The Flipped Classroom as a Pedagogical Tool for Leadership Development in Postgraduate Medical Education

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Setting and Participants
2.1.2. Instructor Selection
2.1.3. Instructional Tools
2.1.4. Content and Format of the Training Module
2.1.5. Questionnaire Design
2.2. Data Collection
2.2.1. Knowledge Acquisition
2.2.2. Perceived Effectiveness of FCM
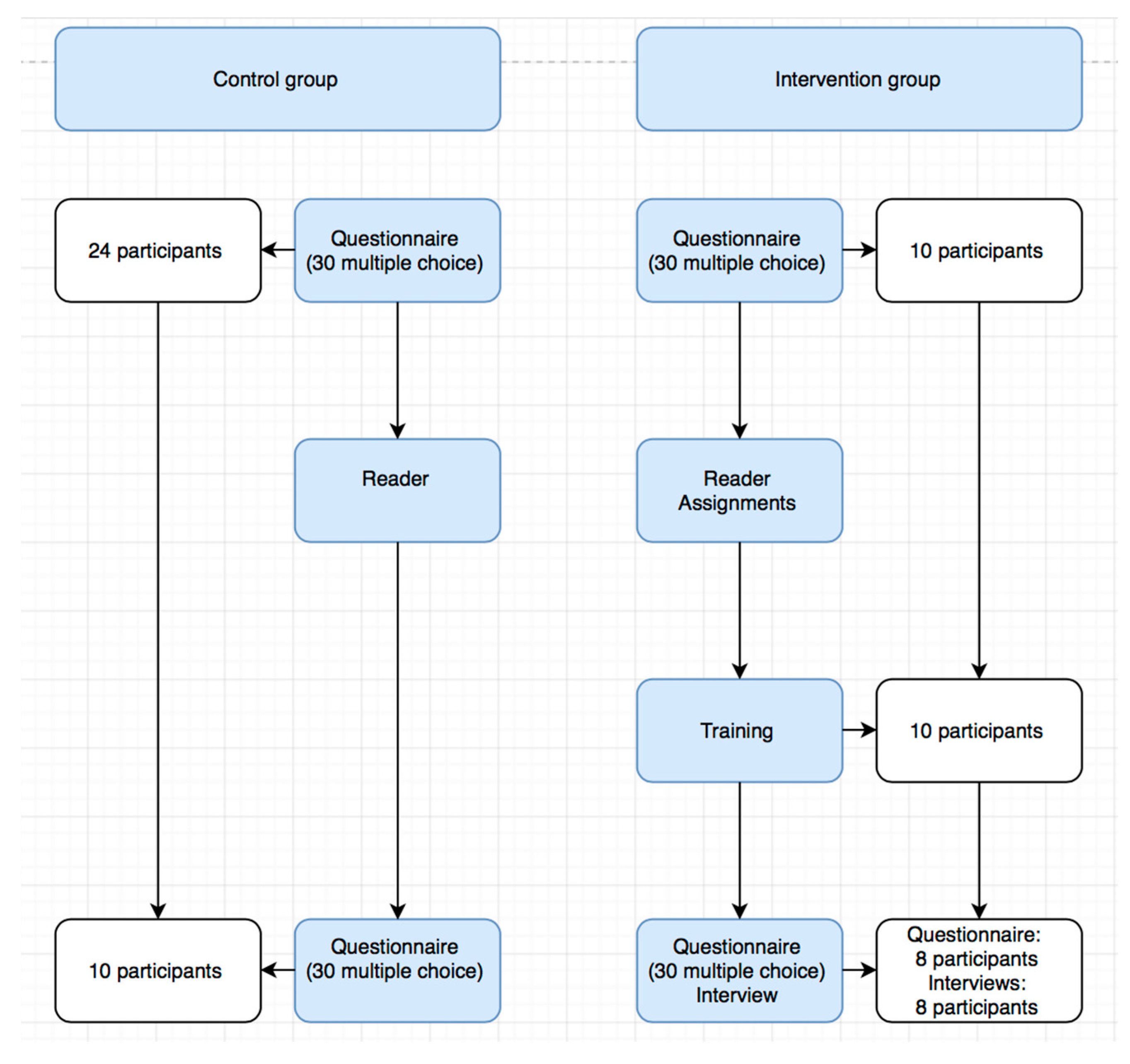
2.3. Procedures
2.3.1. General Procedure
2.3.2. Intervention Group
2.4. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Knowledge Acquisition
3.3. Semi-structured Interviews
4. Discussion
5. Conclusions
Supplementary Materials
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ACGME | Accreditation Council for Graduate Medical Education |
| CanMEDS | Canadian Medical Education Directives for Specialists |
| ILOs | Intended Learning Outcomes |
| METC | Medical Ethics Committee |
| VLE | Virtual Learning Environment |
Ethics Approval and Consent to Participate
References
- Busari, J.O.; Berkenbosch, L.; Brouns, J.W. Physicians as managers of health care delivery and the implications for postgraduate medical training: A literature review. Teach. Learn. Med. 2011, 23, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Berkenbosch, L. Management and leadership education for medical residents. Evaluating needs and developing an educational intervention. In Enschede; Ipskamp Drukkers BV: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Ackerly, D.; Sangvai, D.; Udayakumar, K.; Shah, B.; Kalman, N.; Cho, A.; Schulman, K.A.; Fulkerson, W.J., Jr.; Dzau, V.J. Training the Next Generation of Physician-Executives: An Innovative Residency Pathway in Management and Leadership. Acad. Med. 2011, 86, 575–579. [Google Scholar] [CrossRef] [PubMed]
- MacCarrick, G. Chapter 1: Introduction. In Medical Leadership and Management A Case-based Approach; Springer: London, UK, 2014. [Google Scholar]
- Busari, J.; Scheele, F. Generatieverschillen: Relevant voor de Nederlandse specialistenopleiding. Ned. Tijdschr. Geneeskd. 2015, 159, A8900. [Google Scholar] [PubMed]
- Busari, J.O. The discourse of generational segmentation and the implications for postgraduate medical education. Perspect. Med. Educ. 2013, 2, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Keckley, P.; Eselius, L. Survey of Health Care Consumers: Key Findings, Strategic Implications; Deloitte Center for Health Solutions: Washington, DC, USA, 2009. [Google Scholar]
- The Royal Dutch Medical Association. Medical Professionalism 2007. 2007. Available online: https://www.nza.nl/1048076/1048181/Reactie_KNMG_bijlage_2.pdf (accessed on 9 June 2017).
- Halpern, R.; Lee, M.Y.; Boulter, P.R.; Phillips, R.R. A synthesis of nine major reports on physicians’ competencies for the emerging practice environment. Acad. Med. 2001, 76, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Severs, M.; Crane, S. Challenges in medical education—What the doctor ordered? Postgrad. Med. J. 2000, 76, 599–601. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.R.; Danoff, D. The CanMEDS initiative: Implementing an outcomes-based framework of physician competencies. Med. Teach. 2007, 29, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Swing, S. Assessing the ACGME general competencies: General considerations and assessment methods. Acad. Emerg. Med. 2002, 9, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Frank, J. The CanMEDS 2005 Physician Competency Framework. Better standards. Better physicians. Better Care. 2005. Available online: http://www.royalcollege.ca/portal/page/portal/rc/common/documents/canmeds/resources/publications/framework_full_e.pdf (accessed on 9 June 2017).
- Frank, J.; Snell, L.; Sherbino, J. CanMEDS 2015 Physician Competency Framework. 2015. Available online: http://canmeds.royalcollege.ca/uploads/en/framework/CanMEDS%202015%20Framework_EN_Reduced.pdf (accessed on 9 June 2017).
- Dath, D.; Chan, M.; Anderson, G.; Burke, A.; Razack, S.; Lieff, S. Leader. In CanMEDS 2015 Physician Competency Framework; Frank, J., Snell, L., Sherbino, J., Eds.; Royal College of Physicians and Surgeons of Canada: Ottawa, ON, Canada, 2015; Available online: http://canmeds.royalcollege.ca/uploads/en/framework/CanMEDS%202015%20Framework_EN_Reduced.pdf (accessed on 9 June 2017).
- Dath, D.; Chan, M.; Abbott, C. CanMEDS 2015: From Manager to Leader. 2015. Available online: https://www.google.nl/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahUKEwiUms355LDUAhWNIlAKHePNAqsQFggqMAA&url=http%3A%2F%2Fwww.royalcollege.ca%2Frcsite%2Fdocuments%2Fcbd%2Fcanmeds-2015-manager-to-leader-e.pdf&usg=AFQjCNFpP4-ke-TRDxU7IyOhiCUdEgYpxw&sig2=gbaZdhiCNZAWHJdejofRRw&cad=rja (accessed on 9 June 2017).
- Busari, J. Longitudinal curriculum for leadership development. Unpublished work. 2014. [Google Scholar]
- Berkenbosch, L.; Brouns, J.W.M.; Heyligers, I.; Busari, J.O. How Dutch medical residents perceive their competency as manager in the revised postgraduate medical curriculum. Postgrad. Med. J. 2011, 87, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Berkenbosch, L.; Bax, M.; Scherpbier, A.; Heyligers, I.; Muijtjens, A.M.M.; Busari, J.O. How Dutch medical specialists perceive the competencies and training needs of medical residents in health care management. Med. Teach. 2013, 35, e1090–e1102. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E. Teaching law to students in the health care professions. Health Law Rev. 2003, 11, 8–19. [Google Scholar]
- Sharma, N.; Lau, C.S.; Doherty, I.; Harbutt, D. How we flipped the medical classroom. Med. Teach. 2015, 37, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Moffett, J. Twelve tips for “flipping” the classroom. Med. Teach. 2015, 37, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Mazur, E. Farewell lecture. J. Tokyo. Med. Univ. 2012, 70, 141–167. [Google Scholar]
- Van den Berg, E.E.P.; Bracey, A.; Van Driel, A.P.G.; Geijsel, F.E.C.; Manders, S. Modular continuing professional development for emergency physicians—The MNSHA masterclass programme. Eur. J. Emerg. Med. 2015, 23, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Brouns, J.W.; Berkenbosch, L.; Ploemen-Suijker, F.D.; Heyligers, I.; Busari, J.O. Medical residents perceptions of the need for management education in the postgraduate curriculum: A preliminary study. Int. J. Med. Educ. 2010, 1, 76–82. [Google Scholar] [CrossRef]
- McLaughlin, J.E.; Roth, M.T.; Glatt, D.M.; Gharkholonarehe, N.; Davidson, C.A.; Griffin, L.M.; Esserman, D.A.; Mumper, R.J. The Flipped Classroom: A course redesign to foster learning and engagement in a health professions school. Acad. Med. 2014, 89, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Lucardie, A.T.; Berkenbosch, L.; Van den Berg, J.; Busari, J.O. Flipping the classroom to teach Millennial residents medical leadership: A proof of concept. Adv. Med. Educ. Pract. 2017, 8, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Lui, A.M.; Martinelli, S.M. A systematic review of the effectiveness of flipped classrooms in medical education. Med. Educ. 2017, 51, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, J.; Ward, R.; Toews, J. Twelve tips for effective short course design. Med. Teach. 2005, 27, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Galway, L.P.; Corbett, K.K.; Takaro, T.K.; Tairyan, K.; Frank, E. A novel integration of online and flipped classroom instructional models in public health higher education. BMC Med. Educ. 2014, 14, 181. [Google Scholar] [CrossRef] [PubMed]
- Bishop, L.; Verleger, M. The Flipped Classroom: A Survey of the Research. In Proceedings of the 2013 ASEE Annual Conference & Exposition, Atlanta, GA, USA, 25 June 2013; p. 6219. [Google Scholar]
- Krathwohl, D.; Anderson, L.W. A Revision of Bloom’s Taxonomy: An Overview. Am. J. Psychol. 2009, 122, 39–52. [Google Scholar] [CrossRef]
- Ericsson, K.A. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad. Med. 2004, 79, S70–S81. [Google Scholar] [CrossRef] [PubMed]
- Busari, J.O.; Scherpbier, A.J. Why residents should teach: A literature review. J. Postgrad. Med. 2004, 50, 205–210. [Google Scholar] [PubMed]
- Berkenbosch, L.; Muijtjens, A.M.M.; Zimmermann, L.J.I.; Heyligers, I.C.; Scherpbier, A.J.J.A.; Busari, J.O. A pilot study of a practice management training module for medical residents. BMC Med. Educ. 2014, 14, 107. [Google Scholar] [CrossRef] [PubMed]
- Fylan, F. Semi-structured interviewing. In A Handbook of Research Methods for Clinical and Health Psychology; Oxford University Press: New York, NY, USA, 2005; pp. 65–67. [Google Scholar]
- Fick, U. An Introduction to Qualitative Research, 2nd ed.; Sage Publishing: London, UK, 2002; pp. 176–195. [Google Scholar]
- Kurup, V.; Hersey, D. The changing landscape of anesthesia education: Is Flipped Classroom the answer? Curr. Opin. Anaesthesiol. 2013, 26, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Butt, A. Student views on the use of lecture time and their experience with a flipped classroom approach. Bus. Educ. Accredit. 2014, 6, 33–43. [Google Scholar] [CrossRef]
- Kerfoot, B.; Conlin, P.; Travison, T.; McMahon, G. Web-Based Education in Systems-Based Practice: A randomized trial. Arch. Intern. Med. 2007, 167, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Rowe, M.; Frantz, J.; Bozalek, V. Beyond knowledge and skills: The use of a Delphi study to develop a technology-mediated teaching strategy. BMC Med. Educ. 2013, 13, 51. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Training Health Care Law | Training Medical Errors/Negligence |
|---|---|
| remembering, understanding | |
| • Knowledge of the different types of law | • The implications of medical incidents and errors for the patient and medical staff |
| • Knowledge of health care laws in the Netherlands | • The difference between medical incidents, complications, calamities and errors. |
| • Knowledge of a disciplinary claim procedure | |
| Training Health Care Law | Training Medical Errors/Negligence |
|---|---|
| applying, analysing, evaluating, creating | |
| • Evaluate the measures issued by the Medical Disciplinary Council in case studies | • (Early) recognition of red flags in the process of care and identification of possible solutions |
| • Provide sound judgements in practical situations and adequately apply health care laws to daily practice | • Make sounds decisions/judgements on the prevention of medical errors |
| • Have the capability to inform both patients and law enforcement adequately | • Apply the procedure of reporting a medical incident in a hospital |
| Intervention Group (n = 10) | Control Group (n = 24) | |
|---|---|---|
| Average age (years) | 29.00 (26–35) | 28.64 (25–35) |
| Gender (male) | 3 (30.0%) | 10 (41.7%) |
| Years of experience | ||
| <1 | 1 (10.0%) | 7 (29.2%) |
| 1–2 | 3 (30.0%) | 7 (29.2%) |
| 3–4 | 3 (30.0%) | 7 (29.2%) |
| 5–6 | 2 (20.0%) | 3 (12.5%) |
| >6 | 1 (10.0%) | 0 (0%) |
| Basic Medical education | ||
| Netherlands | 9 (90.0%) | 23 (95.8%) |
| Belgium | 1 (10.0%) | 1 (4.2%) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucardie, A.T.; Busari, J.O. The Flipped Classroom as a Pedagogical Tool for Leadership Development in Postgraduate Medical Education. Educ. Sci. 2017, 7, 63. https://doi.org/10.3390/educsci7020063
Lucardie AT, Busari JO. The Flipped Classroom as a Pedagogical Tool for Leadership Development in Postgraduate Medical Education. Education Sciences. 2017; 7(2):63. https://doi.org/10.3390/educsci7020063
Chicago/Turabian StyleLucardie, Alicia T., and Jamiu O. Busari. 2017. "The Flipped Classroom as a Pedagogical Tool for Leadership Development in Postgraduate Medical Education" Education Sciences 7, no. 2: 63. https://doi.org/10.3390/educsci7020063
APA StyleLucardie, A. T., & Busari, J. O. (2017). The Flipped Classroom as a Pedagogical Tool for Leadership Development in Postgraduate Medical Education. Education Sciences, 7(2), 63. https://doi.org/10.3390/educsci7020063