedy, D.; Coyne, E. Quality of life and associated factors among adults living with cancer and their family caregivers. Nurs. Health Sci. 2021, 23, 419–429. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Kravitz, K.; Borneman, T.; Friedmann, E.T. Family Caregivers: A Qualitative Study to Better Understand the Quality-of-Life Concerns and Needs of This Population. Clin. J. Oncol. Nurs. 2018, 22, 286–294. [Google Scholar] [CrossRef]
- Gabriel, I.; Creedy, D.; Coyne, E. A systematic review of psychosocial interventions to improve quality of life of people with cancer and their family caregivers. Nurs. Open 2020, 7, 1299–1312. [Google Scholar] [CrossRef]
- Kim, Y.; Carver, C.S. Unmet needs of family cancer caregivers predict quality of life in long-term cancer survivorship. J. Cancer Surviv. 2019, 13, 749–758. [Google Scholar] [CrossRef]
- Chappell, N.L.; Reid, C. Burden and well-being among caregivers: Examining the distinction. Gerontologist 2002, 42, 772–780. [Google Scholar] [CrossRef]
- Fu, F.; Zhao, H.; Tong, F.; Chi, I. A Systematic Review of Psychosocial Interventions to Cancer Caregivers. Front. Psychol. 2017, 8, 834. [Google Scholar] [CrossRef] [PubMed]
- Batbaatar, E.; Dorjdagva, J.; Luvsannyam, A.; Savino, M.M.; Amenta, P. Determinants of patient satisfaction: A systematic review. Perspect. Public Health 2017, 137, 89–101. [Google Scholar] [CrossRef] [PubMed]

| Total (n = 82) | Intervention Group (n = 41) | Control Group (n = 41) | p-Value | |
|---|---|---|---|---|
| Age (years) | 62.71 (12.56) | 63.12 (12.81) | 62.31 (12.46) | 0.626 |
| Sex | ||||
| Female | 72 (87.8%) | 34 (82.9%) | 38 (92.7%) | 0.177 |
| Male | 10 (12.2%) | 7 (17.1%) | 3 (7.3%) | |
| Education | ||||
| No formal education | 11 (13.4%) | 5 (12.2%) | 6 (14.6%) | 1.000 |
| Primary | 39 (47.6%) | 21 (51.2%) | 18 (43.9%) | |
| Secondary | 22 (26.8%) | 10 (24.4%) | 12 (29.3%) | |
| University | 10 (12.2%) | 5 (12.2%) | 5 (9.8%) | |
| Relationship to the person cared for | ||||
| Spouse | 47 (57.3%) | 27 (65.9%) | 20 (48.8%) | 0.101 |
| Daughter/son | 25 (30.5%) | 8 (19.5%) | 17 (41.5%) | |
| Other | 10 (12.2%) | 6 (14.6%) | 4 (9.8%) | |
| Hours of daily care | 17.47 (7.14) | 18.07 (6.98). | 16.87 (7.34) | 0.448 |
| VAS of the EuroQol-5D-5L | 82.61 (14.79) | 81.71 (15.99) | 83.51 (13.63) | 0.694 |
| QOL-FV (scores) | ||||
| Physical well-being | 7.08 (2.46) | 7.12 (2.42) | 7.04 (2.53) | 0.948 |
| Psychological well-being | 5.56 (1.51) | 5.42 (1.62) | 5.71 (1.38) | 0.649 |
| Social concerns | 5.95 (1.93) | 5.91 (2.04) | 6.00 (1.83) | 0.981 |
| Spiritual wellness | 3,98 (1,81) | 4.17 (1.85) | 3.79 (1.78) | 0.452 |
| Total QOL-FV | 5.64 (1.43) | 5.65 (1.58) | 5.63 (1.28) | 0.742 |
| Intervention Group | Control Group | p-Value between Groups | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Change | p-Value | Pre | Post | Change | p-Value | ||
| QOL-FV (scores) | |||||||||
| Physical well-being | 7.12 (2.47) | 7.56 (1.84) | 0.44 (1.70) | 0.006 | 7.04 (2.53) | 6.18 (2.34) | −0.86 (1.89) | 0.106 | 0.004 |
| Psychological well-being | 5.42 (1.67) | 5.63 (1.58) | 0.22 (1.00) | 0.297 | 5.71 (1.39) | 5.53 (1.60) | −0.18 (1.09) | 0.272 | 0.119 |
| Social concerns | 5.91 (2.04) | 6.19 (1.84) | 0.28 (1.03) | 0.233 | 6.00 (1.83) | 5.69 (2.04) | −0.31 (1.62) | 0.065 | 0.024 |
| Spiritual wellness | 4.17 (1.85) | 3.97 (1.54) | −0.30 (1.27) | 0.825 | 3.79 (1.78) | 3.76 (1.85) | −0.03 (1.00) | 0.196 | 0.883 |
| Total QOL-FV | 5.65 (1.58) | 5.81 (1.23) | 0.16 (0.75) | 0.023 | 5.63 (1.28) | 5.28 (1.25) | −0.35 (0.94) | 0.102 | 0.008 |
| VAS of the EuroQol-5D-5L | 81.71 (15.99) | 88.00(13.03) | 6.29 (10.71) | 0.002 | 83.51 (13.63) | 79.76 (12.1) | −3.76 (7.26) | 0.001 | <0.001 |
| CSQ-8 (score) | - | 27.54 (3.25) | - | - | - | 24.80 (4.03) | - | - | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valero-Cantero, I.; Casals, C.; Espinar-Toledo, M.; Barón-López, F.J.; García-Agua Soler, N.; Vázquez-Sánchez, M.Á. Effects of Music on the Quality of Life of Family Caregivers of Terminal Cancer Patients: A Randomised Controlled Trial. Healthcare 2023, 11, 1985. https://doi.org/10.3390/healthcare11141985
Valero-Cantero I, Casals C, Espinar-Toledo M, Barón-López FJ, García-Agua Soler N, Vázquez-Sánchez MÁ. Effects of Music on the Quality of Life of Family Caregivers of Terminal Cancer Patients: A Randomised Controlled Trial. Healthcare. 2023; 11(14):1985. https://doi.org/10.3390/healthcare11141985
Chicago/Turabian StyleValero-Cantero, Inmaculada, Cristina Casals, Milagrosa Espinar-Toledo, Francisco Javier Barón-López, Nuria García-Agua Soler, and María Ángeles Vázquez-Sánchez. 2023. "Effects of Music on the Quality of Life of Family Caregivers of Terminal Cancer Patients: A Randomised Controlled Trial" Healthcare 11, no. 14: 1985. https://doi.org/10.3390/healthcare11141985
APA StyleValero-Cantero, I., Casals, C., Espinar-Toledo, M., Barón-López, F. J., García-Agua Soler, N., & Vázquez-Sánchez, M. Á. (2023). Effects of Music on the Quality of Life of Family Caregivers of Terminal Cancer Patients: A Randomised Controlled Trial. Healthcare, 11(14), 1985. https://doi.org/10.3390/healthcare11141985