
Multiplex Social Network Analysis to Understand the Social Engagement of Patients in Online Health Communities


Abstract
:1. Introduction
2. Literature Review
2.1. Social Network Theory
2.1.1. Network Structural Effects
2.1.2. Actor Attribute Effects
2.2. Multiplex Social Network
3. Methods
3.1. Research Context and Data Collection
3.2. Exponential Random Graph Models
- represents the probability of the network variable X taking the observed value x;
- A defines the network configurations that are patterns of social network ties assumed to represent underlying social processes or mechanisms of network tie formation;
- is the summation over all different configuration types in the model;
- is the network statistic corresponding to the network configuration of type A;
- is the parameter corresponding to the configuration of type A;
- is a normalizing constant to ensure that the sum of probabilities in Equation (1) over all possible x equals 1; that is,
- Q is a network configuration of type Q comprising tie variables that are conditionally dependent given the rest of the network;
- is a joint attribute-network configuration comprising tie variables as well as nodal attribute variables;
- are sufficient statistics representing the network endogenous effects;
- is the vector of parameters corresponding to the graph statistics without nodal attributes;
- are sufficient statistics for the interactions between the network and nodal attributes;
- is the vector of parameters corresponding to the graph statistics representing the interaction between network tie variables and nodal attributes .
4. Results
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Rains, S.A.; Peterson, E.B.; Wright, K.B. Communicating Social Support in Computer-mediated Contexts: A Meta-analytic Review of Content Analyses Examining Support Messages Shared Online among Individuals Coping with Illness. Commun. Monogr. 2015, 82, 403–430. [Google Scholar] [CrossRef]
- Leimeister, J.M.; Schweizer, K.; Leimeister, S.; Krcmar, H. Do virtual communities matter for the social support of patients? Inf. Technol. People 2013, 21, 350–374. [Google Scholar] [CrossRef]
- Coulson, N.S.; Bullock, E.; Rodham, K. Exploring the Therapeutic Affordances of Self-Harm Online Support Communities: An Online Survey of Members. JMIR Ment. Health 2017, 4, e44. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Mo, X.; Liu, S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int. J. Med. Inform. 2014, 83, 210–224. [Google Scholar] [CrossRef]
- Dickerson, S.S. Women’s Use of the Internet: What Nurses Need to Know. J. Obstet. Gynecol. Neonatal Nurs. 2010, 35, 151–156. [Google Scholar] [CrossRef]
- Bi, Q.; Shen, L.; Evans, R.; Zhang, Z.; Dai, W. Determining the Topic Evolution and Sentiment Polarity for Albinism in a Chinese Online Health Community: Machine Learning and Social Network Analysis. JMIR Med. Inform. 2020, 8, e17813. [Google Scholar] [CrossRef]
- Ziebland, S.; Chapple, A.; Dumelow, C.; Evans, J.; Rozmovits, L. How the internet affects patients’ experience of cancer: A qualitative study. BMJ 2004, 328, 564. [Google Scholar] [CrossRef]
- Swan, M. Emerging Patient-Driven Health Care Models: An Examination of Health Social Networks, Consumer Personalized Medicine and Quantified Self-Tracking. Int. J. Environ. Res. Public Health 2009, 6, 492–525. [Google Scholar] [CrossRef]
- Eijk, M.V.D.; Faber, M.J.; Aarts, J.W.; Kremer, J.A.; Bloem, B.R. Using Online Health Communities to Deliver Patient-Centered Care to People With Chronic Conditions. J. Med. Internet Res. 2013, 15, e115. [Google Scholar] [CrossRef]
- Willis, E. The making of expert patients: The role of online health communities in arthritis self-management. J. Health Psychol. 2013, 19, 1613–1625. [Google Scholar] [CrossRef]
- Ma, D.; Zuo, M.; Liu, L. The Information Needs of Chinese Family members of Cancer Patients in the Online Health Community: What and Why? Inf. Process. Manag. 2021, 58, 102517. [Google Scholar] [CrossRef]
- Wang, T.-H.; Zhou, X.-F.; Ni, Y.; Pan, Z.-G. Health information needs regarding diabetes mellitus in China: An internet-based analysis. BMC Public Health 2020, 20, 990. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wu, Y.; Liu, J.; Li, J.; Zhang, P. Understanding Health Care Social Media Use From Different Stakeholder Perspectives: A Content Analysis of an Online Health Community. J. Med. Internet Res. 2017, 19, e109. [Google Scholar] [CrossRef] [PubMed]
- Little, M.; Wicks, P.; Vaughan, T.; Pentland, A. Quantifying Short-Term Dynamics of Parkinson’s Disease Using Self-Reported Symptom Data From an Internet Social Network. J. Med. Internet Res. 2013, 15, e20. [Google Scholar] [CrossRef]
- Eichhorn, K.C. Soliciting and Providing Social Support Over the Internet: An Investigation of Online Eating Disorder Support Groups. J. Comput. Mediat. Commun. 2008, 14, 67–78. [Google Scholar] [CrossRef]
- Nath, C.; Huh, J.; Adupa, A.K.; Jonnalagadda, S.R. Website Sharing in Online Health Communities: A Descriptive Analysis. J. Med. Internet Res. 2016, 18, e11. [Google Scholar] [CrossRef]
- Buis, L.R. Emotional and Informational Support Messages in an Online Hospice Support Community. Comput. Inform. Nurs. CIN 2008, 26, 358. [Google Scholar] [CrossRef]
- Park, A.; Conway, M. Longitudinal Changes in Psychological States in Online Health Community Members: Understanding the Long-Term Effects of Participating in an Online Depression Community. J. Med. Internet Res. 2017, 19, e71. [Google Scholar] [CrossRef]
- Wang, L.W.; Liu, X.; Li, J. The Establishment of Friendship Ties in the Online Health Forum Based on Exponential Random Graph Model. In Proceedings of the 2016 Pacific Asia Conference on Information Systems, Chiayi City, Taiwan, 27 June–1 July 2016. [Google Scholar]
- Li, Y.; Yan, X. How Could Peers in Online Health Community Help Improve Health Behavior. Int. J. Environ. Res. Public Health 2020, 17, 2995. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, K.; Street, N. Analyzing and Predicting User Participations in Online Health Communities: A Social Support Perspective. J. Med. Internet Res. 2017, 19, e130. [Google Scholar] [CrossRef]
- Stewart Loane, S.; Webster, C.M.; D’Alessandro, S. Identifying Consumer Value Co-created through Social Support within Online Health Communities. J. Macromarketing 2014, 35, 353–367. [Google Scholar] [CrossRef]
- Dang-Pham, D.; Pittayachawan, S.; Bruno, V. Applying network analysis to investigate interpersonal influence of information security behaviours in the workplace. Inf. Manag. 2017, 54, 625–637. [Google Scholar] [CrossRef]
- Robins, G.; Snijders, T.; Wang, P.; Handcock, M.; Pattison, P. Recent developments in exponential random graph (p*) models for social networks. Soc. Netw. 2007, 29, 192–215. [Google Scholar] [CrossRef]
- Robins, G.; Pattison, P.; Kalish, Y.; Lusher, D. An introduction to exponential random graph (p*) models for social networks. Soc. Netw. 2007, 29, 173–191. [Google Scholar] [CrossRef]
- Caimo, A.; Gollini, I. A multilayer exponential random graph modelling approach for weighted networks. Comput. Stat. Data Anal. 2020, 142, 106825. [Google Scholar] [CrossRef]
- Koskinen, J.; Broccatelli, C.; Wang, P.; Robins, G. Bayesian analysis of ERG models for multilevel, multiplex, and multilayered networks with sampled or missing data. In New Statistical Developments in Data Science; Springer Proceedings in Mathematics & Statistics; Springer: Berlin/Heidelberg, Germany, 2019; Volume 288, pp. 105–117. [Google Scholar]
- Todd, N.R.; Blevins, E.J.; Yi, J. A Social Network Analysis of Friendship and Spiritual Support in a Religious Congregation. Am. J. Community Psychol. 2019, 65, 107–124. [Google Scholar] [CrossRef]
- Lusher, D.; Koskinen, J.; Robins, G. Exponential Random Graph Models for Social Networks: Theory, Methods and Applications; Cambridge University Press: Cambridge, UK, 2013. [Google Scholar]
- Xu, R.; Zhang, Q. Understanding Online Health Groups for Depression: Social Network and Linguistic Perspectives. J. Med. Internet Res. 2016, 18, e63. [Google Scholar] [CrossRef]
- Yang, H.; Du, H.S.; Wang, L.; Wu, T. The Influence of Social Support Networks on Health Conditions Via User Engagement: Gender as a Moderator. J. Electron. Commer. Res. 2019, 20, 35–54. [Google Scholar]
- Thompson, A.E.; Anisimowicz, Y.; Miedema, B.; Hogg, W.; Wodchis, W.P.; Aubrey-Bassler, K. The influence of gender and other patient characteristics on health care-seeking behaviour: A QUALICOPC study. BMC Fam. Pract. 2016, 17, 38. [Google Scholar] [CrossRef]
- Chai, S.; Das, S.; Rao, H.R. Factors Affecting Bloggers’ Knowledge Sharing: An Investigation Across Gender. J. Manag. Inf. Syst. 2014, 28, 309–342. [Google Scholar] [CrossRef]
- Lieberman, M.A. Gender and online cancer support groups: Issues facing male cancer patients. J. Cancer Educ. Off. J. Am. Assoc. Cancer Educ. 2008, 23, 167–171. [Google Scholar]
- Matud, M.P. Gender differences in stress and coping styles. Personal. Individ. Differ. 2004, 37, 1401–1415. [Google Scholar] [CrossRef]
- Mackenzie, C.S.; Gekoski, W.L.; Knox, V.J. Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging Ment. Health 2006, 10, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Ding, H.; Li, Z. Does Internet Use Impact the Health Status of Middle-Aged and Older Populations? Evidence from China Health and Retirement Longitudinal Study (CHARLS). Int. J. Environ. Res. Public Health 2022, 19, 3619. [Google Scholar] [CrossRef] [PubMed]
- Setoyama, Y.; Yamazaki, Y.; Namayama, K. Benefits of Peer Support in Online Japanese Breast Cancer Communities: Differences Between Lurkers and Posters. J. Med. Internet Res. 2011, 13, e122. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Y. Exploring the User Interaction Network in an Anxiety Disorder Online Community: An Exponential Random Graph Model with Topical and Emotional Effects. Int. J. Environ. Res. Public Health 2022, 19, 6354. [Google Scholar] [CrossRef]
- Nambisan, P. Information seeking and social support in online health communities: Impact on patients’ perceived empathy. J. Am. Med. Inform. Assoc. 2011, 18, 298–304. [Google Scholar] [CrossRef]
- Lu, Y.; Luo, S.; Liu, X. Development of Social Support Networks by Patients With Depression Through Online Health Communities: Social Network Analysis. JMIR Med. Inform. 2021, 9, e24618. [Google Scholar] [CrossRef]
- Mustafa, S.; Zhang, W. Why Do I Share? Participants’ Personality Traits and Online Participation. Int. J. Hum.–Comput. Interact. 2023; 1–19. [Google Scholar] [CrossRef]
- Yan, L.; Tan, Y. Feeling Blue? Go Online: An Empirical Study of Social Support Among Patients. Inf. Syst. Res. 2014, 25, 690–709. [Google Scholar] [CrossRef]
- Song, X.; Yan, X.; Li, Y. Modelling liking networks in an online healthcare community: An exponential random graph model analysis approach. J. Inf. Sci. 2014, 41, 89–96. [Google Scholar] [CrossRef]
- Batenburg, A.; Das, E. Emotional Approach Coping and the Effects of Online Peer-Led Support Group Participation Among Patients With Breast Cancer: A Longitudinal Study. J. Med. Internet Res. 2014, 16, e256. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T. Understanding users’ participation in online health communities: A social capital perspective. Inf. Dev. 2019, 36, 403–413. [Google Scholar] [CrossRef]
- Kim, H.-S.; Shyam Sundar, S. Can online buddies and bandwagon cues enhance user participation in online health communities? Comput. Hum. Behav. 2014, 37, 319–333. [Google Scholar] [CrossRef]
- Heaney, M.T. Multiplex networks and interest group influence reputation: An exponential random graph model. Soc. Netw. 2014, 36, 66–81. [Google Scholar] [CrossRef]
- Krivitsky, P.N.; Coletti, P.; Hens, N. A Tale of Two Datasets: Representativeness and Generalisability of Inference for Samples of Networks. J. Am. Stat. Assoc. 2022, 1–11. [Google Scholar] [CrossRef]
- Bianchi, F.; Casnici, N.; Squazzoni, F. Solidarity as a byproduct of professional collaboration: Social support and trust in a coworking space. Soc. Netw. 2018, 54, 61–72. [Google Scholar] [CrossRef]
- Krivitsky, P.N.; Koehly, L.; Marcum, C.S. Exponential-Family Random Graph Models for Multi-Layer Networks. Psychometrika 2020, 85, 630–659. [Google Scholar] [CrossRef]
- Lusher, D.; Robins, G.; Pattison, P.E.; Lomi, A. “Trust Me”: Differences in expressed and perceived trust relations in an organization. Soc. Netw. 2012, 34, 410–424. [Google Scholar] [CrossRef]
- Liu, X.; Sun, M.; Li, J. Research on gender differences in online health communities. Int. J. Med. Inform. 2018, 111, 172–181. [Google Scholar] [CrossRef]
- Chung, J.E. Social Networking in Online Support Groups for Health: How Online Social Networking Benefits Patients. J. Health Commun. 2013, 19, 639–659. [Google Scholar] [CrossRef]
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Sinha, A.; Porter, T.; Wilson, A. The Use of Online Health Forums by Patients With Chronic Cough: Qualitative Study. J. Med. Internet Res. 2018, 20, e19. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Deng, Z.; Chen, X. Knowledge sharing motivations in online health communities: A comparative study of health professionals and normal users. Comput. Hum. Behav. 2017, 75, 797–810. [Google Scholar] [CrossRef]
- Blei, D.M.; Ng, A.Y.; Jordan, M.I. Latent Dirichlet Allocation. J. Mach. Learn. Res. 2003, 3, 993–1022. [Google Scholar]
- Hirsch, J.E. An index to quantify an individual’s scientific research output. Proc. Natl. Acad. Sci. USA 2005, 102, 16569–16572. [Google Scholar] [CrossRef] [PubMed]
- Pattison, D.P.; Wasserman, S. Logit models and logistic regressions for social networks: II. Multivariate relations. Br. J. Math. Stat. Psychol. 1999, 52, 169–193. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
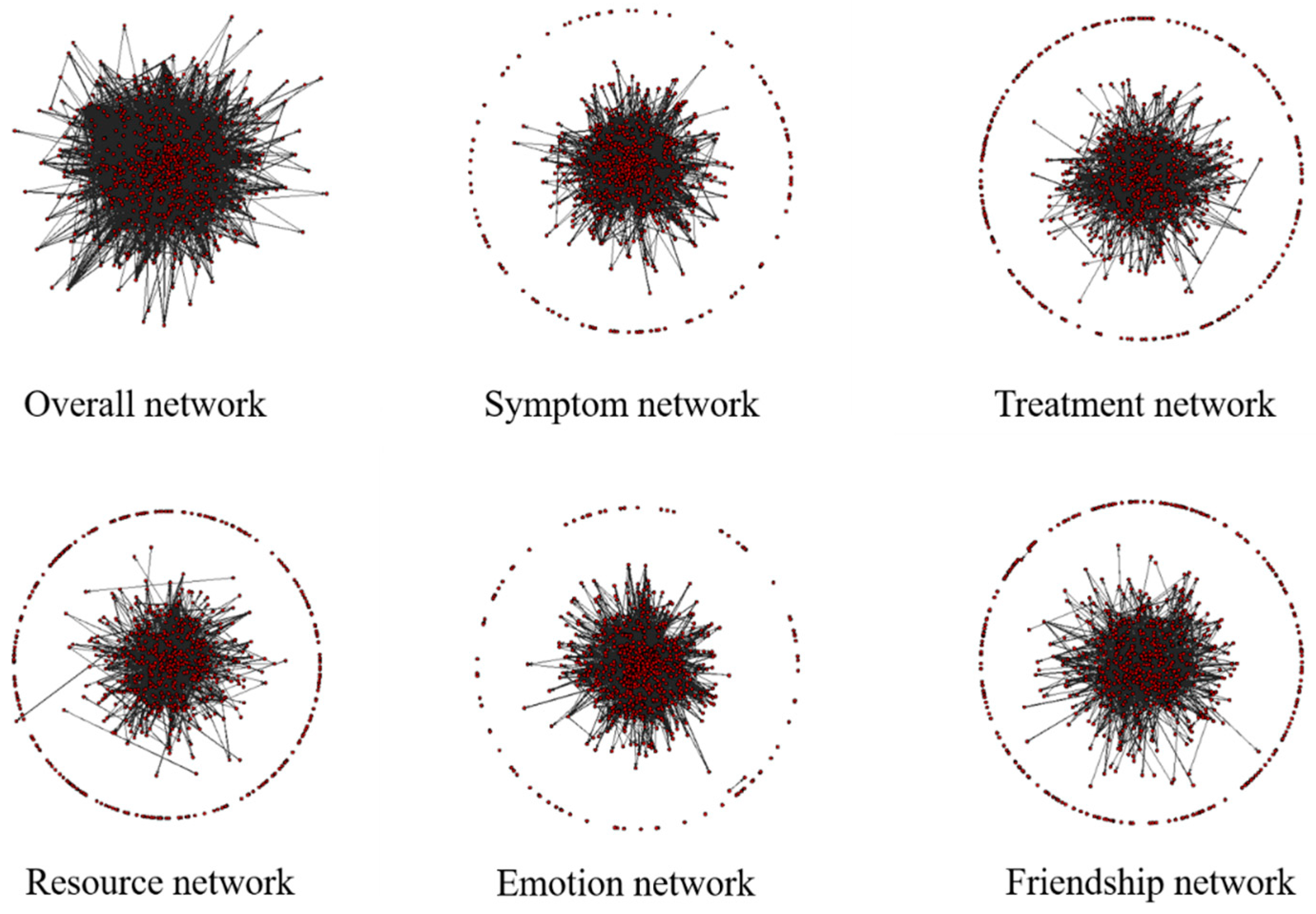
| Network | No. of Arcs | Density |
|---|---|---|
| Overall | 12,276 | 0.0206 |
| Symptom | 4483 | 0.0075 |
| Treatment | 2261 | 0.0038 |
| Resource | 2686 | 0.0045 |
| Emotion | 6402 | 0.0107 |
| Friendship | 2306 | 0.0039 |
| Network Effect | Configuration | Statistic | Hypothesis |
|---|---|---|---|
| Network structural effects | |||
| Arc |  | ||
| Reciprocity |  | H1 | |
| Actor attribute effects | |||
| Sender effects |  | H2a, H3a, H4a, H5a, H6a | |
| Receiver effects |  | H2b, H3b, H4b, Hb, H6b | |
| Homophily effects |  | H2c | |
| Heterophily effects |  | H3c, H4c, H5c, H6c | |
| Cross-network effects | |||
| Entrainment effects |  | H7 | |
| Exchange effects |  | H8 |
| Parameter | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | SE | p-Value | Estimate | SE | p-Value | Estimate | SE | p-Value | |
| Network structural effects | |||||||||
| Arc | −4.252 | 0.011 | <0.001 | −5.529 | 0.031 | <0.001 | −6.275 | 0.065 | <0.001 |
| Reciprocity | 3.550 | 0.031 | <0.001 | 3.352 | 0.032 | <0.001 | 1.717 | 0.045 | <0.001 |
| Actor attribute effects | |||||||||
| Gender-Sender | 0.113 | 0.019 | <0.001 | 0.245 | 0.023 | <0.001 | |||
| Gender-Receiver | −0.235 | 0.019 | <0.001 | −0.055 | 0.023 | 0.015 | |||
| Gender-Homophily | 0.044 | 0.015 | 0.004 | 0.061 | 0.021 | 0.003 | |||
| Age-Sender | 3.026 | 0.067 | <0.001 | 1.364 | 0.084 | <0.001 | |||
| Age-Receiver | 1.653 | 0.069 | <0.001 | 0.476 | 0.084 | <0.001 | |||
| Age-Heterophily | −1.228 | 0.069 | <0.001 | −1.347 | 0.085 | <0.001 | |||
| Sentiment-Sender | 1.139 | 0.068 | <0.001 | ||||||
| Sentiment-Receiver | −0.581 | 0.069 | <0.001 | ||||||
| Sentiment-Heterophily | −1.131 | 0.076 | <0.001 | ||||||
| Influence-Sender | 7.133 | 0.171 | <0.001 | ||||||
| Influence-Receiver | 12.395 | 0.168 | <0.001 | ||||||
| Influence-Heterophily | −7.167 | 0.134 | <0.001 | ||||||
| Duration-Sender | 3.335 | 0.140 | <0.001 | ||||||
| Duration-Receiver | −0.132 | 0.142 | 0.353 | ||||||
| Duration-Heterophily | −0.218 | 0.125 | 0.083 | ||||||
| AIC | 110,799 | 106,854 | 84,459 | ||||||
| BIC | 110,822 | 106,945 | 84,651 | ||||||
| Parameter | Symptom | Treatment | Resource | Emotion | Friendship |
|---|---|---|---|---|---|
| Network structural effects | |||||
| Arc | −6.752 *** | −6.853 *** | −7.827 *** | −6.873 *** | −8.592 *** |
| Reciprocity | 1.595 *** | 2.425 *** | 1.381 *** | 1.685 *** | 1.244 *** |
| Actor attribute effects | |||||
| Gender-Sender | 0.430 *** | 0.322 *** | 0.378 *** | 0.148 *** | 0.403 *** |
| Gender-Receiver | −0.030 | −0.060 | 0.177 *** | −0.248 *** | 0.130 * |
| Gender-Homophily | 0.052 | 0.054 | −0.022 | 0.099 *** | 0.009 |
| Age-Sender | 1.574 *** | 2.356 *** | 0.933 *** | 1.161 *** | 1.362 *** |
| Age-Receiver | 0.813 *** | 0.968 *** | 0.580 *** | 0.354 ** | 0.101 |
| Age-Heterophily | −1.714 *** | −1.799 *** | −1.329 *** | −1.391 *** | −1.980 *** |
| Sentiment-Sender | 0.747 *** | 0.106 | 0.898 *** | 1.326 *** | 1.567 *** |
| Sentiment-Receiver | −1.348 *** | −1.396 *** | −0.688 *** | −0.372 *** | 0.028 |
| Sentiment-Heterophily | −1.233 *** | −1.611 *** | −1.407 *** | −1.265 *** | −0.435 ** |
| Influence-Sender | 6.969 *** | 5.028 *** | 7.701 *** | 7.597 *** | 6.993 *** |
| Influence-Receiver | 11.142 *** | 8.865 *** | 11.046 *** | 12.219 *** | 11.342 *** |
| Influence-Heterophily | −7.219 *** | −5.616 *** | −7.525 *** | −7.404 *** | −7.257 *** |
| Duration-Sender | 1.790 *** | 1.713 *** | 2.341 *** | 2.567 *** | 1.587 *** |
| Duration-Receiver | −1.731 *** | −2.004 *** | 0.879 *** | −0.400 * | −0.805 *** |
| Duration-Heterophily | 1.655 *** | 1.543 *** | 0.610 *** | 0.262 | 1.800 *** |
| AIC | 40,134 | 24,455 | 23,080 | 49,575 | 21,842 |
| BIC | 40,326 | 24,647 | 23,272 | 49,767 | 22,034 |
| Cross-Network Effects | Entrainment Effect | Exchange Effect | ||||
|---|---|---|---|---|---|---|
| Estimate | SE | t-Ratio | Estimate | SE | t-Ratio | |
| Symptom—Treatment | 4.335 * | 0.064 | 0.026 | 0.787 * | 0.121 | 0.058 |
| Symptom—Resource | 3.944 * | 0.064 | 0.03 | 0.548 * | 0.097 | 0.023 |
| Symptom—Emotion | 4.125 * | 0.043 | 0.027 | 0.679 * | 0.077 | 0.064 |
| Symptom—Friendship | 3.901 * | 0.069 | 0.086 | 1.155 * | 0.097 | −0.062 |
| Treatment—Resource | 3.376 * | 0.082 | −0.039 | 0.750 * | 0.112 | −0.044 |
| Treatment—Emotion | 3.732 * | 0.063 | 0.056 | 0.622 * | 0.091 | 0.055 |
| Treatment—Friendship | 3.344 * | 0.081 | 0.09 | 0.851 * | 0.122 | −0.025 |
| Resource—Emotion | 4.110 * | 0.052 | 0.044 | 1.117 * | 0.082 | −0.009 |
| Resource—Friendship | 3.849 * | 0.068 | 0.098 | 1.238 * | 0.112 | −0.004 |
| Emotion—Friendship | 3.855 * | 0.066 | 0.062 | 1.305 * | 0.085 | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.; Wang, X.; Su, L.; Zhao, H. Multiplex Social Network Analysis to Understand the Social Engagement of Patients in Online Health Communities. Mathematics 2023, 11, 4412. https://doi.org/10.3390/math11214412
Lu Y, Wang X, Su L, Zhao H. Multiplex Social Network Analysis to Understand the Social Engagement of Patients in Online Health Communities. Mathematics. 2023; 11(21):4412. https://doi.org/10.3390/math11214412
Chicago/Turabian StyleLu, Yingjie, Xinwei Wang, Lin Su, and Han Zhao. 2023. "Multiplex Social Network Analysis to Understand the Social Engagement of Patients in Online Health Communities" Mathematics 11, no. 21: 4412. https://doi.org/10.3390/math11214412
APA StyleLu, Y., Wang, X., Su, L., & Zhao, H. (2023). Multiplex Social Network Analysis to Understand the Social Engagement of Patients in Online Health Communities. Mathematics, 11(21), 4412. https://doi.org/10.3390/math11214412