
Interprofessional Collaborative Clinical Practice in Medicine and Pharmacy: Measure of Student Perceptions Using the SPICE-R2F Instrument to Bridge Health-Care Policy and Education in France

Abstract
:1. Introduction
2. Materials and Methods
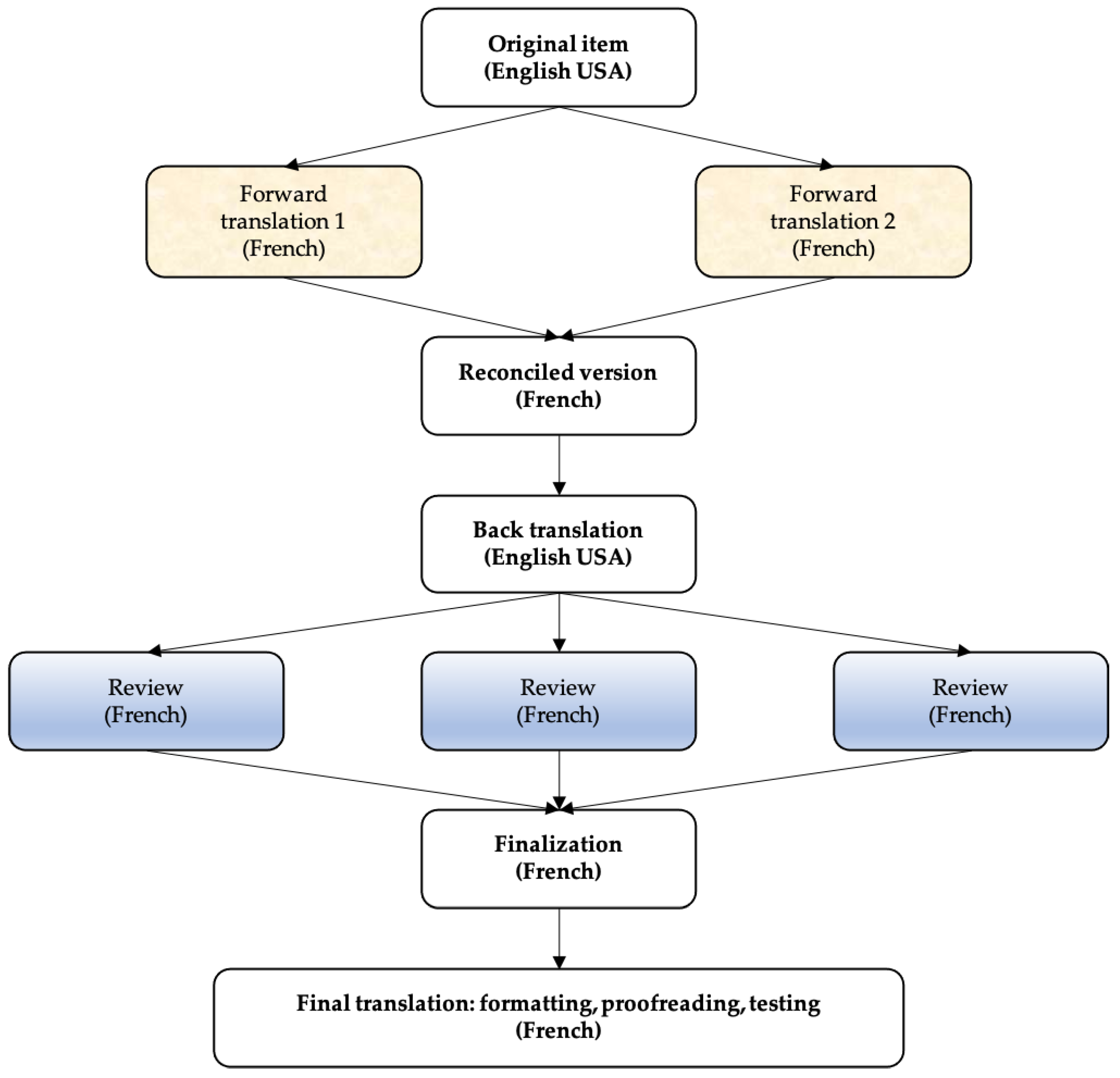
2.1. Translation Process
2.2. Cohorts
2.3. Statistical Analysis
3. Results
3.1. Translation
3.2. Psychometric Validation of the Translation
3.2.1. Descriptive Statistics
3.2.2. Confirmatory Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Délégation, Transfert, Nouveaux Métiers. Comment Favoriser les Formes Nouvelles de Coopération Entre Professionnels de Santé. Haute Autorité de Santé. Available online: https://www.has-sante.fr/jcms/c_497724/fr/delegation-transfert-nouveaux-metiers-comment-favoriser-les-formes-nouvelles-de-cooperation-entre-professionnels-de-sante (accessed on 16 September 2021).
- Article 51-LOI n° 2009-879 du 21 Juillet 2009 Portant Réforme de L’hôpital et Relative aux Patients, à la Santé et aux Territoires-Légifrance. Available online: https://www.legifrance.gouv.fr/jorf/article_jo/JORFARTI000020879543 (accessed on 3 July 2021).
- Protocole de Coopération Entre Professionnels de Santé. Haute Autorité de Santé. Available online: https://www.has-sante.fr/jcms/c_1240280/fr/protocole-de-cooperation-entre-professionnels-de-sante (accessed on 13 September 2021).
- Grande Conférence de la Santé. Conseil économique, Social et Environnemental (Paris, 11 February 2016). Available online: https://solidarites-sante.gouv.fr/archives/grande-conference-de-la-sante-10527/ (accessed on 14 September 2021).
- DGOS. L’exercice Coordonné. Ministère des Solidarités et de la Santé (Paris, 2021). Available online: https://solidarites-sante.gouv.fr/professionnels/se-former-s-installer-exercer/l-exercice-coordonne-entre-professionnels-de-sante/article/l-exercice-coordonne (accessed on 14 September 2021).
- World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. 2010. Available online: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice (accessed on 14 September 2021).
- Boland, D.H.; Scott, M.A.; Kim, H.; White, T.; Adams, E. Interprofessional immersion: Use of interprofessional education collaborative competencies in side-by-side training of family medicine, pharmacy, nursing, and counselling psychology trainees. J. Interprofessional Care 2016, 30, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Birk, T.J. Principles for Developing an Interprofessional Education Curriculum in a Healthcare Program. J. Healthc. Commun. 2017, 2, 1–4. Available online: https://healthcare-communications.imedpub.com/principles-for-developing-an-interprofessional-education-curriculum-in-a-healthcare-program.php?aid=18276 (accessed on 16 September 2021). [CrossRef]
- Committee on Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes; Board on Global Health; Institute of Medicine. Conceptual Framework for Measuring the Impact of IPE. In Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes; National Academies Press: Washington, DC, USA, 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK338356/ (accessed on 16 September 2021).
- Health Professions Accreditors Collaborative. Available online: https://healthprofessionsaccreditors.org/ (accessed on 16 September 2021).
- Accreditation Council for Pharmacy Education. Accreditation Standards and Key Elements for the Professional Program in Pharmacy Leading to the Doctor of Pharmacy Degree. Standards 2016; Accreditation Council for Pharmacy Education: Chicago, IL, USA, 2015; Available online: https://www.acpe-accredit.org/pdf/Standards2016FINAL.pdf (accessed on 16 September 2021).
- Accreditation Council for Graduate Medical Education. Common Program Requirements (Residency) 2021. Available online: https://www.acgme.org/globalassets/PFAssets/ProgramRequirements/CPRResidency2020.pdf (accessed on 18 September 2021).
- Cloutier, J.; Lafrance, J.; Michallet, B.; Marcoux, L.; Cloutier, F. French translation and validation of the Readiness for Interprofessional Learning Scale (RIPLS) in a Canadian undergraduate healthcare student context. J. Interprofessional Care 2015, 29, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Mahler, C.; Berger, S.; Reeves, S. The Readiness for Interprofessional Learning Scale (RIPLS): A problematic evaluative scale for the interprofessional field. J. Interprofessional Care 2015, 29, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Fike, D.S.; Zorek, J.A.; MacLaughlin, A.A.; Samiuddin, M.; Young, R.B.; MacLaughlin, E.J. Development and Validation of the Student Perceptions of Physician-Pharmacist Interprofessional Clinical Education (SPICE) Instrument. Am. J. Pharm. Educ. 2013, 77, 190. Available online: https://www.ajpe.org/content/77/9/190 (accessed on 18 January 2021). [CrossRef] [PubMed]
- Zorek, J.A.; MacLaughlin, E.J.; Fike, D.S.; MacLaughlin, A.A.; Samiuddin, M.; Young, R.B. Measuring changes in perception using the Student Perceptions of Physician-Pharmacist Interprofessional Clinical Education (SPICE) instrument. BMC Med. Educ. 2014, 14, 101. [Google Scholar] [CrossRef] [PubMed]
- Pudritz, Y.M.; Fischer, M.R.; Eickhoff, J.C.; Zorek, J.A. Validity and reliability of an adapted German version of the Student Perceptions of Physician-Pharmacist Interprofessional Clinical Education Instrument, version 2 (SPICE-2D). Int. J. Pharm. Pract. 2020, 28, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Brisolara, K.F.; Culbertson, R.; Levitzky, E.; Mercante, D.E.; Smith, D.G.; Gunaldo, T.P. Supporting Health System Transformation: The development of an integrated interprofessional curriculum inclusive of public health students. J. Health Adm. Educ. 2019, 36, 111–121. [Google Scholar] [PubMed]
- Eremenco, S.L.; Cella, D.; Arnold, B.J. A comprehensive method for the translation and cross-cultural validation of health status questionnaires. Eval. Health Prof. 2005, 28, 212–232. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Larousse. Dictionnaire de français Larousse. Available online: https://www.larousse.fr/dictionnaires/francais/%C3%A9ducation/27867 (accessed on 2 October 2021).
- Bentler, P.M. Alpha, Dimension-Free, and Model-Based Internal Consistency Reliability. Psychometrika 2008, 74, 137. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.; Kim, S. Cronbach’s Coefficient Alpha: Well Known but Poorly Understood. Organ. Res. Meth. 2015, 18, 207–230. [Google Scholar] [CrossRef]
- Green, S.B.; Yang, Y. Commentary on Coefficient Alpha: A Cautionary Tale. Psychometrika 2009, 74, 121–135. [Google Scholar] [CrossRef]
- Revelle, W.; Zinbarg, R.E. Coefficients Alpha, Beta, Omega, and the glb: Comments on Sijtsma. Psychometrika 2008, 74, 145. [Google Scholar] [CrossRef]
- Sijtsma, K. On the Use, the Misuse, and the Very Limited Usefulness of Cronbach’s Alpha. Psychometrika 2008, 74, 107. [Google Scholar] [CrossRef] [PubMed]
- Couty, E.; Kouchner, C.; Laude, A.; Tabuteau, D. La loi HPST Regards sur la Réforme de Santé. Available online: https://www.presses.ehesp.fr/wp-content/uploads/2016/03/9782810900220.pdf (accessed on 11 February 2021).
- Vezinat, N. Vers une médecine collaborative: Politique des maisons de santé pluri-professionnelles en France; Presses Universitaires de France: Paris, France, 2019; 213p. [Google Scholar]
- Zorek, J.A. Chapitre 2 Community Pharmacy-Community Pharmacists’ Contributions to Interprofessional Health Teams. In Interprofessional Practice in Pharmacy: Featuring Illustrated Case Studies; McGraw-Hill Education/Medical: New York, NY, USA, 2021; 384p. [Google Scholar]
- Arrêté du 9 Mars 2018 Portant Approbation de L’avenant 12 à la Convention Nationale du 4 mai 2012, Organisant les Rapports Entres les Pharmaciens Titulaires d’officine et L’assurance Maladie. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000036711358/ (accessed on 11 February 2021).
- Harden, R.M. What is a spiral curriculum? Med. Teach. 1999, 21, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Rosalind Franklin University of Medecine and Science. Curriculum for the Chicago Medical School. Phase I M2 Year, Professionnal Developpement Skills: Team-Based Care (Interprofessionnal). Rosalind Franklin University. Available online: https://www.rosalindfranklin.edu/academics/chicago-medical-school/degree-programs/allopathic-medicine-md/curriculum/ (accessed on 13 September 2021).
- Fiquet, L.; Huge, S.; Annezo, F.; Chapron, A.; Allory, E.; Renaut, P. Une formation inter professionnelle pour apprendre à travailler ensemble. La perception des étudiants en santé. Pédagogie Médicale 2015, 16, 105–117. [Google Scholar] [CrossRef]
- CNG, Concours Médicaux. Available online: https://www.cng.sante.fr/concours-examens/concours-medicaux (accessed on 8 November 2021).
- Si-Mohamed, S.; Boussel, L.; Milot, L.; Rousset, P. Mise au point didactique: L’examen clinique objectif et structuré ou «ECOS» en imagerie médicale. J. Imag. Diagn. Interv. 2021, 5, 43–54. [Google Scholar] [CrossRef]
- Cruess, R.L.; Cruess, S.R.; Boudreau, J.D.; Snell, L.; Steinert, Y. A Schematic Representation of the Professional Identity Formation and Socialization of Medical Students and Residents: A Guide for Medical Educators. Acad. Med. 2015, 90, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Canadian Interprofessional Health Collaborative. Available online: http://www.cihc-cpis.com/ (accessed on 12 August 2022).
- Interprofessional Education Collaborative. Available online: https://www.ipecollaborative.org/ (accessed on 12 August 2022).
- National Academies Sciences Engineering Medicine. Available online: https://www.nationalacademies.org/ (accessed on 12 August 2022).


{kind=link}
| Items | SPICE-R2 | SPICE-R2F |
|---|---|---|
| Factor 1 | ||
| Q1 | Working with students from different disciplines enhances my education. | Travailler avec des étudiants d’autres filières améliore ma formation. |
| Q4 | Participating in educational experiences with students from different disciplines enhances my ability to work on an interprofessional team. | Participer à des expériences éducatives avec des étudiants issus d’autres formations améliore ma capacité future à travailler avec une équipe interprofessionnelle. |
| Q7 | Health professional students from different disciplines should be educated to establish collaborative relationships with one another. | Les étudiants des professions de santé venant de différentes disciplines devraient être formés pour établir des relations de collaboration les uns avec les autres. |
| Q10 | During their education, health professional students should be involved in teamwork with students from different disciplines in order to understand their respective roles. | Au cours de leur formation, les étudiants des professions de santé devraient être Impliqués dans du travail en équipe avec des étudiants venant de différentes disciplines afin de comprendre leurs rôles respectifs. |
| Factor 2 | ||
| Q2 | My role within an interprofessional team is clearly defined. | Mon rôle au sein d’une équipe interprofessionnelle est clairement défini. |
| Q5 | I have an understanding of the courses taken by, and training requirements of, other health professionals. | J’ai une compréhension des cours suivis par les autres professionnels de santé, ainsi que des exigences de leurs formations. |
| Q8 | I understand the roles of other health professionals within an interprofessional team. | Je comprends le rôle des autres professionnels au sein d’une équipe interprofessionnelle. |
| Factor 3 | ||
| Q3 | Patient/client satisfaction is improved when care is delivered by an interprofessional team. | La satisfaction des patients est améliorée quand ils/elles reçoivent des soins dispensés par une équipe interprofessionnelle. |
| Q6 | Health-care costs are reduced when patients/clients are treated by an interprofessional team. | Les coûts des soins de santé sont réduits quand les patients reçoivent des soins par une équipe interprofessionnelle. |
| Q9 | Patient/client-centeredness increases when care is delivered by an interprofessional team. | La place centrale du patient dans le soin est renforcée quand il est dispensé par une équipe interprofessionnelle. |
| Data Type | Number of Participants (%) |
|---|---|
| Curriculum | |
| Pharmacy | 617 (69) |
| Medicine | 284 (31) |
| University | |
| Montpellier | 583 (65) |
| Paris | 195 (22) |
| Strasbourg | 101 (11) |
| Bordeaux | 22 (2) |
| Year of study | |
| 4 | 252 (28) |
| 5 | 227 (25) |
| 3 | 188 (21) |
| 2 | 129 (14) |
| 6 | 105 (12) |
| N | RMSEA | CFI | SRMR | |
|---|---|---|---|---|
| Total | 901 | 0.038 (95% CI: 0.027-0.050) | 0.976 | 0.040 |
| Pharmacy | 617 | 0.037 (95% CI: 0.022-0.052) | 0.973 | 0.046 |
| Medicine | 284 | 0.0046 (95% CI: 0.020-0.069) | 0.967 | 0.060 |
| Factor 1 | Factor 2 | Factor 3 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | Standard Deviation | Mean | Standard Deviation | Mean | Standard Deviation | Mean | Standard Deviation | |
| Combined | 901 | 17.8 | 2.1 | 10.5 | 2.0 | 12.2 | 1.7 | 40.5 | 3.9 |
| Pharmacy | 617 | 18.0 | 3.7 | 10.7 | 1.9 | 12.4 | 1.7 | 41.2 | 3.7 |
| Medicine | 284 | 17.2 | 2.2 | 9.8 | 2.1 | 11.8 | 1.6 | 38.8 | 3.8 |
| Item | Estimation | Standard Deviation | p-Value | |
|---|---|---|---|---|
| Factor 1 | Q1 | 0.555 | 0.033 | <0.0001 |
| Q4 | 0.706 | 0.028 | <0.0001 | |
| Q7 | 0.553 | 0.028 | <0.0001 | |
| Q10 | 0.746 | 0.027 | <0.0001 | |
| Factor 2 | Q2 | 0.379 | 0.047 | <0.0001 |
| Q5 | 0.526 | 0.045 | <0.0001 | |
| Q8 | 0.648 | 0.056 | <0.0001 | |
| Factor 3 | Q3 | 0.538 | 0.040 | <0.0001 |
| Q6 | 0.419 | 0.041 | <0.0001 | |
| Q9 | 0.754 | 0.043 | <0.0001 |
| Item | Estimation | Standard Deviation | p-Value | |
|---|---|---|---|---|
| Factor 1 | Q1 | 0.571 | 0.039 | <0.0001 |
| Q4 | 0.662 | 0.038 | <0.0001 | |
| Q7 | 0.478 | 0.039 | <0.0001 | |
| Q10 | 0.751 | 0.039 | <0.0001 | |
| Factor 2 | Q2 | 0.354 | 0.055 | <0.0001 |
| Q5 | 0.508 | 0.053 | <0.0001 | |
| Q8 | 0.667 | 0.072 | <0.0001 | |
| Factor 3 | Q3 | 0.574 | 0.052 | <0.0001 |
| Q6 | 0.442 | 0.049 | <0.0001 | |
| Q9 | 0.783 | 0.053 | <0.0001 |
| Item | Estimation | Standard Deviation | p-Value | |
|---|---|---|---|---|
| Factor 1 | Q1 | 0.533 | 0.058 | <0.0001 |
| Q4 | 0.747 | 0.043 | <0.0001 | |
| Q7 | 0.620 | 0.042 | <0.0001 | |
| Q10 | 0.733 | 0.037 | <0.0001 | |
| Factor 2 | Q2 | 0.364 | 0.088 | <0.0001 |
| Q5 | 0.410 | 0.087 | <0.0001 | |
| Q8 | 0.788 | 0.141 | <0.0001 | |
| Factor 3 | Q3 | 0.426 | 0.065 | <0.0001 |
| Q6 | 0.360 | 0.079 | <0.0001 | |
| Q9 | 0.614 | 0.081 | <0.0001 |
| N | Alpha Coefficient | |
|---|---|---|
| Total | 901 | 0.6 (total) 0.66 (factor 1) 0.45 (factor 2) 0.48 (factor 3) |
| Pharmacy | 617 | 0.58 (total) 0.62 (factor 1) 0.44 (factor 2) 0.51 (factor 3) |
| Medecine | 284 | 0.55 (total) 0.7 (factor 1) 0.43 (factor 2) 0.37 (factor 3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piogé, A.; Zorek, J.; Eickhoff, J.; Debien, B.; Finkel, J.; Trouillard, A.; Poucheret, P. Interprofessional Collaborative Clinical Practice in Medicine and Pharmacy: Measure of Student Perceptions Using the SPICE-R2F Instrument to Bridge Health-Care Policy and Education in France. Healthcare 2022, 10, 1531. https://doi.org/10.3390/healthcare10081531
Piogé A, Zorek J, Eickhoff J, Debien B, Finkel J, Trouillard A, Poucheret P. Interprofessional Collaborative Clinical Practice in Medicine and Pharmacy: Measure of Student Perceptions Using the SPICE-R2F Instrument to Bridge Health-Care Policy and Education in France. Healthcare. 2022; 10(8):1531. https://doi.org/10.3390/healthcare10081531
Chicago/Turabian StylePiogé, Alexandre, Joseph Zorek, Jens Eickhoff, Blaise Debien, Julie Finkel, Alexandre Trouillard, and Patrick Poucheret. 2022. "Interprofessional Collaborative Clinical Practice in Medicine and Pharmacy: Measure of Student Perceptions Using the SPICE-R2F Instrument to Bridge Health-Care Policy and Education in France" Healthcare 10, no. 8: 1531. https://doi.org/10.3390/healthcare10081531
APA StylePiogé, A., Zorek, J., Eickhoff, J., Debien, B., Finkel, J., Trouillard, A., & Poucheret, P. (2022). Interprofessional Collaborative Clinical Practice in Medicine and Pharmacy: Measure of Student Perceptions Using the SPICE-R2F Instrument to Bridge Health-Care Policy and Education in France. Healthcare, 10(8), 1531. https://doi.org/10.3390/healthcare10081531