
Non-Motherhood between Obligation and Choice: Statistical Analysis Based on Permutation Tests of Spontaneous and Induced Abortion Rates in the Italian Context

 ,
,  , and
, and
Abstract
:1. Introduction
1.1. Spontaneous Abortion: Generalities
- -
- complete: when the product of conception is totally expelled;
- -
- incomplete: when the fetus is partially expelled;
- -
- internal: when the fetus is not viable and remains in the uterine cavity;
- -
- early: if it occurs before the twelfth week of gestation;
- -
- late: when it occurs between the twelfth and twentieth week of gestation;
- -
- recurrent: when two or more consecutive spontaneous abortions occur.
1.2. Induced Abortion: Generalities
1.3. Abortion as Trauma: Psychological Consequences
1.4. Scientific Background
2. Materials and Methods
2.1. NPC: Methodological Issue
- -
- property of similarity: whatever the distribution of the data, the probability of rejecting the null hypothesis is invariant with respect to the set of actually observed data, whatever the method of disclosure of the data;
- -
- for any α significance level, for any distribution and for all possible observed datasets, if under the alternative, the distribution dominates the null hypothesis, and then there exists an undistorted conditional test, such that the probability to reject the null hypothesis is always lower than the α significance level.
- -
- the assumptions of normality and homoscedasticity are not required [36];
- -
- the analyzed variables can be of any nature (nominal, ordinal, and numerical);
- -
- it can be applied even when there are missing data [37];
- -
- it guarantees statistical power even in presence of low sampling size [38];
- -
- -
- it offers the possibility of stratified analyses with respect to a confounding factor [41];
- -
- it allows to verify restricted alternative hypotheses (stochastic ordering) [35];
- -
- it can be applied even when the number of observed subjects is smaller than the number of variables [42].
- -
- the first phase foresees the decomposition of the multivariate hypothesis system into one-dimensional sub-hypothesis, for each of which there is a partial permutation test. This allows examining the marginal contribution of each individual response variable in the comparison between the groups [43];
- -
- the second phase foresees the non-parametric combination of partial tests in a single second-order test related to the multivariate global hypothesis [44].
2.2. The Data
3. Results
3.1. Comparison among Italian Macro-Areas, Stratifying for Year
3.2. Comparison among Italian Macro-Areas, Stratifying for Age Classes
3.3. Stochastic Ordering: Evaluation of a Monotone Decreasing Trend over Years, Stratifying for Italian Macro-Areas
4. Discussion
5. Conclusions
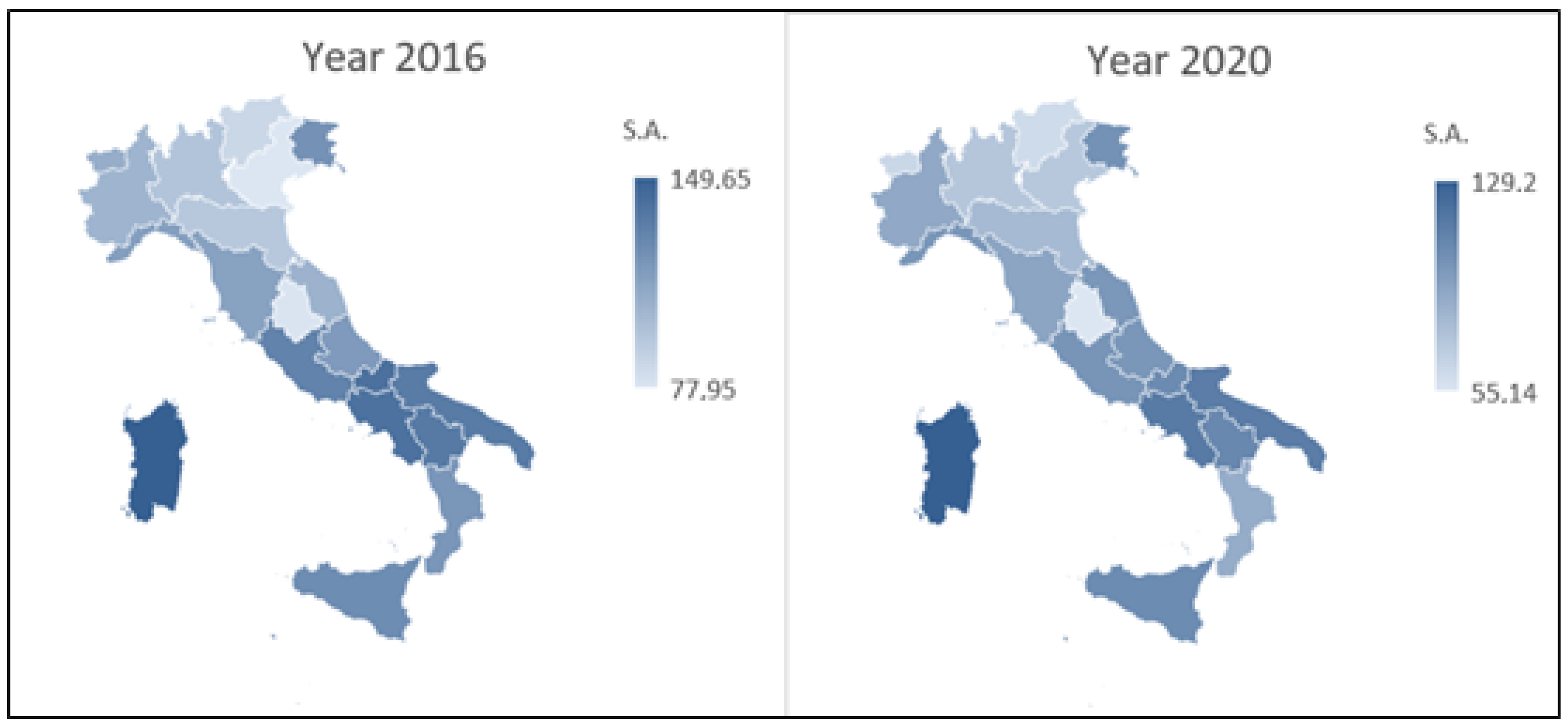
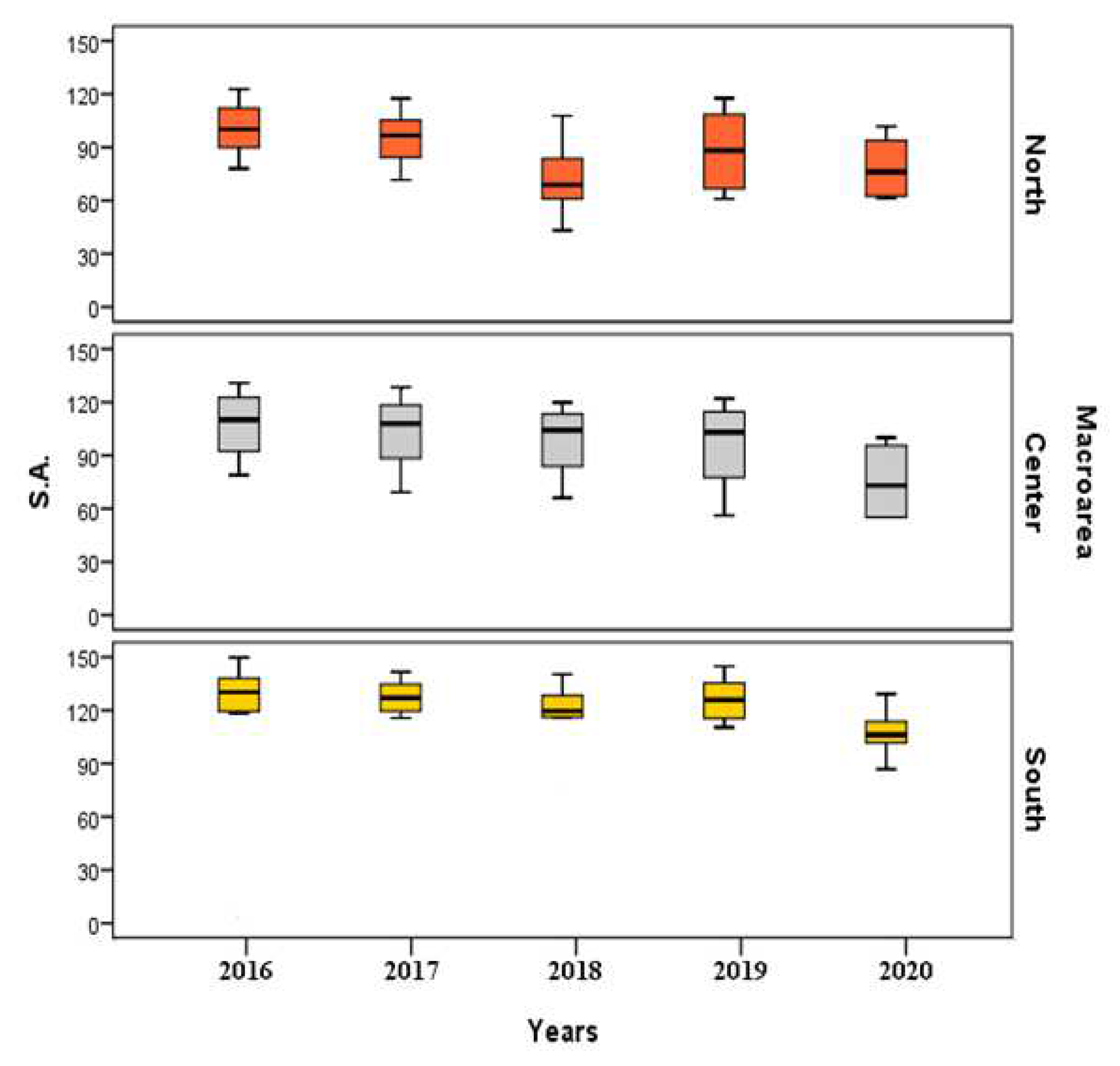
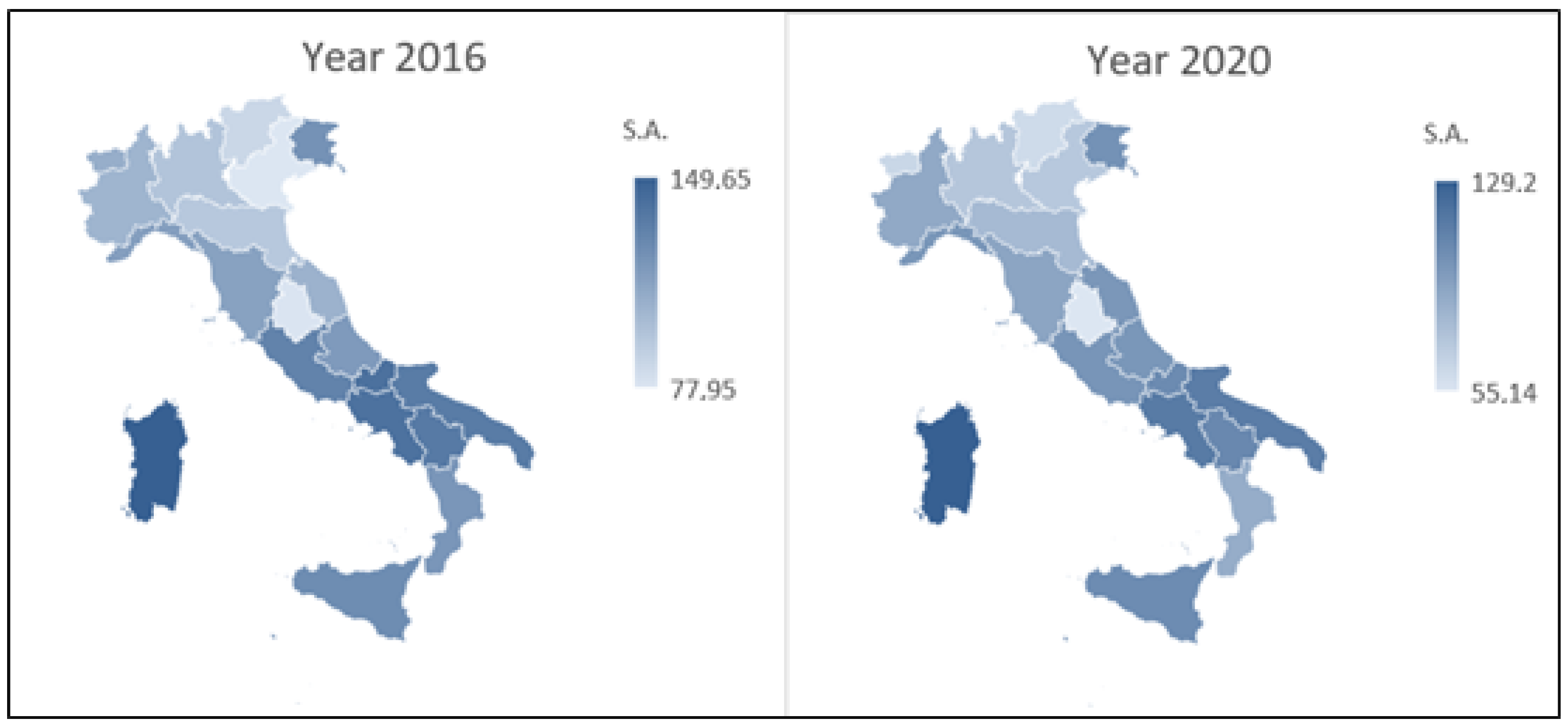
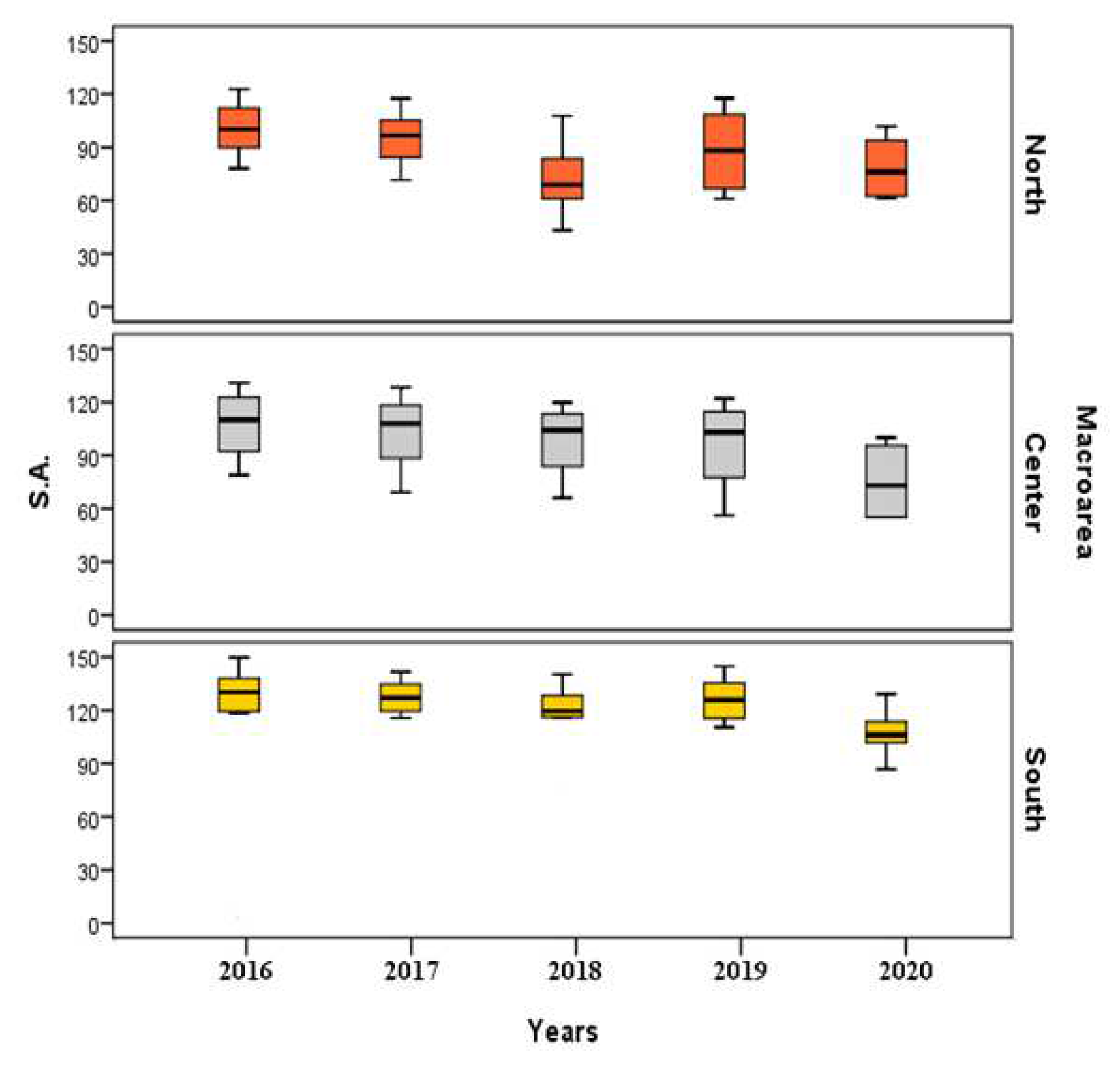
- only for SA, there are significant differences among the three territorial divisions from 2017 onwards; on the other hand, the rates of IA are similar in the three macro-areas of Italian territory for each examined year. From the pairwise comparisons performed for only SA, in all the examined years, standardized rates of SA in North and Center are similar; South, recording higher SA standardized rates, significantly differs from North and Center both globally and for the specific years 2017 and 2019 too. In relation to the year 2020, the significance is recorded only in the North versus South comparison since the Center versus South comparison is not significant, denoting a similarity condition;
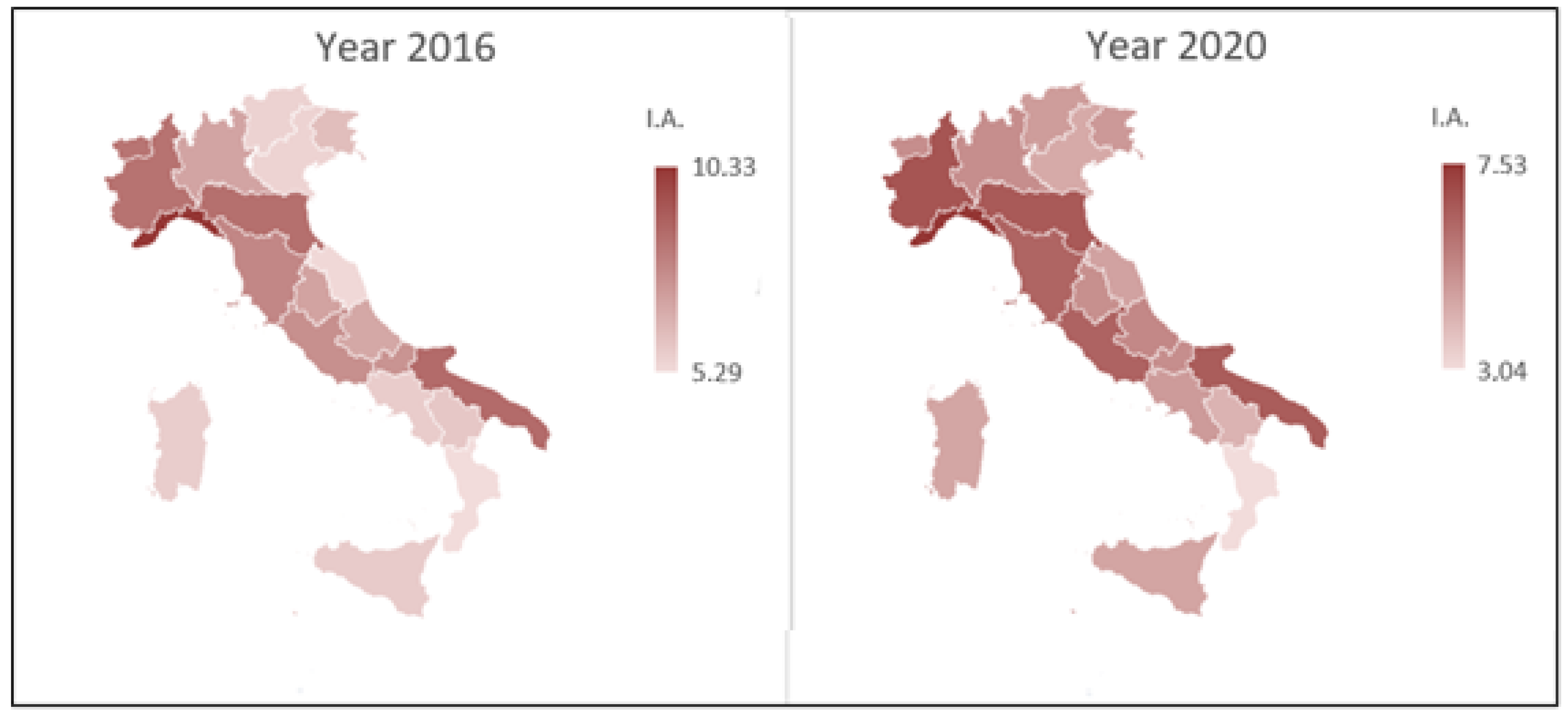
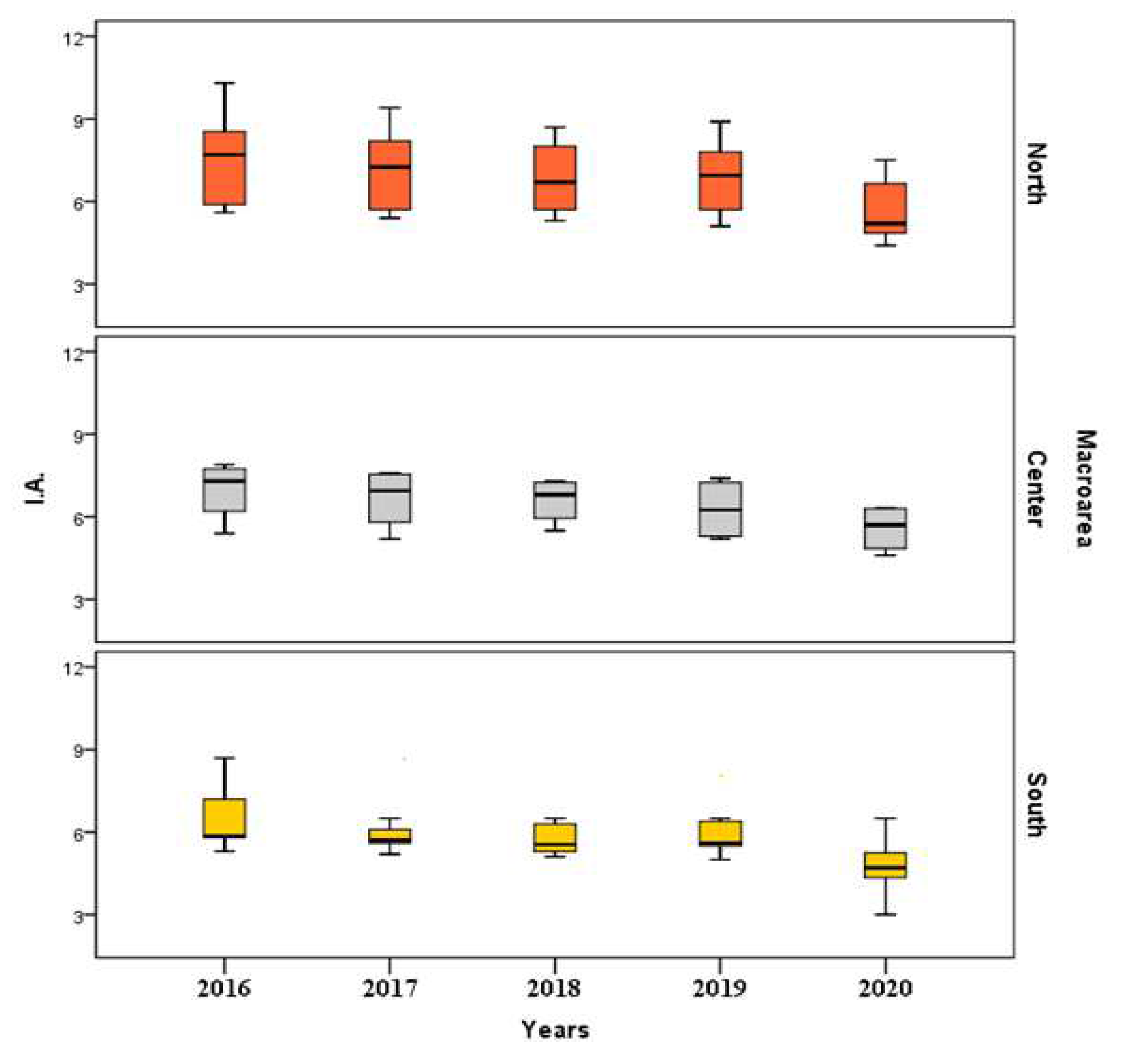
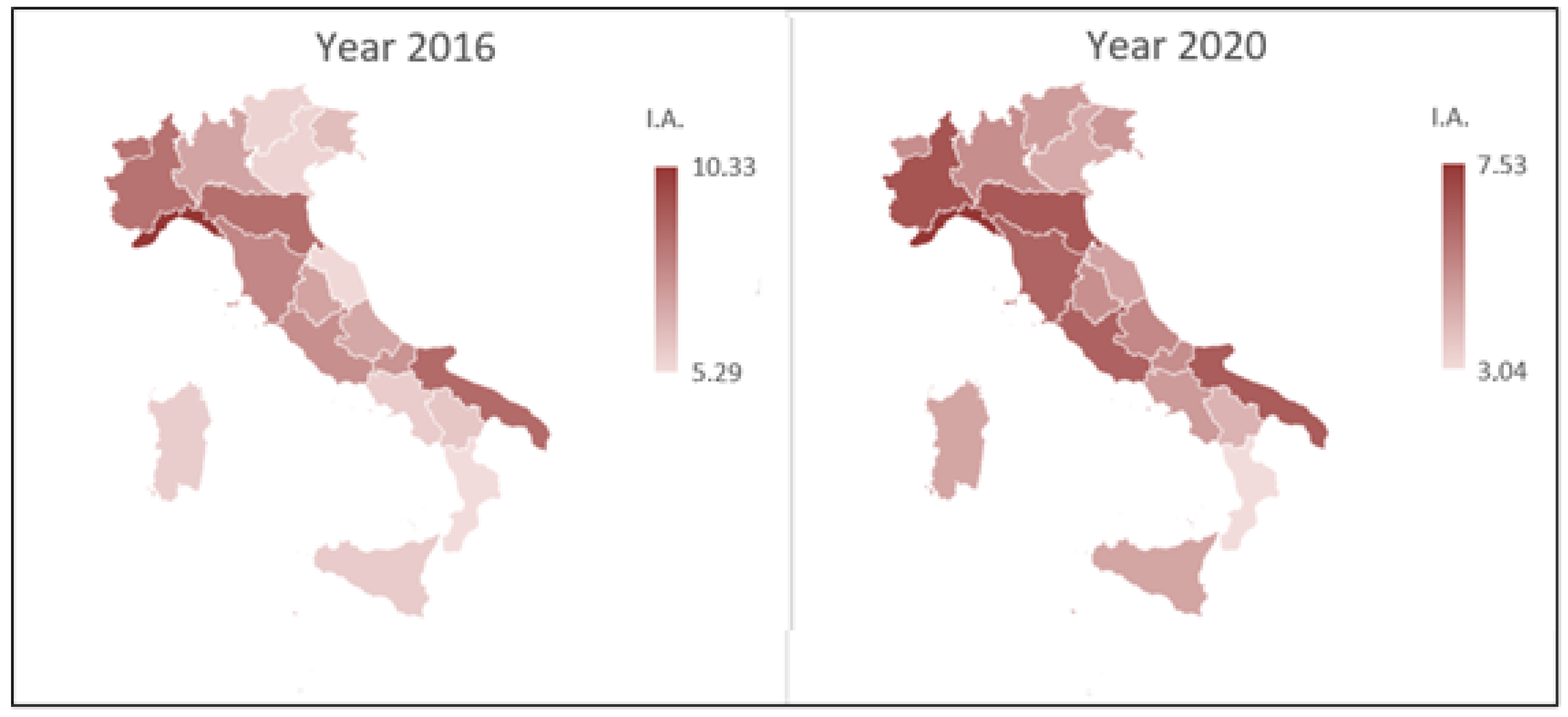
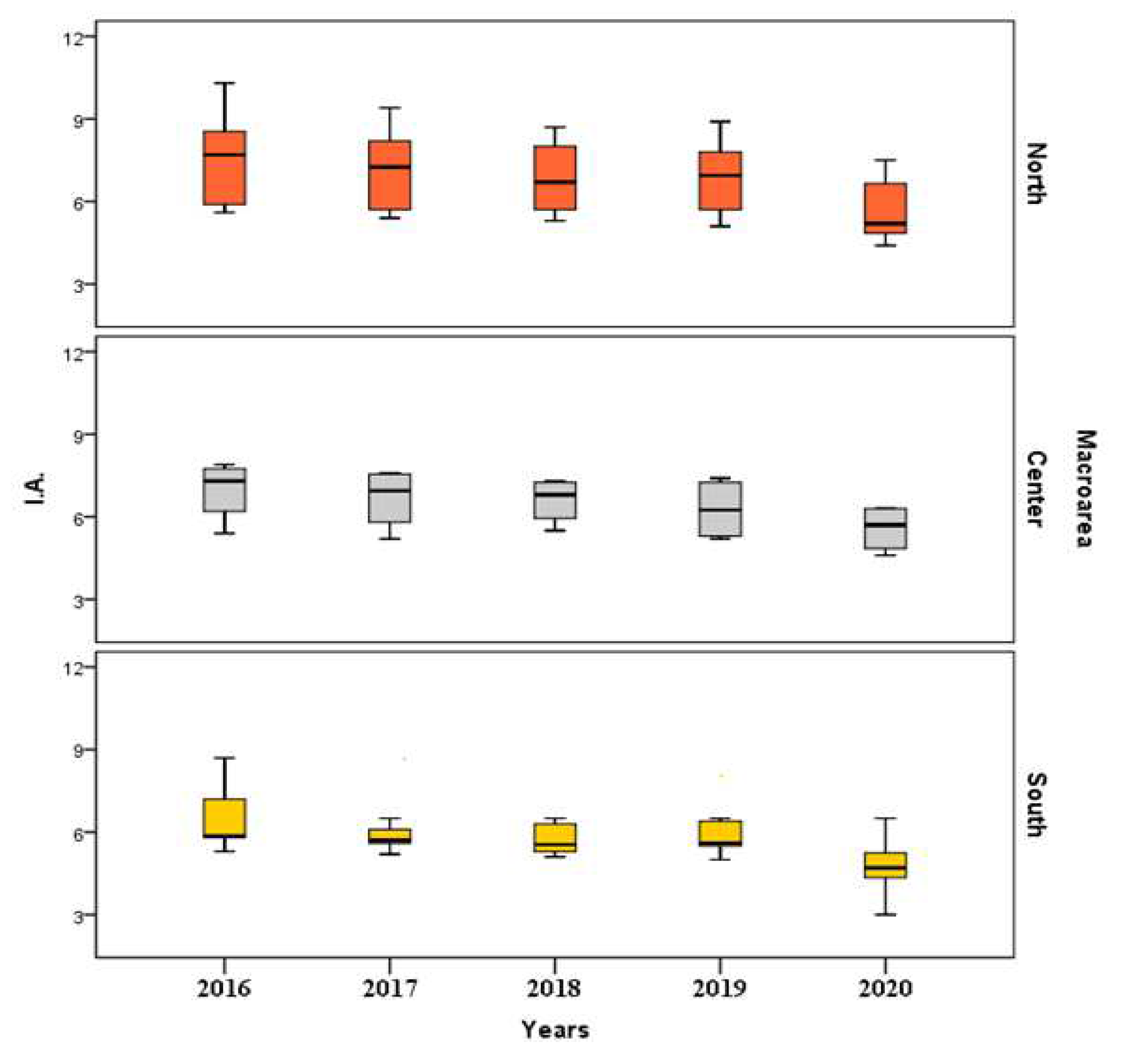
- the SA standardized rates, referring to the distinct age classes, do not show significant differences among the three analyzed geographical areas; different results are highlighted, however, in relation to IA, denoting significant differences among the three territorial macro-areas. We note, in fact, an evident significance referring to classes from 20 to 24 and 40 to 44 years of age. Two-by-two comparisons, which allowed to verify restricted alternative hypotheses, highlighted, for IA, a similarity condition between North and Center and a statistical significance in the comparison of North versus South and Center versus South, both globally and in the single age groups; in fact, the restricted alternative hypothesis, according to which North and Center have higher IA standardized rates compared to South, is verified with reference to classes from 20 to 24 and 40 to 44 years;
- the trend of SA rates is not characterized by a stochastic ordering that decreases over the years. More interesting results, on the other hand, are highlighted in relation to IA standardized rates: throughout the Italian territory, IA standardized rates are characterized by a significant monotonous decreasing trend over the years.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reardon, D.C. The abortion and mental health controversy: A comprehensive literature review of common ground agreements, disagreements, actionable recommendations, and research opportunities. SAGE Open Med. 2018, 6, 2050312118807624. [Google Scholar] [CrossRef]
- Séjourné, N.; Callahan, S.; Chabrol, H. The utility of a psychological intervention for coping with spontaneous abortion. J. Reprod. Infant Psychol. 2010, 28, 287–296. [Google Scholar] [CrossRef]
- Nguyen, B.T.; Hebert, L.E.; Newton, S.L.; Gilliam, M.L. Supporting Women at the Time of Abortion: A Mixed-Methods Study of Male Partner Experiences and Perspectives. Perspect. Sex. Reprod. Health 2018, 50, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Osborn, J.F.; Cattaruzza, M.S.; Spinelli, A. Risk of spontaneous abortion in Italy, 1978–1995, and the effect of maternal age, gravidity, marital status, and education. Am. J. Epidemiol. 2000, 151, 98–105. [Google Scholar] [CrossRef]
- Fretts, R.C.; Schmittdiel, J.; McLean, F.H.; Usher, R.H.; Goldman, M.B. Increased maternal age and the risk of fetal death. N. Engl. J. Med. 1995, 333, 953–957. [Google Scholar] [CrossRef]
- Nybo Andersen, A.M.; Wohlfahrt, J.; Christens, P.; Olsen, J.; Melbye, M. Maternal age and fetal loss: Population based register linkage study. Br. Med. J. 2000, 320, 1708–1712. [Google Scholar] [CrossRef]
- Zheng, D.; Li, C.; Wu, T.; Tang, K. Factors associated with spontaneous abortion: A cross-sectional study of Chinese populations. Reprod. Health 2017, 14, 33. [Google Scholar] [CrossRef]
- Fan, X.; Wang, W.; Liu, R.; Dang, S.; Kang, Y. Epidemiological features and risk factors of spontaneous abortion among rural Tibetan women at childbearing age. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 401–405. [Google Scholar]
- Yassin, K.M. Incidence and socioeconomic determinants of abortion in rural upper Egypt. Public Health 2000, 114, 269–272. [Google Scholar] [CrossRef]
- Baba, S.; Noda, H.; Nakayama, M.; Waguri, M.; Mitsuda, N.; Iso, H. Risk factors of early spontaneous abortions among Japanese: A matched case-control study. Hum. Reprod. 2011, 26, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Norsker, F.; Espenhain, L.; Rogvi, S.; Morgen, C.S.; Andersen, P.K.; Andersen, A.-M.N. Socioeconomic position and the risk of spontaneous abortion: A study within the Danish National Birth Cohort. Br. Med. J. 2012, 2, e001077. [Google Scholar] [CrossRef]
- Adjei, G.; Enuameh, Y.; Asante, K.P. Predictors of abortions in Rural Ghana: A cross-sectional study. BMC Public Health 2015, 15, 202. [Google Scholar] [CrossRef]
- Grippo, A.; Zhang, J.; Chu, L.; Guo, Y.; Qiao, L.; Myneni, A.A.; Mu, L. Air pollution exposure during pregnancy and spontaneous abortion and stillbirth. Rev. Environ. Health 2018, 33, 247–264. [Google Scholar] [CrossRef] [PubMed]
- Hyland, A.; Piazza, K.M.; Hovey, K.M.; Ockene, J.K.; Andrews, C.A.; Rivard, C.; Wactawski-Wende, J. Associations of lifetime active and passive smoking with spontaneous abortion, stillbirth and tubal ectopic pregnancy: A cross-sectional analysis of historical data from the Women’s Health Initiative. Tob. Control 2015, 24, 328–335. [Google Scholar] [CrossRef]
- Oliveira, L.A.; El Dib, R.P.; Figueiredo, D.B.S.; Braz, L.G.; Braz, M.G. Spontaneous abortion in women occupationally exposed to inhalational anesthetics: A critical systematic review. Environ. Sci. Pollut. Res. 2021, 28, 10436–10449. [Google Scholar] [CrossRef]
- Kim, H.; Kwon, H.-J.; Rhie, J.; Lim, S.; Kang, Y.-D.; Eom, S.-Y.; Lim, H.; Myong, J.-P.; Roh, S. The relationship between spontaneous abortion and female workers in the semiconductor industry. Ann. Occup. Environ. Med. 2017, 29, 49. [Google Scholar] [CrossRef]
- Kumar, S. Occupational, environmental and lifestyle factors associated with spontaneous abortion. Reprod. Sci. 2011, 18, 915–930. [Google Scholar] [CrossRef]
- Shirangi, A.; Fritschi, L.; Holman, C.D.J. Associations of unscavenged anesthetic gases and long working hours with preterm delivery in female veterinarians. Obstet. Gynecol. 2009, 113, 1008–1017. [Google Scholar] [CrossRef]
- Boivin, J.F. Risk of spontaneous abortion in women occupationally exposed to anaesthetic gases: A meta-analysis. Occup. Environ. Med. 1997, 54, 541–548. [Google Scholar] [CrossRef]
- Lindbohm, M.-L.; Taskinen, H. Spontaneous abortions among veterinarians. Scand. J. Work. Environ. Health 2000, 26, 501–506. [Google Scholar] [CrossRef]
- Munk-Olsen, T.; Laursen, T.M.; Pedersen, C.B.; Lidegaard, Ø.; Mortensen, P.B. Induced first-trimester abortion and risk of mental disorder. N. Engl. J. Med. 2011, 364, 332–339. [Google Scholar] [CrossRef]
- Anselmi, N.; D’aloise, A.; Di Febo, R.; Pezzuti, L.; Leone, C. Psychological implications of abortion: A longitudinal study on two cohorts of women who recur to elective and therapeutic abortion. Riv. Psichiatr. 2018, 53, 324–330. [Google Scholar] [CrossRef]
- Coleman, P.K.; Rue, V.M.; Coyle, C.T. Induced abortion and intimate relationship quality in the Chicago Health and Social Life Survey. Public Health 2009, 123, 331–338. [Google Scholar] [CrossRef]
- Chae, S.; Desai, S.; Crowell, M.; Sedgh, G. Reasons why women have induced abortions: A synthesis of findings from 14 countries. Contraception 2017, 96, 233–241. [Google Scholar] [CrossRef]
- Megersa, B.S.; Ojengbede, O.A.; Deckert, A.; Fawole, O.I. Factors associated with induced abortion among women of reproductive age attending selected health facilities in Addis Ababa, Ethiopia: A case control study. BMC Women’s Health 2020, 20, 188. [Google Scholar] [CrossRef]
- Niinimäki, M.; Suhonen, S.; Mentula, M.; Hemminki, E.; Heikinheimo, O.; Gissler, M. Comparison of rates of adverse events in adolescent and adult women undergoing medical abortion: Population register based study. Br. Med. J. 2011, 342, d2111. [Google Scholar] [CrossRef]
- Carlsson, I.; Breding, K.; Larsson, P.G. Complications related to induced abortion: A combined retrospective and longitudinal follow-up study. BMC Women’s Health 2018, 18, 158. [Google Scholar] [CrossRef]
- Bankole, A.; Singh, S.; Haas, T. Reasons Why Women Have Induced Abortions: Evidence from 27 Countries. Int. Perspect. Sex. Reprod. Health 1998, 24, 117. [Google Scholar] [CrossRef]
- Pesarin, F. Permutation Testing of Multidimensional Hypotheses; Cleup Editrice: Padova, Italy, 1997. [Google Scholar]
- Pesarin, F. Multivariate Permutation Tests, with Applications in Biostatistics; Wiley: Hoboken, NJ, USA, 2001. [Google Scholar]
- Pesarin, F.; Salmaso, L. Permutation Tests for Complex Data: Theory, Applications and Software; John Wiley & Sons: New York, NY, USA, 2010. [Google Scholar]
- Pesarin, F. Extending permutation conditional inference to unconditional ones. Stat. Methods Appl. 2002, 11, 161–173. [Google Scholar] [CrossRef]
- Ludbrook, J.; Dudley, H. Why Permutation Tests are Superior to t and F Tests in Biomedical Research. Am. Stat. 1998, 52, 127–132. [Google Scholar] [CrossRef]
- Lehmann, E.L.; Romano, J.P. Testing Statistical Hypotheses; Wiley: Hoboken, NJ, USA, 2006. [Google Scholar]
- Arboretti, R.; Ceccato, R.; Salmaso, L. Permutation testing for goodness-of-fit and stochastic ordering with multivariate mixed variables. J. Stat. Comput. Simul. 2020, 91, 876–896. [Google Scholar] [CrossRef]
- Giancristofaro, R.A.; Brombin, C. Overview of Non-Parametric Combination-based permutation tests for Multivariate multi-sample problems. Statistica 2014, 74, 233–246. [Google Scholar] [CrossRef]
- Arboretti, R.; Bathke, A.C.; Carrozzo, E.; Pesarin, F.; Salmaso, L. Multivariate permutation tests for two sample testing in presence of nondetects with application to microarray data. Stat. Methods Med. Res. 2019, 29, 258–271. [Google Scholar] [CrossRef]
- Brombin, C.; Salmaso, L. Multi-aspect permutation tests in shape analysis with small sample size. Comput. Stat. Data Anal. 2009, 53, 3921–3931. [Google Scholar] [CrossRef]
- Bonnini, S.; Corain, L.; Marozzi, M.; Salmaso, L. Nonparametric Hypothesis Testing: Rank and Permutation Methods with Applications in R; John Wiley & Sons: New York, NY, USA, 2014. [Google Scholar]
- Corain, L.; Salmaso, L. Improving power of multivariate combination-based permutation tests. Stat. Comput. 2013, 25, 203–214. [Google Scholar] [CrossRef]
- Corain, L.; Salmaso, L. Multivariate and multistrata nonparametric tests: The nonparametric combination method. J. Mod. Appl. Stat. Methods 2004, 3, 443–461. [Google Scholar] [CrossRef]
- Finos, L.; Salmaso, L. Weighted methods controlling the multiplicity when the number of variables is much higher than the number of observations. J. Nonparametric Stat. 2006, 18, 245–261. [Google Scholar] [CrossRef]
- Folks, J.J. Combination of independent tests. Handb. Stat. 1984, 4, 113–121. [Google Scholar]
- Caughey, D.; Dafoe, A.; Seawright, J. Nonparametric combination (NPC): A framework for testing elaborate theories. J. Politics 2017, 79, 688–701. [Google Scholar] [CrossRef]
- Pesarin, F. On a nonparametric combination method for dependent permutation tests with applications. Psychother. Psychosom. 1990, 54, 172–179. [Google Scholar] [CrossRef]
- Pesarin, F. A resampling procedure for nonparametric combination of several dependent tests. Stat. Methods Appl. 1992, 1, 87–101. [Google Scholar] [CrossRef]
- Brombin, C.; Midena, E.; Salmaso, L. Robust non-parametric tests for complex-repeated measures problems in ophthalmology. Stat. Methods Med Res. 2011, 22, 643–660. [Google Scholar] [CrossRef]
- Brombin, C.; Di Serio, M. Evaluating treatment e effect within a multivariate stochastic ordering framework: NPC methodology applied to a study on Multiple Sclerosis. Stat. Methods Med Res. 2012, 25, 366–384. [Google Scholar] [CrossRef]
- Giacalone, M.; Zirilli, A.; Cozzucoli, P.C.; Alibrandi, A. Bonferroni-Holm and permutation tests to compare health data: Methodological and applicative issues. BMC Med. Res. Methodol. 2018, 18, 81. [Google Scholar] [CrossRef]
- Giacalone, M.; Zirilli, A.; Moleti, M.; Alibrandi, A. Does the iodized salt therapy of pregnant mothers increase the children IQ? Empirical evidence of a statistical study based on permutation tests. Qual. Quant. 2017, 52, 1423–1435. [Google Scholar] [CrossRef]
- Zirilli, A.; Alibrandi, A. A permutation solution to compare two hepatocellular carcinoma markers. JP J. Biostat. 2011, 5, 109–119. [Google Scholar]
- Zirilli, A.; Alibrandi, A. The alteration of t,t-muconic acid and s-phenilmercapturic acid levels due to benzene exposure: An application of NPC test. JP J. Biostat. 2012, 7, 91–104. [Google Scholar]
- Arboretti, R.; Fontana, R.; Pesarin, F.; Salmaso, L. Nonparametric combination tests for comparing two survival curves with informative and non-informative censoring. Stat. Methods Med. Res. 2018, 27, 3739–3769. [Google Scholar] [CrossRef]
- Winkler, A.M.; Webster, M.A.; Brooks, J.C.; Tracey, I.; Smith, S.M.; Nichols, T.E. Non-parametric combination and related permutation tests for neuroimaging. Hum. Brain Mapp. 2016, 37, 1486–1511. [Google Scholar] [CrossRef]
- Alfieri, R.; Bonnini, S.; Brombin, C.; Castoro, C.; Salmaso, L. Iterated combination-based paired permutation tests to determine shape effects of chemotherapy in patients with esophageal cancer. Stat. Methods Med Res. 2012, 25, 598–614. [Google Scholar] [CrossRef]
- Nilsson, S.F.; Andersen, P.K.; Strandberg-Larsen, K.; Andersen, A.M.N. Risk factors for miscarriage from a prevention perspective: A nationwide follow-up study. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 1440. [Google Scholar] [CrossRef]
- Ravaldi, C. Assistere la Morte Perinatale: Il Ruolo del Personale Ospedaliero nel Sostegno ai Genitori e ai Familiari in Lutto, CiaoLapo ed.; Officina Grafica Editore: Pisa, Italy, 2018. [Google Scholar]
- Ravaldi, C. Il Sogno Infranto; Officina Grafica Editoriale, Officina Grafica Editore: Pisa, Italy, 2016. [Google Scholar]
- Zaręba, K.; La Rosa, V.L.; Ciebiera, M.; Makara-Studzińska, M.; Gierus, J.; Jakiel, G. Psychosocial Profile and Reproductive Decisions of Women Undergoing Pregnancy Termination for Medical Reasons-A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3413. [Google Scholar] [CrossRef]
- Zaręba, C.; Commodari, E.; La Rosa, V.L.; Makara-Studzińska, M.; Ciebiera, M.; Gierus, J.; Caruso, S.; Jakiel, G. Religiosity among women undergoing pregnancy termination for medical reasons: The experiences and views of Polish women. Eur. J. Contracept. Reprod. Health Care 2020, 25, 381–386. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stratum 1: Year 2016 | Combined | |||
|---|---|---|---|---|
| SA | IA | p-Value | ||
| North | 100.6 ± 15.1 | 7.5 ± 1.7 | ||
| Center | 107.5 ± 21.7 | 6.9 ± 1.1 | ||
| South | 115.6 ± 47.9 | 6.4 ± 1.2 | ||
| ↓ | ↓ | |||
| p-value | 0.689 | 0.335 | → | 0.571 |
| Stratum 2: Year 2017 | ||||
| North | 95.2 ± 15.1 | 7.1 ± 1.5 | ||
| Center | 103.4 ± 24.7 | 6.7 ± 1.1 | ||
| South | 129.2 ± 9.0 | 6.2 ± 1.1 | ||
| ↓ | ↓ | |||
| p-value | 0.001 | 0.330 | → | 0.003 |
| Stratum 3: Year 2018 | ||||
| North | 64.6 ± 32.5 | 6.9 ± 1.3 | ||
| Center | 98.6 ± 23.0 | 6.6 ± 0.8 | ||
| South | 103.9 ± 45.7 | 5.9 ± 0.9 | ||
| ↓ | ↓ | |||
| p-value | 0.044 | 0.224 | → | 0.047 |
| Stratum 4: Year 2019 | ||||
| North | 92.1 ± 21.5 | 6.8 ± 1.0 | ||
| Center | 96.1 ± 28.3 | 6.3 ± 1.14 | ||
| South | 126.0 ± 12.2 | 5.9 ± 0.9 | ||
| ↓ | ↓ | |||
| p-value | 0.005 | 0.333 | → | 0.011 |
| Stratum 5: Year 2020 | ||||
| North | 80.9 ± 16.2 | 5.7 ± 1.1 | ||
| Center | 82.1 ± 23.8 | 5.6 ± 0.9 | ||
| South | 107.4 ± 12.3 | 4.8 ± 1.0 | ||
| ↓ | ↓ | |||
| p-value | 0.006 | 0.202 | → | 0.008 |
| Year | North vs. Center | North vs. South | Center vs. South |
|---|---|---|---|
| 2016 | 0.526 | 0.478 | 0.825 |
| 2017 | 0.485 | 0.004 | 0.014 |
| 2018 | 0.096 | 0.047 | 0.877 |
| 2019 | 0.792 | 0.001 | 0.010 |
| 2020 | 0.906 | 0.003 | 0.025 |
| ↓ | ↓ | ↓ | |
| Combined | 0.876 | 0.001 | 0.011 |
| Age Classes (Years) | SA | IA | ||
|---|---|---|---|---|
| 15–19 | 0.057 | 0.264 | ||
| 20–24 | 0.386 | 0.006 | ||
| 25–29 | 0.598 | 0.001 | ||
| 30–34 | 0.470 | 0.002 | ||
| 35–39 | 0.094 | 0.001 | ||
| 40–44 | 0.058 | 0.007 | ||
| 45–49 | 0.065 | 0.099 | ||
| ↓ | ↓ | |||
| Combined | 0.118 | 0.001 | → | 0.014 |
| Age Classes (Years) | North > Center | North > South | Center > South |
|---|---|---|---|
| 15–19 | 0.665 | 0.137 | 0.129 |
| 20–24 | 0.774 | 0.016 | 0.002 |
| 25–29 | 0.707 | 0.008 | 0.007 |
| 30–34 | 0.719 | 0.006 | 0.006 |
| 35–39 | 0.058 | 0.007 | 0.008 |
| 40–44 | 0.041 | 0.016 | 0.009 |
| 45–49 | 0.055 | 0.250 | 0.231 |
| ↓ | ↓ | ↓ | |
| Combined | 0.091 | 0.001 | 0.001 |
| Italian | 2016 > 2017 | 2017 > 2018 | 2018 > 2019 | 2019 > 2020 | Combined | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Macro-Areas | SA | IA | SA | IA | SA | IA | SA | IA | SA | IA |
| North | 0.237 | 0.031 | 0.038 | 0.034 | 0.267 | 0.985 | 0.294 | 0.036 | 0.334 | 0.029 |
| Center | 0.381 | 0.048 | 0.346 | 0.471 | 0.852 | 0.047 | 0.285 | 0.033 | 0.140 | 0.014 |
| South | 0.289 | 0.042 | 0.059 | 0.029 | 0.217 | 0.847 | 0.054 | 0.010 | 0.449 | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alibrandi, A.; Merlino, L.; Guarneri, C.; Ingrasciotta, Y.; Zirilli, A. Non-Motherhood between Obligation and Choice: Statistical Analysis Based on Permutation Tests of Spontaneous and Induced Abortion Rates in the Italian Context. Healthcare 2022, 10, 1514. https://doi.org/10.3390/healthcare10081514
Alibrandi A, Merlino L, Guarneri C, Ingrasciotta Y, Zirilli A. Non-Motherhood between Obligation and Choice: Statistical Analysis Based on Permutation Tests of Spontaneous and Induced Abortion Rates in the Italian Context. Healthcare. 2022; 10(8):1514. https://doi.org/10.3390/healthcare10081514
Chicago/Turabian StyleAlibrandi, Angela, Lavinia Merlino, Claudio Guarneri, Ylenia Ingrasciotta, and Agata Zirilli. 2022. "Non-Motherhood between Obligation and Choice: Statistical Analysis Based on Permutation Tests of Spontaneous and Induced Abortion Rates in the Italian Context" Healthcare 10, no. 8: 1514. https://doi.org/10.3390/healthcare10081514
APA StyleAlibrandi, A., Merlino, L., Guarneri, C., Ingrasciotta, Y., & Zirilli, A. (2022). Non-Motherhood between Obligation and Choice: Statistical Analysis Based on Permutation Tests of Spontaneous and Induced Abortion Rates in the Italian Context. Healthcare, 10(8), 1514. https://doi.org/10.3390/healthcare10081514