

Analyzing the Associations between Facets of Physical Literacy, Physical Fitness, and Physical Activity Levels: Gender- and Age-Specific Cross-Sectional Study in Preadolescent Children

 ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
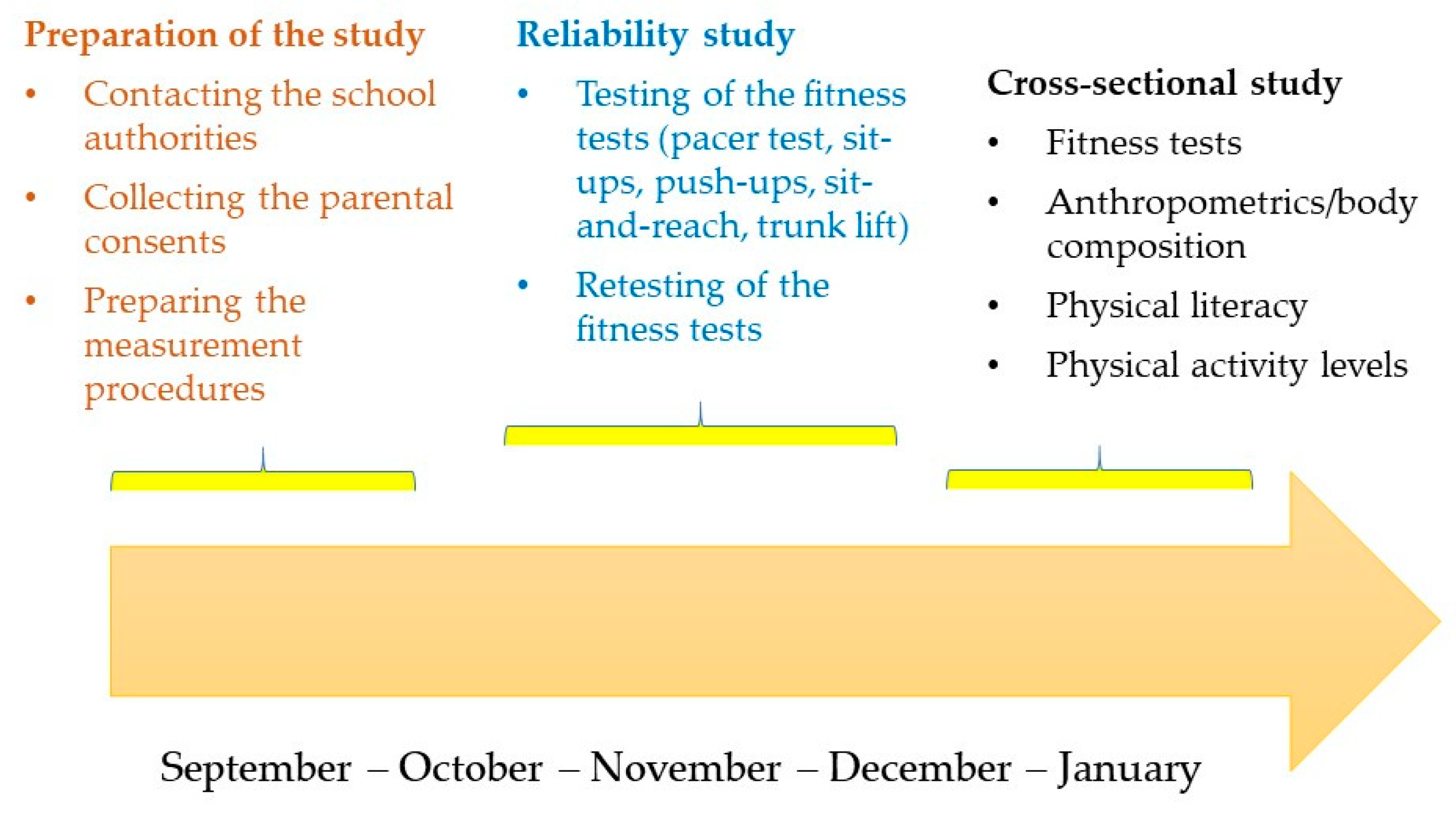
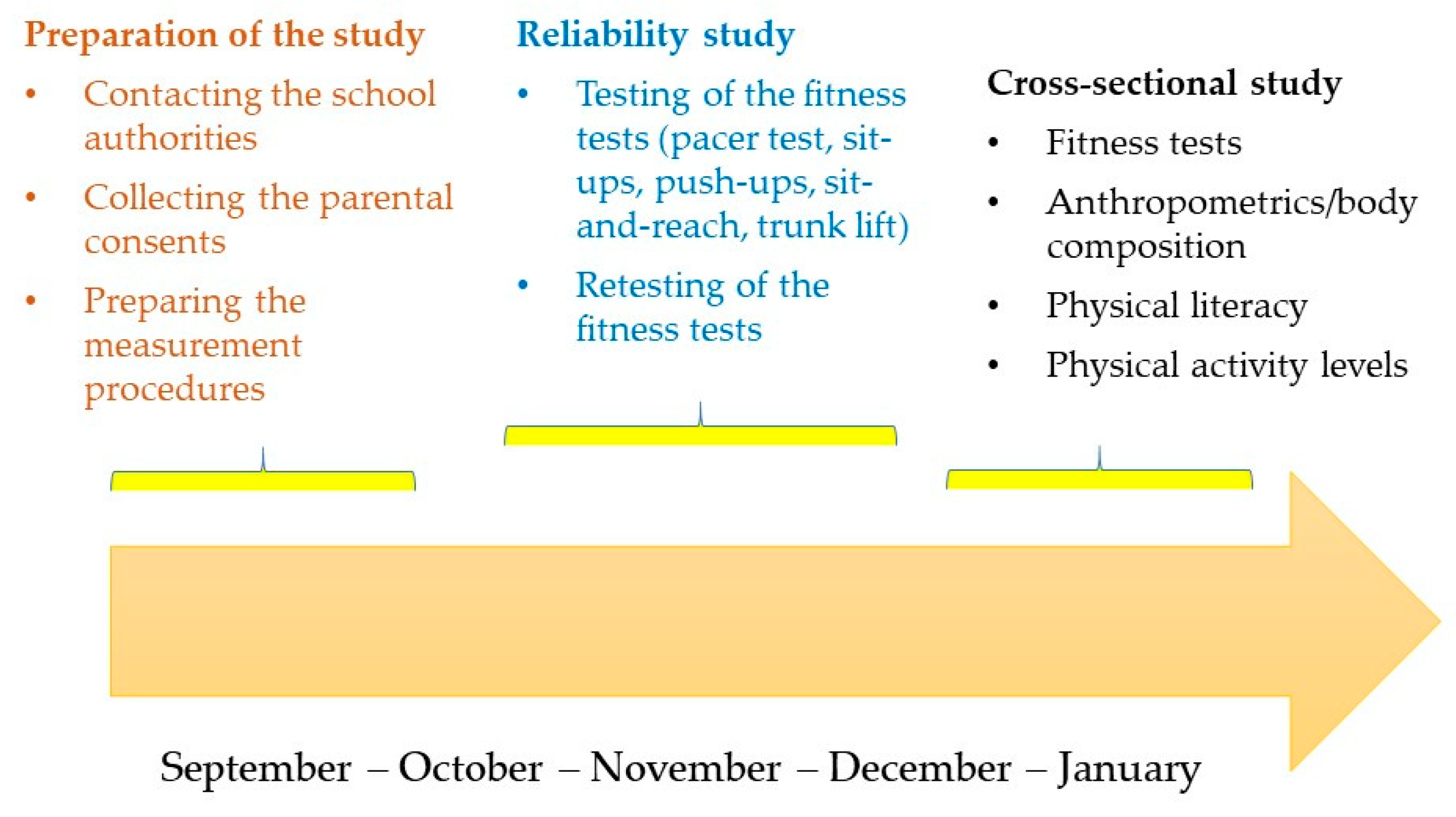
2.1. Participants and Study Design
2.2. Variables and Procedures
2.3. Statistics
3. Results
4. Discussion
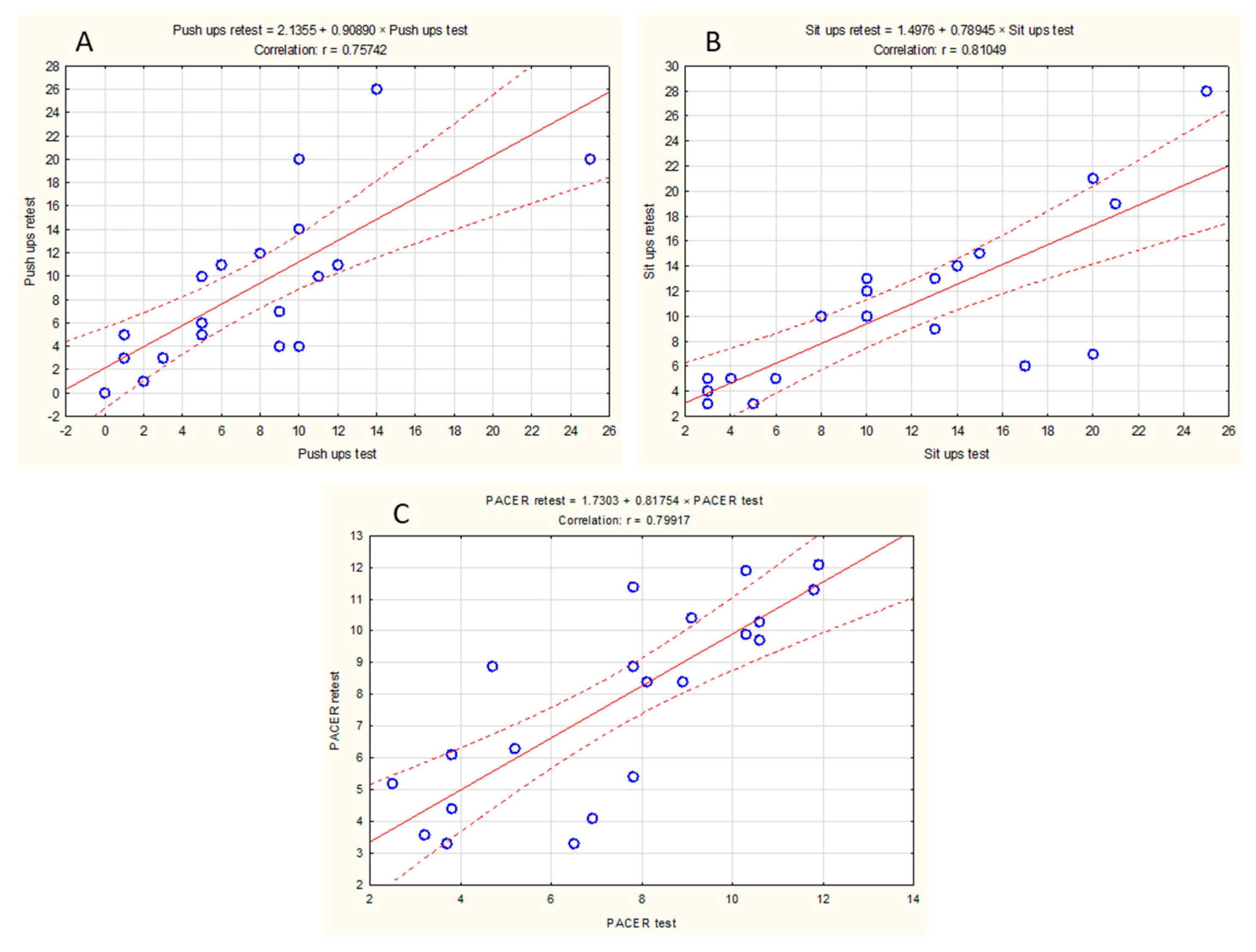
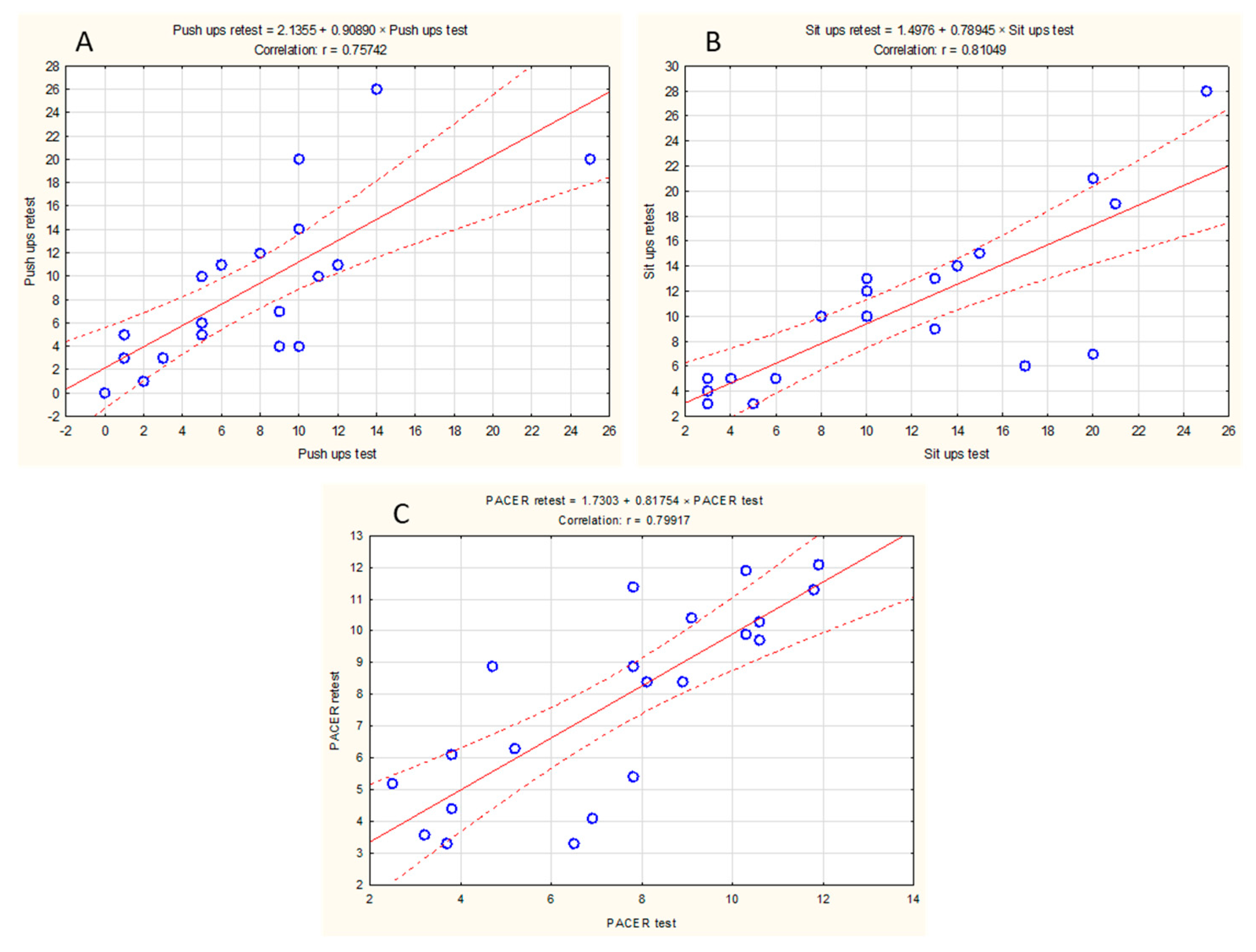
4.1. Reliability of the Physical Fitness Tests in Preadolescent Children
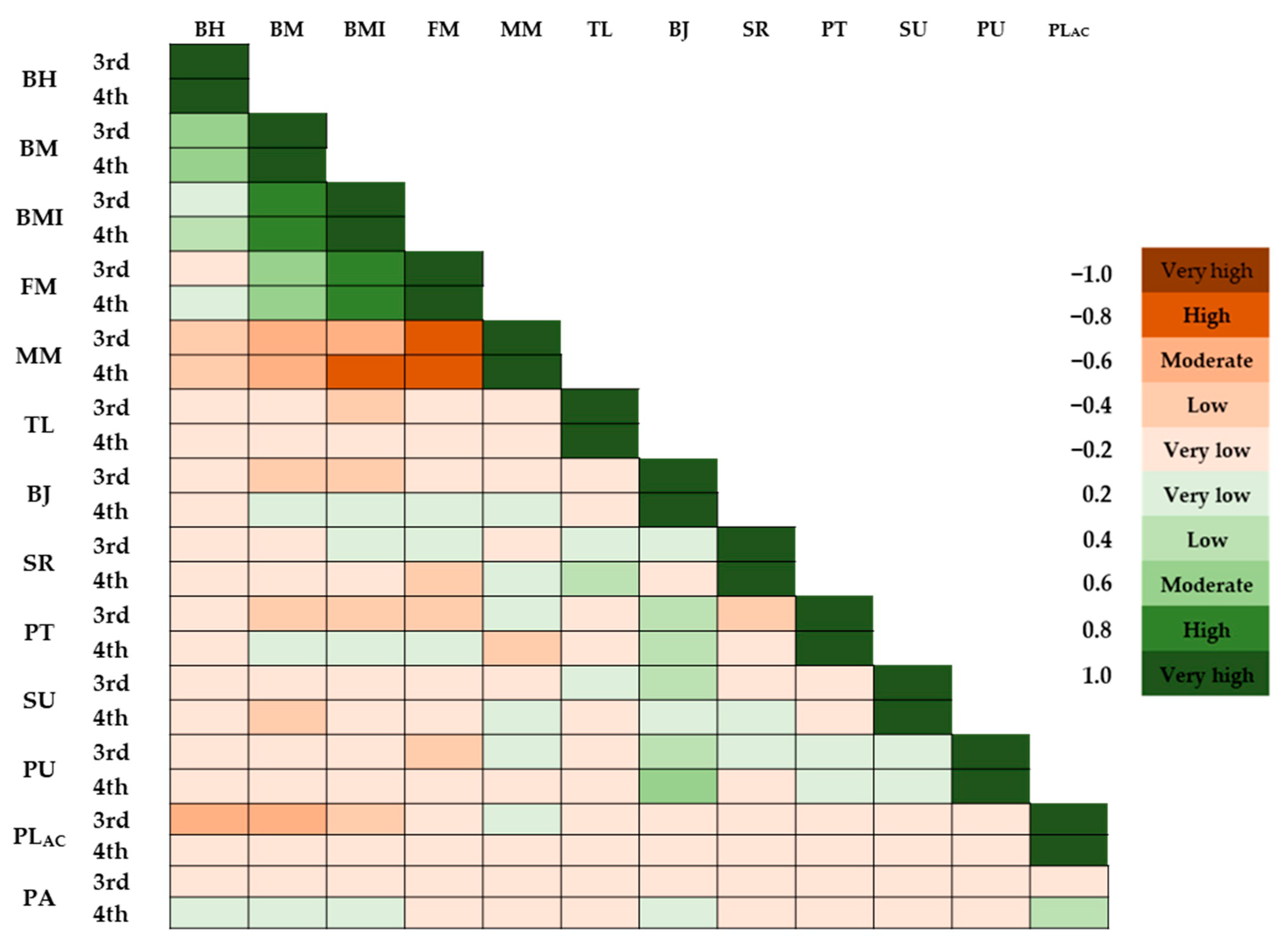
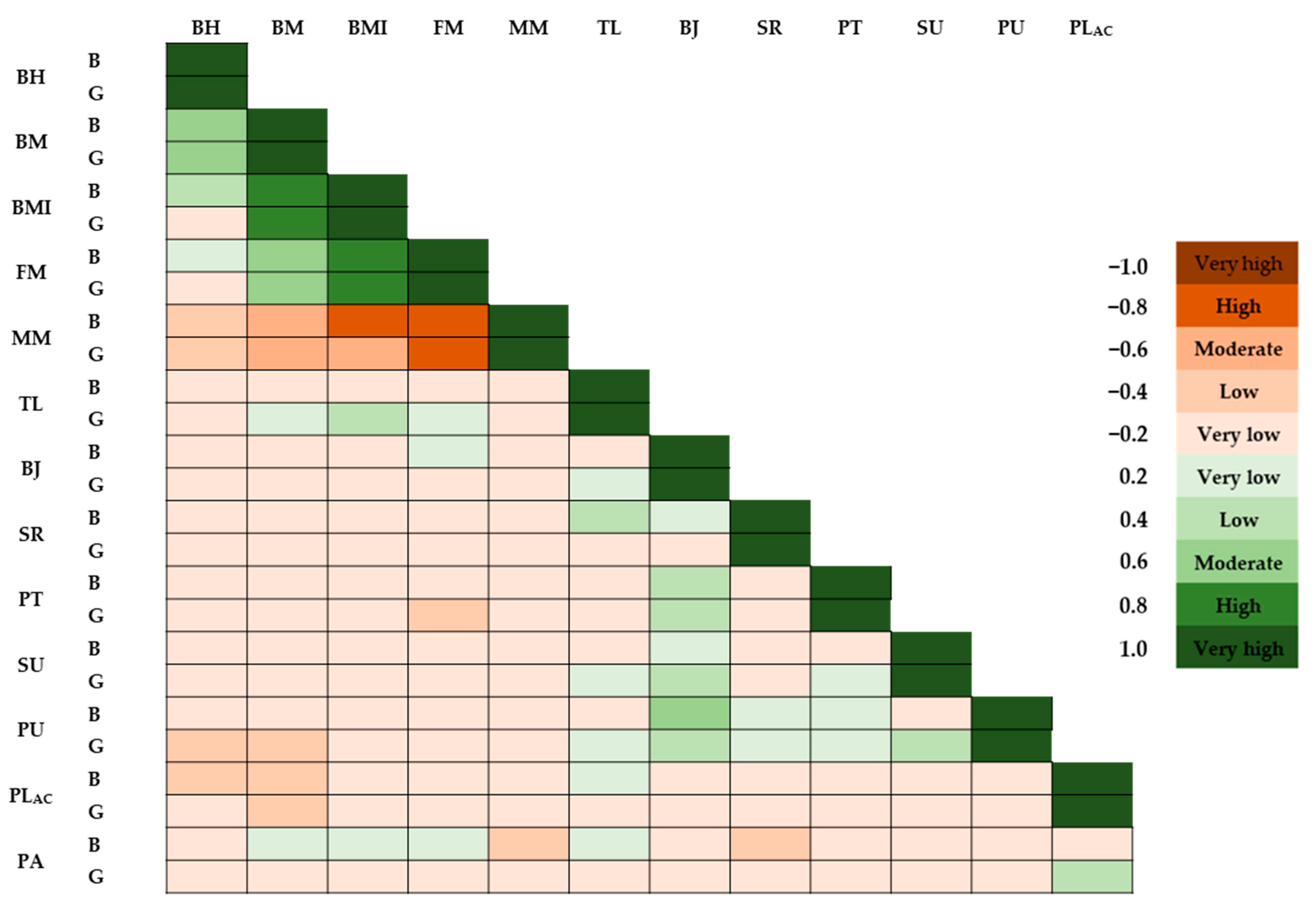
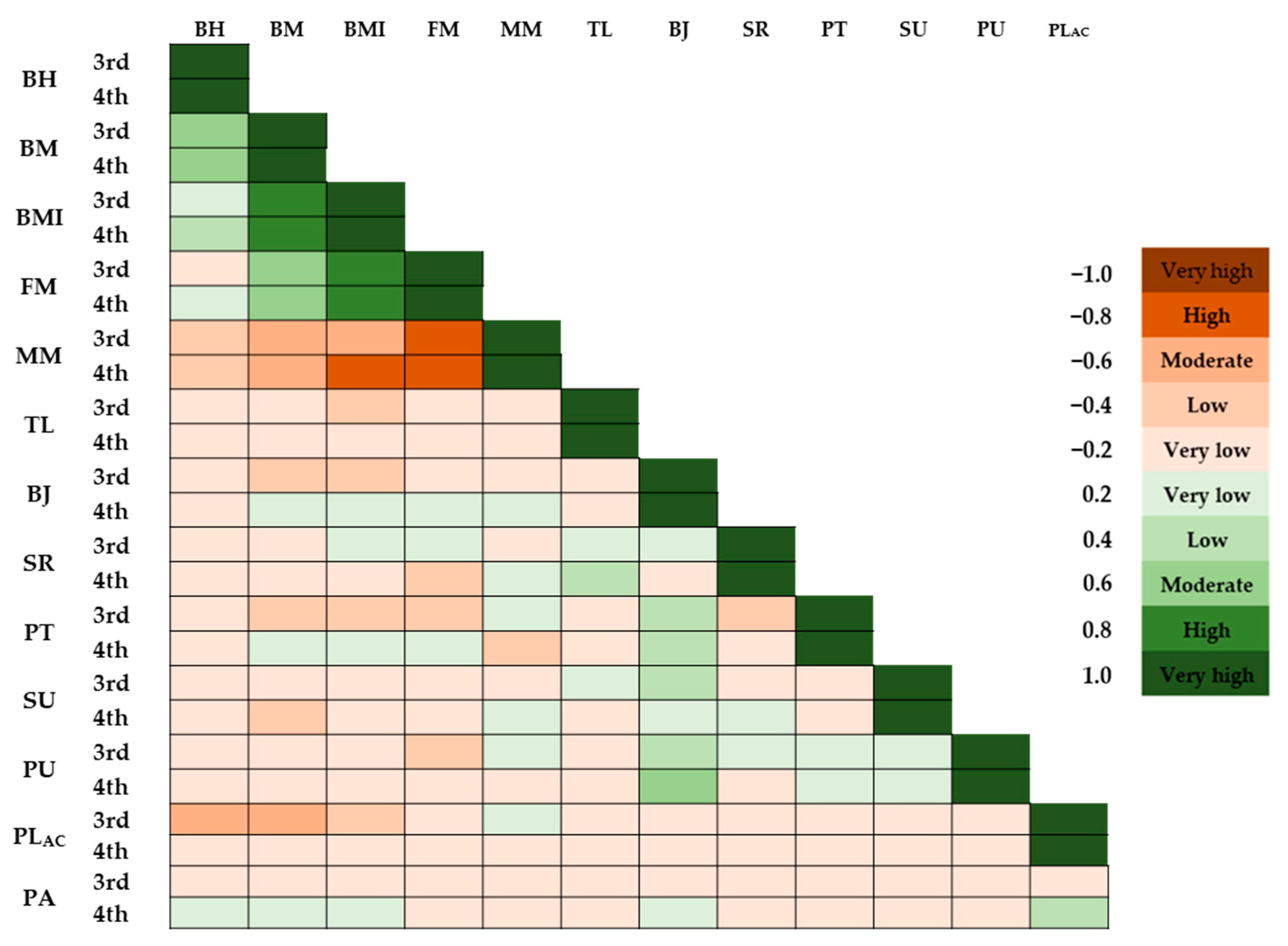
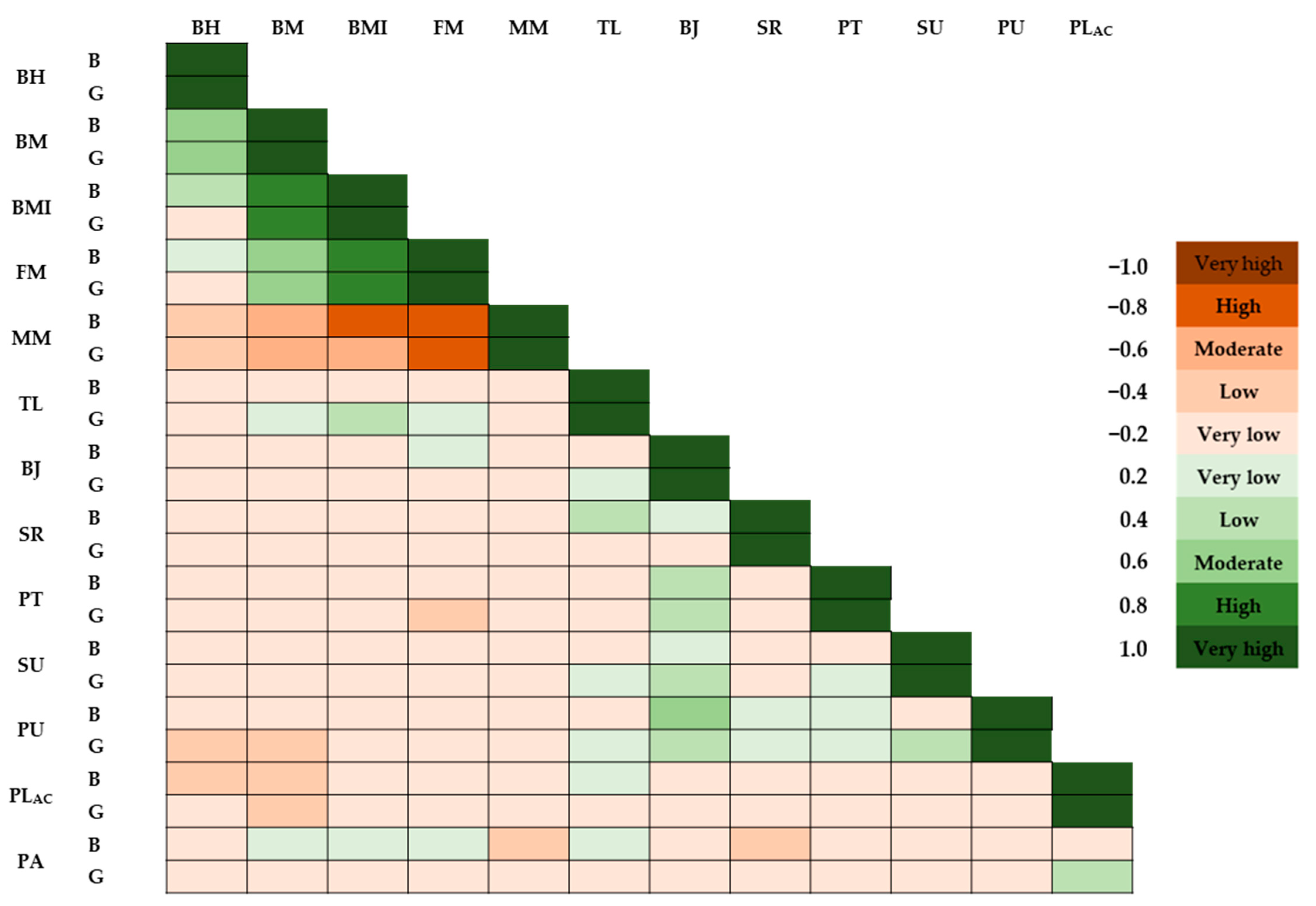
4.2. Association between Physical Literacy and Physical Fitness
4.3. Correlations between Physical Literacy and Physical Activity Levels
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siedentop, D.; Van der Mars, H. Introduction to Physical Education, Fitness, and Sport; Human kinetics: Champaign, IL, USA, 2022. [Google Scholar]
- Moliner-Urdiales, D.; Ruiz, J.R.; Ortega, F.B.; Jiménez-Pavón, D.; Vicente-Rodriguez, G.; Rey-López, J.P.; Martínez-Gómez, D.; Casajús, J.A.; Mesana, M.I.; Marcos, A.; et al. Secular trends in health-related physical fitness in Spanish adolescents The AVENA and HELENA Studies. J. Sci. Med. Sport 2010, 13, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Silventoinen, K.; Maia, J.; Jelenkovic, A.; Pereira, S.; Gouveia, É.; Antunes, A.; Thomis, M.; Lefevre, J.; Kaprio, J.; Freitas, D. Genetics of somatotype and physical fitness in children and adolescents. Am. J. Hum. Biol. 2021, 33, e23470. [Google Scholar] [CrossRef] [PubMed]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Brit J. Sport Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The Health Benefits of Muscular Fitness for Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef]
- Cadenas-Sanchez, C.; Mena-Molina, A.; Torres-Lopez, L.V.; Migueles, J.H.; Rodriguez-Ayllon, M.; Lubans, D.R.; Ortega, F.B. Healthier Minds in Fitter Bodies: A Systematic Review and Meta-Analysis of the Association between Physical Fitness and Mental Health in Youth. Sports Med. 2021, 51, 2571–2605. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Cantarero, A.; Álvarez-Bueno, C.; Martínez-Vizcaino, V.; Redondo-Tébar, A.; Pozuelo-Carrascosa, D.P.; Sánchez-López, M. Relationship between both cardiorespiratory and muscular fitness and health-related quality of life in children and adolescents: A systematic review and meta-analysis of observational studies. Health Qual. Life Outcomes 2021, 19, 127. [Google Scholar] [CrossRef]
- Rodriguez, C.C.; de Camargo, E.M.; Rodriguez-Añez, C.R.; Reis, R.S. Physical Activity, Physical Fitness and Academic Achievement in Adolescents: A Systematic Review. Rev. Bras. Med. Esporte 2020, 26, 441–448. [Google Scholar] [CrossRef]
- Alvarez-Pitti, J.; Mallen, J.A.C.; Trabazo, R.L.; Lucia, A.; de Lara, D.L.; Aznar, L.A.M.; Martinez, G.R. Exercise as medicine in chronic diseases during childhood and adolescence. An. Pediatr. 2020, 92, 173.e1–173.e8. [Google Scholar] [CrossRef]
- Ariza, C.; Sanchez-Martinez, F.; Serral, G.; Valmayor, S.; Juarez, O.; Pasarin, M.I.; Castell, C.; Rajmil, L.; Lopez, M.J.; Ariza, C.; et al. The Incidence of Obesity, Assessed as Adiposity, Is Reduced After 1 Year in Primary Schoolchildren by the POIBA Intervention. J. Nutr. 2019, 149, 258–269. [Google Scholar] [CrossRef]
- Whiting, S.; Buoncristiano, M.; Gelius, P.; Abu-Omar, K.; Pattison, M.; Hyska, J.; Duleva, V.; Musić Milanović, S.; Zamrazilová, H.; Hejgaard, T. Physical activity, screen time, and sleep duration of children aged 6–9 years in 25 countries: An analysis within the WHO European childhood obesity surveillance initiative (COSI) 2015–2017. Obes. Facts 2021, 14, 32–44. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1· 6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Giroir, B.P.; Wright, D. Physical Activity Guidelines for Health and Prosperity in the United States. J. Am. Med. Assoc. 2018, 320, 1971–1972. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, H.; Eslamis, B. Relationship Between Obesity, Physical Activity, and Cardiorespiratory Fitness Levels in Children and Adolescents in Bosnia and Herzegovina: An Analysis of Gender Differences. Front. Physiol. 2018, 9, 1734. [Google Scholar] [CrossRef] [PubMed]
- Escapite, A.O.; Lopez-Alonzo, S.J.; Barron-Lujan, J.C.; Guedea-Delgado, J.C.; Balderrama, C.V.V. Physical education, motor development and physical activity in preschool children: A systematic review. Viref-Rev. Educ. Fis. 2022, 11, 28–41. [Google Scholar]
- Goodyear, V.A.; Skinner, B.; McKeever, J.; Grifftiths, M. The influence of online physical activity interventions on children and young people‘s engagement with physical activity: A systematic review. Phys. Educ. Sport Peda 2023, 28, 94–108. [Google Scholar] [CrossRef]
- Holt, N.L.; Deal, C.J.; Pankow, K. Positive youth development through sport. In Handbook of Sport Psychology, 4th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2020; pp. 429–446. [Google Scholar]
- Kriemler, S.; Meyer, U.; Martin, E.; van Sluijs, E.M.F.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Brit J. Sport Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.W.R.; Kemper, H.C.G.; van Mechelen, W. The relationship between physical fitness and physical activity during adolescence and cardiovascular disease risk factors at adult age. The Amsterdam Growth and Health Longitudinal Study. Study Int. J. Sports Med. 2002, 23, S8–S14. [Google Scholar]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Vizcaíno, V.; Sánchez-López, M. Relación entre actividad física y condición física en niños y adolescentes. Elsevier Doyma 2008, 61, 108–111. [Google Scholar] [CrossRef]
- Whitehead, M. Definition of physical literacy and clarification of related issues. Icsspe Bull. 2013, 65, 28–33. [Google Scholar]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical Literacy, Physical Activity and Health: Toward an Evidence-Informed Conceptual Model. Sports Med. 2019, 49, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Holler, P.; Carl, J.; van Poppel, M.N.M.; Jaunig, J. Development of the Perceived Physical Literacy Questionnaire (PPLQ) for the adult population. J. Exerc. Sci. Fit. 2023, 21, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Shearer, C.; Goss, H.R.; Boddy, L.M.; Knowles, Z.R.; Durden-Myers, E.J.; Foweather, L. Assessments Related to the Physical, Affective and Cognitive Domains of Physical Literacy Amongst Children Aged 7–11.9 Years: A Systematic Review. Sports Med. Open 2021, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, S.L. Physical literacy in children and adolescents: Definitions, assessments, and interventions. Eur. Phys. Educ. Rev. 2021, 27, 96–112. [Google Scholar] [CrossRef]
- de Dieu, H.J.; Zhou, K. Physical Literacy Assessment Tools: A Systematic Literature Review for Why, What, Who, and How. Int. J. Environ. Res. Public Health 2021, 18, 7954. [Google Scholar] [CrossRef]
- Geets-Kesić, M.; Maras, N.; Gilić, B. Analysis of the Association Between Health Literacy, Physical Literacy, and Scholastic Achievement; A Preliminary Cross-Sectional Study Among High-School Students From Southern Croatia. Montenegrin J. Sports Sci. Med. 2023, 12. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, Y.; Xu, S.; Sum, R.K.W.; Ma, R.S.; Zhong, P.; Liu, S.X.; Li, M.H. Exploring the Level of Physical Fitness on Physical Activity and Physical Literacy Among Chinese University Students: A Cross-Sectional Study. Front. Psychol. 2022, 13, 833461. [Google Scholar] [CrossRef]
- Caldwell, H.A.T.; Di Cristofaro, N.A.; Cairney, J.; Bray, S.R.; MacDonald, M.J.; Timmons, B.W. Physical Literacy, Physical Activity, and Health Indicators in School-Age Children. Int. J. Environ. Res. Public Health 2020, 17, 5367. [Google Scholar] [CrossRef] [PubMed]
- Nezondet, C.; Gandrieau, J.; Nguyen, P.; Zunquin, G. Perceived Physical Literacy Is Associated with Cardiorespiratory Fitness, Body Composition and Physical Activity Levels in Secondary School Students. Children 2023, 10, 712. [Google Scholar] [CrossRef]
- Vuletic, P.R.; Kesic, M.G.; Gilic, B.; Pehar, M.; Uzicanin, E.; Idrizovic, K.; Sekulic, D. Evaluation of Physical Literacy in 9-to 11-Year-Old Children: Reliability and Validity of Two Measurement Tools in Three Southeastern European Countries. Children 2023, 10, 1722. [Google Scholar] [CrossRef]
- Kriellaars, D.; Kozera, T.; Robillard, B. Physical literacy assessment for youth. PLAY Workbook. Canadian Sport Institute—Pacific. 2013. Available online: http://sportforlife.ca/wp-content/uploads/2016/12/PLAYbasic-workbook.pdf (accessed on 10 February 2024).
- Crocker, P.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGrath, R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Samaržija, D.V.; Mišigoj-Duraković, M. Reliability of Croatian version of the questionnaire for assessment of overall level of physical activity of younger school children. Hrvat. Športskomedicinski Vjesn. 2013, 28, 24–32. [Google Scholar]
- Meredith, M.D.; Welk, G. Fitnessgram and Activitygram Test Administration Manual-Updated, 4th ed.; Human Kinetics: Champaign, IL, USA, 2010. [Google Scholar]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Hammond-Bennett, A.; Hypnar, A.; Mason, S. Health-related physical fitness and physical activity in elementary school students. BMC Public Health 2018, 18, 195. [Google Scholar] [CrossRef]
- Thomas, E.; Petrigna, L.; Tabacchi, G.; Teixeira, E.; Pajaujiene, S.; Sturm, D.J.; Sahin, F.N.; Gomez-Lopez, M.; Pausic, J.; Paoli, A.; et al. Percentile values of the standing broad jump in children and adolescents aged 6–18 years old. Eur. J. Transl. Myol. 2020, 30, 240–246. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Sekulic, D.; Uljevic, O.; Peric, M.; Spasic, M.; Kondric, M. Reliability and Factorial Validity of Non-Specific and Tennis-Specific Pre-Planned Agility Tests; Preliminary Analysis. J. Hum. Kinet. 2017, 55, 107–116. [Google Scholar] [CrossRef]
- Uljevic, O.; Esco, M.R.; Sekulic, D. Reliability, validity, and applicability of isolated and combined sport-specific tests of conditioning capacities in top-level junior water polo athletes. J. Strength. Cond. Res. 2014, 28, 1595–1605. [Google Scholar] [CrossRef]
- Gogoi, P.; Bhattacharyya, N.C. Interrater reliability of fitness gram test to be used as a reliable tool for assessing physical fitness for school children in guwahati urban society of north-east india. Int. J. Res. Med. Sci. 2020, 8, 312. [Google Scholar] [CrossRef]
- Morrow, J.R.; Martin, S.B.; Jackson, A.W. Reliability and Validity of the FITNESSGRAM®: Quality of Teacher-Collected Health-Related Fitness Surveillance Data. Res. Q. Exerc. Sport 2010, 81, S24–S30. [Google Scholar] [CrossRef]
- McManis, B.G.; Baumgartner, T.A.; Wuest, D.A. Objectivity and reliability of the 90 push-up test. Meas. Phys. Educ. Exerc. 2000, 4, 57–67. [Google Scholar] [CrossRef]
- Saint Romain, B.; Mahar, M.T. Norm-referenced and criterion-referenced reliability of the push-up and modified pull-up. Meas. Phys. Educ. Exerc. 2001, 5, 67–80. [Google Scholar] [CrossRef]
- Patterson, P.; Bennington, J.; De la Rosa, T. Psychometric properties of child- and teacher-reported curl-up scores in children ages 10–12 years. Res. Q. Exerc. Sport 2001, 72, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Pitetti, K.H.; Fernhall, B.; Figoni, S. Comparing two regression formulas that predict VO using the 20-m shuttle run for children and adolescents. Pediatr. Exerc. Sci. 2002, 14, 125–134. [Google Scholar] [CrossRef]
- Fernandez-Santos, J.R.; Ruiz, J.R.; Cohen, D.D.; Gonzalez-Montesinos, J.L.; Castro-Piñero, J. Reliability and Validity of Tests to Assess Lower-Body Muscular Power in Children. J. Strength. Cond. Res. 2015, 29, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Fjortoft, I.; Pedersen, A.V.; Sigmundsson, H.; Vereijken, B. Measuring Physical Fitness in Children Who Are 5 to 12 Years Old With a Test Battery That Is Functional and Easy to Administer. Phys. Ther. 2011, 91, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.; Malina, R.; Beunen, G. The contribution of biological maturation to the strength and motor fitness of children. Ann. Hum. Biol. 1997, 24, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Huck, S.W. Reading Statistics and Research: Pearson New International Edition; Pearson Education: London, UK, 2013. [Google Scholar]
- Neljak, B.; Novak, D.; Sporiš, G.; Višković, S.; Markuš, D. Cro-Fit Norme; Faculty of Kinesiology, University of Zagreb: Zagreb, Croatia, 2012. (In Croatian) [Google Scholar]
- Lang, J.J.; Chaput, J.P.; Longmuir, P.E.; Barnes, J.D.; Belanger, K.; Tomkinson, G.R.; Anderson, K.D.; Bruner, B.; Copeland, J.L.; Gregg, M.J.; et al. Cardiorespiratory fitness is associated with physical literacy in a large sample of Canadian children aged 8 to 12 years. BMC Public Health 2018, 18, 1041. [Google Scholar] [CrossRef] [PubMed]
- Gilic, B.; Malovic, P.; Sunda, M.; Maras, N.; Zenic, N. Adolescents with Higher Cognitive and Affective Domains of Physical Literacy Possess Better Physical Fitness: The Importance of Developing the Concept of Physical Literacy in High Schools. Children 2022, 9, 796. [Google Scholar] [CrossRef]
- Jones, M.A.; Hitchen, P.J.; Stratton, G. The importance of considering biological maturity when assessing physical fitness measures in girls and boys aged 10 to 16 years. Ann. Hum. Biol. 2000, 27, 57–65. [Google Scholar] [CrossRef]
- Marta, C.C.; Marinho, D.A.; Izquierdo, M.; Marques, M.C. Differentiating maturational influence on training-induced strength and endurance adaptations in prepubescent children. Am. J. Hum. Biol. 2014, 26, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Belanger, K.; Barnes, J.D.; Longmuir, P.E.; Anderson, K.D.; Bruner, B.; Copeland, J.L.; Gregg, M.J.; Hall, N.; Kolen, A.M.; Lane, K.N.; et al. The relationship between physical literacy scores and adherence to Canadian physical activity and sedentary behaviour guidelines. Bmc Public Health 2018, 18, 1042. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Meng, Y.; Wang, L.; Zhang, T.; Chen, L.; Li, H. Research on the Relationship between Physical Literacy, Physical Activity and Sedentary Behavior. Int. J. Environ. Res. Public Health 2022, 19, 16455. [Google Scholar] [CrossRef] [PubMed]
- Cairney, J.; Clark, H.J.; James, M.E.; Mitchell, D.; Dudley, D.A.; Kriellaars, D. The Preschool Physical Literacy Assessment Tool: Testing a New Physical Literacy Tool for the Early Years. Front. Pediatr. 2018, 6, 138. [Google Scholar] [CrossRef] [PubMed]
- Bucksch, J.; Sigmundova, D.; Hamrik, Z.; Troped, P.J.; Melkevik, O.; Ahluwalia, N.; Borraccino, A.; Tynjälä, J.; Kalman, M.; Inchley, J. International Trends in Adolescent Screen-Time Behaviors From 2002 to 2010. J. Adolesc. Health 2016, 58, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Jekauc, D.; Reimers, A.K.; Wagner, M.O.; Woll, A. Physical activity in sports clubs of children and adolescents in Germany: Results from a nationwide representative survey. J. Public Health-Heid 2013, 21, 505–513. [Google Scholar] [CrossRef]
- Kalman, M.; Inchley, J.; Sigmundova, D.; Iannotti, R.J.; Tynjälä, J.A.; Hamrik, Z.; Haug, E.; Bucksch, J. Secular trends in moderate-to-vigorous physical activity in 32 countries from 2002 to 2010: A cross-national perspective. Eur. J. Public Health 2015, 25, 37–40. [Google Scholar] [CrossRef]
- Van Hecke, L.; Loyen, A.; Verloigne, M.; van der Ploeg, H.P.; Lakerveld, J.; Brug, J.; De Bourdeaudhuij, I.; Ekelund, U.; Donnelly, A.; Hendriksen, I.; et al. Variation in population levels of physical activity in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phy 2016, 13, 70. [Google Scholar] [CrossRef] [PubMed]
- Carsley, S.; Liang, L.Y.; Chen, Y.; Parkin, P.; Maguire, J.; Birken, C.S.; Collaboration, T.A.K. The impact of daycare attendance on outdoor free play in young children. J. Public Health 2017, 39, 145–152. [Google Scholar] [CrossRef]
- Jefferies, P.; Bremer, E.; Kozera, T.; Cairney, J.; Kriellaars, D. Psychometric properties and construct validity of PLAYself: A self-reported measure of physical literacy for children and youth. Appl. Physiol. Nutr. Metab. 2021, 46, 579–588. [Google Scholar] [CrossRef]
- Šunda, M. Utjecaj Učenja na Daljinu i Unaprjeđenja Tjelesne Pismenosti na Promjene Stanja Fitnesa i Tjelesne Aktivnosti Adolescenata. Ph.D. Thesis, Faculty of Kinesiology, University of Zagreb, Zagreb, Croatia, 2022. [Google Scholar]
- Sunda, M.; Gilic, B.; Sekulic, D.; Matic, R.; Drid, P.; Alexe, D.I.; Cucui, G.G.; Lupu, G.S. Out-of-School Sports Participation Is Positively Associated with Physical Literacy, but What about Physical Education? A Cross-Sectional Gender-Stratified Analysis during the COVID-19 Pandemic among High-School Adolescents. Children 2022, 9, 753. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Salmon, J.; Parrish, A.M.; Stanley, R.M.; Okely, A.D. Physical Activity During School Recess A Systematic Review. Am. J. Prev. Med. 2012, 43, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Chen, S.; Zhang, X. Physical Literacy at the Start Line: Young Children’s Motor Competence, Fitness, Physical Activity, and Fitness Knowledge. J. Teach. Phys. Educ. 2019, 38, 146–154. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICC | 95% CI | |
|---|---|---|
| Trunk lift | 0.66 | 0.61–0.71 |
| Broad jump | 0.91 | 0.89–0.93 |
| Sit and reach | 0.83 | 0.80–0.86 |
| Main Effects | Interaction | |||||
|---|---|---|---|---|---|---|
| Group | Gender | Group x Gender | ||||
| F-Test | p | F-Test | p | F-Test | p | |
| Body height | 3.31 | 0.07 | 0.78 | 0.38 | 1.53 | 0.22 |
| Body mass | 0.40 | 0.53 | 0.29 | 0.59 | 5.09 | 0.03 |
| Body mass index | 0.42 | 0.52 | 0.05 | 0.82 | 4.2 | 0.04 |
| Fat mass | 0.32 | 0.57 | 0.01 | 0.94 | 7.86 | 0.01 |
| Muscle mass | 0.86 | 0.36 | 0.20 | 0.65 | 4.00 | 0.06 |
| Torso lift | 0.47 | 0.49 | 14.31 | 0.001 | 0.01 | 0.94 |
| Broad jump | 6.05 | 0.02 | 2.68 | 0.11 | 0.22 | 0.64 |
| Sit and reach | 0.88 | 0.35 | 18.82 | 0.001 | 0.09 | 0.76 |
| PACER | 1.22 | 0.29 | 12.11 | 0.001 | 3.47 | 0.08 |
| Sit-ups | 0.73 | 0.40 | 0.87 | 0.35 | 0.05 | 0.82 |
| Push-ups | 0.56 | 0.46 | 7.55 | 0.01 | 2.38 | 0.13 |
| PLAYself | 0.46 | 0.50 | 0.00 | 1.00 | 0.39 | 0.53 |
| PAQ-C | 3.55 | 0.06 | 0.23 | 0.63 | 1.17 | 0.28 |
| Third Grade | Fourth Grade | |||
|---|---|---|---|---|
| Boys (n = 27) | Girls (n = 25) | Boys (n = 27) | Girls (n = 28) | |
| Body height (cm) | 143.79 ± 5.8 | 143.85 ± 6.2 | 147.42 ± 6.29 | 144.93 ± 7.06 |
| Body mass (kg) | 36.37 ± 7.34 * ¥ | 39.1 ± 8.63 ¥ | 40.54 ± 8.78 * | 36.49 ± 7.49 |
| Body mass index (kg/m2) | 17.49 ± 2.8 * | 18.83 ± 3.54 ¥ | 18.32 ± 3.05 | 17.24 ± 2.47 |
| Fat mass (%) | 22.86 ± 4.08 *¥ | 25.78 ± 5.57 | 25.64 ± 6.43 | 23.55 ± 5.2 |
| Muscle mass (%) | 43.67 ± 2.31 | 42.52 ± 3.85 | 42.08 ± 3.63 | 43.26 ± 2.95 |
| Torso lift (cm) | 16.62 ± 3.88 * | 19.45 ± 5.19 | 17.46 ± 4.45 * | 20.48 ± 3.94 |
| Broad jump (cm) | 134.79 ± 19.38 | 131.00 ± 13.58 | 145.71 ± 20.63 | 137.16 ± 22.15 |
| Sit and reach (cm) | 42.41 ± 7.72 * | 53.00 ± 15.27 | 41.75 ± 11.4 * | 55.00 ± 9.69 |
| PACER (ml/kg/min) | 56.65 ± 6.81 * | 50.85 ± 4.5 | 54.63 ± 6.5 | 52.32 ± 3.9 |
| Sit-ups (reps) | 12.24 ± 8.46 | 13.82 ± 13.92 | 9.83 ± 6.91 | 12.32 ± 10.17 |
| Push-ups (reps) | 8.97 ± 6.39 * | 6.5 ± 6.05 | 11.73 ± 9.96 * | 6.2 ± 6.79 |
| PLAYself (score) | 71.6 ± 13.31 | 73.06 ± 10.66 | 75.18 ± 8.69 | 73.57 ± 10.99 |
| PAQ-C (score) | 3.38 ± 0.62 | 3.43 ± 0.68 | 3.69 ± 0.38 | 3.48 ± 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajkovic Vuletic, P.; Gilic, B.; Zenic, N.; Pavlinovic, V.; Kesic, M.G.; Idrizovic, K.; Sunda, M.; Manojlovic, M.; Sekulic, D. Analyzing the Associations between Facets of Physical Literacy, Physical Fitness, and Physical Activity Levels: Gender- and Age-Specific Cross-Sectional Study in Preadolescent Children. Educ. Sci. 2024, 14, 391. https://doi.org/10.3390/educsci14040391
Rajkovic Vuletic P, Gilic B, Zenic N, Pavlinovic V, Kesic MG, Idrizovic K, Sunda M, Manojlovic M, Sekulic D. Analyzing the Associations between Facets of Physical Literacy, Physical Fitness, and Physical Activity Levels: Gender- and Age-Specific Cross-Sectional Study in Preadolescent Children. Education Sciences. 2024; 14(4):391. https://doi.org/10.3390/educsci14040391
Chicago/Turabian StyleRajkovic Vuletic, Petra, Barbara Gilic, Natasa Zenic, Vladimir Pavlinovic, Marijana Geets Kesic, Kemal Idrizovic, Mirela Sunda, Marko Manojlovic, and Damir Sekulic. 2024. "Analyzing the Associations between Facets of Physical Literacy, Physical Fitness, and Physical Activity Levels: Gender- and Age-Specific Cross-Sectional Study in Preadolescent Children" Education Sciences 14, no. 4: 391. https://doi.org/10.3390/educsci14040391
APA StyleRajkovic Vuletic, P., Gilic, B., Zenic, N., Pavlinovic, V., Kesic, M. G., Idrizovic, K., Sunda, M., Manojlovic, M., & Sekulic, D. (2024). Analyzing the Associations between Facets of Physical Literacy, Physical Fitness, and Physical Activity Levels: Gender- and Age-Specific Cross-Sectional Study in Preadolescent Children. Education Sciences, 14(4), 391. https://doi.org/10.3390/educsci14040391