
Change of Direction Speed and Reactive Agility in Prediction of Injury in Football; Prospective Analysis over One Half-Season





Abstract
1. Introduction
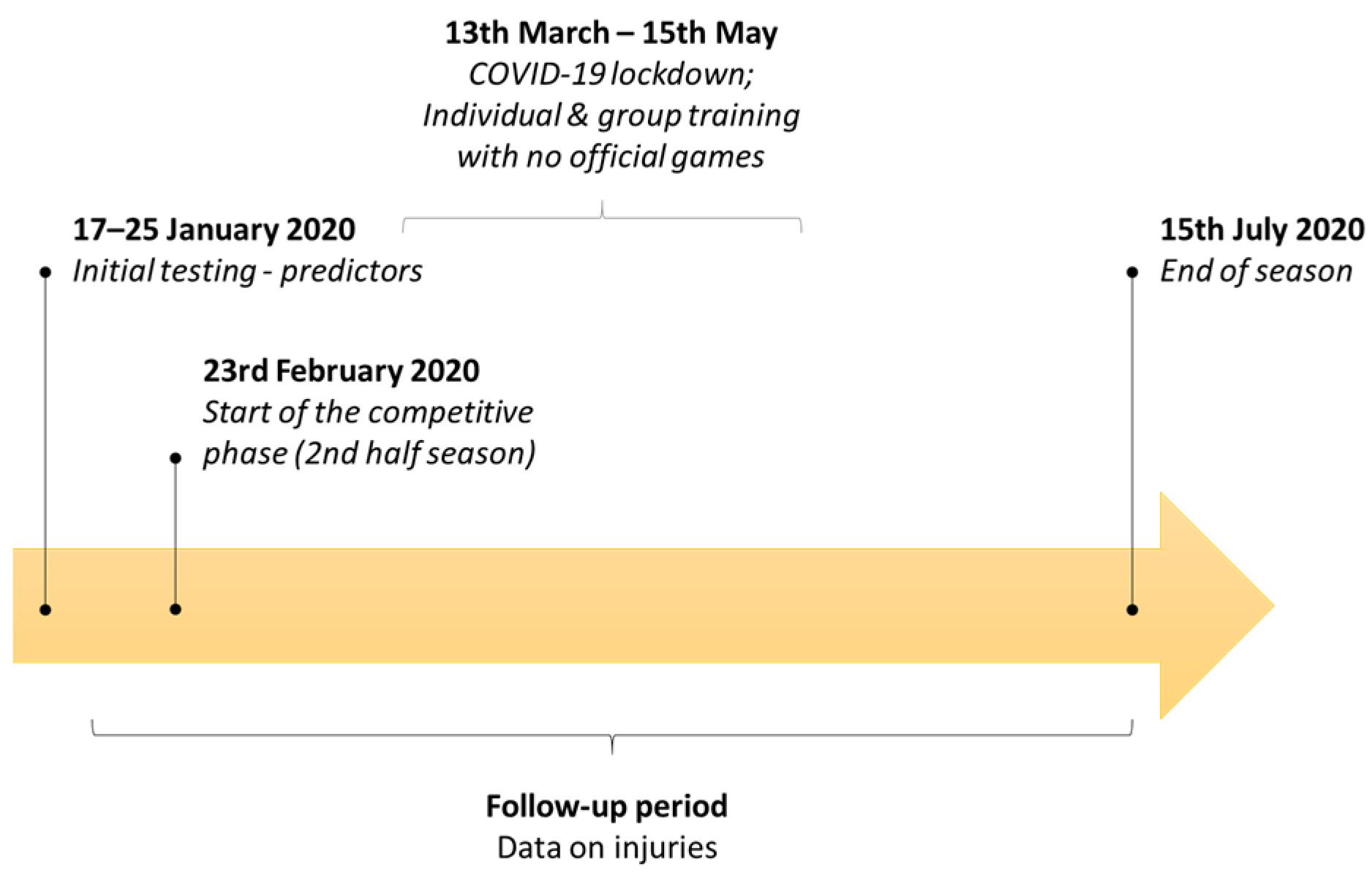
2. Materials and Methods
2.1. Participants
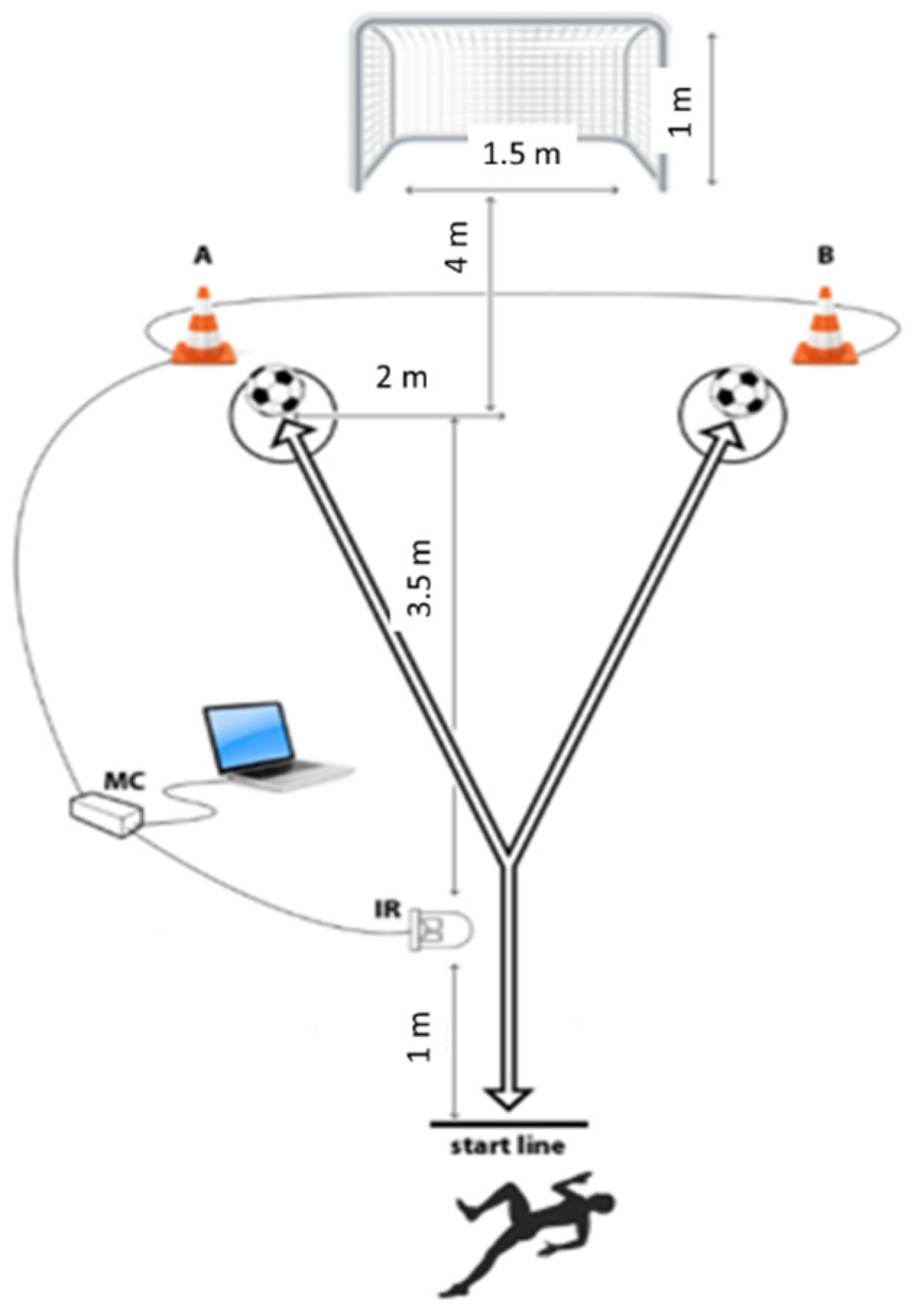
2.2. Variables and Measurements
2.3. Statistics
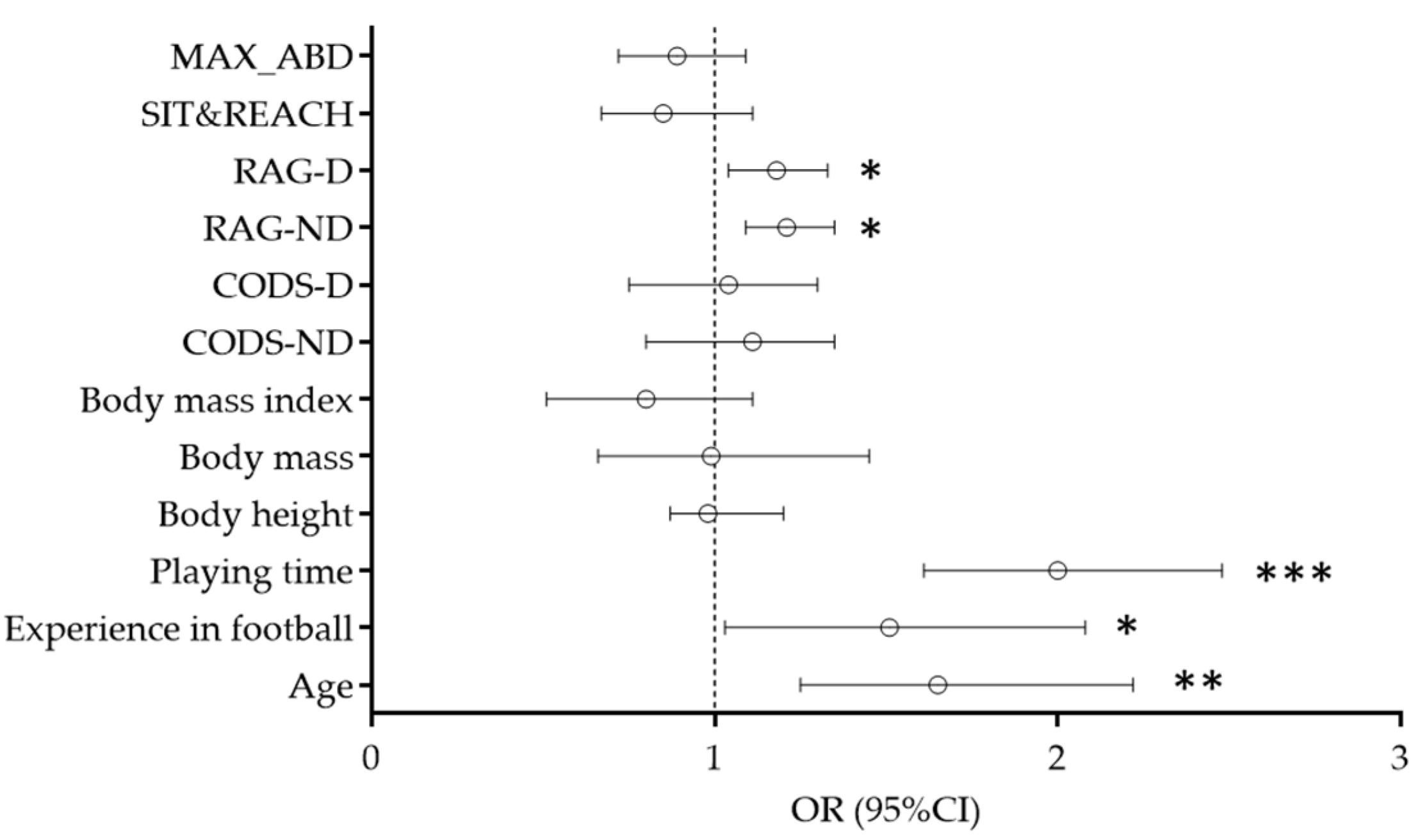
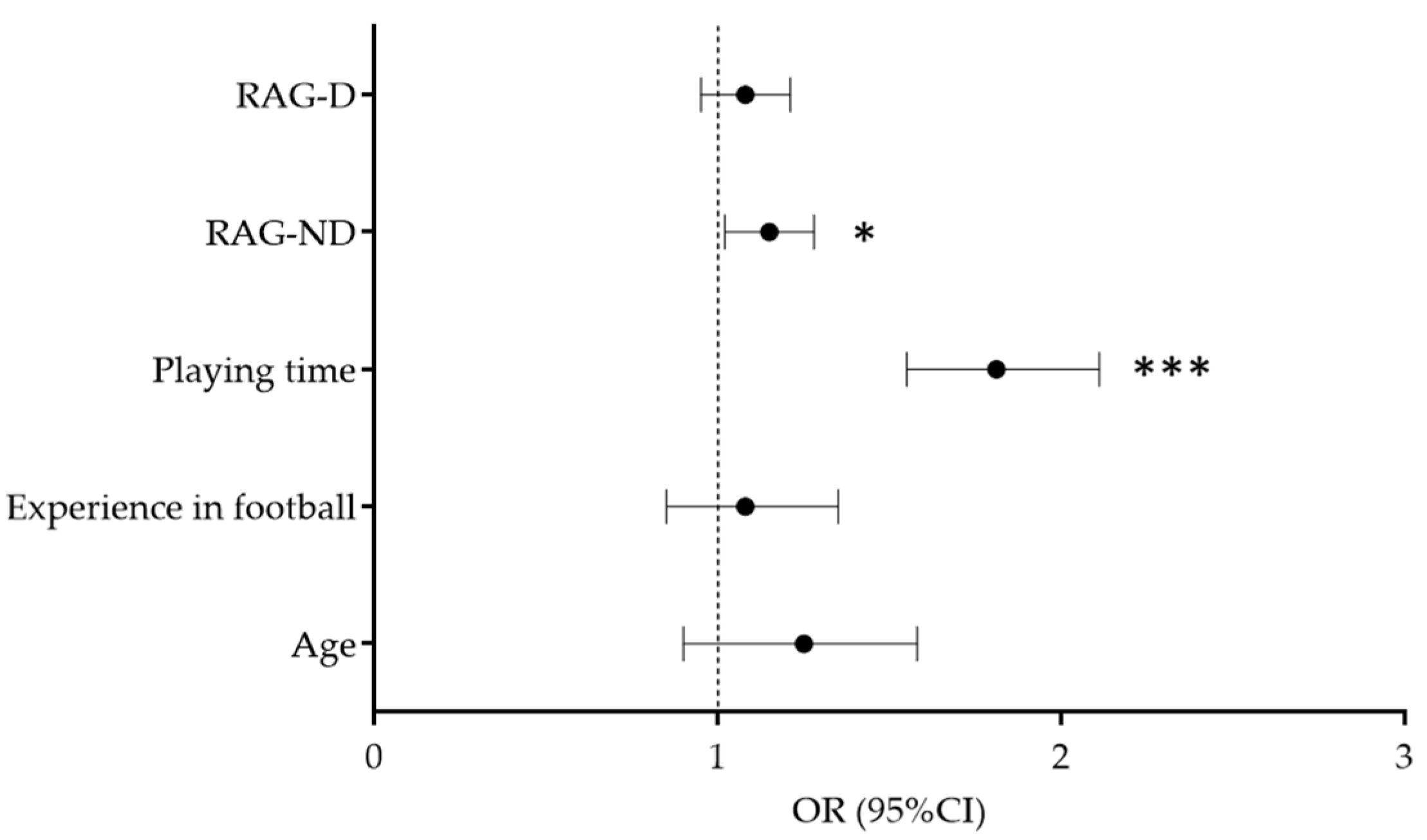
3. Results
4. Discussion
4.1. Age and Playing Time as Predictors of Injury
4.2. Reactive Agility and Injury Occurence
4.3. Dominant vs. Non-Dominant Side Reactive Agility Performances and Injury Occurence
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Enright, K.; Green, M.; Hay, G.; Malone, J.J. Workload and injury in professional soccer players: Role of injury tissue type and injury severity. Int. J. Sports Med. 2020, 41, 89–97. [Google Scholar] [CrossRef]
- Owen, A.L.; Forsyth, J.J.; Wong, D.P.; Dellal, A.; Connelly, S.P.; Chamari, K. Heart rate–based training intensity and its impact on injury incidence among elite-level professional soccer players. J. Strength Cond. Res. 2015, 29, 1705–1712. [Google Scholar] [CrossRef]
- Fang, B.; Kim, Y.; Choi, M. Effect of Cycle-Based High-Intensity Interval Training and Moderate to Moderate-Intensity Continuous Training in Adolescent Soccer Players. Healthcare 2021, 9, 1628. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C.; Archer, D.; Hogg, B.; Bush, M.; Bradley, P. The evolution of physical and technical performance parameters in the English Premier League. Int. J. Sports Med. 2014, 35, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Dupont, G.; Nedelec, M.; McCall, A.; McCormack, D.; Berthoin, S.; Wisløff, U. Effect of 2 soccer matches in a week on physical performance and injury rate. Am. J. Sports Med. 2010, 38, 1752–1758. [Google Scholar] [CrossRef]
- Ekstrand, J.; Lundqvist, D.; Davison, M.; D’Hooghe, M.; Pensgaard, A.M. Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs. Br. J. Sports Med. 2019, 53, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef]
- Jaspers, A.; Brink, M.S.; Probst, S.G.; Frencken, W.G.; Helsen, W.F. Relationships between training load indicators and training outcomes in professional soccer. Sports Med. 2017, 47, 533–544. [Google Scholar] [CrossRef]
- Sarah, J.; Lisman, P.; Gribbin, T.C.; Murphy, K.; Deuster, P.A. Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 3—flexibility, power, speed, balance, and agility. J. Strength Cond. Res. 2019, 33, 1723–1735. [Google Scholar]
- Daneshjoo, A.; Nobari, H.; Kalantari, A.; Amiri-Khorasani, M.; Abbasi, H.; Rodal, M.; Pérez-Gómez, J.; Ardigò, L.P. Comparison of Knee and Hip Kinematics during Landing and Cutting between Elite Male Football and Futsal Players. Healthcare 2021, 9, 606. [Google Scholar] [CrossRef]
- Ekstrand, J. Keeping your top players on the pitch: The key to football medicine at a professional level. Br. J. Sports Med. 2013, 47, 723–724. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef]
- Jaspers, A.; Kuyvenhoven, J.P.; Staes, F.; Frencken, W.G.; Helsen, W.F.; Brink, M.S. Examination of the external and internal load indicators’ association with overuse injuries in professional soccer players. J. Sports Sci. Med. 2018, 21, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, J.; Junge, A.; Chomiak, J.; Graf-Baumann, T.; Peterson, L.; Rosch, D.; Hodgson, R. Risk factor analysis for injuries in football players. Am. J. Sports Med. 2016. [Google Scholar] [CrossRef]
- de la Motte, S.J.; Gribbin, T.C.; Lisman, P.; Murphy, K.; Deuster, P.A. Systematic Review of the Association Between Physical Fitness and Musculoskeletal Injury Risk: Part 2—Muscular Endurance and Muscular Strength. J. Strength Cond. Res. 2017, 31, 3218–3234. [Google Scholar] [CrossRef] [PubMed]
- Ursej, E.; Sekulic, D.; Prus, D.; Gabrilo, G.; Zaletel, P. Investigating the Prevalence and Predictors of Injury Occurrence in Competitive Hip Hop Dancers: Prospective Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3214. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.; Chalmers, S.; Milanese, S.; Fuller, J. The association between Y-balance test scores, injury, and physical performance in elite adolescent Australian footballers. J. Sci. Med. Sport 2021. [Google Scholar] [CrossRef]
- Lisman, P.J.; de la Motte, S.J.; Gribbin, T.C.; Jaffin, D.P.; Murphy, K.; Deuster, P.A. A Systematic Review of the Association Between Physical Fitness and Musculoskeletal Injury Risk: Part 1—Cardiorespiratory Endurance. J. Strength Cond. Res. 2017, 31, 1744–1757. [Google Scholar] [CrossRef]
- Sheppard, J.M.; Young, W.B. Agility literature review: Classifications, training and testing. J. Sports Sci. Med. 2006, 24, 919–932. [Google Scholar] [CrossRef]
- Sekulic, D.; Spasic, M.; Esco, M.R. Predicting agility performance with other performance variables in pubescent boys: A multiple-regression approach. Percept. Mot. Skills 2014, 118, 447–461. [Google Scholar] [CrossRef]
- Pehar, M.; Sisic, N.; Sekulic, D.; Coh, M.; Uljevic, O.; Spasic, M.; Krolo, A.; Idrizovic, K. Analyzing the relationship between anthropometric and motor indices with basketball specific pre-planned and non-planned agility performances. J. Sports Med. Phys. Fitness 2018, 58, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Pehar, M.; Krolo, A.; Spasic, M.; Uljevic, O.; Calleja-González, J.; Sattler, T. Evaluation of Basketball-Specific Agility: Applicability of Preplanned and Nonplanned Agility Performances for Differentiating Playing Positions and Playing Levels. J. Strength Cond. Res. 2017, 31, 2278–2288. [Google Scholar] [CrossRef]
- Sekulic, D.; Krolo, A.; Spasic, M.; Uljevic, O.; Peric, M. The development of a New Stop’n’go reactive-agility test. J. Strength Cond. Res. 2014, 28, 3306–3312. [Google Scholar] [CrossRef]
- Gabbett, T.J.; Kelly, J.N.; Sheppard, J.M. Speed, change of direction speed, and reactive agility of rugby league players. J. Strength Cond. Res. 2008, 22, 174–181. [Google Scholar] [CrossRef]
- Coh, M.; Vodicar, J.; Žvan, M.; Šimenko, J.; Stodolka, J.; Rauter, S.; Mackala, K. Are Change-of-Direction Speed and Reactive Agility Independent Skills Even When Using the Same Movement Pattern? J. Strength Cond. Res. 2018, 32, 1929–1936. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.; Afonso, J.; Camões, M.; Sarmento, H.; Sá, M.; Lima, R.; Oliveira, R.; Clemente, F.M. Methodological Characteristics, Physiological and Physical Effects, and Future Directions for Combined Training in Soccer: A Systematic Review. Healthcare 2021, 9, 1075. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, H.; Åslin, E.; Krolo, A.; Jukic, I.; Uljevic, O.; Spasic, M.; Sekulic, D. Importance of reactive agility and change of direction speed in differentiating performance levels in junior soccer players: Reliability and validity of newly developed soccer-specific tests. Front. Physiol. 2018, 9, 506. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic, M.; Sporis, G.; Omrcen, D.; Fiorentini, F. Effects of speed, agility, quickness training method on power performance in elite soccer players. J. Strength Cond. Res. 2011, 25, 1285–1292. [Google Scholar] [CrossRef]
- Trecroci, A.; Longo, S.; Perri, E.; Iaia, F.M.; Alberti, G. Field-based physical performance of elite and sub-elite middle-adolescent soccer players. Res. Sports Med. 2019, 27, 60–71. [Google Scholar] [CrossRef]
- Purnell, M.; Shirley, D.; Nicholson, L.; Adams, R. Acrobatic gymnastics injury: Occurrence, site and training risk factors. Phys. Ther. Sport 2010, 11, 40–46. [Google Scholar] [CrossRef]
- Faude, O.; Junge, A.; Kindermann, W.; Dvorak, J. Injuries in female soccer players: A prospective study in the German national league. Am. J. Sports Med. 2005, 33, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Sanz, A.; Pablos, C.; Ballester, R.; Sanchez-Alarcos, J.V.; Huertas, F. Range of Motion and Injury Occurrence in Elite Spanish Soccer Academies. Not Only a Hamstring Shortening-Related Problem. J. Strength Cond. Res. 2020, 34, 1924–1932. [Google Scholar] [CrossRef]
- Lemmink, K.A.; Kemper, H.C.; Greef, M.H.; Rispens, P.; Stevens, M. The validity of the sit-and-reach test and the modified sit-and-reach test in middle-aged to older men and women. Res. Q. Exerc. Sport 2003, 74, 331–336. [Google Scholar] [CrossRef]
- Malliaras, P.; Hogan, A.; Nawrocki, A.; Crossley, K.; Schache, A. Hip flexibility and strength measures: Reliability and association with athletic groin pain. Br. J. Sports Med. 2009, 43, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Versic, S.; Pehar, M.; Modric, T.; Pavlinovic, V.; Spasic, M.; Uljevic, O.; Corluka, M.; Sattler, T.; Sekulic, D. Bilateral Symmetry of Jumping and Agility in Professional Basketball Players: Differentiating Performance Levels and Playing Positions. Symmetry 2021, 13, 1316. [Google Scholar] [CrossRef]
- Clarsen, B.; Ronsen, O.; Myklebust, G.; Florenes, T.W.; Bahr, R. The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. Br. J. Sports Med. 2014, 48, 754–760. [Google Scholar] [CrossRef]
- Sekulic, D.; Prus, D.; Zevrnja, A.; Peric, M.; Zaletel, P. Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study. Children 2020, 7, 297. [Google Scholar] [CrossRef]
- Keller, C.S.; Noyes, F.R.; Buncher, C.R. The medical aspects of soccer injury epidemiology. Am. J. Sports Med. 1988, 16, S-105–S-112. [Google Scholar] [CrossRef]
- Östenberg, A.; Roos, H. Injury risk factors in female European football. A prospective study of 123 players during one season. Scand. J. Med. Sci. Sports 2000, 10, 279–285. [Google Scholar] [CrossRef]
- Kalén, A.; Rey, E.; de Rellán-Guerra, A.S.; Lago-Peñas, C. Are Soccer Players Older Now Than Before? Aging Trends and Market Value in the Last Three Decades of the UEFA Champions League. Front. Psychol. 2019, 10, 76. [Google Scholar] [CrossRef]
- Bowen, L.; Gross, A.S.; Gimpel, M.; Li, F.-X. Accumulated workloads and the acute: Chronic workload ratio relate to injury risk in elite youth football players. Br. J. Sports Med. 2017, 51, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Lundblad, M.; Waldén, M.; Magnusson, H.; Karlsson, J.; Ekstrand, J. The UEFA injury study: 11-year data concerning 346 MCL injuries and time to return to play. Br. J. Sports Med. 2013, 47, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Söderman, K.; Alfredson, H.; Pietilä, T.; Werner, S. Risk factors for leg injuries in female soccer players: A prospective investigation during one out-door season. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Tropp, H. The incidence of ankle sprains in soccer. Foot Ankle Int. 1990, 11, 41–44. [Google Scholar] [CrossRef]
- Calligeris, T.; Burgess, T. The incidence of injuries and exposure time of professional football club players in the Premier Soccer League during football season. S. Afr. J. Sports Med. 2015, 27, 16–19. [Google Scholar] [CrossRef][Green Version]
- Gabbett, T.J.; Ullah, S.; Jenkins, D.; Abernethy, B. Skill qualities as risk factors for contact injury in professional rugby league players. J. Sports Sci. 2012, 30, 1421–1427. [Google Scholar] [CrossRef]
- Gabbett, T.; Kelly, J.; Ralph, S.; Driscoll, D. Physiological and anthropometric characteristics of junior elite and sub-elite rugby league players, with special reference to starters and non-starters. J. Sci. Med. Sport 2009, 12, 215–222. [Google Scholar] [CrossRef]
- Gabbett, T.; Wake, M.; Abernethy, B. Use of dual-task methodology for skill assessment and development: Examples from rugby league. J. Sports Sci. 2011, 29, 7–18. [Google Scholar] [CrossRef]
- McNeil, D.G.; Spittle, M.; Mesagno, C. Imagery training for reactive agility: Performance improvements for decision time but not overall reactive agility. Int. J. Sport Exerc. Psycho. 2021, 19, 429–445. [Google Scholar] [CrossRef]
- Jeffreys, I. A task-based approach to developing context-specific agility. Strength Cond. J. 2011, 33, 52–59. [Google Scholar] [CrossRef]
- Sporis, G.; Jukic, I.; Ostojic, S.M.; Milanovic, D. Fitness profiling in soccer: Physical and physiologic characteristics of elite players. J. Strength Cond. Res. 2009, 23, 1947–1953. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.; O’Donoghue, P. A movement classification for the investigation of agility demands and injury risk in sport. Int. J. Perform. Anal. Sport 2008, 8, 127–144. [Google Scholar] [CrossRef]
- Bloomfield, J.; Polman, R.; O’Donoghue, P. Turning movements performed during FA Premier League soccer matches. J. Sports Sci. Med. 2007, 6, 9–10. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Injured (n = 35) | Non-Injured (n = 75) | t-test | Effect Size | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t-test | p | d (95%CI) | |
| Age (years) | 26.2 | 4.4 | 23.8 | 4.8 | 2.43 | 0.02 | 0.51 (0.11–0.92) |
| Experience in football (years) | 16.97 | 2.93 | 14.79 | 2.87 | 2.02 | 0.03 | 0.75 (0.34–1.16) |
| Playing time (min/game) | 67.11 | 7.03 | 58.98 | 8.98 | 4.23 | 0.01 | 0.96 (0.54–1.38) |
| Body height (cm) | 187.87 | 6.78 | 185.25 | 7.21 | 0.25 | 0.79 | 0.37 (−0.03–0.77) |
| Body mass (kg) | 78.99 | 7.51 | 79.00 | 6.25 | 0.01 | 0.99 | 0.01 (−0.4–0.40) |
| Body mass index (kg/m2) | 23.32 | 1.23 | 23.26 | 1.18 | 0.22 | 0.81 | 0.05 (−0.35–0.45) |
| CODS-ND (s) | 2.87 | 0.25 | 2.89 | 0.31 | 0.24 | 0.78 | 0.06 (−0.33–0.46) |
| CODS-D (s) | 2.74 | 0.2 | 2.76 | 0.39 | 0.3 | 0.74 | 0.06 (−0.34–0.46) |
| RAG-ND (s) | 3.15 | 0.20 | 2.94 | 0.24 | 2.47 | 0.02 | 0.92 (0.50–1.34) |
| RAG-D (s) | 3.08 | 0.19 | 2.94 | 0.25 | 2.03 | 0.04 | 0.66 (0.25–1.07) |
| SIT&REACH (cm) | 30.26 | 7.51 | 29.69 | 7.39 | 0.34 | 0.72 | 0.07 (−0.32–0.47) |
| MAXABD (cm) | 138.35 | 12.79 | 138.57 | 13.25 | 0.07 | 0.8 | 0.016 (−0.38–0.42) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mijatovic, D.; Krivokapic, D.; Versic, S.; Dimitric, G.; Zenic, N. Change of Direction Speed and Reactive Agility in Prediction of Injury in Football; Prospective Analysis over One Half-Season. Healthcare 2022, 10, 440. https://doi.org/10.3390/healthcare10030440
Mijatovic D, Krivokapic D, Versic S, Dimitric G, Zenic N. Change of Direction Speed and Reactive Agility in Prediction of Injury in Football; Prospective Analysis over One Half-Season. Healthcare. 2022; 10(3):440. https://doi.org/10.3390/healthcare10030440
Chicago/Turabian StyleMijatovic, Dragan, Dragan Krivokapic, Sime Versic, Goran Dimitric, and Natasa Zenic. 2022. "Change of Direction Speed and Reactive Agility in Prediction of Injury in Football; Prospective Analysis over One Half-Season" Healthcare 10, no. 3: 440. https://doi.org/10.3390/healthcare10030440
APA StyleMijatovic, D., Krivokapic, D., Versic, S., Dimitric, G., & Zenic, N. (2022). Change of Direction Speed and Reactive Agility in Prediction of Injury in Football; Prospective Analysis over One Half-Season. Healthcare, 10(3), 440. https://doi.org/10.3390/healthcare10030440