A Mixed Methods Study on the Effect of Flipping the Undergraduate Medical Classroom



 ,
, {kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Materials
2.3. Procedure
2.4. Analyses
3. Results
3.1. The Impact of the Flipped Classroom on Learning Outcomes
3.2. Analysis of Focus Group Data
3.3. Analysis of Survey Data
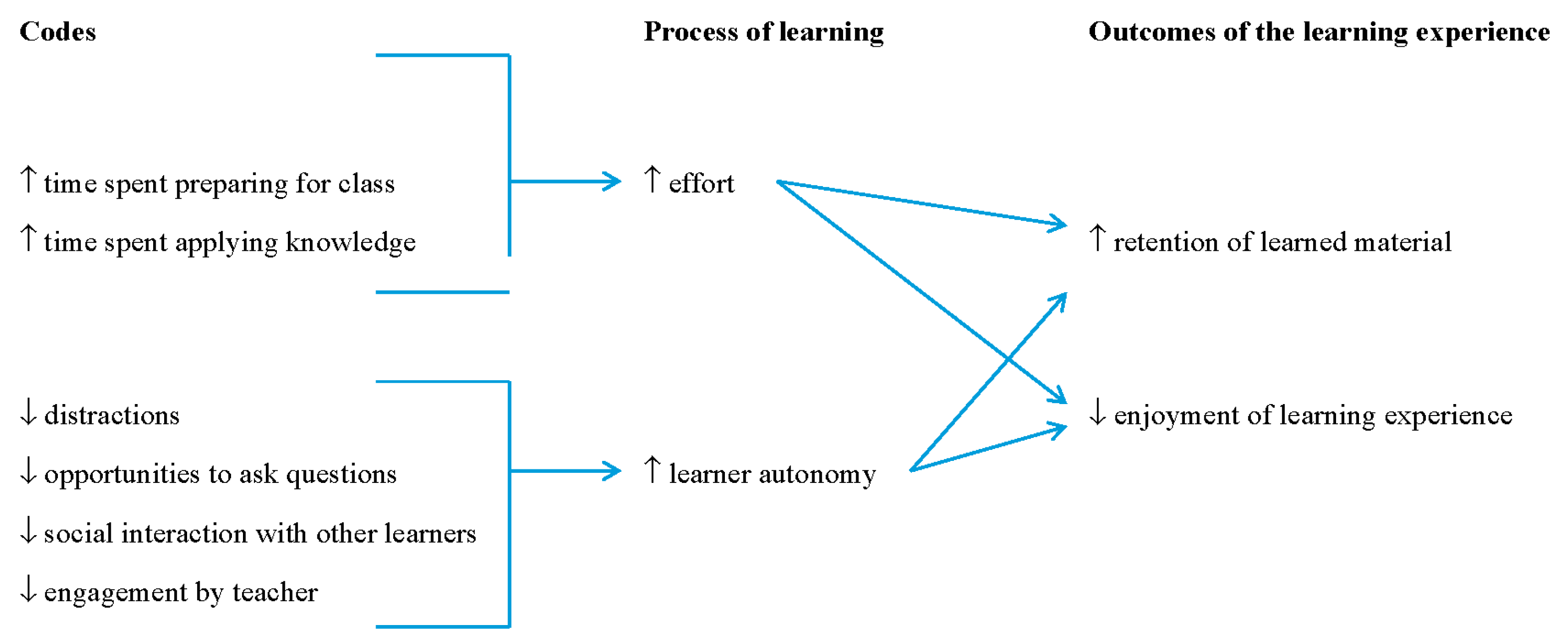
Theoretical Relationship between the Learning in the Flipped Classroom and Learning Outcomes
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Mazur, E. Peer Instruction: A User’s Manual Series in Educational Innovation; Prentice Hall: Upper Saddle River, NJ, USA, 1997. [Google Scholar]
- Next Genlearation Learning. Available online: https://docs.gatesfoundation.org/Documents/nextgenlearning.pdf (accessed on 4 October 2017).
- You Can Lean Anything. Available online: https://www.khanacademy.org/ (accessed on 4 October 2017).
- Prober, C.G.; Khan, S. Medical education reimagined: A call to action. Acad. Med. 2013, 88, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Sait, M.S.; Siddiqui, Z.; Ashraf, Y. Advances in medical education and practice: Student perceptions of the flipped classroom. Adv. Med. Educ. Pract. 2017, 8, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Lui, A.M.; Martinelli, S.M. A systematic review of the effectiveness of flipped classrooms in medical education. Med. Educ. 2017, 51, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.A.; Ellaway, R.H. Evaluating technology-enhanced learning: A comprehensive framework. Med. Teach. 2015, 37, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, D. Revisiting Kirkpatrick’s four-level model. Train. Dev. 1996, 50, 54–59. [Google Scholar]
- Presti, C.R. The flipped learning approach in nursing education: A literature review. J. Nurs. Educ. 2016, 55, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Missildine, K.; Fountain, R.; Summers, L.; Gosselin, K. Flipping the classroom to improve student performance and satisfaction. J. Nurs. Educ. 2013, 52, 597–599. [Google Scholar] [CrossRef] [PubMed]
- Ratta, C.B. Flipping the classroom with team-based learning in undergraduate nursing education. Nurse Educ. 2015, 40, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Westhorp, G.; Pawson, R.; Greenhalgh, T. Realist Synthesis: RAMSES Training Materials. Available online: www.ramesesproject.org/media/Realist_reviews_training_materials.pdf (accessed on 1 July 2013).
- Linsley, P.; Howard, D.; Owen, S. The construction of context-mechanisms-outcomes in realistic evaluation. Nurse Res. 2015, 3, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.; Clark, V.P. Designing and Conducting Mixed Methods Research, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Strauss, A.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Newbury Park, CA, USA, 1998. [Google Scholar]
- Bjork, E.L.; Bjork, R.A. Making things hard on yourself, but in a good way: Creating desirable difficulties to enhance learning. In Psychology and the Real World: Essays Illustrating Fundamental Contributions to Society; Gernsbacher, M.A., Pew, R.W., Hough, L.M., Pomerantz, J.R., Eds.; Worth Publishers: New York, NY, USA, 2010. [Google Scholar]
- Benner, P.; Sutphen, M.; Leonard, V.; Day, L. Educating Nurses: A Call for Radical Transformation; Jossey-Bass: San Francisco, CA, USA, 2010. [Google Scholar]

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burak, K.W.; Raman, M.; Paget, M.; Busche, K.; Coderre, S.; McLaughlin, K. A Mixed Methods Study on the Effect of Flipping the Undergraduate Medical Classroom. Educ. Sci. 2017, 7, 83. https://doi.org/10.3390/educsci7040083
Burak KW, Raman M, Paget M, Busche K, Coderre S, McLaughlin K. A Mixed Methods Study on the Effect of Flipping the Undergraduate Medical Classroom. Education Sciences. 2017; 7(4):83. https://doi.org/10.3390/educsci7040083
Chicago/Turabian StyleBurak, Kelly W., Maitreyi Raman, Michael Paget, Kevin Busche, Sylvain Coderre, and Kevin McLaughlin. 2017. "A Mixed Methods Study on the Effect of Flipping the Undergraduate Medical Classroom" Education Sciences 7, no. 4: 83. https://doi.org/10.3390/educsci7040083
APA StyleBurak, K. W., Raman, M., Paget, M., Busche, K., Coderre, S., & McLaughlin, K. (2017). A Mixed Methods Study on the Effect of Flipping the Undergraduate Medical Classroom. Education Sciences, 7(4), 83. https://doi.org/10.3390/educsci7040083