
The Effect of a Resistance Training, Detraining and Retraining Cycle on Postural Stability and Estimated Fall Risk in Institutionalized Older Persons: A 40-Week Intervention

 ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Postural Stability and Fall Risk Assessment
2.2. Muscular Strength Exercise Protocol
2.3. Anthropometric Assessment
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Regional Office for Europe. World Health Statistics. 2018. Available online: https://www.euro.who.int/en/data-and-evidence/european-health-report/european-health-report-2018 (accessed on 22 July 2021).
- Macklai, N.S.; Spagnoli, J.; Junod, J.; Santos-Eggimann, B. Prospective association of the SHARE-operationalized frailty phenotype with adverse health outcomes: Evidence from 60+ community-dwelling Europeans living in 11 countries. BMC Geriatr. 2013, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Salini, S.; Sisto, A.; Picca, A.; et al. Sarcopenia: An overview on current definitions, diagnosis and treatment. Curr. Protein Pept. Sci. 2018, 19, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Rapp, K.; Becker, C.; Cameron, I.D.; König, H.-H.; Büchele, G. Epidemiology of falls in residential aged care: Analysis of more than 70,000 falls from residents of Bavarian nursing homes. J. Am. Med Dir. Assoc. 2012, 13, 187.e1–187.e6. [Google Scholar] [CrossRef]
- Nnodim, J.O. Balance and its Clinical Assessment in Older Adults-A Review. J. Geriatr. Med. Gerontol. 2015, 1, 3. [Google Scholar] [CrossRef]
- MacKinnon, C.D. Sensorimotor anatomy of gait, balance, and falls. Handb. Clin. Neurol. 2018, 159, 3–26. [Google Scholar] [CrossRef]
- Maidan, I.; Droby, A.; Jacob, Y.; Giladi, N.; Hausdorff, J.M.; Mirelman, A. The neural correlates of falls: Alterations in large-scale resting-state networks in elderly fallers. Gait Posture 2020, 80, 56–61. [Google Scholar] [CrossRef]
- Almeida, R.; Abreu, C.; Mendes, A. Quedas em doentes hospitalizados: Contributos para uma prática baseada na prevenção. Rev. Enferm. Ref. 2010, 3, 163–172. [Google Scholar] [CrossRef]
- De Menezes, R.L.; Bachion, M.M. Estudo da presença de fatores de riscos intrínsecos para quedas, em idosos institucionalizados. Cien. Saude Colet. 2008, 13, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and fall injuries among adults aged ≥65 years—United States, 2014. Morb. Mortal. Wkly Rep. 2016, 65, 938–983. [Google Scholar] [CrossRef] [PubMed]
- Center of Disease Control and Prevention. Behavioral Risk Factor Surveillance System, LLCP 2020 Codebook Report. 2021. Available online: https://www.cdc.gov/brfss/annual_data/2020/pdf/codebook20_llcp-v2-508.pdf (accessed on 8 March 2022).
- Center of Disease Control and Prevention. Fact About Falls. 2021. Available online: https://www.cdc.gov/falls/facts.html (accessed on 11 March 2022).
- Center of Disease Control and Prevention. Older Adult Fall Prevention. 2019. Available online: https://www.cdc.gov/falls/ (accessed on 13 March 2022).
- Haagsma, J.A.; Olij, B.F.; Majdan, M.; Van Beeck, E.F.; Vos, T.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; et al. Falls in older aged adults in 22 European countries: Incidence, mortality and burden of disease from 1990 to 2017. Inj. Prev. 2020, 26 (Suppl. S1), i67–i74. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabil. 2015, 39, 1897–1908. [Google Scholar] [CrossRef]
- Cuevas-Trisan, R. Balance Problems and Fall Risks in the Elderly Balance Falls Older adults Risk factors. Clin. Geriatr. Med. 2019, 35, 173–183. Available online: https://www.tandfonline.com/doi/full/10.1080/09638288.2016.1212282 (accessed on 13 November 2020). [CrossRef] [PubMed]
- Gotzmeister, D.; Zecevic, A.A.; Klinger, L.; Salmoni, A. People are Getting Lost a Little Bit: Systemic Factors that Contribute to Falls in Community-Dwelling Octogenarians. Can. J. Aging 2015, 34, 397–410. [Google Scholar] [CrossRef]
- Åhlund, K.; Ekerstad, N.; Bäck, M.; Karlson, B.W.; Öberg, B. Preserved physical fitness is associated with lower 1-year mortality in frail elderly patients with a severe comorbidity burden. Clin. Interv. Aging 2019, 14, 577–586. Available online: https://www.dovepress.com/preserved-physical-fitness-is-associated-with-lower-1-year-mortality-i-peer-reviewed-article-CIA (accessed on 26 November 2021). [CrossRef]
- García-Molina, R.; Ruíz-Grao, M.C.; Noguerón-García, A.; Martínez-Reig, M.; Esbrí-Víctor, M.; Izquierdo, M.; Abizanda, P. Benefits of a multicomponent Falls Unit-based exercise program in older adults with falls in real life. Exp. Gerontol. 2018, 110, 79–85. [Google Scholar] [CrossRef]
- Chupel, M.U.; Direito, F.; Furtado, G.E.; Minuzzi, L.G.; Pedrosa, F.M.; Colado, J.C.; Ferreira, J.P.; Filaire, E.; Teixeira, A.M. Strength training decreases inflammation and increases cognition and physical fitness in older women with cognitive impairment. Front. Physiol. 2017, 8, 377. [Google Scholar] [CrossRef]
- Rieping, T.; Furtado, G.E.; Letieri, R.V.; Chupel, M.U.; Colado, J.C.; Hogervorst, E.; Filaire, E.; Teixeira, A.; Ferreira, J.P. Effects of Different Chair-Based Exercises on Salivary Biomarkers and Functional Autonomy in Institutionalized Older Women. Res. Q. Exerc. Sport 2019, 90, 36–45. [Google Scholar] [CrossRef]
- Figliolino, J.A.M.; Morais, T.B.; Berbel, A.M.; Dal Corso, S. Análise da influência do exercício físico em idosos com relação a equilíbrio, marcha e atividade de vida diária. Rev. Bras Geriatr. Gerontol. 2009, 12, 227–238. [Google Scholar] [CrossRef]
- Freiberger, E.; Haeberle, L.; Spirduso, W.W.; Rixt Zijlstra, G.A. Long-term effects of three multicomponent exercise interventions on physical performance and fall-related psychological outcomes in community-dwelling older adults: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Bruton, A.; Navarrete-Villanueva, D.; Pérez-Gómez, J.; Vila-Maldonado, S.; Gesteiro, E.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; Gonzalez-Gross, M.; Casajus, J.A.; et al. The effects of age, organized physical activity and sedentarism on fitness in older adults: An 8-year longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 4312. [Google Scholar] [CrossRef]
- Casas, A.; Izquierdo, M. Physical exercise as an efficient intervention in frail elderly persons physical exercise as an efficient intervention in frail elderly persons [English;Spanish] Ejercicio fisico como intervencion eficaz en el anciano fragil. An. Sist. Sanit. Navar. 2012, 35, 69–85. [Google Scholar]
- Bruininks, B.D.; Hansen, D.; Wikstrom, L.; Korak, J.A. Short-term Multicomponent Exercise: Effective For Addressing Major Variables That Influence Fall Risk In Older Adults. Med. Sci. Sport Exerc. 2020, 52, 736. [Google Scholar] [CrossRef]
- Guo, J.-L.; Tsai, Y.-Y.; Liao, J.-Y.; Tu, H.-M.; Huang, C.-M. Interventions to reduce the number of falls among older adults with/without cognitive impairment: An exploratory meta-analysis. Int. J. Geriatr. Psychiatry 2014, 29, 661–669. [Google Scholar] [CrossRef] [PubMed]
- de Souza Bezerra, E.; Diefenthaeler, F.; Sakugawa, R.L.; Cadore, E.L.; Izquierdo, M.; Moro, A.R.P. Effects of different strength training volumes and subsequent detraining on strength performance in aging adults. J. Bodyw. Mov. Ther. 2019, 23, 466–472. [Google Scholar] [CrossRef]
- Sakugawa, R.L.; Moura, B.M.; Orssatto, L.B.D.R.; Bezerra, E.D.S.; Cadore, E.L.; Diefenthaeler, F. Effects of resistance training, detraining, and retraining on strength and functional capacity in elderly. Aging Clin. Exp. Res. 2019, 31, 31–39. [Google Scholar] [CrossRef]
- Dipietro, L.; Campbell, W.W.; Buchner, D.M.; Erickson, K.I.; Powell, K.E.; Bloodgood, B.; Hughes, T.; Day, K.R.; Piercy, K.L.; Vaux-Bjerke, A.; et al. Physical Activity, Injurious Falls, and Physical Function in Aging: An Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1303–1313. [Google Scholar] [CrossRef]
- Mujika, I.; Padilla, S. Detraining: Loss of Training-Induced Physiological and Performance Adaptations. Part I. Sport Med. 2000, 30, 79–87. [Google Scholar] [CrossRef]
- Albornos-Muñoz, L.; Moreno-Casbas, M.T.; Sánchez-Pablo, C.; Bays-Moneo, A.; Fernández-Domínguez, J.C.; Rich-Ruiz, M.; Gea-Sánchez, M.; the Otago Project Working Group. Efficacy of the Otago Exercise Programme to reduce falls in community-dwelling adults aged 65–80 years old when delivered as group or individual training. J. Adv. Nurs. 2018, 74, 1700–1711. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Ditroilo, M.; Delahunt, E.; De Vito, G. Age Related Changes in Motor Function (II)Decline in Motor Performance Outcomes. Int. J. Sports Med. 2021, 42, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Taani, M.H.; Kovach, C.R.; Buehring, B. Muscle Mechanography: A Novel Method to Measure Muscle Function in Older Adults. Res. Gerontol. Nurs. 2017, 10, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Manini, T.M.; Clark, B.C. Dynapenia and Aging: An Update. J. Gerontol. Ser. A 2011, 67, 28–40. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Braga, R. Ética na publicação de trabalhos científicos. Rev. Port. Med. Geral. Fam. 2013, 29, 354–356. [Google Scholar] [CrossRef]
- Bigelow, K.E.; Berme, N. Development of a Protocol for Improving the Clinical Utility of Posturography as a Fall-Risk Screening Tool. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 228–233. Available online: https://academic.oup.com/biomedgerontology/article-lookup/doi/10.1093/gerona/glq202 (accessed on 18 January 2020). [CrossRef]
- Pajala, S.; Era, P.; Koskenvuo, M.; Kaprio, J.; Törmäkangas, T.; Rantanen, T. Force Platform Balance Measures as Predictors of Indoor and Outdoor Falls in Community-Dwelling Women Aged 63–76 Years. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 171–178. Available online: https://academic.oup.com/biomedgerontology/article-lookup/doi/10.1093/gerona/63.2.171 (accessed on 20 January 2020). [CrossRef]
- King, A.C.; Whitt-Glover, M.C.; Marquez, D.X.; Buman, M.P.; Napolitano, M.A.; Jakicic, J.; Fulton, J.E.; Tennant, B.L. ACSM Physical Activity Promotion: Highlights from the 2018 Physical Activity Guidelines Advisory Committee Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1340–1353. [Google Scholar] [CrossRef]
- de Souto Barreto, P.; Morley, J.E.; Chodzko-Zajko, W.; Pitkala, K.H.; Weening-Djiksterhuis, E.; Rodriguez-Mañas, L.; Barbagallo, M.; Rosendahl, E.; Sinclair, A.; Landi, F.; et al. Recommendations on Physical Activity and Exercise for Older Adults Living in Long-Term Care Facilities: A Taskforce Report. J. Am. Med. Dir. Assoc. 2016, 17, 381–392. [Google Scholar] [CrossRef]
- Ziv, G.; Lidor, R. Music, exercise performance, and adherence in clinical populations and in the elderly: A review. J. Clin. Sport Psychol. 2011, 5, 1–23. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical Bases of Perception Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Colado, J.C.; Pedrosa, F.M.; Juesas, A.; Gargallo, P.; Carrasco, J.J.; Flandez, J.; Chupel, M.U.; Teixeira, A.M.; Naclerio, F. Concurrent validation of the OMNI-Resistance Exercise Scale of perceived exertion with elastic bands in the elderly. Exp. Gerontol. 2018, 103, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Roche, A.F.; Martorell, F. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- Gallucci, M. GAMLj: General Analyses for Linear Models. [jamovi module]. 2019. Available online: https://gamlj.github.io/ (accessed on 5 January 2022).
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Hamed, A.; Bohm, S.; Mersmann, F.; Arampatzis, A. Follow-up efficacy of physical exercise interventions on fall incidence and fall risk in healthy older adults: A systematic review and meta-analysis. Sport Med-Open 2018, 4, 56. [Google Scholar] [CrossRef]
- Wiesmeier, I.K.; Dalin, D.; Maurer, C. Elderly use proprioception rather than visual and vestibular cues for postural motor control. Front. Aging Neurosci. 2015, 7, 97. [Google Scholar] [CrossRef]
- Spink, M.J.; Menz, H.B.; Fotoohabadi, M.R.; Wee, E.; Landorf, K.B.; Hill, K.D.; Lord, S.R. Effectiveness of a multifaceted podiatry intervention to prevent falls in community dwelling older people with disabling foot pain: Randomised controlled trial. BMJ 2011, 342. [Google Scholar] [CrossRef]
- Chan, W.C.; Yeung, J.W.F.; Wong, C.S.M.; Lam, L.C.W.; Chung, K.F.; Luk, J.K.H.; Lee, J.S.W.; Law, A.C.K. Efficacy of physical exercise in preventing falls in older adults with cognitive impairment: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 149–154. [Google Scholar] [CrossRef]
- De Oliveira, M.R.; Inokuti, T.T.; da Costa Bispo, N.N.; de Almeida Pires Oliveira, D.A.; de Oliveira, R.F.; da Silva, R.A., Jr. Elderly individuals with increased risk of falls show postural balance impairment. Fisioter. Mov. 2015, 28, 269–276. [Google Scholar] [CrossRef]
- De Carvalho, M.P.; Luckow, E.L.T.; Siqueira, F.V. Quedas e fatores associados em idosos institucionalizados no município de Pelotas (RS, Brasil). Cien. Saude Colet. 2011, 16, 2945–2952. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Padoin, P.G.; Gonçalves, M.P.; Comaru, T.; Silva, A.M.V. Análise comparativa entre idosos praticantes de exercício físico e sedentários quanto ao risco de quedas. O Mundo. Saúde. 2010, 35, 158–164. [Google Scholar] [CrossRef]
- Ribeiro, F.; Gomes, S.; Teixeira, F.; Brochado, G.; Oliveira, J. Impacto da prática regular de exercício físico no equilíbrio, mobilidade funcional e risco de queda em idosos institucionalizados. Rev. Port. Ciências Desporto. 2016, 9, 36–42. [Google Scholar] [CrossRef]
- Prioli, A.C.; Freitas Júnior, P.B.; Barela, J.A. Physical activity and postural control in the elderly: Coupling between visual information and body sway. Gerontology 2005, 51, 145–148. [Google Scholar] [CrossRef]
- Lelard, T.; Doutrellot, P.L.; David, P.; Ahmaidi, S. Effects of a 12-Week Tai Chi Chuan Program Versus a Balance Training Program on Postural Control and Walking Ability in Older People. Arch. Phys. Med. Rehabil. 2010, 91, 9–14. [Google Scholar] [CrossRef]
- Tokmakidis, S.P.; Kalapotharakos, V.I.; Smilios, I.; Parlavantzas, A. Effects of detraining on muscle strength and mass after high or moderate intensity of resistance training in older adults. Clin. Physiol. Funct. Imaging 2009, 29, 316–319. [Google Scholar] [CrossRef]
- Salzman, B. Gait and balance disorders in older adults. Am. Fam. Physician 2011, 82, 61–68. [Google Scholar]
- Ramalho, F.; Santos-Rocha, R.; Branco, M.; Moniz-Pereira, V.; André, H.I.; Veloso, A.P.; Carnide, F. Effect of 6-month community-based exercise interventions on gait and functional fitness of an older population: A quasi-experimental study. Clin. Interv. Aging 2018, 13, 595–606. [Google Scholar] [CrossRef]
- Johnson, M.; George, A.; Tran, D.T. Analysis of falls incidents: Nurse and patient preventive behaviours. Int. J. Nurs. Pract. 2011, 17, 60–66. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S.G. A review of physical and cognitive interventions in aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Warm-Up (Dynamic Flexibility and Walk around the Room): 5 min and RPE 3–5 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Exercises | Sets | Reps | Cadence | Resting Interval | RPE | Progression | Weeks | Intensity * |
| Front squat | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 10−15 | 2 | Yellow |
| Unilateral hip flexion (chair) | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 15−20 | 2 | Yellow |
| Row (with flexion) (chair) | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 10−15 | 2 | Red |
| Chest Press (stand/chair) | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 15−20 | 2 | Red |
| Reverse fly (stand/chair) | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 10−15 | 2 | Green |
| Shoulder Press/twist | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 15−20 | 2 | Green |
| Frontal raiser (stand/chair) | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 3 × 15−20 | 2 | Blue |
| Biceps curl (stand/chair) | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | 4 × 15−20 | 2 | Blue |
| Overhead triceps extension | 2–3 | 10–20 | 2:3 | 30” | 6 to 7 | |||
| Circuit format | ||||||||
| Multidirectional walk around the room with an obstacle, cones, etc. | 3–5 min | 4 to 7 | ||||||
| Balance/ agility/motor coordinator exercises | 3–5 min | 4 to 7 | ||||||
| Cooling down | ||||||||
| Upper and Lower body’s static stretching (seated and standing) | 5 min | 2 to 3 | ||||||
| Variables | MSEG ẋ ± SD | CG ẋ ± SD | p-Value |
|---|---|---|---|
| Total of participants Male Female | 14 4 10 | 13 3 10 | |
| Chronological age (years) | 86 ± 3 | 87 ± 4 | 0.589 |
| Height (cm) | 155 ± 7.4 | 152 ± 10.2 | 0.389 |
| Weight (kg) | 70.4 ± 15.3 | 69.4 ± 11 | 0.845 |
| Body mass index | 29.1 ± 5.2 | 30 ± 4 | 0.616 |
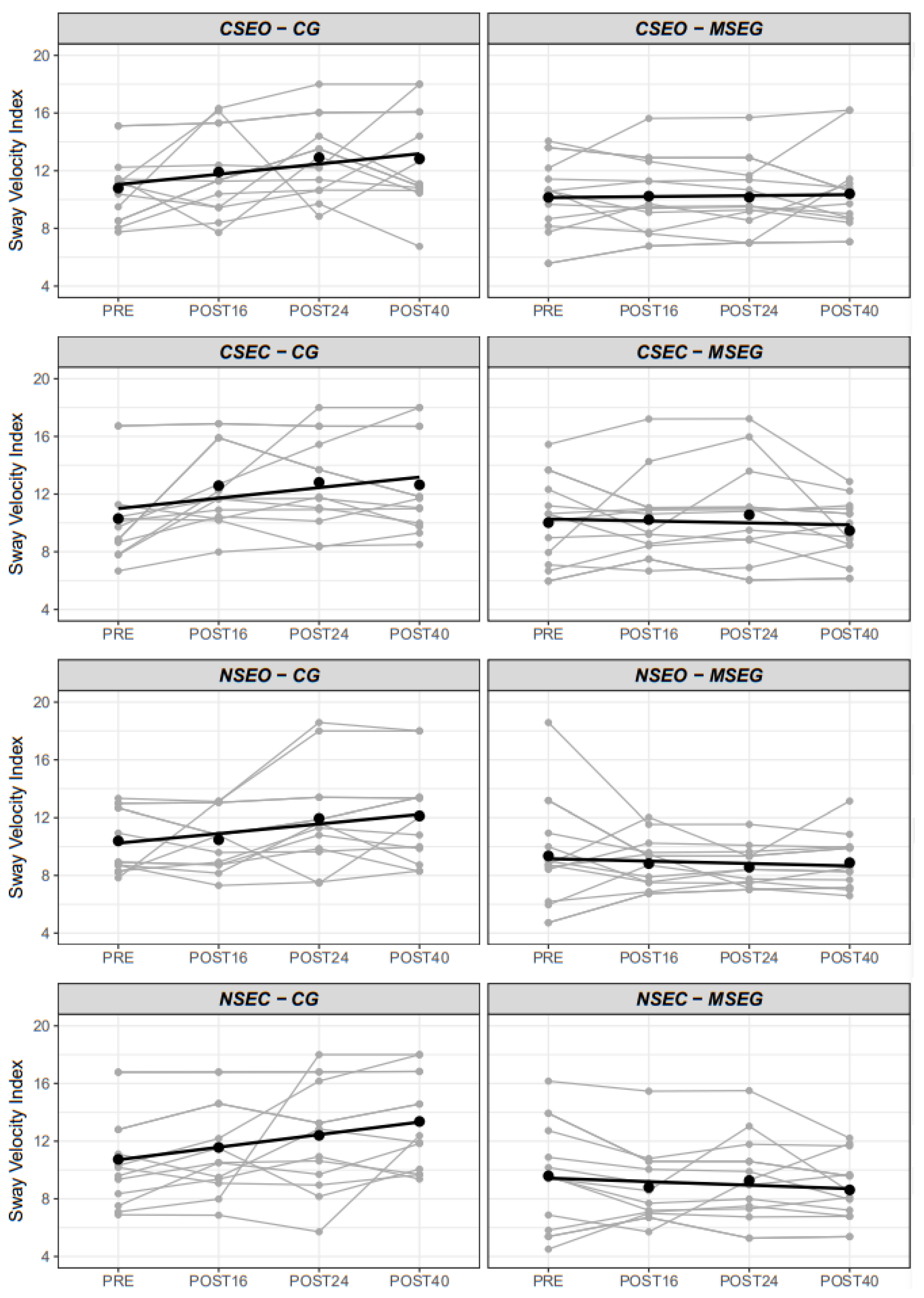
| Postural Control: | ẋ [95%CI] | ẋ [95%CI] | p-value |
| (i) CSEO | 10.2 [8.6 to 11.7] | 10.8 [9.2 to 12.4] | 0.566 |
| (ii) CSEC | 10 [8.5 to 11.6] | 10.3 [8.7 to 11.9] | 0.801 |
| (iii) NSEO | 9.4 [7.8 to 10.9] | 10.4 [8.8 to 12] | 0.353 |
| (iv) NSEC | 9.6 [8 to 11.1] | 10.7 [9.1 to 12.3] | 0.308 |
| Composite Index | 10.1 [8.9 to 11.4] | 10.5 [9.2 to 11.8] | 0.665 |
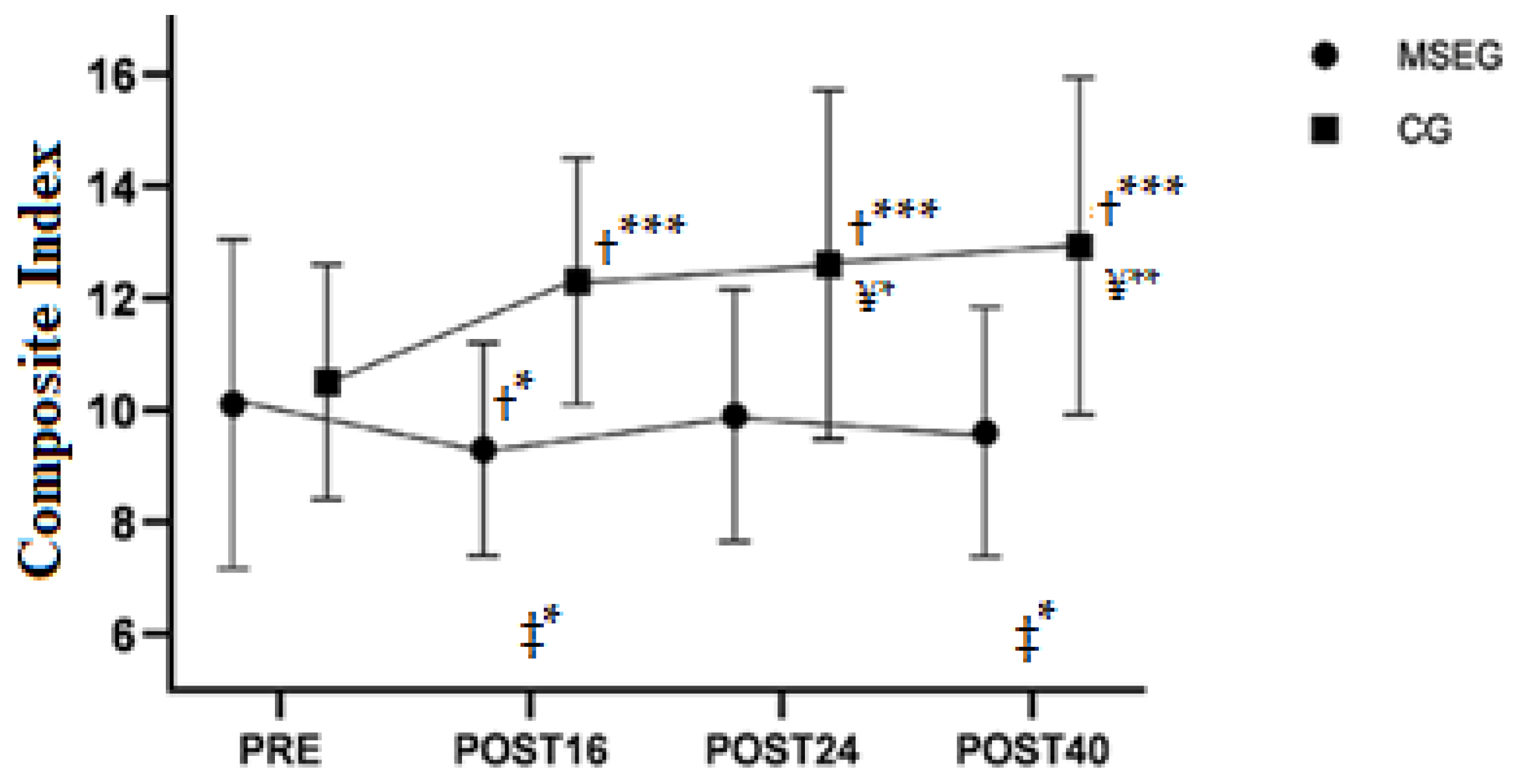
| Condition and Moment | MSEG ẋ [95%CI] | MSEG ∆% | CG ẋ [95%CI] | CG ∆% |
|---|---|---|---|---|
| Composite Index—Baseline, PRE | 10.1 [8.9 to 11.4] | 10.5 [9.2 to 11.8] | ||
| Composite Index—Training, POST16 | 9.3 [8.1 to 10.1] | −7.9% | 12.3 [11 to 13.6] | 17.2% * |
| Composite Index—Detraining, POST24 | 9.9 [8.7 to 11.1] | 6.4% | 12.6 [11.4 to 13.9] | 2.4% |
| Composite Index—Retraining, POST40 | 9.6 [8.4 to 10.8] | −3.1% | 12.9 [11.6 to 14.2] | 2.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, R.N.; Carballeira, E.; Silva, F.; Caldo-Silva, A.; Abreu, C.; Furtado, G.E.; Teixeira, A.M. The Effect of a Resistance Training, Detraining and Retraining Cycle on Postural Stability and Estimated Fall Risk in Institutionalized Older Persons: A 40-Week Intervention. Healthcare 2022, 10, 776. https://doi.org/10.3390/healthcare10050776
Rodrigues RN, Carballeira E, Silva F, Caldo-Silva A, Abreu C, Furtado GE, Teixeira AM. The Effect of a Resistance Training, Detraining and Retraining Cycle on Postural Stability and Estimated Fall Risk in Institutionalized Older Persons: A 40-Week Intervention. Healthcare. 2022; 10(5):776. https://doi.org/10.3390/healthcare10050776
Chicago/Turabian StyleRodrigues, Rafael Nogueira, Eduardo Carballeira, Fernanda Silva, Adriana Caldo-Silva, Cidalina Abreu, Guilherme Eustaquio Furtado, and Ana Maria Teixeira. 2022. "The Effect of a Resistance Training, Detraining and Retraining Cycle on Postural Stability and Estimated Fall Risk in Institutionalized Older Persons: A 40-Week Intervention" Healthcare 10, no. 5: 776. https://doi.org/10.3390/healthcare10050776
APA StyleRodrigues, R. N., Carballeira, E., Silva, F., Caldo-Silva, A., Abreu, C., Furtado, G. E., & Teixeira, A. M. (2022). The Effect of a Resistance Training, Detraining and Retraining Cycle on Postural Stability and Estimated Fall Risk in Institutionalized Older Persons: A 40-Week Intervention. Healthcare, 10(5), 776. https://doi.org/10.3390/healthcare10050776