
Computational Evaluation of IABP, Impella 2.5, TandemHeart and Combined IABP and Impella 2.5 Support in Cardiogenic Shock

 , , and
, , and 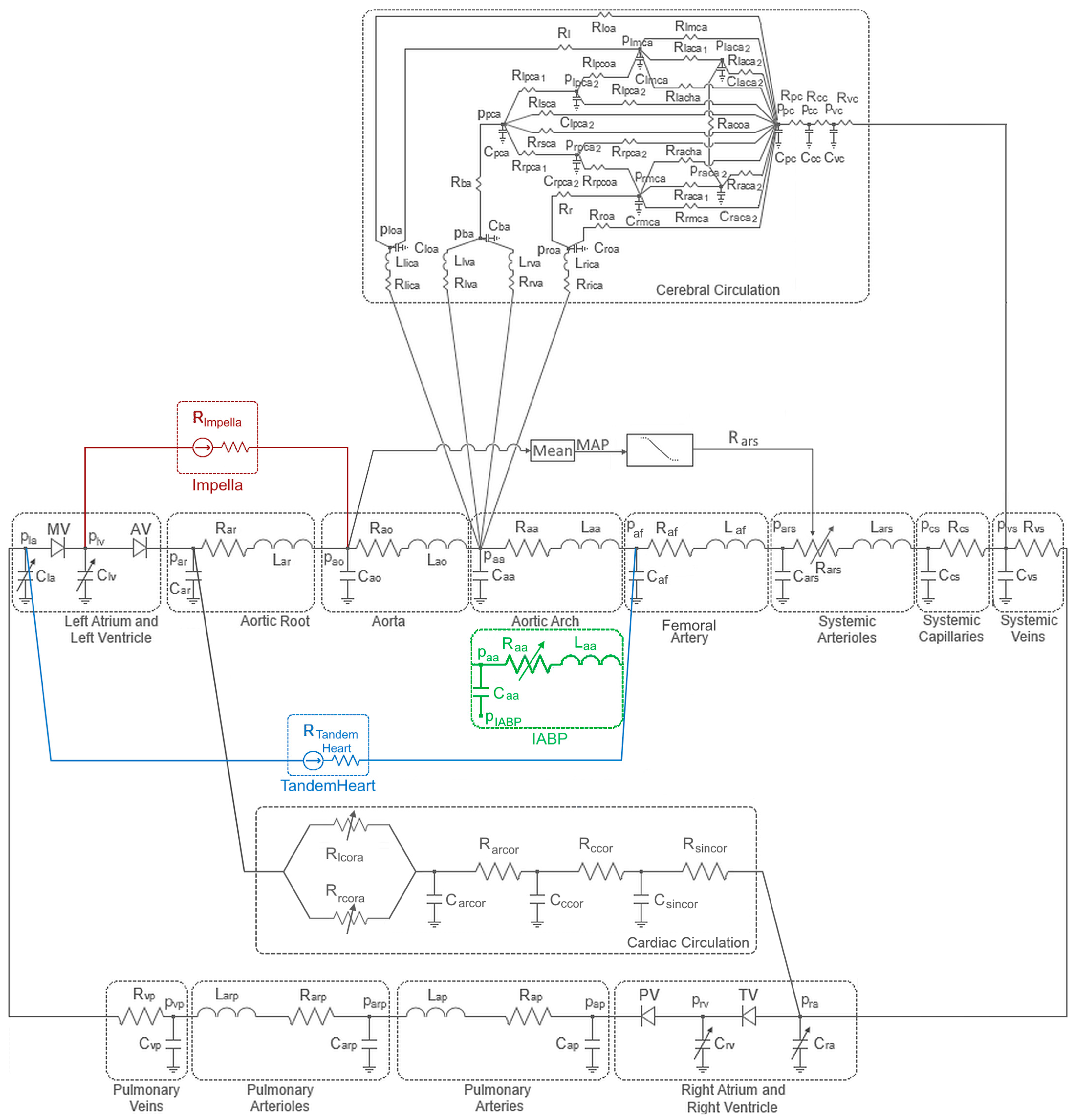{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
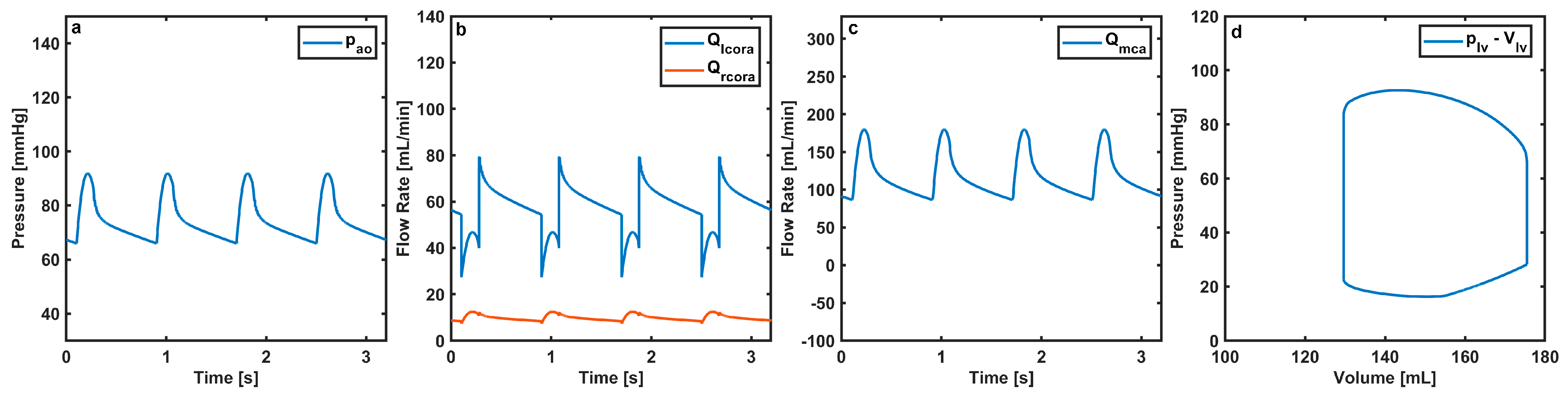
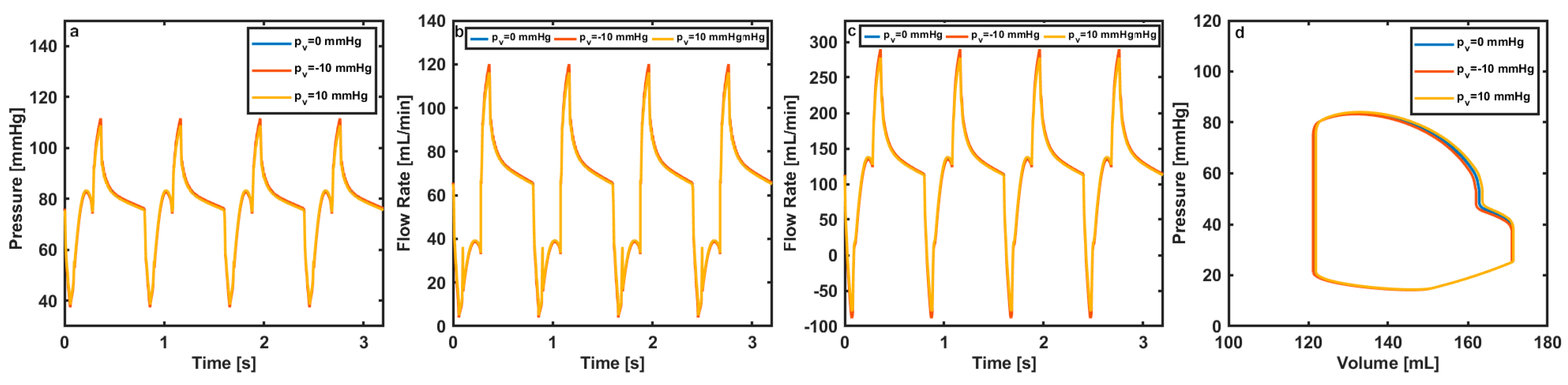
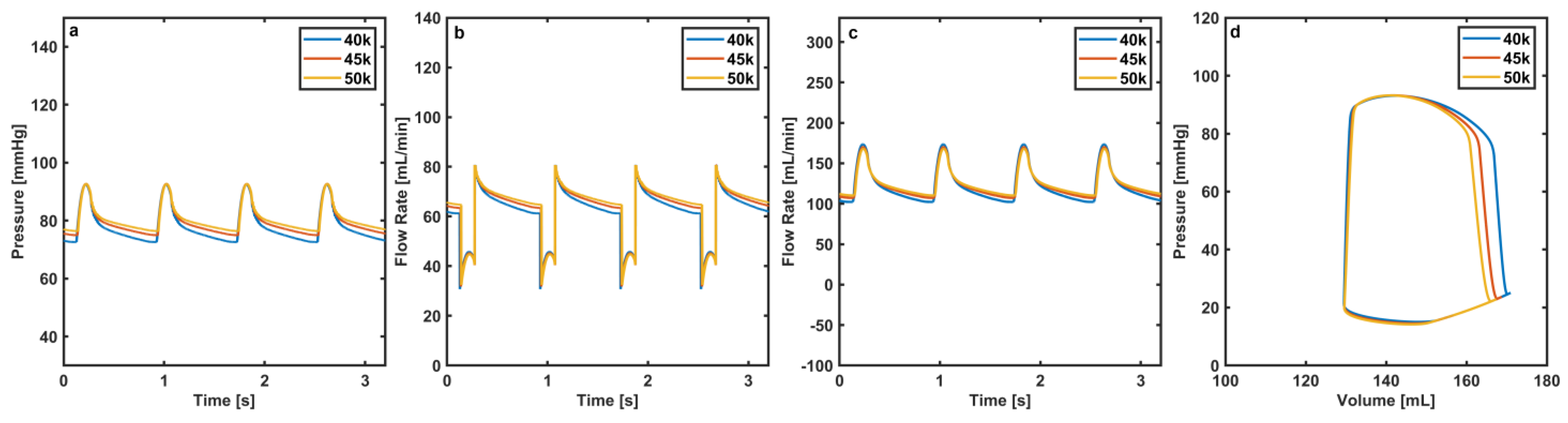
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Thiele, H.; Ohman, E.M.; de Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of Cardiogenic Shock Complicating Myocardial Infarction: An Update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef]
- Kosaraju, A.; Pendela, V.S.; Hai, O. Cardiogenic Shock. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Telukuntla, K.S.; Estep, J.D. Acute Mechanical Circulatory Support for Cardiogenic Shock. Methodist. Debakey Cardiovasc. J. 2020, 16, 27–35. [Google Scholar] [CrossRef]
- Atti, V.; Narayanan, M.A.; Patel, B.; Balla, S.; Siddique, A.; Lundgren, S.; Velagapudi, P. A Comprehensive Review of Mechanical Circulatory Support Devices. Heart Int. 2022, 16, 37–48. [Google Scholar] [CrossRef]
- Miller, P.E.; Solomon, M.A.; McAreavey, D. Advanced Percutaneous Mechanical Circulatory Support Devices for Cardiogenic Shock. Crit. Care Med. 2017, 45, 1922–1929. [Google Scholar] [CrossRef]
- Jneid, H. Chapter 18—Cardiogenic Shock. In Cardiology Secrets, 5th ed.; Levine, G.N., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 164–171. ISBN 978-0-323-47870-0. [Google Scholar]
- De Lazzari, C.; De Lazzari, B.; Iacovoni, A.; Marconi, S.; Papa, S.; Capoccia, M.; Badagliacca, R.; Vizza, C.D. Intra-Aortic Balloon Counterpulsation Timing: A New Numerical Model for Programming and Training in the Clinical Environment. Comput. Methods Programs Biomed. 2020, 194, 105537. [Google Scholar] [CrossRef]
- Khan, T.M.; Siddiqui, A.H. Intra-Aortic Balloon Pump. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Parissis, H.; Leotsinidis, M.; Akbar, M.T.; Apostolakis, E.; Dougenis, D. The Need for Intra Aortic Balloon Pump Support Following Open Heart Surgery: Risk Analysis and Outcome. J. Cardiothorac. Surg. 2010, 5, 20. [Google Scholar] [CrossRef]
- Salter, B.S.; Gross, C.R.; Weiner, M.M.; Dukkipati, S.R.; Serrao, G.W.; Moss, N.; Anyanwu, A.C.; Burkhoff, D.; Lala, A. Temporary Mechanical Circulatory Support Devices: Practical Considerations for All Stakeholders. Nat. Rev. Cardiol. 2023, 20, 263–277. [Google Scholar] [CrossRef]
- Abiragi, M.; Singer-Englar, T.; Cole, R.M.; Emerson, D.; Esmailian, F.; Megna, D.; Moriguchi, J.; Kobashigawa, J.A.; Kittleson, M.M. Temporary Mechanical Circulatory Support in Patients with Cardiogenic Shock: Clinical Characteristics and Outcomes. J. Clin. Med. 2023, 12, 1622. [Google Scholar] [CrossRef]
- Kar, B.; Adkins, L.E.; Civitello, A.B.; Loyalka, P.; Palanichamy, N.; Gemmato, C.J.; Myers, T.J.; Gregoric, I.D.; Delgado, R.M. Clinical Experience with the TandemHeart® Percutaneous Ventricular Assist Device. Tex. Heart Inst. J. 2006, 33, 111–115. [Google Scholar]
- Schwartz, B.G.; Ludeman, D.J.; Mayeda, G.S.; Kloner, R.A.; Economides, C.; Burstein, S. Treating Refractory Cardiogenic Shock With the TandemHeart and Impella Devices: A Single Center Experience. Cardiol. Res. 2012, 3, 54–66. [Google Scholar] [CrossRef]
- Upadhyay, R. Current Landscape of Temporary Percutaneous Mechanical Circulatory Support Technology. US Cardiol. Rev. 2021, 15, 1–7. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; de Waha, A.; Richardt, G.; Hennersdorf, M.; Empen, K.; et al. Intra-Aortic Balloon Counterpulsation in Acute Myocardial Infarction Complicated by Cardiogenic Shock (IABP-SHOCK II): Final 12 Month Results of a Randomised, Open-Label Trial. Lancet 2013, 382, 1638–1645. [Google Scholar] [CrossRef]
- Lauten, A.; Engström, A.E.; Jung, C.; Empen, K.; Erne, P.; Cook, S.; Windecker, S.; Bergmann, M.W.; Klingenberg, R.; Lüscher, T.F.; et al. Percutaneous Left-Ventricular Support With the Impella-2.5–Assist Device in Acute Cardiogenic Shock. Circ. Heart Fail. 2013, 6, 23–30. [Google Scholar] [CrossRef]
- O’neill, W.W.; Schreiber, T.; Wohns, D.H.W.; Rihal, C.; Naidu, S.S.; Civitello, A.B.; Dixon, S.R.; Massaro, J.M.; Maini, B.; Ohman, E.M. The Current Use of Impella 2.5 in Acute Myocardial Infarction Complicated by Cardiogenic Shock: Results from the USpella Registry. J. Interv. Cardiol. 2014, 27, 1–11. [Google Scholar] [CrossRef]
- Seyfarth, M.; Sibbing, D.; Bauer, I.; Fröhlich, G.; Bott-Flügel, L.; Byrne, R.; Dirschinger, J.; Kastrati, A.; Schömig, A. A Randomized Clinical Trial to Evaluate the Safety and Efficacy of a Percutaneous Left Ventricular Assist Device versus Intra-Aortic Balloon Pumping for Treatment of Cardiogenic Shock Caused by Myocardial Infarction. J. Am. Coll. Cardiol. 2008, 52, 1584–1588. [Google Scholar] [CrossRef]
- Kar, B.; Gregoric, I.D.; Basra, S.S.; Idelchik, G.M.; Loyalka, P. The Percutaneous Ventricular Assist Device in Severe Refractory Cardiogenic Shock. J. Am. Coll. Cardiol. 2011, 57, 688–696. [Google Scholar] [CrossRef]
- Burkhoff, D.; Cohen, H.; Brunckhorst, C.; O’Neill, W.W. A Randomized Multicenter Clinical Study to Evaluate the Safety and Efficacy of the TandemHeart Percutaneous Ventricular Assist Device versus Conventional Therapy with Intraaortic Balloon Pumping for Treatment of Cardiogenic Shock. Am. Heart J. 2006, 152, 469.e1–469.e8. [Google Scholar] [CrossRef]
- Giraud, R.; Assouline, B.; Banfi, C.; Bendjelid, K. Impella Combined with Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO) for Advanced Hemodynamic Support. Rev. Cardiovasc. Med. 2022, 23, 3. [Google Scholar] [CrossRef]
- Abdolrazaghi, M.; Navidbakhsh, M.; Hassani, K. Mathematical Modelling of Intra-Aortic Balloon Pump. Comput. Methods Biomech. Biomed. Eng. 2010, 13, 567–576. [Google Scholar] [CrossRef]
- Sun, Y. Modeling the Dynamic Interaction between Left Ventricle and Intra-Aortic Balloon Pump. Am. J. Physiol. 1991, 261, H1300–H1311. [Google Scholar] [CrossRef]
- Schampaert, S.; Rutten, M.C.M.; van T Veer, M.; van Nunen, L.X.; Tonino, P.A.L.; Pijls, N.H.J.; van de Vosse, F.N. Modeling the Interaction between the Intra-Aortic Balloon Pump and the Cardiovascular System: The Effect of Timing. ASAIO J. 2013, 59, 30–36. [Google Scholar] [CrossRef]
- De Lazzari, B.; Capoccia, M.; Badagliacca, R.; Bozkurt, S.; De Lazzari, C. IABP versus Impella Support in Cardiogenic Shock: “In Silico” Study. J. Cardiovasc. Dev. Dis. 2023, 10, 140. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.-C.; Simaan, M.A.; Mushi, S.E.; Zorn, N.V. Performance Prediction of a Percutaneous Ventricular Assist System Using Nonlinear Circuit Analysis Techniques. IEEE Trans. Biomed. Eng. 2008, 55, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, S. Mathematical Modeling of Cardiac Function to Evaluate Clinical Cases in Adults and Children. PLoS ONE 2019, 14, e0224663. [Google Scholar] [CrossRef]
- Bozkurt, S.; Volkan Yilmaz, A.; Bakaya, K.; Bharadwaj, A.; Safak, K.K. A Novel Computational Model for Cerebral Blood Flow Rate Control Mechanisms to Evaluate Physiological Cases. Biomed. Signal Process. Control 2022, 78, 103851. [Google Scholar] [CrossRef]
- Bozkurt, S. Effect of Cerebral Flow Autoregulation Function on Cerebral Flow Rate Under Continuous Flow Left Ventricular Assist Device Support. Artif. Organs 2018, 42, 800–813. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Andreassen, S.; Shaw, G.M.; Jensen, P.L.; Rees, S.E.; Chase, J.G. Simulation of Cardiovascular System Diseases by Including the Autonomic Nervous System into a Minimal Model. Comput. Methods Programs Biomed. 2007, 86, 153–160. [Google Scholar] [CrossRef]
- Khalafbeigui, F.; Suga, H.; Sagawa, K. Left Ventricular Systolic Pressure-Volume Area Correlates with Oxygen Consumption. Am. J. Physiol. Heart Circ. Physiol. 1979, 237, H566–H569. [Google Scholar] [CrossRef] [PubMed]
- Saku, K.; Yokota, S.; Nishikawa, T.; Kinugawa, K. Interventional Heart Failure Therapy: A New Concept Fighting against Heart Failure. J. Cardiol. 2022, 80, 101–109. [Google Scholar] [CrossRef]
- Møller-Helgestad, O.K.; Poulsen, C.B.; Christiansen, E.H.; Lassen, J.F.; Ravn, H.B. Support with Intra-Aortic Balloon Pump vs. Impella2.5® and Blood Flow to the Heart, Brain and Kidneys—An Experimental Porcine Model of Ischaemic Heart Failure. Int. J. Cardiol. 2015, 178, 153–158. [Google Scholar] [CrossRef]
- Brass, L.M. Reversed Intracranial Blood Flow in Patients with an Intra-Aortic Balloon Pump. Stroke 1990, 21, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Schachtrupp, A.; Wrigge, H.; Busch, T.; Buhre, W.; Weyland, A. Influence of Intra-Aortic Balloon Pumping on Cerebral Blood Flow Pattern in Patients after Cardiac Surgery. Eur. J. Anaesthesiol. 2005, 22, 165–170. [Google Scholar] [CrossRef] [PubMed]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkan, R.; De Lazzari, B.; Capoccia, M.; De Lazzari, C.; Bozkurt, S. Computational Evaluation of IABP, Impella 2.5, TandemHeart and Combined IABP and Impella 2.5 Support in Cardiogenic Shock. Mathematics 2023, 11, 3606. https://doi.org/10.3390/math11163606
Alkan R, De Lazzari B, Capoccia M, De Lazzari C, Bozkurt S. Computational Evaluation of IABP, Impella 2.5, TandemHeart and Combined IABP and Impella 2.5 Support in Cardiogenic Shock. Mathematics. 2023; 11(16):3606. https://doi.org/10.3390/math11163606
Chicago/Turabian StyleAlkan, Rahmi, Beatrice De Lazzari, Massimo Capoccia, Claudio De Lazzari, and Selim Bozkurt. 2023. "Computational Evaluation of IABP, Impella 2.5, TandemHeart and Combined IABP and Impella 2.5 Support in Cardiogenic Shock" Mathematics 11, no. 16: 3606. https://doi.org/10.3390/math11163606
APA StyleAlkan, R., De Lazzari, B., Capoccia, M., De Lazzari, C., & Bozkurt, S. (2023). Computational Evaluation of IABP, Impella 2.5, TandemHeart and Combined IABP and Impella 2.5 Support in Cardiogenic Shock. Mathematics, 11(16), 3606. https://doi.org/10.3390/math11163606