
Strengths and Weaknesses of Cancer Pain Management in Italy: Findings from a Nationwide SIAARTI Survey

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Participants
2.3. Statistical Analysis
3. Results
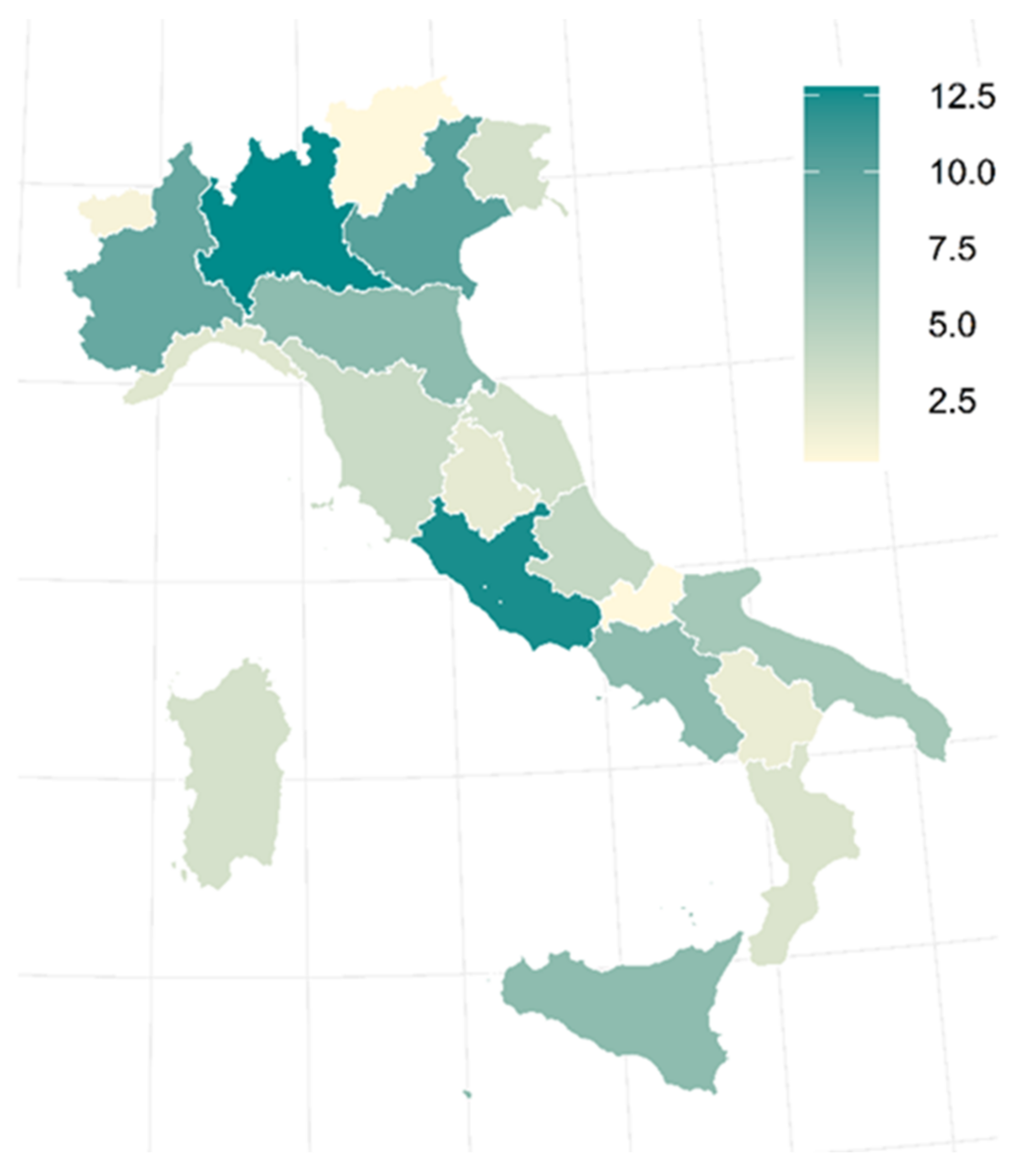
3.1. Demographics and Center Features
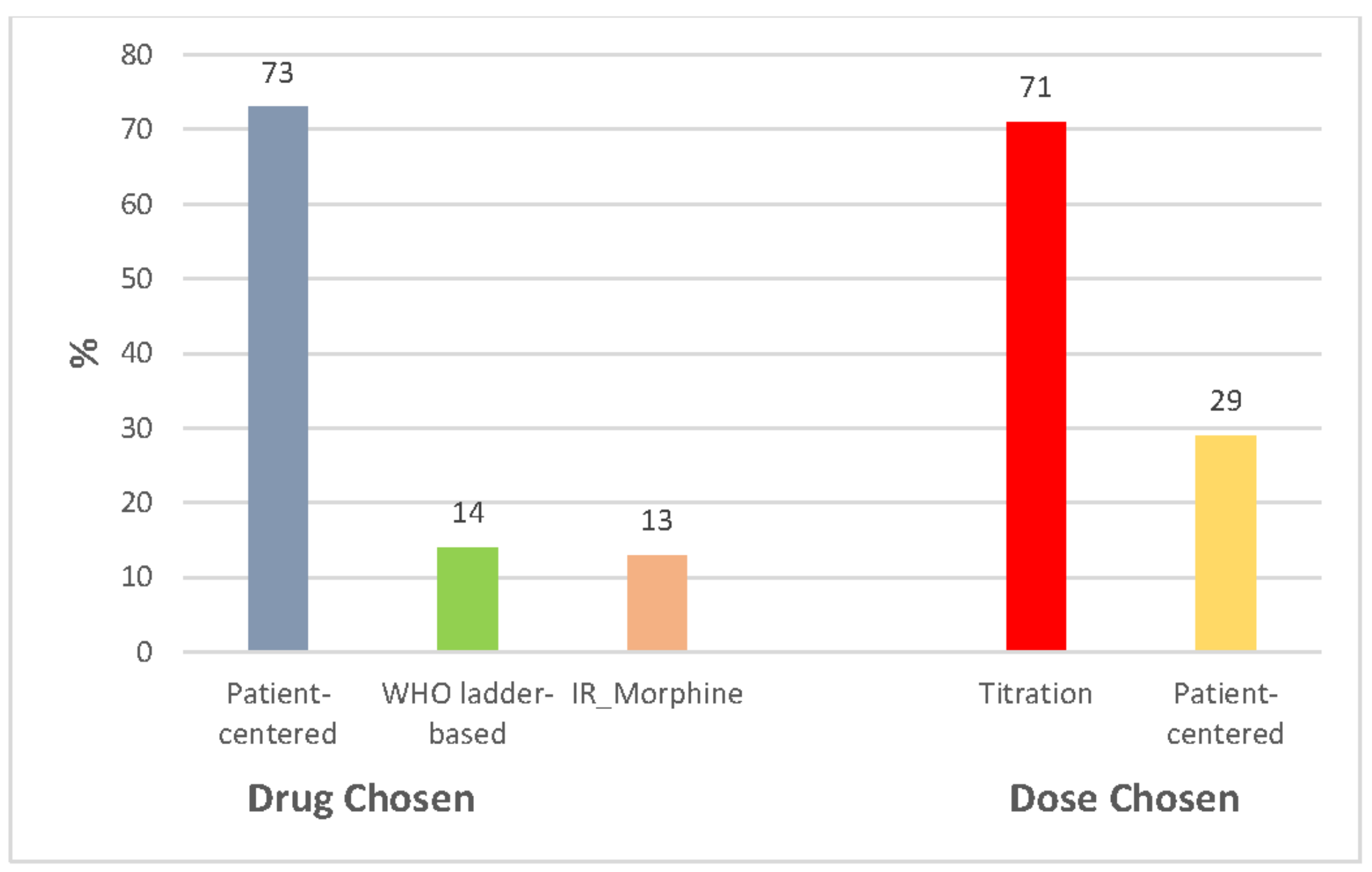
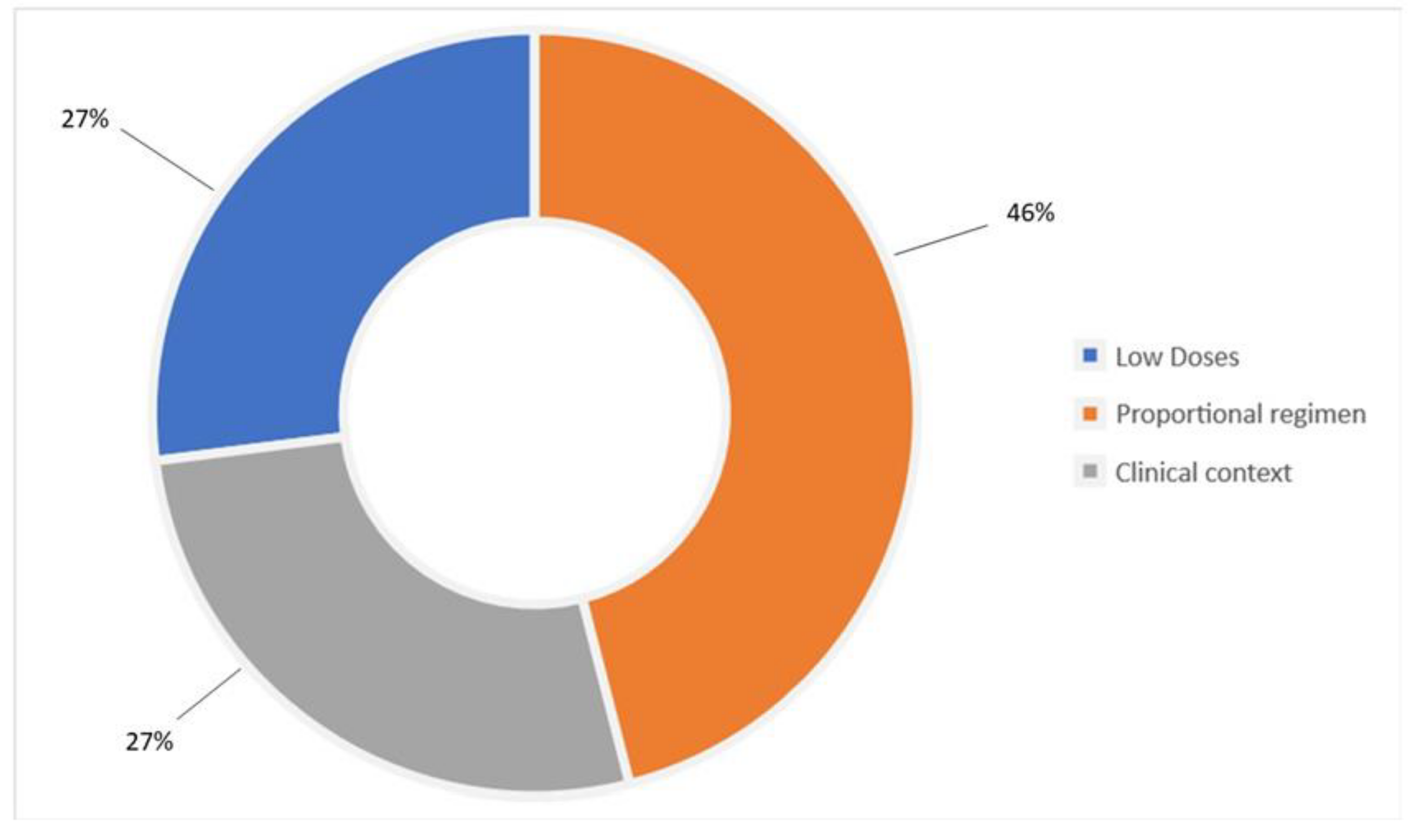
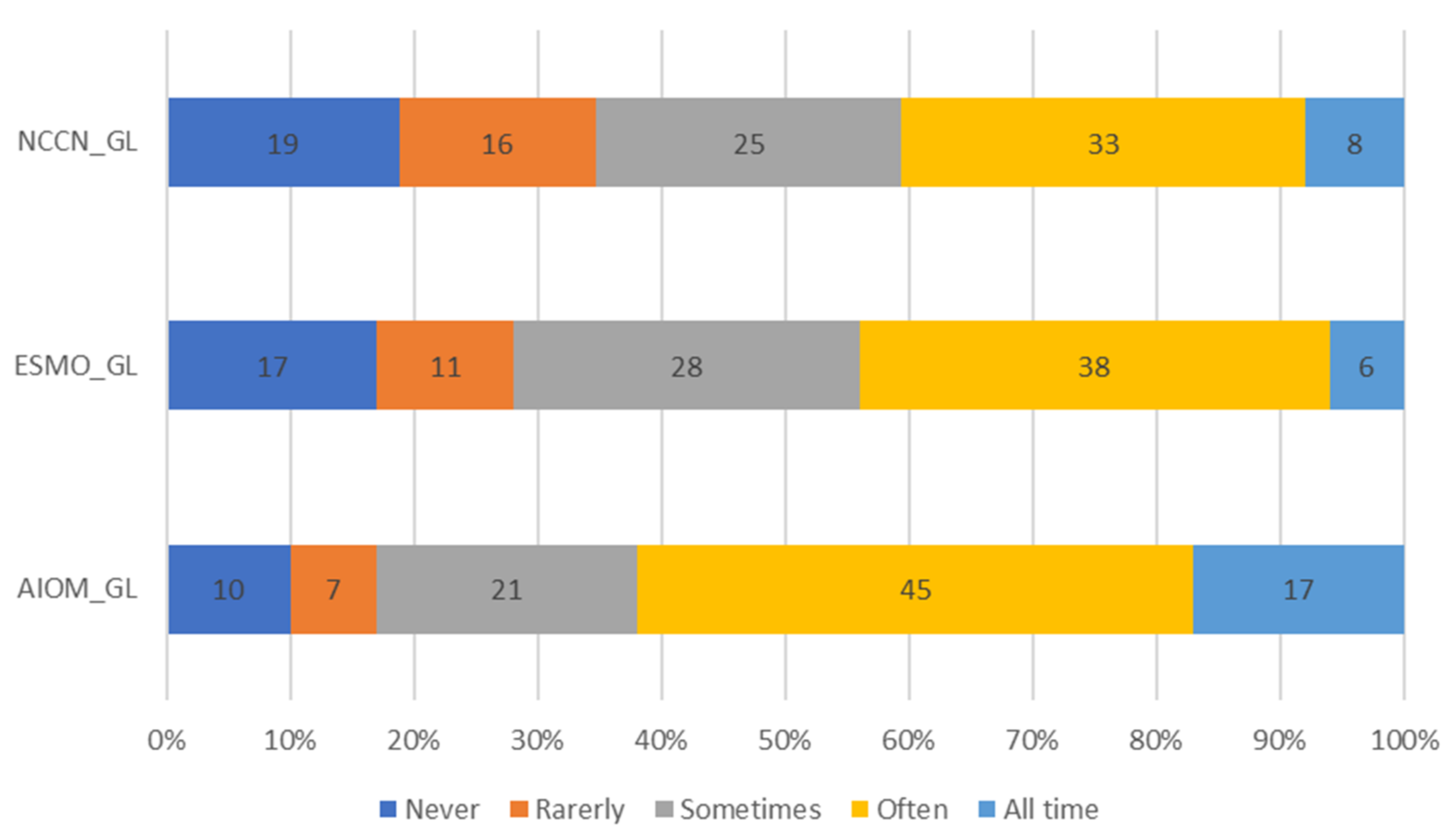
3.2. Strengths
3.3. Weaknesses
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I.; on behalf of the ESMO Guidelines Committee. Management of Cancer Pain in Adult Patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29 (Suppl. S4), iv166–iv191. [Google Scholar] [CrossRef] [PubMed]
- Swarm, R.A.; Paice, J.A.; Anghelescu, D.L.; Are, M.; Bruce, Y.B.; Buga, S.; Chwistek, M.; Cleeland, C.; Craig, D.; Gafford, E.; et al. Adult Cancer Pain, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 977–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents. Available online: https://www.who.int/publications/i/item/9789241550390 (accessed on 26 December 2021).
- Italian Association of Oncologistsd (AIOM). Lineguida sulla Terapia del Dolore in Oncologia [Guidelines on Cancer Pain Management]. Available online: https://www.aiom.it/linee-guida-aiom-terapia-del-dolore-in-oncologia-2019/ (accessed on 15 January 2022).
- Greco, M.T.; Roberto, A.; Corli, O.; Deandrea, S.; Bandieri, E.; Cavuto, S.; Apolone, G. Quality of cancer pain management: An update of a systematic review of undertreatment of patients with cancer. J. Clin. Oncol. 2014, 32, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Beuken-van Everdingen, M.H.; Hochstenbach, L.M.; Joosten, E.A.; Tjan-Heijnen, V.C.; Janssen, D.J. Update on Prevalence of Pain in Patients with Cancer: Systematic Review and Meta-Analysis. J Pain Symptom Manag. 2016, 51, 1070–1090.e9. [Google Scholar] [CrossRef] [Green Version]
- Van den Beuken-van Everdingen, M.H.; de Rijke, J.M.; Kessels, A.G.; Schouten, H.C.; van Kleef, M.; Patijn, J. Prevalence of pain in patients with cancer: A systematic review of the past 40 years. Ann. Oncol. 2007, 18, 1437–1449. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Farquhar-Smith, P. Pain in cancer survivors; filling in the gaps. Br. J. Anaesth. 2017, 119, 723–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasasbeh, M.A.M.; McCabe, C.; Payne, S. Cancer-related pain management: A review of knowledge and attitudes of healthcare professionals. Eur. J. Cancer Care 2017, 26, e12625. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, B.M.; Smith, C.B. Optimal pain management for patients with cancer in the modern era. CA Cancer J. Clin. 2018, 68, 182–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjermstad, M.J.; Fossa, S.D.; Bjordal, K.; Kaasa, S. Test/retest study of the European Organization for Research and Treatment of Cancer Core Quality-of-Life Questionnaire. J. Clin. Oncol. 1995, 13, 1249–1254. [Google Scholar] [CrossRef]
- Hui, D.; Bruera, E. The Edmonton Symptom Assessment System 25 Years Later: Past, Present, and Future Developments. J. Pain Symptom Manag. 2017, 53, 630–643. [Google Scholar] [CrossRef] [Green Version]
- Vittori, A.; Petrucci, E.; Cascella, M.; Innamorato, M.; Cuomo, A.; Giarratano, A.; Petrini, F.; Marinangeli, F. Pursuing the Recovery of Severe Chronic Musculoskeletal Pain in Italy: Clinical and Organizational Perspectives from a SIAARTI Survey. J Pain Res. 2021, 14, 3401–3410. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Miceli, L.; Cutugno, F.; Di Lorenzo, G.; Morabito, A.; Oriente, A.; Massazza, G.; Magni, A.; Marinangeli, F.; Cuomo, A.; et al. A Delphi Consensus Approach for the Management of Chronic Pain during and after the COVID-19 Era. Int. J. Environ. Res. Public Health 2021, 18, 13372. [Google Scholar] [CrossRef]
- Ventafridda, V.; Saita, L.; Ripamonti, C.; De Conno, F. WHO guidelines for the use of analgesics in cancer pain. Int. J. Tissue React. 1985, 7, 93–96. [Google Scholar] [PubMed]
- Stjernswärd, J.; Colleau, S.M.; Ventafridda, V. The World Health Organization cancer pain and palliative care program past, present, and future. J. Pain Symptom Manag. 1996, 12, 65–72. [Google Scholar] [CrossRef]
- Vargas-Schaffer, G. Is the WHO analgesic ladder still valid? Twenty-four years of experience. Can. Fam. Physician 2010, 56, 514–517. [Google Scholar] [PubMed]
- Liu, W.C.; Zheng, Z.X.; Tan, K.H.; Meredith, G.J. Multidimensional Treatment of Cancer Pain. Curr. Oncol. Rep. 2017, 19, 10. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, A.; Bimonte, S.; Forte, C.A.; Botti, G.; Cascella, M. Multimodal approaches and tailored therapies for pain management: The trolley analgesic model. J. Pain Res. 2019, 12, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Te Boveldt, N.; Vernooij-Dassen, M.; Leppink, I.; Samwel, H.; Vissers, K.; Engels, Y. Patient empowerment in cancer pain management: An integrative literature review. Psychooncology 2014, 23, 1203–1211. [Google Scholar] [CrossRef] [Green Version]
- Valenta, S.; Spirig, R.; Miaskowski, C.; Zaugg, K.; Spichiger, E. Testing a pain self-management intervention by exploring reduction of analgesics’ side effects in cancer outpatients and the involvement of family caregivers: A study protocol (PEINCA-FAM). BMC Nurs. 2018, 17, 54. [Google Scholar] [CrossRef] [Green Version]
- Davies, A.N.; Elsner, F.; Filbet, M.J.; Porta-Sales, J.; Ripamonti, C.; Santini, D.; Webber, K. Breakthrough cancer pain (BTcP) management: A review of international and national guidelines. BMJ Support. Palliat. Care 2018, 8, 241–249. [Google Scholar] [CrossRef]
- Mercadante, S.; Lazzari, M.; Reale, C.; Cuomo, A.; Fusco, F.; Marchetti, P.; Mediati, R.; Vhiurazzi, B.; Ciuffedra, L.; Caraceni, A.; et al. Italian Oncological Pain Survey (IOPS): A multicentre Italian study of breakthrough pain performed in different settings. Clin. J. Pain 2015, 31, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camps Herrero, C.; Batista, N.; Díaz Fernández, N.; Escobar Álvarez, Y.; Gonzalo Gómez, A.; Isla Casado, D.; Salud, A.; Terrasa Pons, J.; Guillem Porta, V. Breakthrough cancer pain: Review and calls to action to improve its management. Clin. Transl. Oncol. 2020, 22, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, A.; Cascella, M.; Forte, C.A.; Bimonte, S.; Esposito, G.; De Santis, S.; Cavanna, L.; Fusco, F.; Dauri, M.; Natoli, S.; et al. Careful Breakthrough Cancer Pain Treatment through Rapid-Onset Transmucosal Fentanyl Improves the Quality of Life in Cancer Patients: Results from the BEST Multicenter Study. J. Clin. Med. 2020, 9, 1003. [Google Scholar] [CrossRef] [Green Version]
- Ndoro, S. Effective multidisciplinary working: The key to high-quality care. Br. J. Nurs. 2014, 23, 724–727. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Cascella, M.; Marinangeli, F.; Vittori, A.; Scala, C.; Piccinini, M.; Braga, A.; Miceli, L.; Vellucci, R. Open Issues and Practical Suggestions for Telemedicine in Chronic Pain. Int. J. Environ. Res. Public Health 2021, 18, 12416. [Google Scholar] [CrossRef] [PubMed]
- Petrucci, E.; Vittori, A.; Cascella, M.; Vergallo, A.; Fiore, G.; Luciani, A.; Pizzi, B.; Degan, G.; Fineschi, V.; Marinangeli, F. Litigation in Anesthesia and Intensive Care Units: An Italian Retrospective Study. Healthcare 2021, 9, 1012. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inadequate Training Level |
|---|
| Quality of life evaluation |
| Underuse of opioid pain medications |
| Underuse of non-pharmacological pain strategies |
| Barriers that preclude adequate treatment (e.g., fear of opioid addiction) |
| Poor patient compliance (e.g., communication barriers) |
| Lack of professional collaboration (multi-professional/interdisciplinary) |
| Insufficient attention to the diagnosis of specific pain conditions |
| Patient/healthcare provider partnerships |
| Respondents (n = 611) | |
|---|---|
| M/F (n) | 306/305 |
| Age (Mean ± SD) | 51.2 (±10.9) |
| Expertise | |
| PS Junior ^ | 29 (5%) |
| PS Senior ° | 18 (3%) |
| Specialist; <40 years | 73 (12%) |
| 41–50 years | 171 (28%) |
| >50 years | 322 (53%) |
| Work activity (%) | |
| Dedicated pain therapist | 22 |
| Anesthesiologist with partial activity as a pain therapist | 40 |
| ICU physician with partial activity as a pain therapist | 13 |
| Oncologist | 3 |
| Radiotherapist | 4 |
| Other | 17 |
| Health facility (%) | |
| Hospital/university | 78 |
| Home palliative care | 3 |
| Research centers | 13 |
| Outpatient territorial clinic | 2 |
| Hospice | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascella, M.; Vittori, A.; Petrucci, E.; Marinangeli, F.; Giarratano, A.; Cacciagrano, C.; Tizi, E.S.; Miceli, L.; Natoli, S.; Cuomo, A. Strengths and Weaknesses of Cancer Pain Management in Italy: Findings from a Nationwide SIAARTI Survey. Healthcare 2022, 10, 441. https://doi.org/10.3390/healthcare10030441
Cascella M, Vittori A, Petrucci E, Marinangeli F, Giarratano A, Cacciagrano C, Tizi ES, Miceli L, Natoli S, Cuomo A. Strengths and Weaknesses of Cancer Pain Management in Italy: Findings from a Nationwide SIAARTI Survey. Healthcare. 2022; 10(3):441. https://doi.org/10.3390/healthcare10030441
Chicago/Turabian StyleCascella, Marco, Alessandro Vittori, Emiliano Petrucci, Franco Marinangeli, Antonino Giarratano, Cristina Cacciagrano, Emiliano Simone Tizi, Luca Miceli, Silvia Natoli, and Arturo Cuomo. 2022. "Strengths and Weaknesses of Cancer Pain Management in Italy: Findings from a Nationwide SIAARTI Survey" Healthcare 10, no. 3: 441. https://doi.org/10.3390/healthcare10030441
APA StyleCascella, M., Vittori, A., Petrucci, E., Marinangeli, F., Giarratano, A., Cacciagrano, C., Tizi, E. S., Miceli, L., Natoli, S., & Cuomo, A. (2022). Strengths and Weaknesses of Cancer Pain Management in Italy: Findings from a Nationwide SIAARTI Survey. Healthcare, 10(3), 441. https://doi.org/10.3390/healthcare10030441