
Effects of a Multicomponent Exercise Program on Prevalence and Severity of the Frailty Syndrome in a Sample of Italian Community-Dwelling Older Adults




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Procedures
2.2. Intervention
2.3. Measures
- Shrinking was measured as a body mass index (BMI) less than 21 kg/m2 [46]. Weight was detected by a Tanita Body Composition Analyzer BF-350, and height by an anthropometer. Weight and height were collected with an accuracy of 0.1 kg and 0.01 m, respectively.
- Weakness was evaluated by handgrip strength using the Smedley hand dynamometer (baseline 12-0286). We administered three trials for each hand with a pause of about 20 s between trials (always alternating right and left hands). The higher mean values between right and left hands were used for analysis. The same cut-off scores of Cardiovascular Health Study were applied to identify frail individuals for this criterion [2].
- Poor endurance and energy were assessed by using the following two items of the Center of Epidemiologic Studies Depression scale (CES-D) [47]: (a) “I felt that everything I did was an effort”, (b) “I could not get going”. The statements referred to the previous week. Those who answered “a moderate amount of the time (3–4 days)” or “most of the time” to at least one of the questions resulted in a positive result for the endurance and energy component.
- Slowness was evaluated by using the Timed Up and Go test (TUG) [48]. At the command “GO”, participants were asked to stand up from a chair, walk 3 m, turn around a cone, walk back to their chair and sit down at their usual pace. The test was performed once. A TUG cut-off of 10 s or more was used to categorize participants level of frailty based on their slowness [49,50].
- Low physical activity was identified in participants who did not engage in leisure activities such as hiking, gardening, dancing or cycling at least once a week, regardless of their participation in the exercise program proposed in this study [46].
2.4. Statistical Analysis
3. Results
3.1. Baseline Participants’ Characteristics
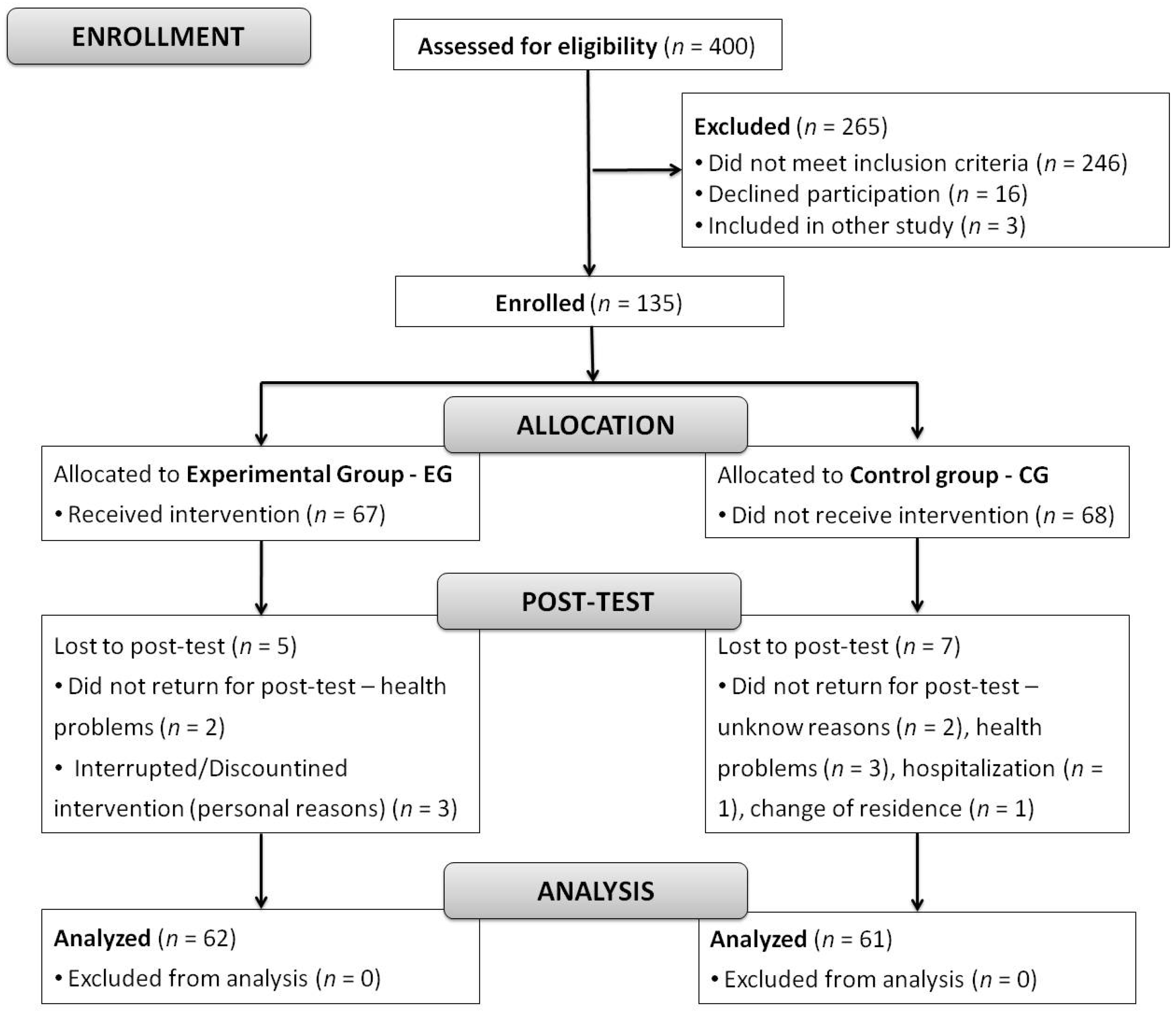
3.2. Drop-Out and Adherence
3.3. Effects of Training
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fried, L.P. Interventions for Human Frailty: Physical Activity as a Model. Cold Spring Harb. Perspect. Med. 2016, 6, a025916. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults Evidence for a Phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M255–M263. [Google Scholar] [CrossRef]
- Hubbard, R.E.; Rockwood, K. Frailty in Older Women. Maturitas 2011, 69, 203–207. [Google Scholar] [CrossRef]
- Rockwood, K.; Hogan, D.B.; MacKnight, C. Conceptualisation and Measurement of Frailty in Elderly People. Drugs Aging 2000, 17, 295–302. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. In Search of an Integral Conceptual Definition of Frailty: Opinions of Experts. J. Am. Med. Dir. Assoc. 2010, 11, 338–343. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Gobbens, R.J.; Rabaglietti, E. Mobility, Balance and Frailty in Community-Dwelling Older Adults: What Is the Best 1-Year Predictor of Falls?: Mobility, Balance, Frailty and Fall Risk. Geriatr. Gerontol. Int. 2016, 17, 1463–1469. [Google Scholar] [CrossRef]
- Gobbens, R.J.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M.G.A. Towards an Integral Conceptual Model of Frailty. J. Nutr. Health Aging 2010, 14, 175–181. [Google Scholar] [CrossRef]
- Rockwood, K.; Stadnyk, K.; MacKnight, C.; McDowell, I.; Hébert, R.; Hogan, D.B. A Brief Clinical Instrument to Classify Frailty in Elderly People. Lancet 1999, 353, 205–206. [Google Scholar] [CrossRef]
- Winograd, C.H.; Gerety, M.B.; Chung, M.; Goldstein, M.K.; Dominguez, F.; Vallone, R. Screening for Frailty: Criteria and Predictors of Outcomes. J. Am. Geriatr. Soc. 1991, 39, 778–784. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between Frailty and Quality of Life among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Rabaglietti, E. The Role of Individual Characteristics and Physical Frailty on Health Related Quality of Life (HRQOL): A Cross Sectional Study of Italian Community-Dwelling Older Adults. Arch. Gerontol. Geriatr. 2014, 59, 542–548. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Rabaglietti, E. Physical Frailty, Disability, and Dynamics in Health Perceptions: A Preliminary Mediation Model. Clin. Interv. Aging 2016, 11, 275–278. [Google Scholar] [CrossRef][Green Version]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of Physical Exercise Interventions in Frail Older Adults: A Systematic Review of Randomized Controlled Trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef]
- Binder, E.F.; Yarasheski, K.E.; Steger-May, K.; Sinacore, D.R.; Brown, M.; Schechtman, K.B.; Holloszy, J.O. Effects of Progressive Resistance Training on Body Composition in Frail Older Adults: Results of a Randomized, Controlled Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1425–1431. [Google Scholar] [CrossRef]
- Binder, E.F.; Schechtman, K.B.; Ehsani, A.A.; Steger-May, K.; Brown, M.; Sinacore, D.R.; Yarasheski, K.E.; Holloszy, J.O. Effects of Exercise Training on Frailty in Community-Dwelling Older Adults: Results of a Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2002, 50, 1921–1928. [Google Scholar] [CrossRef]
- Fairhall, N.; Sherrington, C.; Lord, S.R.; Kurrle, S.E.; Langron, C.; Lockwood, K.; Monaghan, N.; Aggar, C.; Cameron, I.D. Effect of a Multifactorial, Interdisciplinary Intervention on Risk Factors for Falls and Fall Rate in Frail Older People: A Randomised Controlled Trial. Age Ageing 2014, 43, 616–622. [Google Scholar] [CrossRef]
- Giné-Garriga, M.; Guerra, M.; Pagès, E.; Manini, T.M.; Jiménez, R.; Unnithan, V.B. The Effect of Functional Circuit Training on Physical Frailty in Frail Older Adults: A Randomized Controlled Trial. J. Aging Phys. Act. 2010, 18, 401–424. [Google Scholar] [CrossRef]
- Lustosa, L.P.; Silva, J.P.; Coelho, F.M.; Pereira, D.S.; Parentoni, A.N.; Pereira, L.S.M. Efeito de Um Programa de Resistência Muscular Na Capacidade Funcional e Na Força Muscular dos Extensores do Joelho em Idosas Pré-Frágeis da Comunidade: Ensaio Clínico Aleatorizado do Tipo Crossover. Rev. Bras. Fisioter. 2011, 15, 318–324. [Google Scholar] [CrossRef]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodriguez-Mañas, L.; Izquierdo, M. Multicomponent Exercises Including Muscle Power Training Enhance Muscle Mass, Power Output, and Functional Outcomes in Institutionalized Frail Nonagenarians. AGE 2014, 36, 773–785. [Google Scholar] [CrossRef]
- Bray, N.W.; Jones, G.J.; Rush, K.L.; Jones, C.A.; Jakobi, J.M. Multi-Component Exercise with High-Intensity, Free-Weight, Functional Resistance Training in Pre-Frail Females: A Quasi-Experimental, Pilot Study. J. Frailty Aging 2020, 9, 111–117. [Google Scholar] [CrossRef]
- Faber, M.J.; Bosscher, R.J.; Chin A Paw, M.J.; van Wieringen, P.C. Effects of Exercise Programs on Falls and Mobility in Frail and Pre-Frail Older Adults: A Multicenter Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2006, 87, 885–896. [Google Scholar] [CrossRef]
- Cameron, I.D.; Fairhall, N.; Langron, C.; Lockwood, K.; Monaghan, N.; Aggar, C.; Sherrington, C.; Lord, S.R.; Kurrle, S.E. A Multifactorial Interdisciplinary Intervention Reduces Frailty in Older People: Randomized Trial. BMC Med. 2013, 11, 65. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Seino, S.; Nishi, M.; Murayama, H.; Narita, M.; Yokoyama, Y.; Nofuji, Y.; Taniguchi, Y.; Amano, H.; Kitamura, A.; Shinkai, S. Effects of a Multifactorial Intervention Comprising Resistance Exercise, Nutritional and Psychosocial Programs on Frailty and Functional Health in Community-Dwelling Older Adults: A Randomized, Controlled, Cross-over Trial: Effects of a Multifactorial Intervention. Geriatr. Gerontol. Int. 2017, 17, 2034–2045. [Google Scholar] [CrossRef]
- Gené Huguet, L.; Navarro González, M.; Kostov, B.; Ortega Carmona, M.; Colungo Francia, C.; Carpallo Nieto, M.; Hervás Docón, A.; Vilarrasa Sauquet, R.; García Prado, R.; Sisó-Almirall, A. Pre Frail 80: Multifactorial Intervention to Prevent Progression of Pre-Frailty to Frailty in the Elderly. J. Nutr. Health Aging 2018, 22, 1266–1274. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Sist, X.; Domenich, R.; Jurado, L.; Saiz, A.; Roces, A.; Palomera, E.; Tarradelles, M.; Papiol, M. Effectiveness of an Intervention to Prevent Frailty in Pre-Frail Community-Dwelling Older People Consulting in Primary Care: A Randomised Controlled Trial. Age Ageing 2017, 46, 401–407. [Google Scholar] [CrossRef]
- Yu, R.; Tong, C.; Ho, F.; Woo, J. Effects of a Multicomponent Frailty Prevention Program in Prefrail Community-Dwelling Older Persons: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 21, 294.e1–294.e10. [Google Scholar] [CrossRef]
- Puts, M.T.E.; Toubasi, S.; Andrew, M.K.; Ashe, M.C.; Ploeg, J.; Atkinson, E.; Ayala, A.P.; Roy, A.; Rodríguez Monforte, M.; Bergman, H.; et al. Interventions to Prevent or Reduce the Level of Frailty in Community-Dwelling Older Adults: A Scoping Review of the Literature and International Policies. Age Ageing 2017, 46, 383–392. [Google Scholar] [CrossRef]
- Theou, O.; Stathokostas, L.; Roland, K.P.; Jakobi, J.M.; Patterson, C.; Vandervoort, A.A.; Jones, G.R. The Effectiveness of Exercise Interventions for the Management of Frailty: A Systematic Review. J. Aging Res. 2011, 2011, 569194. [Google Scholar] [CrossRef]
- Walston, J.; Buta, B.; Xue, Q.-L. Frailty Screening and Interventions. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef]
- Cesari, M.; Vellas, B.; Hsu, F.-C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.M.; Miller, M.E.; et al. A Physical Activity Intervention to Treat the Frailty Syndrome in Older Persons--Results from the LIFE-P Study. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 216–222. [Google Scholar] [CrossRef]
- Arrieta, H.; Rezola-Pardo, C.; Gil, S.M.; Virgala, J.; Iturburu, M.; Antón, I.; González-Templado, V.; Irazusta, J.; Rodriguez-Larrad, A. Effects of Multicomponent Exercise on Frailty in Long-Term Nursing Homes: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2019, 67, 1145–1151. [Google Scholar] [CrossRef]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J. A Multicomponent Exercise Intervention That Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef]
- Losa-Reyna, J.; Baltasar-Fernandez, I.; Alcazar, J.; Navarro-Cruz, R.; Garcia-Garcia, F.J.; Alegre, L.M.; Alfaro-Acha, A. Effect of a Short Multicomponent Exercise Intervention Focused on Muscle Power in Frail and Pre Frail Elderly: A Pilot Trial. Exp. Gerontol. 2019, 115, 114–121. [Google Scholar] [CrossRef]
- Takano, E.; Teranishi, T.; Watanabe, T.; Ohno, K.; Kitaji, S.; Sawa, S.; Kanada, Y.; Toba, K.; Kondo, I. Differences in the Effect of Exercise Interventions between Prefrail Older Adults and Older Adults without Frailty: A Pilot Study: Exercise Interventions in Older Adults. Geriatr. Gerontol. Int. 2017, 17, 1265–1269. [Google Scholar] [CrossRef]
- Kwon, J.; Yoshida, Y.; Yoshida, H.; Kim, H.; Suzuki, T.; Lee, Y. Effects of a Combined Physical Training and Nutrition Intervention on Physical Performance and Health-Related Quality of Life in Prefrail Older Women Living in the Community: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 263.e1–263.e8. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Chen, I.-H.; Wang, R.-Y. Effects of Kinect-Based Exergaming on Frailty Status and Physical Performance in Prefrail and Frail Elderly: A Randomized Controlled Trial. Sci. Rep. 2019, 9, 9353. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Liubicich, M.E.; Settanni, M.; Rabagliett, E. A Multicomponent Exercise Program for Older Adults Living in Residential Care Facilities: Direct and Indirect Effects on Physical Functioning. J. Aging Phys. Act. 2015, 23, 409–416. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Ethical Principles of Psychologists and Code of Conduct. Am. Psychol. 2002, 57, 1060–1073. [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical Activity and Public Health in Older Adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Giannotta, F.; Rabaglietti, E. Associations of Frailty and Psychosocial Factors with Autonomy in Daily Activities: A Cross-Sectional Study in Italian Community-Dwelling Older Adults. Clin. Interv. Aging 2016, 11, 37. [Google Scholar]
- Ávila-Funes, J.A.; Amieva, H.; Barberger-Gateau, P.; Le Goff, M.; Raoux, N.; Ritchie, K.; Carrière, I.; Tavernier, B.; Tzourio, C.; Gutiérrez-Robledo, L.M.; et al. Cognitive Impairment Improves the Predictive Validity of the Phenotype of Frailty for Adverse Health Outcomes: The Three-City Study: Cognitive Impairment and Frailty. J. Am. Geriatr. Soc. 2009, 57, 453–461. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Savva, G.M.; Donoghue, O.A.; Horgan, F.; O’Regan, C.; Cronin, H.; Kenny, R.A. Using Timed Up-and-Go to Identify Frail Members of the Older Population. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 441–446. [Google Scholar] [CrossRef]
- Lee, J.E.; Chun, H.; Kim, Y.-S.; Jung, H.-W.; Jang, I.-Y.; Cha, H.-M.; Son, K.Y.; Cho, B.; Kwon, I.S.; Yoon, J.L. Association between Timed Up and Go Test and Subsequent Functional Dependency. J. Korean Med. Sci. 2020, 35, e25. [Google Scholar] [CrossRef]
- Apóstolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D’Avanzo, B.; Gwyther, H.; et al. Effectiveness of Interventions to Prevent Pre-Frailty and Frailty Progression in Older Adults: A Systematic Review. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 140–232. [Google Scholar] [CrossRef]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise Training and Nutritional Supplementation for Physical Frailty in Very Elderly People. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet Lond. Engl. 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Gill, T.M.; Baker, D.I.; Gottschalk, M.; Peduzzi, P.N.; Allore, H.; Byers, A. A Program to Prevent Functional Decline in Physically Frail, Elderly Persons Who Live at Home. N. Engl. J. Med. 2002, 347, 1068–1074. [Google Scholar] [CrossRef]
- Del Pozo-Cruz, B.; Mañas, A.; Martín-García, M.; Marín-Puyalto, J.; García-García, F.J.; Rodriguez-Mañas, L.; Guadalupe-Grau, A.; Ara, I. Frailty Is Associated with Objectively Assessed Sedentary Behaviour Patterns in Older Adults: Evidence from the Toledo Study for Healthy Aging (TSHA). PLoS ONE 2017, 12, e0183911. [Google Scholar] [CrossRef]


{kind=link}
| Intervention Characteristics: 16 Weeks, 2 Sessions/Week, 70 Min/Session | |
|---|---|
| Day 1 | Day 2 |
| Warm up (10 min) | Warm up (5 min) |
| Balance training (15 min) | Endurance walking exercises (25 min) |
| Resistance training (20 min) | Balance training (15 min) |
| Walking exercises (15 min) | Resistance training (15 min) |
| Range of movement (10 min) | Breathing and stretching (10 min) |
| Variable | Whole Sample n = 123 | EG n = 62 | CG n = 61 | p Value 1 |
|---|---|---|---|---|
| Age, years, mean (SD), years | 74 (6) | 73 (5) | 74 (6) | 0.917 |
| Gender, n (%) of female | 79 (64.2) | 35 (56.5) | 44 (72.1) | 0.070 |
| Level of education, n (%) | 0.796 | |||
| Primary school, 5 years | 61 (49.6) | 28 (45.2) | 33 (54.1) | |
| Secondary school, 8 years | 38 (30.9) | 21 (33.9) | 17 (27.9) | |
| High school diploma, 13 years | 20 (16.3) | 11 (17.7) | 9 (14.8) | |
| University degree, 18 years | 4 (3.3) | 2 (3.2) | 2 (3.3) | |
| Marital status, n (%) | 0.037 | |||
| Married/Cohabiting | 66 (53.7) | 37 (59.7) | 29 (47.5) | |
| Not married | 5 (4.0) | 3 (4.8) | 2 (3.3) | |
| Widowed | 45 (36.6) | 16 (25.8) | 29 (47.5) | |
| Divorced | 7 (5.7) | 6 (9.7) | 1 (1.7) | |
| Past job, n (%) | 0.451 | |||
| Housewife | 13 (10.6) | 8 (12.9) | 5 (8.2) | |
| Manual | 64 (52.0) | 29 (46.8) | 35 (57.4) | |
| Non-manual | 46 (37.4) | 25 (40.3) | 21 (34.4) | |
| Chronic disease (CD), n (%) of people with at least 1 CD | 66 (53.7) | 30 (48.4) | 36 (59.0) | 0.237 |
| Pharmacotherapy, n (%) of Yes | 107 (87.0) | 54 (87.1) | 53 (86.9) | 0.972 |
| Perception of health, n (%) | 0.239 | |||
| Poor | 1 (0.8) | 0 (0.0) | 1 (1.6) | |
| Fair | 50 (40.7) | 21 (33.9) | 29 (47.5) | |
| Good | 68 (55.3) | 38 (61.3) | 30 (49.2) | |
| Excellent | 4 (3.3) | 3 (4.8) | 1 (1.6) | |
| MMSE, mean (SD) | 28.5 (1.9) | 28.2 (1.9) | 28.9 (1.9) | 0.056 |
| Physical frailty, mean (SD) | 1.44 (1.12) | 1.48 (1.10) | 1.39 (1.14) | 0.655 |
| Physical frailty status, n (%) 2 | 0.959 | |||
| Robust | 27 (22.0) | 13 (21.0) | 14 (23.0) | |
| Pre-frail | 72 (58.5) | 37 (59.7) | 35 (57.4) | |
| Frail | 24 (19.5) | 12 (19.4) | 12 (19.7) |
| CHS Frailty Criteria | Group | T0 Baseline n (%) | T1 Post-Test n (%) | |
|---|---|---|---|---|
| No Frail | Frail | |||
| Shrinking | EG | No frail | 58 (94) | 2 (3) |
| Frail | 2 (3) | 0 (0) | ||
| CG | No frail | 60 (98) | 1 (2) | |
| Frail | 0 (0) | 0 (0) | ||
| Weakness | EG | No frail | 34 (55) | 2 (3) |
| Frail | 10 (16) | 16 (26) | ||
| CG | No frail | 22 (36) | 15 (25) | |
| Frail | 8 (13) | 16 (26) | ||
| Poor endurance and energy | EG | No frail | 23 (37) | 5 (8) |
| Frail | 23 (37) | 11 (18) | ||
| CG | No frail | 23 (38) | 15 (25) | |
| Frail | 7 (11) | 16 (26) | ||
| Slowness | EG | No frail | 45 (73) | 2 (3) |
| Frail | 5 (8) | 10 (16) | ||
| CG | No frail | 36 (59) | 11 (18) | |
| Frail | 6 (10) | 8 (13) | ||
| Low physical activity | EG | No frail | 47 (76) | 0 (0) |
| Frail | 4 (6) | 11 (18) | ||
| CG | No frail | 37 (61) | 0 (0) | |
| Frail | 0 (0) | 24 (39) | ||
| EG | CG | ||||||
|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | F(1114) | p Value | ƞ2p | |
| Physical frailty | 1.48 (1.10) | 0.95 (1.08) | 1.39 (1.14) | 1.74 (1.15) | 43.51 | <0.001 | 0.276 |
| Group | Physical Frailty Status | n | Physical Frailty Change, Mean (SD) | F | p-Value | ƞ2p |
|---|---|---|---|---|---|---|
| EG | Robust | 13 | 0.23 (0.44) *,** | 11.32 | <0.001 | 0.299 |
| Pre-frail | 37 | −0.76 (0.72) | ||||
| Frail | 12 | −0.67 (0.78) | ||||
| CG | Robust | 14 | 0.57 (0.65) | 1.62 | n.s. | 0.059 |
| Pre-frail | 35 | 0.34 (0.91) | ||||
| Frail | 12 | 0.08 (0.79) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulasso, A.; Roppolo, M.; Rainoldi, A.; Rabaglietti, E. Effects of a Multicomponent Exercise Program on Prevalence and Severity of the Frailty Syndrome in a Sample of Italian Community-Dwelling Older Adults. Healthcare 2022, 10, 911. https://doi.org/10.3390/healthcare10050911
Mulasso A, Roppolo M, Rainoldi A, Rabaglietti E. Effects of a Multicomponent Exercise Program on Prevalence and Severity of the Frailty Syndrome in a Sample of Italian Community-Dwelling Older Adults. Healthcare. 2022; 10(5):911. https://doi.org/10.3390/healthcare10050911
Chicago/Turabian StyleMulasso, Anna, Mattia Roppolo, Alberto Rainoldi, and Emanuela Rabaglietti. 2022. "Effects of a Multicomponent Exercise Program on Prevalence and Severity of the Frailty Syndrome in a Sample of Italian Community-Dwelling Older Adults" Healthcare 10, no. 5: 911. https://doi.org/10.3390/healthcare10050911
APA StyleMulasso, A., Roppolo, M., Rainoldi, A., & Rabaglietti, E. (2022). Effects of a Multicomponent Exercise Program on Prevalence and Severity of the Frailty Syndrome in a Sample of Italian Community-Dwelling Older Adults. Healthcare, 10(5), 911. https://doi.org/10.3390/healthcare10050911