1. Introduction
The trend in population aging has been formed in developed countries and is either taking shape in developing countries or has yet to be formed. However, this trend is inevitable worldwide. At present, China is facing the dual pressure of deep aging and rapid urbanization [
1]. According to the statistics of the seventh population census, in 2020 the number of people over 60 years of age in China reached 264 million, accounting for 18.7% of the total population, and the number of people aged 65 and over reached 190 million, accounting for 13.5% of the total population [
2]. It is expected that China will become an aging society in 2022, and that by the 2060s the population of over 65-year-olds will be close to its peak, with roughly one in every three Chinese being over 65 years old, accounting for 33%. It will be a deeply aging society [
3].
The first country to propose the concept of medical and elderly care was the United Kingdom. In the 1960s, the notion of integrating medical with elderly care in the UK appeared. With a view to “reducing costs, improving quality, and putting service first”, “integrated care” was regarded as an economic elderly care service model, ranging from the management of the elderly stage to the close management of different age stages, and from managing the patient himself to the family and social support systems [
4]. With the increase in China’s elderly population, ensuring their health has become a challenge for families. The aging of the population is becoming more and more serious, and the demand for the elderly service industry is becoming more and more great. However, the development of China’s elderly care service industry started late and there are still many problems. With regards building a better elderly care service model, due to the current shortage of pension resources, the state has launched the pension model of institutional pensions, home care, pension real estate, and other aspects. However, the traditional pension services can no longer meet the growing needs of the elderly [
5]. Majorly developing the integrated undertakings and industries of medical and elderly care is an inevitable choice to cope with the problems of an aging society [
6]. The number of elderly people in China’s medical security system is increasing, which has a far-reaching impact on social and economic development. Therefore, from the perspective of the combination of medical care and nursing, we should give full attention to the function of family old-age security and improve the functions of community medical treatment, rehabilitation, and nursing [
7].
Since 2013, China has promulgated a series of policies related to the integration of medical with elderly care, which has promoted the high-quality development of integrated medical and elderly care services [
8]. Improving the overall health level is of great significance and can improve the health level of the elderly. The search found that as of 24 September 2020, a total of 180 “integrated medical and nursing care” documents have been issued [
8]. When it comes to building an elderly care service system in China, there exists a contradiction between the need for healthy aging and the imbalance and insufficient supply of medical and elderly care resources [
9]. The policy response to resolve this local contradiction in the present era is to integrate medical and health resources with elderly care service resources to provide high-quality integrated medical and elderly care services for all the elderly [
10]. At present, from a policy perspective China has a home-based, community-based, and institution-supplemented nursing care system. Not only has the number of policies specifically aimed at integrating medical with nursing care gradually increased, but also the number of policies that mention the integration of medical with nursing care in terms of content has gradually increased [
11]. The old service model and the community–home–medical–elderly care integrated service serve the elderly living in the community and at home by providing them with comprehensive, economical, and convenient, sustainable health and elderly care services. Their simple service supply and broad population coverage have become one of the mainstream forms of the medical and elderly care service model, which is theoretically more in line with the concept of healthy aging. Compared with professional elderly care service institutions, community homes allow the elderly’s families to take residence as the properties. For the elderly, staying in a suitable elderly care environment such as in the community or with family has positive significance for extending the lives and social relationships of the elderly and improving the overall health level [
12]. The “combination of medical and nursing care” model is suitable for implementation in elderly care communities, elderly care institutions, nursing institutions, and medical and health institutions, and is a new type of old-age security service model that effectively combines medical service technology with the old-age insurance model to improve the utilization rate of medical resources and improve the quality of old-age services, thereby greatly improving the quality of life of the elderly and realizing “treatment with diseases and recuperation without diseases” [
13].
Western developed countries have explored the needs of the elderly for old-age care and medical services since the 20th century. A relatively mature old-age medical service system has been established so far [
14]. The integration of medical with elderly care is developed on the basis of long-term care, which refers to the healthy elderly care model of providing life care services, health management services, and medical care services for the elderly through the integration of medical treatment with old-age care [
15]. An efficient integrated care system is a complete chain including care recipients, care providers, managers, care delivery sites, care content, coordination of various functional departments, etc., and is an organic whole in which all departments work together [
16,
17].
In the future, it is inevitable that China will become a deep aging population and that the country will face the severe challenge of aging. With the rapid development of today’s economy and the increasing improvement of people’s living standards, it is proposed that “the combination of medical health and elderly care services is a long-term plan to actively cope with the aging of the population, which is conducive to meeting the growing multi-level and diversified demand for health and elderly care services of the people” [
4,
18]. In the future, the use of new technologies to help elderly care institutions will be strengthened. The four major tasks of elderly care include healthy aging, active aging, successful aging, and productive aging. With the development of the times, intelligent elderly care has emerged; especially in the post-epidemic era, intelligent and intelligent elderly care services are particularly important. This is also the development trend of China’s medical and oxygen integration [
19]. In this context, the combination of medical care and nursing care is emerging and will become increasingly important [
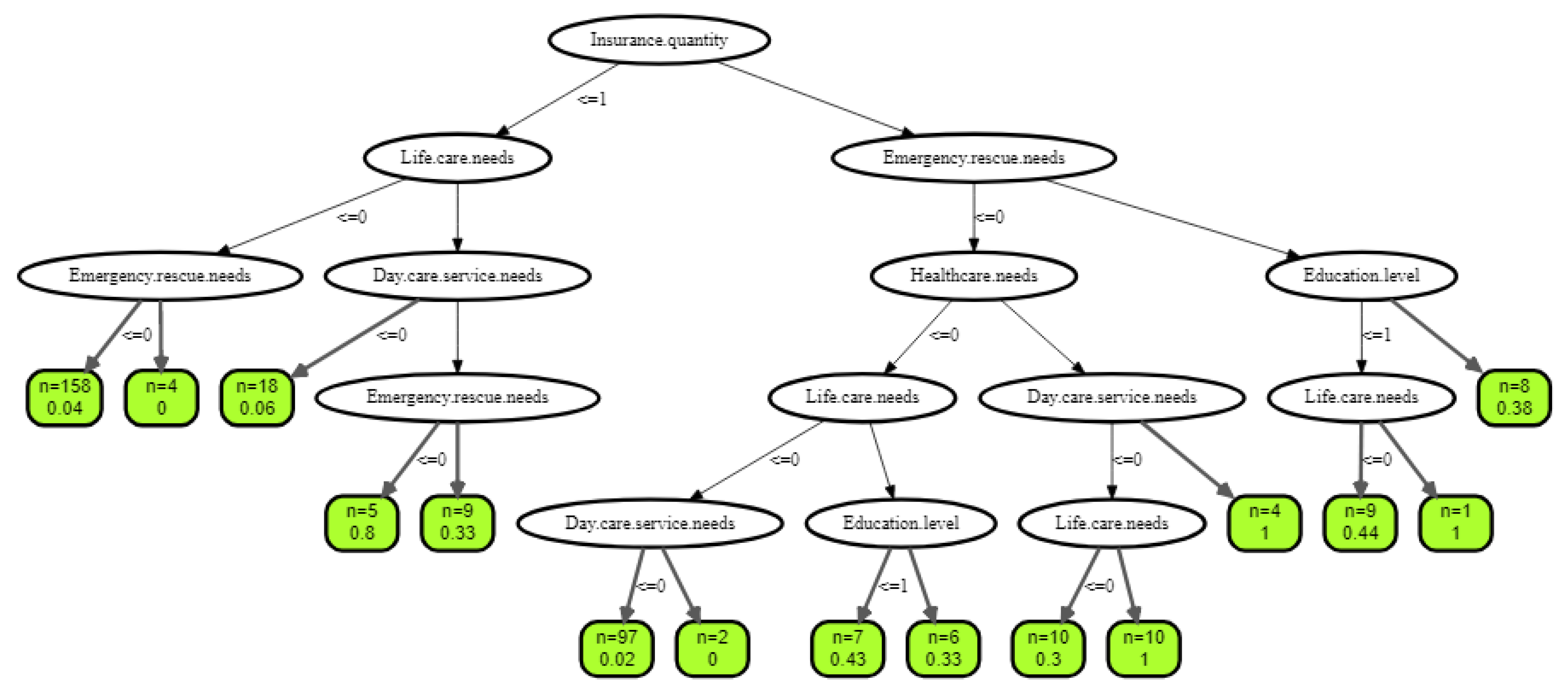
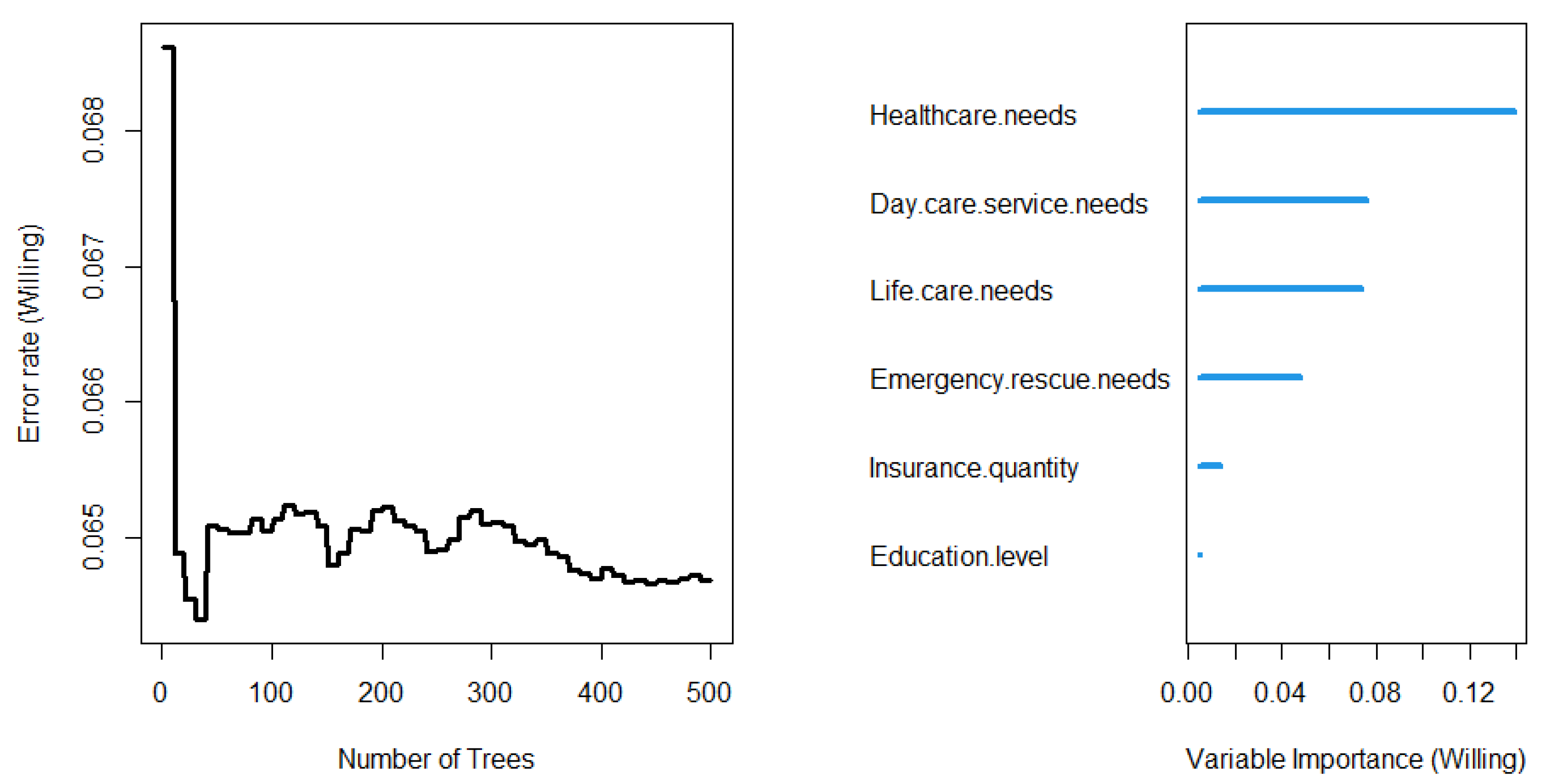
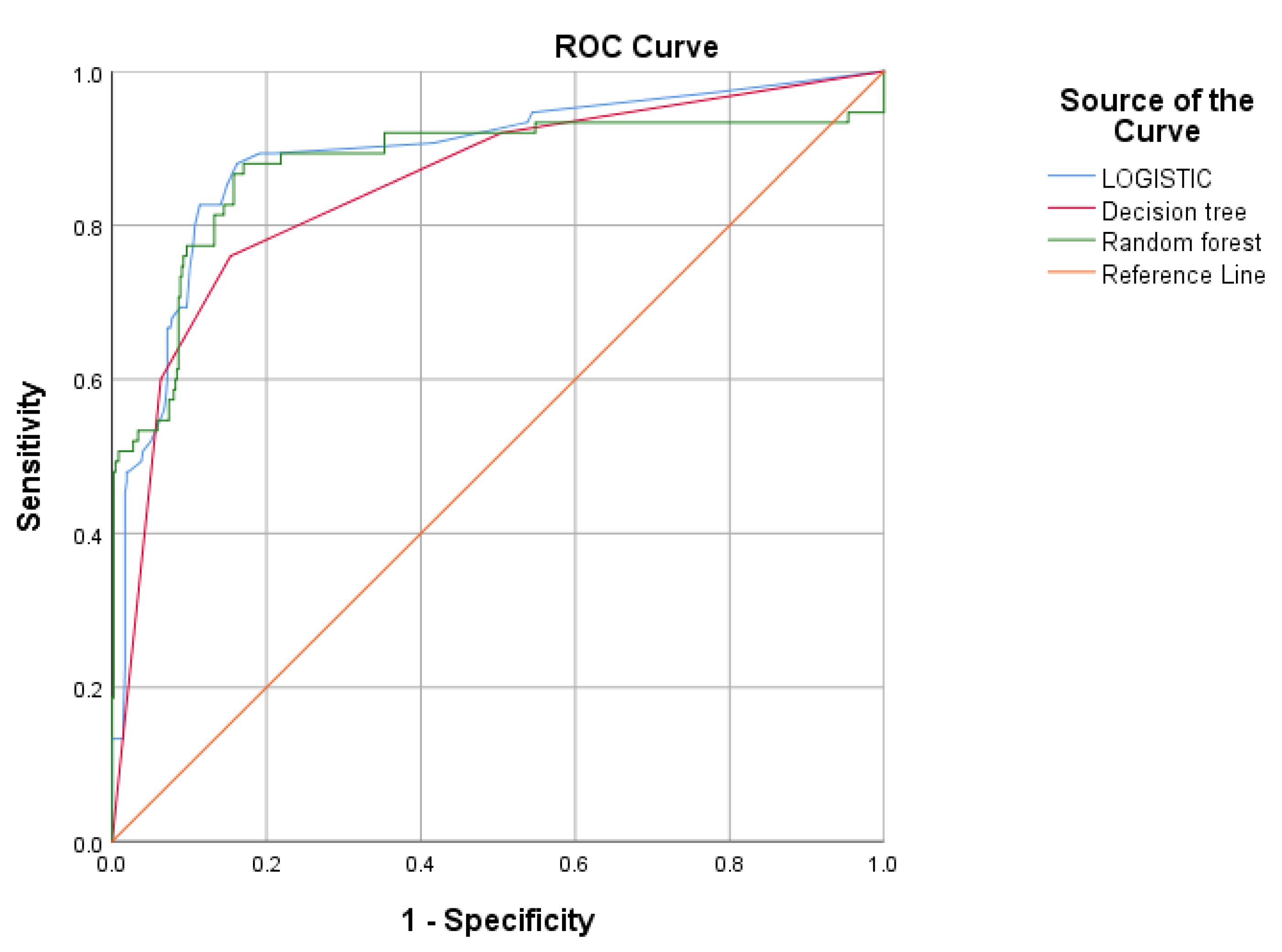
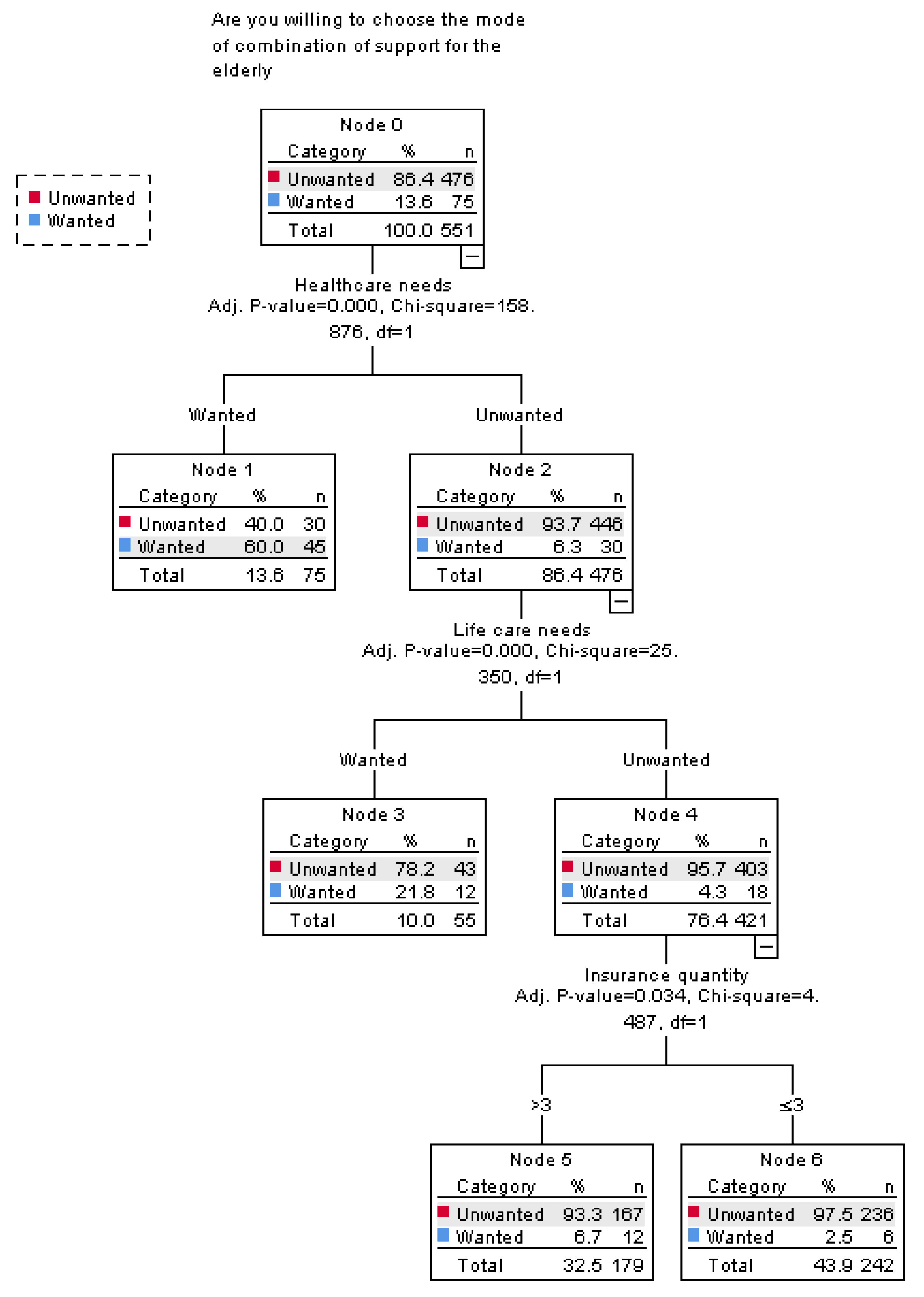
20]. At present, some studies have been conducted on this issue, but they have only scratched the surface and have not explored in depth the reasons and factors that influence the willingness of elderly people to accept this model, nor have they provided good solutions to improve the implementation of this model. In order to better serve the elderly, we conducted a survey on the elderly aged 60 and above in Tangshan by means of questionnaires based on Andersen’s behavior model. We analyzed the factors that affected the attitude of the elderly to community healthcare and elderly care services through logical regression model, decision tree model, and random forest model. We hope that the results of this study can provide a basis for continuous improvement of community medical and nursing services and make them the best choice for the elderly.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}