
Effects of Exercise Intervention (with and without Joint Mobilization) in Patients with Adhesive Capsulitis: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Literature Search Strategy
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- A peer-reviewed study published in English between 2000 and 2021 investigating the effect of exercise and joint mobilization in patients with AC;
- Outcome variables including shoulder ROM, subjective function, and pain;
- Studies in which the results were described or converted to mean and standard deviation.
2.2.2. Exclusion Criteria
- Case studies using a single-subject design;
- Studies that did not definitively establish that the participants were patients with AC;
- Studies in which interventions other than exercise and/or exercise with joint mobilization were added and applied as confounding variables (e.g., injection, operation, drug, ultrasound).
2.3. Assessment of Methodologic Quality
2.4. Assessment of Publication Bias
2.5. Data Synthesis and Extraction
3. Results
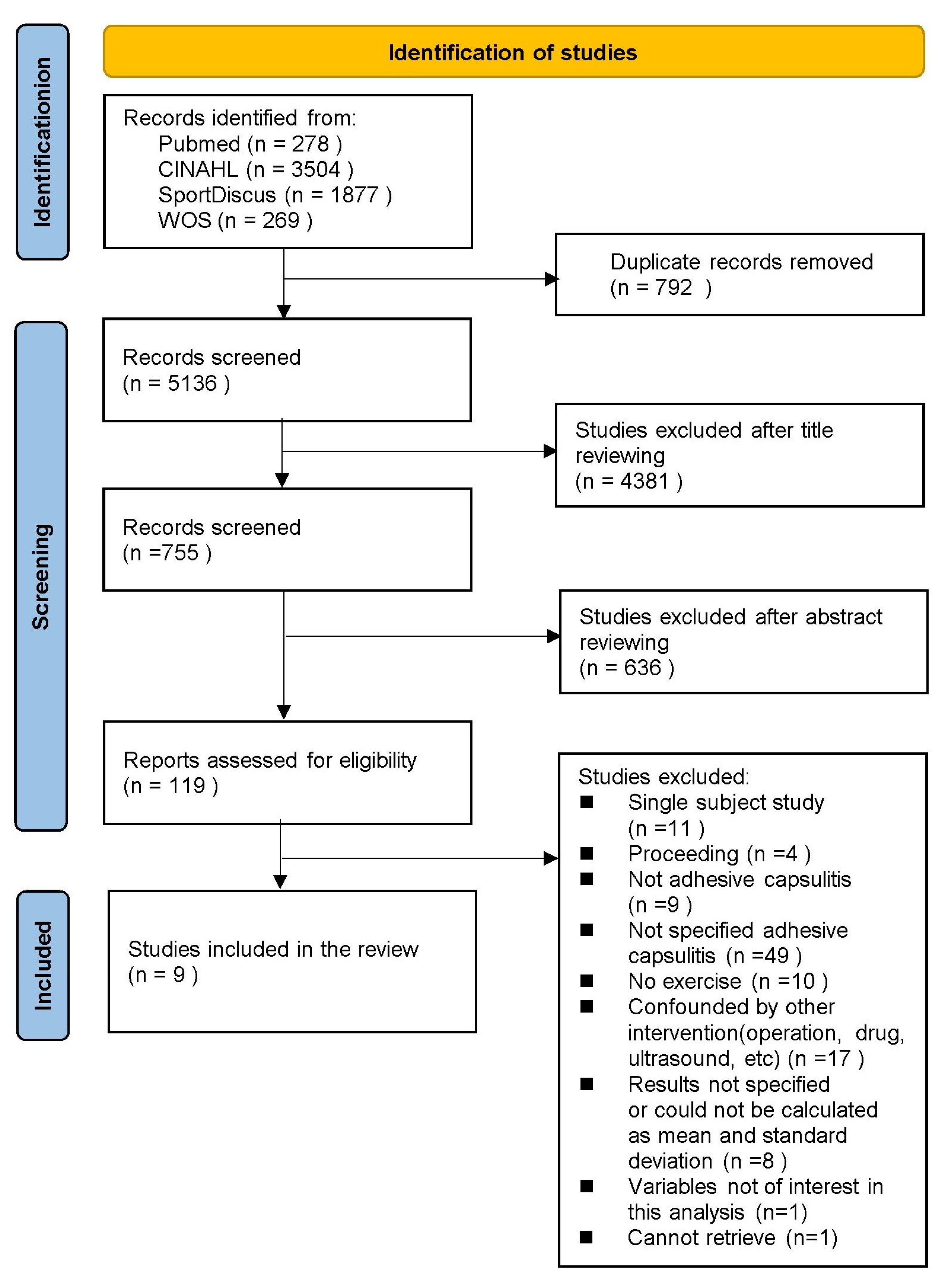
3.1. Study Selection
3.2. Level of Evidence and Strength of Recommendation
3.3. Publication Bias
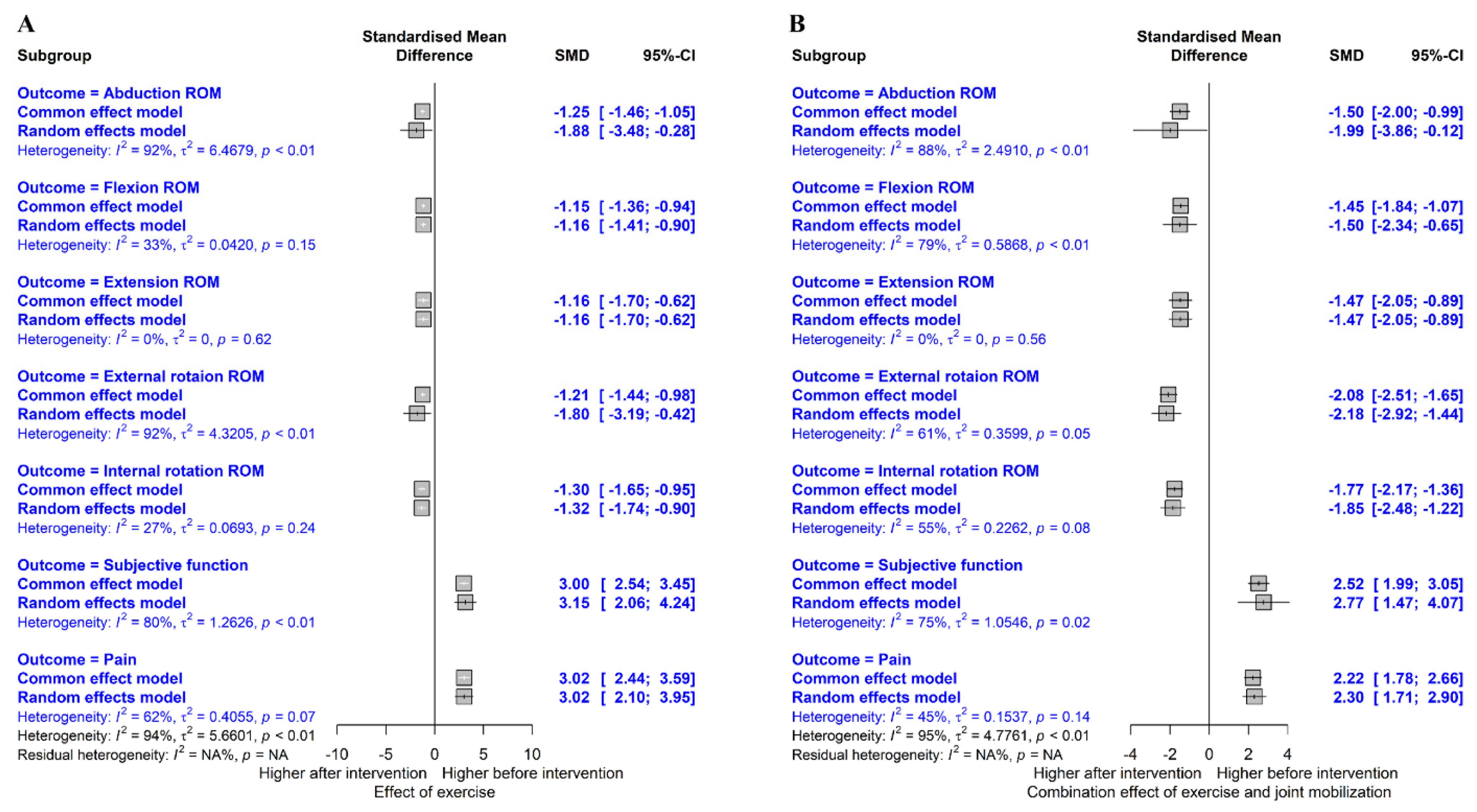
3.4. Data Synthesis
3.4.1. Flexion ROM
3.4.2. Extension ROM
3.4.3. Internal Rotation ROM
3.4.4. External Rotation ROM
3.4.5. Abduction ROM
3.4.6. Subjective Function
3.4.7. Pain
4. Discussion
4.1. Effect on Shoulder ROM
4.2. Effect on Shoulder Subjective Function and Pain
4.3. Implications of Virtual Reality Training and Coracohumeral Ligament Stretching
4.4. Overall Implications and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Codman, E.A. Rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. In The Shoulder; Thomas Todd Company: Boston, MA., USA, 1934; p. 514. [Google Scholar]
- Nakandala, P.; Nanayakkara, I.; Wadugodapitiya, S.; Gawarammana, I. The efficacy of physiotherapy interventions in the treatment of adhesive capsulitis: A systematic review. J. Back Musculoskelet. Rehabil. 2021, 34, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.E.; Anakwenze, O.A.; Warrender, W.J.; Abboud, J.A. Current review of adhesive capsulitis. J. Shoulder Elb. Surg. 2011, 20, 502–514. [Google Scholar] [CrossRef] [PubMed]
- Neviaser, R.J.; Neviaser, T.J. The frozen shoulder. Diagnosis and management. Clin. Orthop. Relat. Res. 1987, 223, 59–64. [Google Scholar] [CrossRef]
- Neviaser, A.S.; Neviaser, R.J. Adhesive capsulitis of the shoulder. J. Am. Acad. Orthop. Surg. 2011, 19, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Mao, C.Y.; Jaw, W.C.; Cheng, H.C. Frozen shoulder: Correlation between the response to physical therapy and follow-up shoulder arthrography. Arch. Phys. Med. Rehabil. 1997, 78, 857–859. [Google Scholar] [CrossRef]
- Ballantyne, B.T.; O’Hare, S.J.; Paschall, J.L.; Pavia-Smith, M.M.; Pitz, A.M.; Gillon, J.F.; Soderberg, G.L. Electromyographic activity of selected shoulder muscles in commonly used therapeutic exercises. Phys. Ther. 1993, 73, 668–677. [Google Scholar] [CrossRef]
- De la Serna, D.; Navarro-Ledesma, S.; Alayón, F.; López, E.; Pruimboom, L. A comprehensive view of frozen shoulder: A mystery syndrome. Front. Med. 2021, 8, 663703. [Google Scholar] [CrossRef]
- Hollmann, L.; Halaki, M.; Kamper, S.J.; Haber, M.; Ginn, K.A. Does muscle guarding play a role in range of motion loss in patients with frozen shoulder? Musculoskelet. Sci. Pract. 2018, 37, 64–68. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Ando, A.; Kanazawa, K.; Koide, M.; Sekiguchi, T.; Hamada, J.; Itoi, E. Arthroscopic coracohumeral ligament release for patients with frozen shoulder. Arthrosc. Tech. 2017, 7, e1–e5. [Google Scholar] [CrossRef]
- Cho, C.H.; Song, K.S.; Kim, B.S.; Kim, D.H.; Lho, Y.M. Biological aspect of pathophysiology for frozen shoulder. Biomed. Res. Int. 2018, 2018, 7274517. [Google Scholar] [CrossRef]
- Harryman, D.T., 2nd; Sidles, J.A.; Clark, J.M.; McQuade, K.J.; Gibb, T.D.; Matsen, F.A., 3rd. Translation of the humeral head on the glenoid with passive glenohumeral motion. J. Bone Jt. Surg. Am. 1990, 72, 1334–1343. [Google Scholar] [CrossRef]
- Neviaser, J.S. Adhesive capsulitis of the shoulder: A study of the pathological findings in periarthritis of the shoulder. J. Bone Jt. Surg. 1945, 27, 211–222. [Google Scholar]
- Reeves, B. The natural history of the frozen shoulder syndrome. Scand. J. Rheumatol. 1975, 4, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Vastamäki, H.; Kettunen, J.; Vastamäki, M. The natural history of idiopathic frozen shoulder: A 2- to 27-year followup study. Clin. Orthop. Relat. Res. 2012, 470, 1133–1143. [Google Scholar] [CrossRef]
- Kaltenborn, F.M. Specializad techniques: Tests and joint-mobilisation. In Manual Therapy for the Extremity Joints; Olaf Norlis Bokhandel: Oslo, Norway, 1976. [Google Scholar]
- Yaver, J. Maitland’s Peripheral Manipulation, ed 4. Phys. Ther. 2007, 87, 118–119. [Google Scholar] [CrossRef]
- Nicholson, G.G. The effects of passive joint mobilization on pain and hypomobility associated with adhesive capsulitis of the shoulder. J. Orthop. Sport. Phys. Ther. 1985, 6, 238–246. [Google Scholar] [CrossRef]
- Zavala-González, J.; Pavez-Baeza, F.; Gutiérrez-Espinoza, H.; Olguín-Huerta, C. The effectiveness of joint mobilization techniques for range of motion in adult patients with primary adhesive capsulitis of the shoulder: A systematic review and meta-analysis. Medwave 2018, 18, e7265. [Google Scholar] [CrossRef]
- Mangus, B.C.; Hoffman, L.A.; Hoffman., M.A.; Altenburger, P. Basic principles of extremity joint mobilization using a Kaltenborn approach. J. Sport Rehabil. 2002, 11, 235–250. [Google Scholar] [CrossRef]
- Vermeulen, H.M.; Rozing, P.M.; Obermann, W.R.; Le Cessie, S.; Vliet Vlieland, T.P. Comparison of high-grade and low-grade mobilization techniques in the management of adhesive capsulitis of the shoulder: Randomized controlled trial. Phys. Ther. 2006, 86, 355–368. [Google Scholar] [CrossRef]
- Çelik, D.; Kaya Mutlu, E.K. Does adding mobilization to stretching improve outcomes for people with frozen shoulder? A randomized controlled clinical trial. Clin. Rehabil. 2016, 30, 786–794. [Google Scholar] [CrossRef]
- Ali, S.A.; Khan, M. Comparison for efficacy of general exercises with and without mobilization therapy for the management of adhesive capsulitis of shoulder-An interventional study. Pak. J. Med. Sci. 2015, 31, 1372–1376. [Google Scholar] [CrossRef] [PubMed]
- Sirajuddin, M.; Quddus, N.; Grover, D. Comparison of anterior versus posterior glide mobilization techniques for improving internal rotation range of motion in shoulder adhesive capsulitis. Indian J. Physiother. Occup. 2010, 4, 152–157. [Google Scholar]
- Chan, S.; Hill, R.; Kerr, J. Passive joint mobilisation: Does it enhance outcome of adhesive capsulitis of the shoulder following corticosteroid injection? Int. Musculoskelet. Med. 2010, 32, 58–67. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Anjum, R.; Aggarwal, J.; Gautam, R.; Pathak, S.; Sharma, A. Evaluating the outcome of two different regimes in adhesive capsulitis: A prospective clinical study. Med. Princ. Pract. 2020, 29, 225–230. [Google Scholar] [CrossRef]
- Bhavana, D.R.; Soni, S. Immediate effects of positional stretching of coracohumeral ligament in individuals with adhesive capsulitis. Indian J. Physiother. Occup. Ther. 2017, 11, 107–111. [Google Scholar] [CrossRef]
- Gupta, D.; Desai, O.P.; Rastogi, S. To compare the effect of home based program and supervised occupational therapy program in adhesive capsulitis patients with diabetes mellitus. Indian J. Physiother. Occup. Ther. 2019, 13, 48–53. [Google Scholar] [CrossRef]
- Jellad, A.; May, W.; Zrig, A.; Kalai, A.; Jguirim, M.; Frih, Z.B.S.; Golli, M. Intra-articular distension preceded by physical therapy versus intra-articular distension followed by physical therapy for treating adhesive capsulitis of the shoulder. J. Back Musculoskelet. Rehabil. 2020, 33, 443–450. [Google Scholar] [CrossRef]
- Lee, S.H.; Yeh, S.C.; Chan, R.C.; Chen, S.; Yang, G.; Zheng, L.-R. Motor ingredients derived from a wearable sensor-based virtual reality system for frozen shoulder rehabilitation. BioMed Res. Int. 2016, 2016, 7075464. [Google Scholar] [CrossRef]
- Shishir, M.S.; Abraham, M.M.; Kanagasabai, R.; Najimudeen, S.; Gnanadoss, J.J. Home based exercise program for frozen shoulder-follow-up of 36 idiopathic frozen shoulder patients. Indian J. Physiother. Occup. Ther. 2013, 7, 221–226. [Google Scholar] [CrossRef]
- Chidambaram, R.; Muruganandam, P.; Bhandure, K.S. The efficacy of sleeper’s stretch and movement with mobilization on pain, range of motion & functional capacity in patients with adhesive capsulitis. Indian J. Physiother. Occup. Ther. 2020, 14, 149–155. [Google Scholar] [CrossRef]
- Kushwah, S.S.; Srivastava, N. Comparison between effectiveness of active release technique and capsular stretch along with conventional therapy in the management of frozen shoulder. Indian J. Physiother. Occup. Ther. 2018, 12, 85–90. [Google Scholar] [CrossRef]
- Hand, C.; Clipsham, K.; Rees, J.L.; Carr, A.J. Long-term outcome of frozen shoulder. J. Shoulder Elb. Surg. 2008, 17, 231–236. [Google Scholar] [CrossRef]
- van den Hout, W.B.; Vermeulen, H.M.; Rozing, P.M.; Vlieland, T.P.V. Impact of adhesive capsulitis and economic evaluation of high-grade and low-grade mobilisation techniques. Aust. J. Physiother. 2005, 51, 141–149. [Google Scholar] [CrossRef]
- Brotzman, S.D.; Manske, R.D. Clinical Orthopaedic Rehabilitation: An Evidence-Based Approach, 3rd ed.; Mosby: Maryland, MO, USA, 2011. [Google Scholar]
- Griggs, S.M.; Ahn, A.; Green, A. Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. JBJS 2000, 82, 1398. [Google Scholar] [CrossRef]
- Dogru, H.; Basaran, S.; Sarpel, T. Effectiveness of therapeutic ultrasound in adhesive capsulitis. Jt. Bone Spine 2008, 75, 445–450. [Google Scholar] [CrossRef]
- Jewell, D.V.; Riddle, D.L.; Thacker, L.R. Interventions associated with an increased or decreased likelihood of pain reduction and improved function in patients with adhesive capsulitis: A retrospective cohort study. Phys. Ther. 2009, 89, 419–429. [Google Scholar] [CrossRef]
- Ruiz, J.O. Positional stretching of the coracohumeral ligament on a patient with adhesive capsulitis: A case report. J. Man Manip. Ther. 2009, 17, 58–63. [Google Scholar] [CrossRef]
- Wattanaprakornkul, D.; Halaki, M.; Boettcher, C.; Cathers, I.; Ginn, K.A.A. Comprehensive analysis of muscle recruitment patterns during shoulder flexion: An electromyographic study. Clin. Anat. 2011, 24, 619–626. [Google Scholar] [CrossRef]
- Kingston, K.; Curry, E.J.; Galvin, J.W.; Li, X. Shoulder adhesive capsulitis: Epidemiology and predictors of surgery. J. Shoulder Elb. Surg. 2018, 27, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.D.; Wirth, M.A.; Rockwood, C.A. Thawing the frozen shoulder: The “patient” patient. Orthopedics 1996, 19, 849–853. [Google Scholar] [CrossRef] [PubMed]
- Minter, W.T., 3rd. The shoulder-hand syndrome in coronary disease. J. Med. Assoc. GA 1967, 56, 45–49. [Google Scholar] [PubMed]
- Ogilvie-Harris, D.J.; Myerthall, S. The diabetic frozen shoulder: Arthroscopic release. Arthroscopy 1997, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (year) | Study Design | Participants (n, Age) | Inclusion Criteria of Participants | Exclusion Criteria of Participants | Exercise Intervention | Outcome Measurement | Major Findings |
|---|---|---|---|---|---|---|---|
| Anjum et al. (2020) [29] | RCT | PT (n = 26, 41.12) PT + IASI (n = 26, 44.46) | Diagnosed idiopathic frozen shoulder of <6 month duration, age between 18 and 65 years, nontraumatic stiff shoulder, non-diabetic state, and restriction of active and passive motion >30° in two or more planes. | Systemic inflammatory joint disease, skeletally immature patients, contraindications to joint distension including allergy to local anesthetic, and shoulder abnormality detected on plain X-ray | Stretching, pendulum exercises, active-assisted exercises. isometric, concentric strengthening exercises | Index (SPADI), pain (VAS), ROM (flexion, abduction, external rotation) muscular power (supraspinatus, infraspinatus, subscapularis) | Range of shoulder flexion, abduction, external rotation, and SPADI significantly improved in PT + IASI compared to PT |
| Bhavana and Soni (2017) [30] | Pre-post | n = 16, 40–80 | Duration of complaints of >3 months, age 40–80 years old, spontaneous onset of the painful stiff shoulder, movement impairment in 1 or more of 3 movement directions, loss of active and passive shoulder motion with external rotation restriction of <50, an extension of <30, and adduction <30 | Not described | Stretching of coracohumeral ligament | ROM (flexion, extension, external rotation, abduction, adduction) | Passive range of motion was significantly improved following stretching of coracohumeral ligament |
| Gupta et al. (2019) [31] | CER | supervised OT (n = 16, 40–60) Home based OT (n = 19, 40–60) | AC with diabetes mellitus, with age group 40–60 | History of any life-threatening disease or history of any musculoskeletal injury, traumatic injury, or shoulder pain due to fracture or any other pathology in past 6 months | Occupational therapy | Index (SPADI) ROM (flexion, extension, internal rotation, abduction | Both groups showed no significant difference in any of the variables. |
| Jellad et al. (2020) [32] | RCT | IAD-PT (n = 34, 55.7 ± 9.8) PT, IAD (n = 46, 55.1 ± 7.7) PT (n = 42, 55 ± 10.4) | Primitive AC of the shoulder | AC secondary to trauma, operation, hypothyroidism, stroke, rotator cuff lesion. Tendon rupture. Those who had a previous IAD, and those who had physical therapy or intra-articular corticosteroid injection in the last three months | Stretching, pendulum exercises passive, active-assisted exercises | Index (DASH), Pain (VAS), PROM, AROM (FLEX, ER, ABD) | IAD followed by PT is more beneficial than IAD preceded by PT in terms of upper extremity function |
| Lee et al. (2016) [33] | Pre-post | n = 16, 58.6 | 20 < age, not received PT, clinically confirmed to have frozen shoulders | History of a proximal humeral fracture or dislocation of glenohumeral joint, received hyaluronic acid injection in the shoulder, experienced cervical radiculopathy or diagnosed with shoulder degenerative joint diseases, at the final stage of a malignant disease, pregnant. | Stretching, shoulder, core strengthening | ROM, strength (FLEX, ER, IR, ABD) | Task performance, motor indices, and the clinical assessments indicated significant improvement for most of the assessed items. Task performance effectively predicted the results of several clinical assessment items. |
| Shishir et al. (2013) [34] | Pre-post | n = 36, 33–73 | Symptom of >4 weeks and <6 months, 25% limited active, passive range of ABD, ER compared with the other shoulder, minimum follow-up 2 years | Pain of <4, osteopenia, received intra-articular injection or prior PT before start of the protocol, limitation of movement in one plane only, pain originated from acromioclavicular joint, presenting with frozen shoulder secondary to other disease, osteoarthritis, rotator cuff tear, cervical spine disease, trauma, inflammation | Shoulder Accelerated Rehabilitation Protocol | Constant score, pain (VAS), ROM (ER, ABD) | The mean constant shoulder score at the start of protocol was 26.69 (SD-8.522), which improved to 98.58 (SD-2.892) at 15 months. Pain score at the start of the protocol was 7.14 (SD-1.222) which improved at 18 months |
| Author (Year) | Study Design | Participants (n, age) | Inclusion Criteria of Participants | Exclusion Criteria of Participants | Exercise & Mobilization | Outcome Variables | Major Findings |
|---|---|---|---|---|---|---|---|
| Chidambaram et al. (2020) [35] | RCT | MWM (n = 25, 40–70) MWM + stretching (n = 25, 40–70) | AC at stage 1 and 2 (David J Magee) were included between the age groups of 40 to 70 years with minimum 90 degrees of shoulder FLEX and ABD. | Possess malignancy, neck pain with radiculopathy and recent shoulder injuries | Sleeper stretching (only for MWM + stretching group), pendular exercises, finger ladder exercises and active ROM and glide to increase FLEX, IR, ER | Index (SPADI), Pain (NPRS) ROM (FLEX, IR, ER) | The group which received sleeper’s stretch with MWM shows high significant in improving range of motion and pain. |
| Çelik and Mutlu (2016) [22] | RCT | Stretching (n = 12, 54.8 ± 6.4) Stretching +mobilization (n = 14, 54.2 ± 7.9) | Range of FLEX, ER, ABD less than 50% in comparison to uninvolved shoulder, normal radiographic results (anteroposterior and lateral views), complaint of >months | Cervical radiculopathy and radiating pain from wrist or hand, diabetes, thoracic outlet syndrome, rheumatological disorders, fractures, or tumors of either upper extremity, neurological disorders that cause muscle weakness in the shoulder corticosteroid injections in the affected shoulder within the previous 4 weeks, rotator cuff tears | Cyclic stretching, strengthening exercises for the scapulothoracic and rotator cuff muscles, and caudal, anterior, posterior glide of glenohumeral joint (stretching +mobilization group) | Index (DASH, Constant score) Pain (VAS), PROM (FLEX, ER, IR, ABD) | Significant increases in ABD, ER and constant score at the 1-year follow-up in the stretching +mobilization, whereas stretching group did not show significant changes. |
| Kushwah and Namrata (2018) [36] | RCT | Capsular stretch (n = 15, 40–60) Capsular stretch +ART (n = 15, 40–60 | Painful stiff shoulder of >3 months, age between 40–60, limited ROM compared to non-involved side, inability to lie on affected shoulder, primary idiopathic periarthritis shoulder | History of surgery on the shoulder, rotator cuff rupture, pain related to trauma, fracture of the shoulder complex, osteoarthritis, or signs of bony damage, inflammatory diseases (i.e., rheumatoid arthritis) | ABD, ER exercise (capsular stretch + ART group alone) Sit or stand exercise and stretch of anterior, posterior, antero-inferior capsule | Pain (VAS), ROM (FLEX, EXT, ER, IR, ABD) | Significant improvement in both groups for VAS and ROM. Significant difference in effect of capsular stretch +ART with conventional therapy than capsular stretch only |
| NIH Study Quality Assessment Tools | Anjum et al. (2020) [29] | Bhavana and Soni (2017) [30] | Çelik and Mutlu (2016) [22] | Chidambaram et al. (2020) [35] | Gupta et al. (2019) [31] | Jellad et al. (2020) [32] | Kushwah and Namrata (2018) [36] | Lee et al. (2016) [33] | Shishir et al. (2013) [34] |
|---|---|---|---|---|---|---|---|---|---|
| 1. Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? Was the method of randomization adequate? | Yes | No | Yes | Yes | No | Yes | Yes | No | No |
| 2. Was the study described as a controlled trial? Was the control group matched on relevant variables (age, gender, education, disorder)? | Yes | No | Yes | Yes | Yes | Yes | Yes | No | No |
| 3. Was the overall dropout rate from the study at endpoint 20% or lower of the number allocated to the intervention? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4. Was the differential dropout rate (between groups) at endpoint 15 percentage points or lower? | Yes | CD | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 5. Was there high adherence to the intervention protocols for each treatment group? (Defined as 75 % attendance or more) | CD | CD | CD | CD | CD | CD | CD | CD | CD |
| 6. Were other interventions avoided or similar in the groups? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 7. Were outcomes assessed using valid and reliable measures? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 8. Were outcomes measured consistently across all study participants? | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes |
| 9. Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 10. Were outcomes reported or subgroups analyzed prespecified (i.e., identified before analyses were conducted)? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 11. For RCTs, were all randomized participants analyzed in the group to which they were originally assigned? For controlled studies, was a recognized statistical method employed? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Score (%) | 10 (91) | 6 (55) | 9 (82) | 10 (91) | 10 (91) | 9 (82) | 10 (91) | 7 (64) | 8 (73) |
| Level of evidence | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Jeon, H.G.; Yoon, Y.J. Effects of Exercise Intervention (with and without Joint Mobilization) in Patients with Adhesive Capsulitis: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 1504. https://doi.org/10.3390/healthcare11101504
Lee JH, Jeon HG, Yoon YJ. Effects of Exercise Intervention (with and without Joint Mobilization) in Patients with Adhesive Capsulitis: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(10):1504. https://doi.org/10.3390/healthcare11101504
Chicago/Turabian StyleLee, Jong Hyeon, Hyung Gyu Jeon, and Yong Jin Yoon. 2023. "Effects of Exercise Intervention (with and without Joint Mobilization) in Patients with Adhesive Capsulitis: A Systematic Review and Meta-Analysis" Healthcare 11, no. 10: 1504. https://doi.org/10.3390/healthcare11101504
APA StyleLee, J. H., Jeon, H. G., & Yoon, Y. J. (2023). Effects of Exercise Intervention (with and without Joint Mobilization) in Patients with Adhesive Capsulitis: A Systematic Review and Meta-Analysis. Healthcare, 11(10), 1504. https://doi.org/10.3390/healthcare11101504