
Digital Contact Tracing and COVID-19: Design, Deployment, and Current Use in Italy


Abstract
:1. Introduction
- (a)
- Contact identification,
- (b)
- Contact listing, and
- (c)
- Contact follow-up.
2. The Digital Contact Tracing: Design, Deployment, and Current Use
3. The Italian National App, “Immuni”, for Digital Contact Tracing: The Running-In and the Initiatives Supporting the Diffusion
4. Deployment and Current Use of the App, “Immuni”
5. Discussion and Conclusions
5.1. Our Contributions
5.2. The Limits in the Deployment and the Current Use of DCT in Italy
5.3. The Impact of the Digital Divide
5.4. Factors Influencing Adoption of the App Based on the Literature
- The limits of the proximity tracing
- High levels of compliance with standards of data privacy are limiting
- High level of integration of functions could improve the use
- Some works are moving towards the definition of protocols for the correct identification of the factors [44].
- Some authors have focused on the desirable requirements that a DCT app must have to be successful and have made them explicit [14].
- Other authors went to the field to review the reports on the app stores relating to these apps [8] to understand what the users were not satisfied with.
5.5. Final Reflections and Further Work
- There is very low-certainty evidence that DCT may produce more reliable counts of contacts and reduce time to complete contact tracing.
- Stronger primary research on the effectiveness of contact tracing technologies is needed.
- Future studies should better consider the access, acceptability, and equity.
- Studies should focus on the relationships between acceptability of DCT and the impact of the privacy that can hamper the diffusion of this technology.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | Contact tracing |
| DCT | Digital contact tracing |
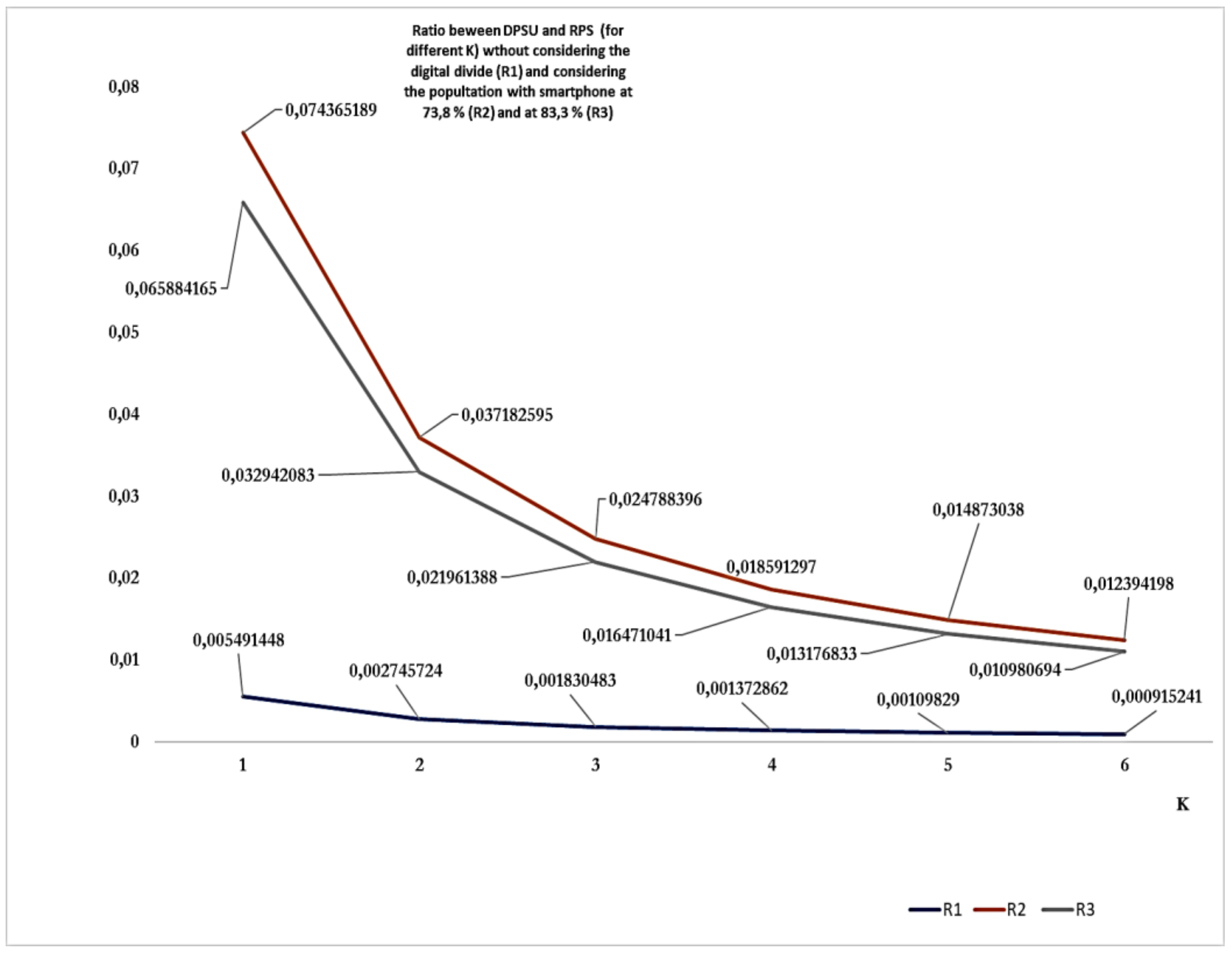
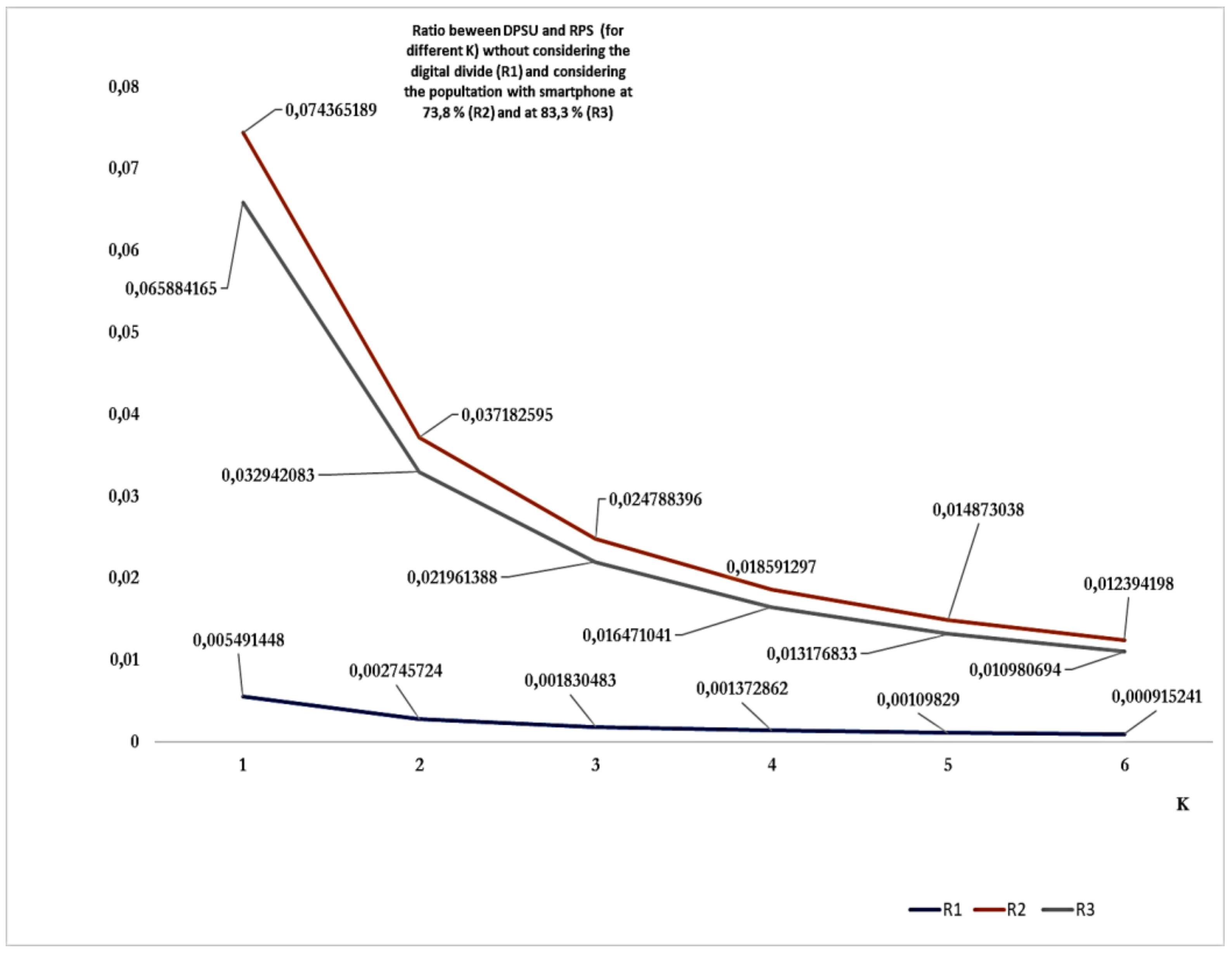
| RPS | Really positive subjects |
| DPS | Diagnosed positive subjects |
| DPSU | Diagnosed positive subjects uploaded |
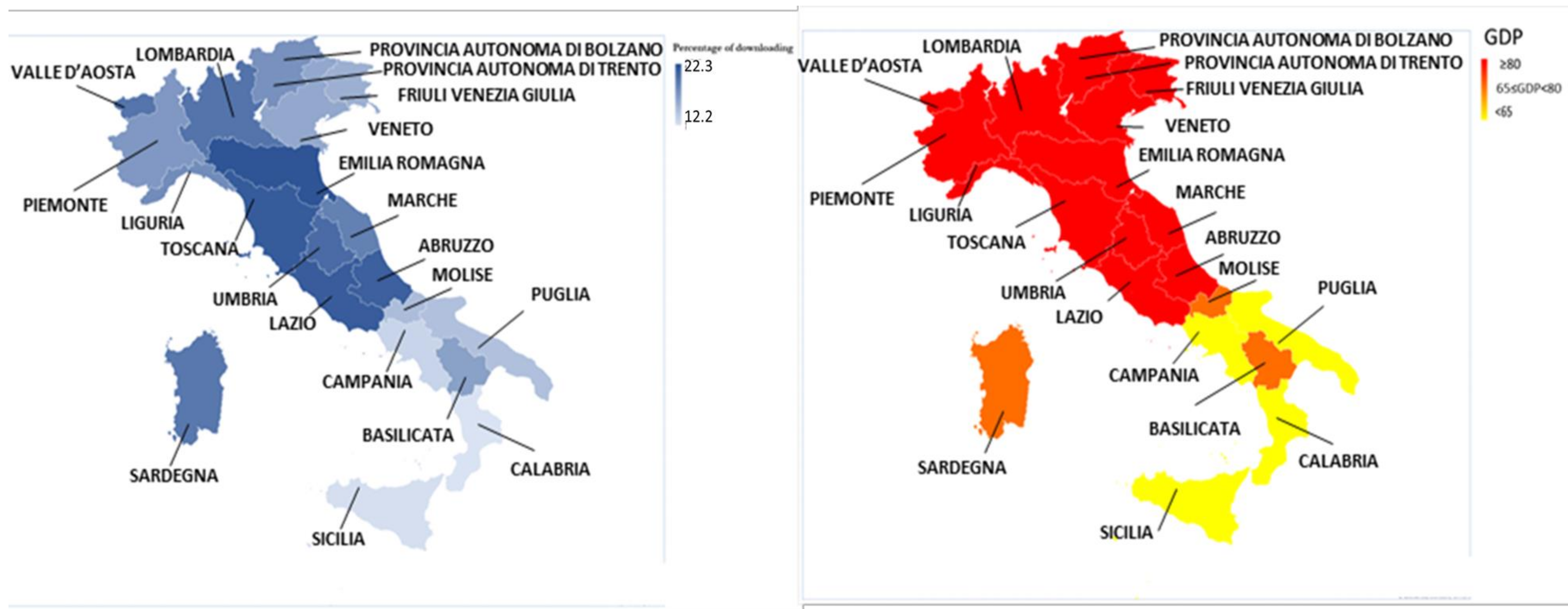
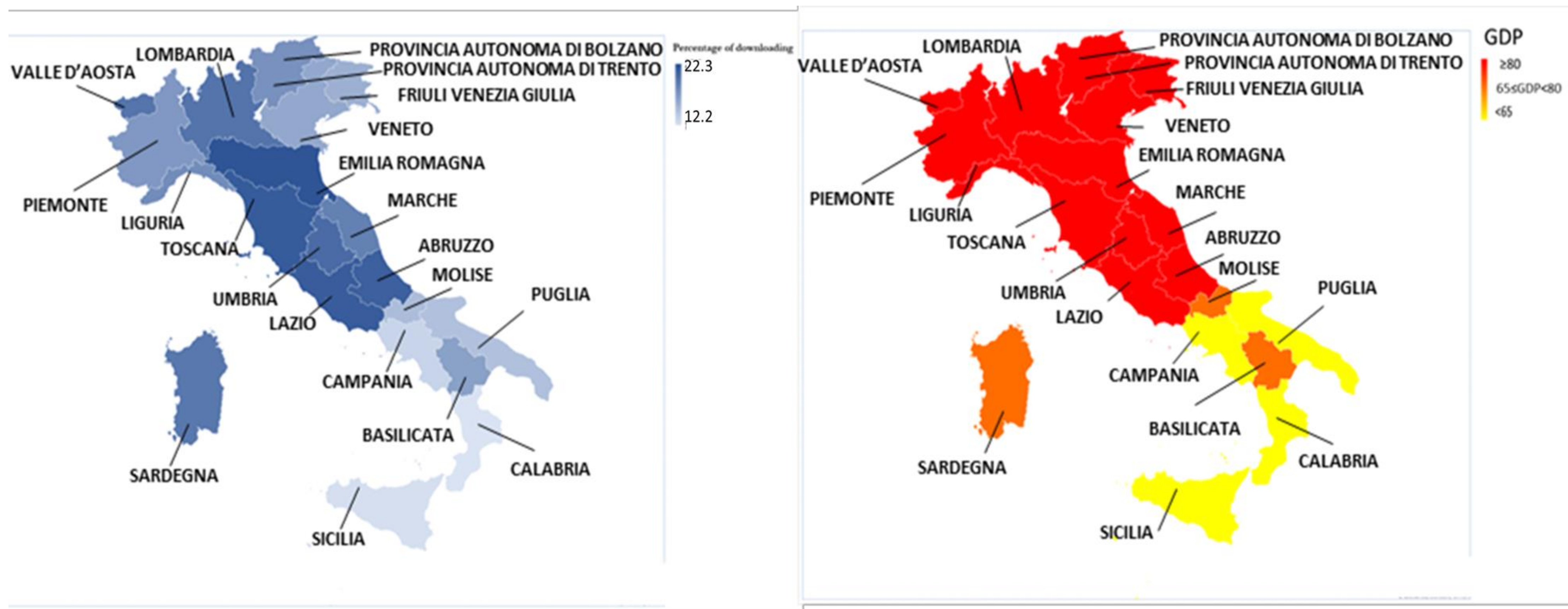
| %D | Percent of downloads |
| GDP | Gross domestic product per capita |
References
- WHO. Contact Tracing during an Outbreak of Ebola Virus Disease. Available online: https://www.who.int/csr/resources/publications/ebola/contact-tracing-during-outbreak-of-ebola.pdf (accessed on 30 December 2021).
- The Brief History of Smartphones. Available online: https://www.thoughtco.com/history-of-smartphones-4096585 (accessed on 15 December 2021).
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dörner, L.; Parker, M.; Bonsall, D.G.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368, eabb6936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, F. COVID-19 and Health Code: How Digital Platforms Tackle the Pandemic in China. Soc. Media + Soc. 2020, 6, 2056305120947657. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, R.A.; Merkel, C. Digital contact tracing for COVID-19. CMAJ 2020, 192, E653–E656. [Google Scholar] [CrossRef] [PubMed]
- Iribarren, S.J.; Schnall, R.; Stone, P.W.; Carballo-Diéguez, A. Smartphone Applications to Support Tuberculosis Prevention and Treatment: Review and Evaluation. JMIR Mhealth Uhealth 2016, 4, e25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruscher, C.; Werber, D.; Thoulass, J.; Zimmermann, R.; Eckardt, M.; Winter, C.; Sagebiel, D. Dating apps and websites as tools to reach anonymous sexual contacts during an outbreak of hepatitis A among men who have sex with men, Berlin, 2017. Euro Surveill 2019, 24, 1800460. [Google Scholar] [CrossRef] [PubMed]
- Garousi, V.; Cutting, D.; Felderer, M. Mining user reviews of COVID contact-tracing apps: An exploratory analysis of nine European apps. J. Syst. Softw. 2021, 184, 111136. [Google Scholar] [CrossRef] [PubMed]
- Elkhodr, M.; Mubin, O.; Iftikhar, Z.; Masood, M.; Alsinglawi, B.; Shahid, S.; Alnajjar, F. Technology, Privacy, and User Opinions of COVID-19 Mobile Apps for Contact Tracing: Systematic Search and Content Analysis. J. Med. Internet Res. 2021, 23, e23467. [Google Scholar] [CrossRef] [PubMed]
- Dp-3/Documents. Available online: https://github.com/DP-3T/documents (accessed on 15 December 2021).
- Pan European Privacy-Preserving Proximity Tracing. Available online: https://github.com/pepp-pt (accessed on 15 December 2021).
- Alanzi, T. A Review of Mobile Applications Available in the App and Google Play Stores Used During the COVID-19 Outbreak. J. Multidiscip. Healthc. 2021, 14, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Kahnbach, L.; Lehr, D.; Brandenburger, J.; Mallwitz, T.; Jent, S.; Hannibal, S.; Funk, B.; Janneck, M. Quality and Adoption of COVID-19 Tracing Apps and Recommendations for Development: Systematic Interdisciplinary Review of European Apps. J. Med. Internet Res. 2021, 23, e27989. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.; Abbas, M.; Beecham, S.; Buckley, J.; Chochlov, M.; Fitzgerald, B.; Glynn, L.; Johnson, K.; Laffey, J.; McNicholas, B.; et al. Best Practice Guidance for Digital Contact Tracing Apps: A Cross-disciplinary Review of the Literature. JMIR Mhealth Uhealth 2021, 9, e27753. [Google Scholar] [CrossRef] [PubMed]
- Immuni. Available online: https://www.immuni.italia.it/ (accessed on 15 December 2021).
- MID—Sottogruppo di Lavoro 6. Report Sulle Attività Svolte dal Sottogruppo di Lavoro Impegnato Nell’individuazione di “Tecnologie per il Governo Dell’emergenza” (in Particolare Contact-Tracing) Mediante Valutazione di 319 Soluzioni Tecnologiche Pervenute con Call for Contribution dal 24 al 26 Marzo; Ministero della Innovazione Tecnologica e della Digitalizzazione: Rome, Italy, 2020. Available online: https://innovazione.gov.it/assets/docs/SGdL6%20-%20Relazione.pdf (accessed on 30 December 2021).
- Immuni Documentation. Available online: https://github.com/immuni-app/immuni-documentation (accessed on 15 December 2021).
- Rapporti Covid in italiano. Available online: https://www.iss.it/rapporti-covid-19 (accessed on 15 December 2021).
- Rapporti Covid in inglese. Available online: https://www.iss.it/rapporti-iss-covid-19-in-english (accessed on 15 December 2021).
- Filia, A.; Urdiales, A.M.; Rota, M.C. Guida per la ricerca e gestione dei contatti (contact tracing) dei casi di COVID-19. In Versione del 25 Giugno 2020; Rapporto ISS COVID-19, n. 53/2020; Istituto Superiore di Sanità: Rome, Italy, 2020. [Google Scholar]
- ISS Bioethics COVID-19 Working Group. Digital Support for Contact Tracing during the Pandemic: Ethical and Governance Considerations; Version of September 17, 2020, Rapporto ISS COVID-19 n. 59/2020—English version; Istituto Superiore di Sanità: Rome, Italy, 2020.
- Giansanti, D.; D’Avenio, G.; Rossi, M.; Spurio, A.; Bertinato, L.; Grigioni, M. Technologies Supporting Proximity Detection: Reflections for Citizens, Professionals and Stakeholders in the COVID-19 Era; Version of October 29, 2020, Rapporto ISS COVID-19 n. 54/2020 Rev.—English version; Istituto Superiore di Sanità: Rome, Italy, 2020.
- Emergenza Epidemiologica COVID-19: Elementi per il Contact Tracing. Available online: https://www.eduiss.it/pluginfile.php/544990/course/summary/165F20_Programma%20senza%20firme%20%28psicologi%29.pdf (accessed on 15 December 2021).
- Web Immuni. Immuni-Dashboard-Data/Dati/Andamento-Download.csv. Available online: https://github.com/immuni-app/immuni-dashboard-data/blob/master/dati/andamento-download.csv (accessed on 15 December 2021).
- WeB GITHUB. Immuni-Dashboard-Data/Dati/Andamento-Dati-Nazionali.csv. Available online: https://github.com/immuni-app/immuni-dashboard-data/blob/master/dati/andamento-dati-nazionali.csv (accessed on 15 December 2021).
- Web Immuni. The Numbers of Immune. Available online: https://www.immuni.italia.it/dashboard.html (accessed on 15 December 2021).
- Web Tuttitalia.it. Popolazione per età, sesso e stato civile 2021. Available online: https://www.tuttitalia.it/statistiche/popolazione-eta-sesso-stato-civile-2021/ (accessed on 15 December 2021).
- Web Lab. Coronavirus, la situazione in Italia. Available online: https://lab.gedidigital.it/gedi-visual/2020/coronavirus-i-contagi-in-italia/ (accessed on 15 December 2021).
- Web Istat. Indagine sierologica su Covid-19 condotta da Ministero della Salute e Istat. Available online: https://www.istat.it/it/archivio/242676 (accessed on 15 December 2021).
- Web Itatt. PRIMI RISULTATI DELL’INDAGINE DI SIEROPREVALENZA SUL SARS-CoV-2. Available online: https://www.istat.it/it/files/2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 15 December 2021).
- Web Censis. I Media Digitali e la fine Dello Star System. Available online: https://www.censis.it/comunicazione/i-media-digitali-e-la-fine-dello-star-system (accessed on 15 December 2021).
- Web Censis. I Media dopo la Pandemia. Available online: https://www.censis.it/comunicazione/i-media-dopo-la-pandemia-1 (accessed on 15 December 2021).
- Web GitHub. Available online: https://user-images.githubusercontent.com/7631137/97900742-65047900-1d3b-11eb-9d0f-67f20ce73398.png (accessed on 15 December 2021).
- Web GitHub. Download per Regione #4. Available online: https://github.com/immuni-app/immuni-dashboard-data/issues/4 (accessed on 15 December 2021).
- Web Ansa. Pil Bolzano sopra la media Ue, Calabria la peggiore d’Italia. Available online: https://www.ansa.it/europa/notizie/la_tua_europa/notizie/2021/03/03/pil-bolzano-sopra-la-media-ue-calabria-la-peggiore-ditalia_57a18efa-5918-4fb4-80fe-9763b36783b9.html (accessed on 15 December 2021).
- Web Eurostat. Regional GDP per Capita Ranged from 32% to 260% of the EU Average in 2019. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20210303-1 (accessed on 15 December 2021).
- Maccari, L.; Cagno, V. Do we need a contact tracing app? Comput. Commun. 2021, 166, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Neter, E.; Brainin, E.; Baron-Epel, O. Group differences in health literacy are ameliorated in ehealth literacy. Health Psychol. Behav. Med. 2021, 9, 480–497. [Google Scholar] [CrossRef] [PubMed]
- van Deursen, A.J.; van Dijk, J.A. The first-level digital divide shifts from inequalities in physical access to inequalities in material access. New Media Soc. 2019, 21, 354–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giansanti, D.; Veltro, G. The Digital Divide in the Era of COVID-19: An Investigation into an Important Obstacle to the Access to the mHealth by the Citizen. Healthcare 2021, 9, 371. [Google Scholar] [CrossRef] [PubMed]
- Partecipa al Cashback con L’app, IO. Available online: https://io.italia.it/cashback/ (accessed on 18 August 2021).
- Ansa IT Economia. Available online: https://www.ansa.it/bannernews/notizie/breaking_news_eco/2020/12/18/-manovraun-cellulare-per-1-anno-con-isee-sotto-20mila-euro-_14e1c456-f1f4-4630-9cc5-ff8ab26d596c.html (accessed on 18 August 2021).
- Kolasa, K.; Mazzi, F.; Leszczuk-Czubkowska, E.; Zrubka, Z.; Péntek, M. State of the Art in Adoption of Contact Tracing Apps and Recommendations Regarding Privacy Protection and Public Health: Systematic Review. JMIR Mhealth Uhealth 2021, 9, e23250. [Google Scholar] [CrossRef] [PubMed]
- Oyibo, K.; Sahu, K.S.; Oetomo, A.; Morita, P.P. Factors Influencing the Adoption of Contact Tracing Applications: Protocol for a Systematic Review. JMIR Res. Protoc. 2021, 10, e28961. [Google Scholar] [CrossRef] [PubMed]
- Anglemyer, A.; Moore, T.H.; Parker, L.; Chambers, T.; Grady, A.; Chiu, K.; Parry, M.; Wilczynska, M.; Flemyng, E.; Bero, L. Digital contact tracing technologies in epidemics: A rapid review. Cochrane Database Syst. Rev. 2020, 8, CD013699. [Google Scholar] [CrossRef] [PubMed]
- Salomon, J.A.; Reinhart, A.; Bilinski, A.; Chua, E.J.; La Motte-Kerr, W.; Rönn, M.; Reitsma, M.; Morris, K.A.; LaRocca, S.; Farag, T.; et al. The U.S. COVID-19 Trends and Impact Survey, 2020–2021: Continuous real-time measurement of COVID-19 symptoms, risks, protective behaviors, testing and vaccination. MedRxiv 2021. [Google Scholar] [CrossRef]
- Smith, S.A.; Whitehead, M.S.; Sheats, J.; Mastromonico, J.; Yoo, W.; Coughlin, S.S. A Community-engaged approach to developing a mobile cancer prevention App: The mCPA Study Protocol. JMIR Res. Protoc. 2016, 5, e34. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Description | Sources (Direct or Indirect) | Reference and Year |
|---|---|---|
| Statistics on people owning smartphones in Italy. | CENSIS (Italian national body designated for social research) reports | N. 31 (2019), N. 32 (2021) |
| Statistics on the use of the app “Immuni” (downloading, uploading of diagnosed positive subjects, etc.) | GitHub and app “Immuni” Webs | N. 15–17, N. 24–26, N. 33–34 (*) |
| Statistics on gross domestic product per capita (GDP) | Eurostat (European body designed for European statistics) reports | N. 35–36(Updated 3 march 2021) |
| Statistics on Italian population | ISTAT (Italian national body designated for social research) reports | N. 27 (*) |
| Serological investigation on COVID-19In Italy | ISTAT (Italian national body designated for social research) reports | N. 28–29 (2021) |
| Statistics on COVID-19 in Italy | Data from Italian Ministry of health | N. 28 (*) |
| Region | Percent of Downloads for Each Region | GDP |
|---|---|---|
| Abruzzo | 21.5 | GDP ≥ 80 |
| Basilicata | 16.9 | 65 ≤ GDP < 80 |
| Calabria | 12.2 | GDP < 65 |
| Campania | 13.3 | GDP < 65 |
| Emilia-Romagna | 22.3 | GDP ≥ 80 |
| Friuli Venezia Giulia | 15.8 | GDP ≥ 80 |
| Lazio | 21.7 | GDP ≥ 80 |
| Liguria | 18.3 | GDP ≥ 80 |
| Lombardia | 20.1 | GDP ≥ 80 |
| Marche | 19.2 | GDP ≥ 80 |
| Molise | 14.9 | 65 ≤ GDP < 80 |
| Piemonte | 17.5 | GDP ≥ 80 |
| Puglia | 14.6 | GDP < 65 |
| Sardegna | 19.8 | 6 ≤GDP < 80 |
| Sicilia | 12.5 | GDP < 65 |
| Toscana | 21.8 | GDP ≥ 80 |
| Provincia autonoma di Trento | 19.4 | GDP ≥ 80 |
| Provincia autonoma di Bolzano | 16.7 | GDP ≥ 80 |
| Umbria | 20.7 | GDP ≥ 80 |
| Valle d’Aosta | 20.0 | GDP ≥ 80 |
| Veneto | 16.4 | GDP ≥ 80 |
| Ref | Cited Article | Brief Description of the Focus |
|---|---|---|
| [8] | Garousi V, Cutting D, Felderer M. Mining user reviews of COVID contact-tracing apps: An exploratory analysis of nine European apps. J Syst Softw. 2021 | Authors went to the field to review the referees relating to these apps to understand what the users were not satisfied with. |
| [9] | Elkhodr M, Mubin O, Iftikhar Z, Masood M, Alsinglawi B, Shahid S, Alnajjar F. Technology, Privacy, and User Opin-ions of COVID-19 Mobile Apps for Contact Tracing: Systematic Search and Content Analysis. J Med Internet Res. 2021 Feb 9;23(2):e23467. doi: 10.2196/23467. PMID: 33493125; PMCID: PMC7879719 Nov 4:111136. doi: 10.1016/j.jss.2021.111136. Epub ahead of print. PMID:34751198; PMCID: PMC8566091 | Reviewed different apps for DCT, highlighted that the app, “Immuni”, is one of the apps with the greatest respect for privacy, with a very low amount of data collected. |
| [12] | Alanzi T. A Review of Mobile Applications Available in the App and Google Play Stores Used During the COVID-19 Outbreak. J Multidiscip Healthc. 2021 Jan 12;14:45–57. doi: 10.2147/JMDH.S285014. PMID: 33469298; PMCID: PMC7812813 | Highlighted that a large integration of functionalities are lacking in the apps developed for the COVID-19. |
| [13] | Kahnbach L, Lehr D, Brandenburger J, Mallwitz T, Jent S, Hannibal S, Funk B, Janneck M. Quality and Adoption of COVID-19 Tracing Apps and Recommendations for Development: Systematic Interdisciplinary Review of European Apps. J Med Internet Res. 2021 Jun 2;23(6):e27989. doi: 10.2196/27989. PMID: 33890867; PMCID: PMC8174558 | The study faced the quality in the apps for DCT. It used the mobile app rating scale to assess the app quality. |
| [14] | O’Connell J, Abbas M, Beecham S, Buckley J, Chochlov M, Fitzgerald B, Glynn L, Johnson K, Laffey J, McNicholas B, Nuseibeh B, O’Callaghan M, O’Keeffe I, Razzaq A, Rekanar K, Richardson I, Simpkin A, Storni C, Tsvyatkova D, Walsh J, Welsh T, O’Keeffe D. Best Practice Guidance for Digital Contact Tracing Apps: A Cross-disciplinary Review of the Literature. JMIR Mhealth Uhealth. 2021 Jun 7;9(6):e27753. doi: 10.2196/27753. PMID: 34003764; PMCID: PMC8189288 | Authors reviewed the desiderable requirements that a DCT app must have to be successful and have made them explicit. |
| [37] | Maccari L, Cagno V. Do we need a contact tracing app? Comput Commun. 2021 Jan 15;166:9–18. doi: 10.1016/j.comcom.2020.11.007. Epub 2020 Nov 19. PMID:33235399; PMCID: PMC7676320 | It has been underlined that the proximity detection using BLTE gave a low contribute to the detection of cases. |
| [43] | .Kolasa K, Mazzi F, Leszczuk-Czubkowska E, Zrubka Z, Péntek M. State of the Art in Adoption of Contact Tracing Apps and Recommendations Regarding Privacy Protection and Public Health: Systematic Review. JMIR Mhealth Uhealth. 2021 Jun 10;9(6):e23250. doi: 10.2196/23250. PMID: 34033581; PMCID: PMC8195202 | Showed that apps with high levels of compliance with standards of data privacy (and “Immuni” is one of them) tend to fulfill public health interests to a limited extent and DCT with a lower level of data privacy protection allow for the collection of more data. |
| [44] | Oyibo K, Sahu KS, Oetomo A, Morita PP. Factors Influencing the Adoption of Contact Tracing Applications: Protocol for a Systematic Review. JMIR Res Protoc. 2021 Jun 1;10(6):e28961. doi: 10.2196/28961. PMID: 33974551; PMCID: PMC8171387 | The study proposed protocols for the correct identification of the factors influencing DCT. |
| [45] | Anglemyer A, Moore TH, Parker L, Chambers T, Grady A, Chiu K, Parry M, Wilczynska M, Flemyng E, Bero L. Digital contact tracing technologies in epidemics: a rapid review. Cochrane Database Syst Rev. 2020 Aug 18;8(8):CD013699. doi: 10.1002/14651858.CD013699. PMID: 33502000; PMCID:PMC8241885 | The study on the Cochrane database system review traced both the reflections and the future directions and efforts in DCT. The outcome from randomized controlled trials (RCTs), cluster-RCTs, quasi-RCTs, cohort studies, cross-sectional studies, and modeling studies in general populations was considered. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scrivano, N.; Gulino, R.A.; Giansanti, D. Digital Contact Tracing and COVID-19: Design, Deployment, and Current Use in Italy. Healthcare 2022, 10, 67. https://doi.org/10.3390/healthcare10010067
Scrivano N, Gulino RA, Giansanti D. Digital Contact Tracing and COVID-19: Design, Deployment, and Current Use in Italy. Healthcare. 2022; 10(1):67. https://doi.org/10.3390/healthcare10010067
Chicago/Turabian StyleScrivano, Noemi, Rosario Alfio Gulino, and Daniele Giansanti. 2022. "Digital Contact Tracing and COVID-19: Design, Deployment, and Current Use in Italy" Healthcare 10, no. 1: 67. https://doi.org/10.3390/healthcare10010067
APA StyleScrivano, N., Gulino, R. A., & Giansanti, D. (2022). Digital Contact Tracing and COVID-19: Design, Deployment, and Current Use in Italy. Healthcare, 10(1), 67. https://doi.org/10.3390/healthcare10010067