
A Quantitative Cross-Sectional Study on the Behavioral Intentions of Polish Medical and Healthcare Students Regarding Interprofessional Collaboration in Their Future Clinical Practice

 ,
, 
 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Questionnaire Development
2.2. Study Settings, Procedure, and Data Analysis
3. Results
3.1. Study Group
3.2. Attitudes
3.3. Subjective Norms
3.4. Perceived Behavioral Control
3.5. Generalized Behavioral Intention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perron, D.; Parent, K.; Gaboury, I.; Bergeron, D.A. Characteristics, barriers and facilitators of initiatives to develop interprofessional collaboration in rural and remote primary healthcare facilities: A scoping review. Rural Remote Health 2022, 22, 7566. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, E.M.; Marvel, F.A.; Jacob, E.; Rahman, A.; Hansen, B.R.; Hanyok, L.A.; Martin, S.S.; Han, H.-R. Interprofessional education and collaboration among healthcare students and professionals: A systematic review and call for action. J. Interprof. Care 2021, 35, 612–621. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Framework for Action on Interprofessional Education & Collaborative Practice. Available online: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice (accessed on 18 August 2024).
- Lee, W.; Kim, M.; Kang, Y.; Lee, Y.-J.; Kim, S.M.; Lee, J.; Hyun, S.-J.; Yu, J.; Park, Y.-S. Nursing and medical students’ perceptions of an interprofessional simulation-based education: A qualitative descriptive study. Korean J. Med. Educ. 2020, 32, 317–327. [Google Scholar] [CrossRef]
- Song, H.-Y.; Nam, K.A. The Need for and Perceptions of Interprofessional Education and Collaboration Among Undergraduate Students in Nursing and Medicine in South Korea. J. Multidiscip. Healthc. 2022, 15, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Lestari, E.; Stalmeijer, R.E.; Widyandana, D.; Scherpbier, A. Does PBL deliver constructive collaboration for students in interprofessional tutorial groups? BMC Med. Educ. 2019, 19, 360. [Google Scholar] [CrossRef] [PubMed]
- Szafran, J.C.H.; Thompson, K.; Pincavage, A.T.; Saathoff, M.; Kostas, T. Interprofessional Education Without Limits: A Video-Based Workshop. MedEdPORTAL 2021, 17, 11125. [Google Scholar] [CrossRef]
- Piquette, D.; Reeves, S.; Leblanc, V.R. Interprofessional intensive care unit team interactions and medical crises: A qualitative study. J. Interprof. Care 2009, 23, 273–285. [Google Scholar] [CrossRef]
- Mangione-Smith, R.; Schonlau, M.; Chan, K.S.; Keesey, J.; Rosen, M.; Louis, T.A.; Keeler, E. Measuring the effectiveness of a collaborative for quality improvement in pediatric asthma care: Does implementing the chronic care model improve processes and outcomes of care? Ambul. Pediatr. 2005, 5, 75–82. [Google Scholar] [CrossRef]
- Rawlinson, C.; Carron, T.; Cohidon, C.; Arditi, C.; Hong, Q.N.; Pluye, P.; Peytremann-Bridevaux, I.; Gilles, I. An Overview of Reviews on Interprofessional Collaboration in Primary Care: Effectiveness. Int. J. Integr. Care 2021, 21, 31. [Google Scholar] [CrossRef]
- Clark, C.E.; Smith, L.F.P.; Taylor, R.S.; Campbell, J.L. Nurse led interventions to improve control of blood pressure in people with hypertension: Systematic review and meta-analysis. BMJ 2010, 341, 491. [Google Scholar] [CrossRef]
- Gaul, C.; Visscher, C.M.; Bhola, R.; Sorbi, M.J.; Galli, F.; Rasmussen, A.V.; Jensen, R. Team players against headache: Multidisciplinary treatment of primary headaches and medication overuse headache. J. Headache Pain 2011, 12, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.L.; Doucette, W.R.; Franciscus, C.L.; Ardery, G.; Kluesner, K.M.; Chrischilles, E.A. Deterioration of blood pressure control after discontinuation of a physician-pharmacist collaborative intervention. Pharmacotherapy 2010, 30, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Prentice, D.; Engel, J.; Taplay, K.; Stobbe, K. Interprofessional Collaboration: The Experience of Nursing and Medical Students’ Interprofessional Education. Glob. Qual. Nurs. Res. 2015, 2, 233339361456056. [Google Scholar] [CrossRef] [PubMed]
- Friman, A.; Wiegleb Edström, D.; Edelbring, S. Attitudes and perceptions from nursing and medical students towards the other profession in relation to wound care. J. Interprof. Care 2017, 31, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Kangas, S.; Jaatinen, P.; Metso, S.; Paavilainen, E.; Rintala, T.-M. Students’ perceptions of interprofessional collaboration on the care of diabetes: A qualitative study. Nurse Educ. Pract. 2021, 53, 103023. [Google Scholar] [CrossRef]
- Zielińska-Tomczak, Ł.; Cerbin-Koczorowska, M.; Przymuszała, P.; Marciniak, R. How to effectively promote interprofessional collaboration?—A qualitative study on physicians’ and pharmacists’ perspectives driven by the theory of planned behavior. BMC Health Serv. Res. 2021, 21, 903. [Google Scholar] [CrossRef]
- Müller, C.; Zimmermann, L.; Körner, M. Förderfaktoren und Barrieren interprofessioneller Kooperation in Rehabilitationskliniken—Eine Befragung von Führungskräften. Rehabilitation 2014, 53, 390–395. [Google Scholar] [CrossRef]
- de la Peña, I.; Koch, J. Teaching Intellectual Humility Is Essential in Preparing Collaborative Future Pharmacists. Am. J. Pharm. Educ. 2021, 85, 8444. [Google Scholar] [CrossRef]
- Katoue, M.G.; Awad, A.I.; Al-Jarallah, A.; Al-Ozairi, E.; Schwinghammer, T.L. Medical and pharmacy students’ attitudes towards physician-pharmacist collaboration in Kuwait. Pharm. Pract. 2017, 15, 1029. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Efficacy of the Theory of Planned Behaviour: A meta-analytic review. Br. J. Soc. Psychol. 2001, 40, 471–499. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Durning, S.J. Education and service: How theories can help in understanding tensions. Med. Educ. 2019, 53, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. Constructing a Theory of Planned Behavior Questionnaire. Available online: https://people.umass.edu/aizen/pdf/tpb.measurement.pdf (accessed on 18 August 2024).
- Francis, J.; Eccles, M.P.; Johnston, M.; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers; Centre for Health Services Research, University of Newcastle upon Tyne.: Newcastle upon Tyne, UK, 2004; Volume 37, ISBN 0954016157. [Google Scholar]
- British Educational Research Association (BERA) Ethical Guidelines for Educational Research, Fourth Edition. 2018. Available online: https://www.bera.ac.uk/researchers-resources/publications/ethical-guidelines-for-educational-research-2018 (accessed on 18 August 2024).
- Krejcie, R.V.; Morgan, D.W. Determining sample size for research activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Avrech Bar, M.; Katz Leurer, M.; Warshawski, S.; Itzhaki, M. The role of personal resilience and personality traits of healthcare students on their attitudes towards interprofessional collaboration. Nurse Educ. Today 2018, 61, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Cerbin-Koczorowska, M.; Przymuszała, P.; Michalak, M.; Piotrowska-Brudnicka, S.E.; Kant, P.; Skowron, A. Comparison of medical and pharmacy students’ readiness for interprofessional learning—A cross-sectional study. Farmacia 2020, 68, 1166–1172. [Google Scholar] [CrossRef]
- El-Awaisi, A.; Saffouh El Hajj, M.; Joseph, S.; Diack, L. Perspectives of pharmacy students in Qatar toward interprofessional education and collaborative practice: A mixed methods study. J. Interprof. Care 2018, 32, 674–688. [Google Scholar] [CrossRef]
- Kara, A.; DeMeester, D.; Lazo, L.; Cook, E.; Hendricks, S. An interprofessional patient assessment involving medical and nursing students: A qualitative study. J. Interprof. Care 2018, 32, 513–516. [Google Scholar] [CrossRef]
- Seaman, K.; Saunders, R.; Dugmore, H.; Tobin, C.; Singer, R.; Lake, F. Shifts in nursing and medical students’ attitudes, beliefs and behaviours about interprofessional work: An interprofessional placement in ambulatory care. J. Clin. Nurs. 2018, 27, 3123–3130. [Google Scholar] [CrossRef]
- Kaifi, A.; Tahir, M.A.; Ibad, A.; Shahid, J.; Anwar, M. Attitudes of nurses and physicians toward nurse–physician interprofessional collaboration in different hospitals of Islamabad–Rawalpindi Region of Pakistan. J. Interprof. Care 2021, 35, 863–868. [Google Scholar] [CrossRef]
- Vestergaard, E.; Nørgaard, B. Interprofessional collaboration: An exploration of possible prerequisites for successful implementation. J. Interprof. Care 2018, 32, 185–195. [Google Scholar] [CrossRef]
- Khalili, H.; Orchard, C.; Laschinger, H.K.S.; Farah, R. An interprofessional socialization framework for developing an interprofessional identity among health professions students. J. Interprof. Care 2013, 27, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Straub, C.; Bode, S.F.N. Patients’ and parents’ perception of care on a paediatric interprofessional training ward. BMC Med. Educ. 2019, 19, 374. [Google Scholar] [CrossRef] [PubMed]
- State of Health in the EU. Poland. Country Health Profile 2017. Available online: https://www.euro.who.int/__data/assets/pdf_file/0006/355992/Health-Profile-Poland-Eng.pdf (accessed on 18 August 2024).
- Mandy, A.; Milton, C.; Mandy, P. Professional stereotyping and interprofessional education. Learn. Health Soc. Care 2004, 3, 154–170. [Google Scholar] [CrossRef]
- Lewitt, M.S.; Ehrenborg, E.; Scheja, M.; Brauner, A. Stereotyping at the undergraduate level revealed during interprofessional learning between future doctors and biomedical scientists. J. Interprof. Care 2010, 24, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Reeves, S.; Tassone, M.; Parker, K.; Wagner, S.J.; Simmons, B. Interprofessional education: An overview of key developments in the past three decades. Work 2012, 41, 233–245. [Google Scholar] [CrossRef]
- Salberg, J.; Ramklint, M.; Öster, C. Nursing and medical students’ experiences of interprofessional education during clinical training in psychiatry. J. Interprof. Care 2022, 36, 582–588. [Google Scholar] [CrossRef]
- Zielińska-Tomczak, Ł.; Cerbin-Koczorowska, M.; Przymuszała, P.; Gałązka, N.; Marciniak, R. Pharmacists’ Perspectives on Interprofessional Collaboration with Physicians in Poland: A Quantitative Study. Int. J. Environ. Res. Public Health 2021, 18, 9686. [Google Scholar] [CrossRef]
- Axelsson, M.; Jakobsson, J.; Carlson, E. Which nursing students are more ready for interprofessional learning? A cross-sectional study. Nurse Educ. Today 2019, 79, 117–123. [Google Scholar] [CrossRef]
- Wilhelmsson, M.; Ponzer, S.; Dahlgren, L.-O.; Timpka, T.; Faresjö, T. Are female students in general and nursing students more ready for teamwork and interprofessional collaboration in healthcare? BMC Med. Educ. 2011, 11, 15. [Google Scholar] [CrossRef]
- Seselja-Perisin, A.; Mestrovic, A.; Klinar, I.; Modun, D. Health care professionals’ and students’ attitude toward collaboration between pharmacists and physicians in Croatia. Int. J. Clin. Pharm. 2016, 38, 16–19. [Google Scholar] [CrossRef]
- Thistlethwaite, J.; Moran, M. Learning outcomes for interprofessional education (IPE): Literature review and synthesis. J. Interprof. Care 2010, 24, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Kent, F.; Keating, J.L. Interprofessional education in primary health care for entry level students—A systematic literature review. Nurse Educ. Today 2015, 35, 1221–1231. [Google Scholar] [CrossRef]
- MacLeod, C.E.; Brady, D.R.; Maynard, S.P. Measuring the effect of simulation experience on perceived self-efficacy for interprofessional collaboration among undergraduate nursing and social work students. J. Interprof. Care 2022, 36, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Cerbin-Koczorowska, M.; Przymuszała, P.; Michalak, M.; Skowron, A. Effective interprofessional training can be implemented without high financial expenses—A prepost study supported with cost analysis. Farmacia 2022, 70, 976–984. [Google Scholar] [CrossRef]
- Cropp, C.; Beall, J.; Buckner, E.; Wallis, F.; Barron, A. Interprofessional Pharmacokinetics Simulation: Pharmacy and Nursing Students’ Perceptions. Pharmacy 2018, 6, 70. [Google Scholar] [CrossRef] [PubMed]
- Rotz, M.E.; Dueñas, G.G.; Zanoni, A.; Grover, A.B. Designing and Evaluating an Interprofessional Experiential Course Series Involving Medical and Pharmacy Students. Am. J. Pharm. Educ. 2016, 80, 85. [Google Scholar] [CrossRef]
- Ferri, P.; Rovesti, S.; Magnani, D.; Barbieri, A.; Bargellini, A.; Mongelli, F.; Bonetti, L.; Vestri, A.; Alunni Fegatelli, D.; Di Lorenzo, R. The efficacy of interprofessional simulation in improving collaborative attitude between nursing students and residents in medicine. A study protocol for a randomised controlled trial. Acta Biomed. 2018, 89, 32–40. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Gender | Female | 453 (78.8%) |
| Male | 113 (19.7%) | |
| Other | 4 (0.7%) | |
| I don’t want to disclose | 5 (0.9%) | |
| Year of study | 1st year of bachelor studies or uniform master’s studies | 284 (49.4%) |
| 2nd year of bachelor studies or uniform master’s studies | 131 (22.6%) | |
| 3rd year of bachelor studies or uniform master’s studies | 88 (15.3%) | |
| 4th year of uniform master’s studies or 1st year of master’s studies | 34 (5.9%) | |
| 5th year of uniform master’s studies or 2nd year of master’s studies | 32 (5.6%) | |
| 6th year of uniform master’s studies | 7 (1.2%) | |
| Degree course | medicine | 222 (38.6%) |
| nursing | 92 (16.0%) | |
| laboratory medicine | 68 (11.8%) | |
| physiotherapy | 39 (6.8%) | |
| dentistry | 34 (5.9%) | |
| midwifery | 24 (4.2%) | |
| medical rescue | 23 (4.0%) | |
| occupational therapy | 21 (3.7%) | |
| pharmacy | 18 (3.1%) | |
| public health | 15 (2.6%) | |
| dental techniques studies | 9 (1.6%) | |
| electroradiology | 5 (0.9%) | |
| cosmetology | 2 (0.3%) | |
| dietetics | 1 (0.2%) | |
| optometry | 1 (0.2%) | |
| medical biotechnology | 1 (0.2%) | |
| Previous experiences with interprofessional education initiatives and their forms (students could choose more than one form of initiative) | No | 327 (56.9%) |
| Yes | 248 (43.1%) | |
| -interprofessional classes as part of the study program (including electives) | n = 171 | |
| -interprofessional classes at the University but outside the study program (additional workshops, courses) | n = 53 | |
| -interprofessional classes outside the University—in Poland | n = 42 | |
| -interprofessional classes outside the University—abroad | n = 8 | |
| -training periods or internships of an interprofessional nature | n = 41 | |
| -scientific conferences of an interprofessional nature | n = 35 |
| Overall, I Think That Undertaking Interprofessional Collaboration in My Future Professional Work Is: | n | Mean ± SD | M |
|---|---|---|---|
| original scale: 1 (harmful) to 7 (beneficial) | 388 | 6.51 ± 0.76 | 7 |
| original scale: 1 (pleasant) to 7 (unpleasant) * | |||
| recoded scale: 1 (unpleasant) to 7 (pleasant) | 388 | 5.75 ± 1.21 | 6 |
| original scale: 1 (the wrong thing to do) to 7 (the right thing to do) | 387 | 6.45 ± 0.83 | 7 |
| original scale: 1 (good practice) to 7 (bad practice) * | |||
| recoded scale: 1 (bad practice) to 7 (good practice) | 389 | 6.47 ± 0.88 | 7 |
| Items Regarding Behavioral Beliefs Scale from 1 (Strongly Disagree) to 7 (Strongly Agree) | n | Mean ± SD | M |
|---|---|---|---|
| Undertaking interprofessional collaboration in my future work will positively influence the treatment process and improve the quality of healthcare | 574 | 6.53 ± 0.87 | 7 |
| Undertaking interprofessional collaboration in my future work will allow me to exchange experiences with representatives of other medical professions and gain new knowledge, skills, or competences | 557 | 6.57 ± 0.84 | 7 |
| Undertaking interprofessional collaboration in my future work will give me additional opportunities for further development | 554 | 6.21 ± 1.10 | 7 |
| Undertaking interprofessional collaboration in my future work will improve the comfort of my work | 552 | 6.01 ± 1.21 | 6 |
| Undertaking interprofessional collaboration in my future work will contribute to a better atmosphere in the workplace | 548 | 5.99 ± 1.29 | 7 |
| Undertaking interprofessional collaboration in my future work will contribute to more frequent conflicts and misunderstandings in the team | 547 | 2.70 ± 1.66 | 2 |
| Undertaking interprofessional collaboration in my future work will reduce my workload | 546 | 4.64 ± 1.56 | 5 |
| Undertaking interprofessional collaboration in my future work will reduce the workload of my co-workers | 544 | 4.70 ± 1.52 | 5 |
| Undertaking interprofessional collaboration in my future work will increase the prestige and appreciation of my profession | 543 | 4.94 ± 1.61 | 5 |
| Undertaking interprofessional collaboration in my future work will contribute to reducing my authority and diluting my competences | 544 | 2.19 ± 1.55 | 2 |
| Undertaking interprofessional collaboration in my future work will lead to a situation where other team members will take advantage of me | 542 | 2.85 ± 1.54 | 3 |
| Items Regarding Outcome Evaluations of Behavioral Beliefs Scale from −3 (Extremely Undesirable) to 3 (Extremely Desirable) | n | Mean ± SD | M |
|---|---|---|---|
| Improving the quality of healthcare | 449 | 2.86 ± 0.60 | 3 |
| Exchanging experience with representatives of other medical professions and gaining new knowledge, skills, or competences | 447 | 2.64 ± 0.69 | 3 |
| Occurrence of additional opportunities for further development | 447 | 2.72 ± 0.66 | 3 |
| Improving the comfort of my future work | 446 | 2.76 ± 0.64 | 3 |
| Improving the atmosphere in the workplace | 445 | 2.76 ± 0.67 | 3 |
| More frequent occurrences of conflicts and misunderstandings in the team | 445 | −2.49 ± 1.34 | −3 |
| Reducing my workload | 445 | 2.19 ± 1.14 | 3 |
| Reducing the workload of my future co-workers | 444 | 2.18 ± 1.10 | 3 |
| Increasing the prestige and appreciation of my profession | 443 | 2.09 ± 1.21 | 3 |
| Reducing my authority and diluting my competences | 443 | −2.31 ± 1.33 | −3 |
| Occurrence of situations where other team members will take advantage of me | 443 | −2.54 ± 1.18 | −3 |
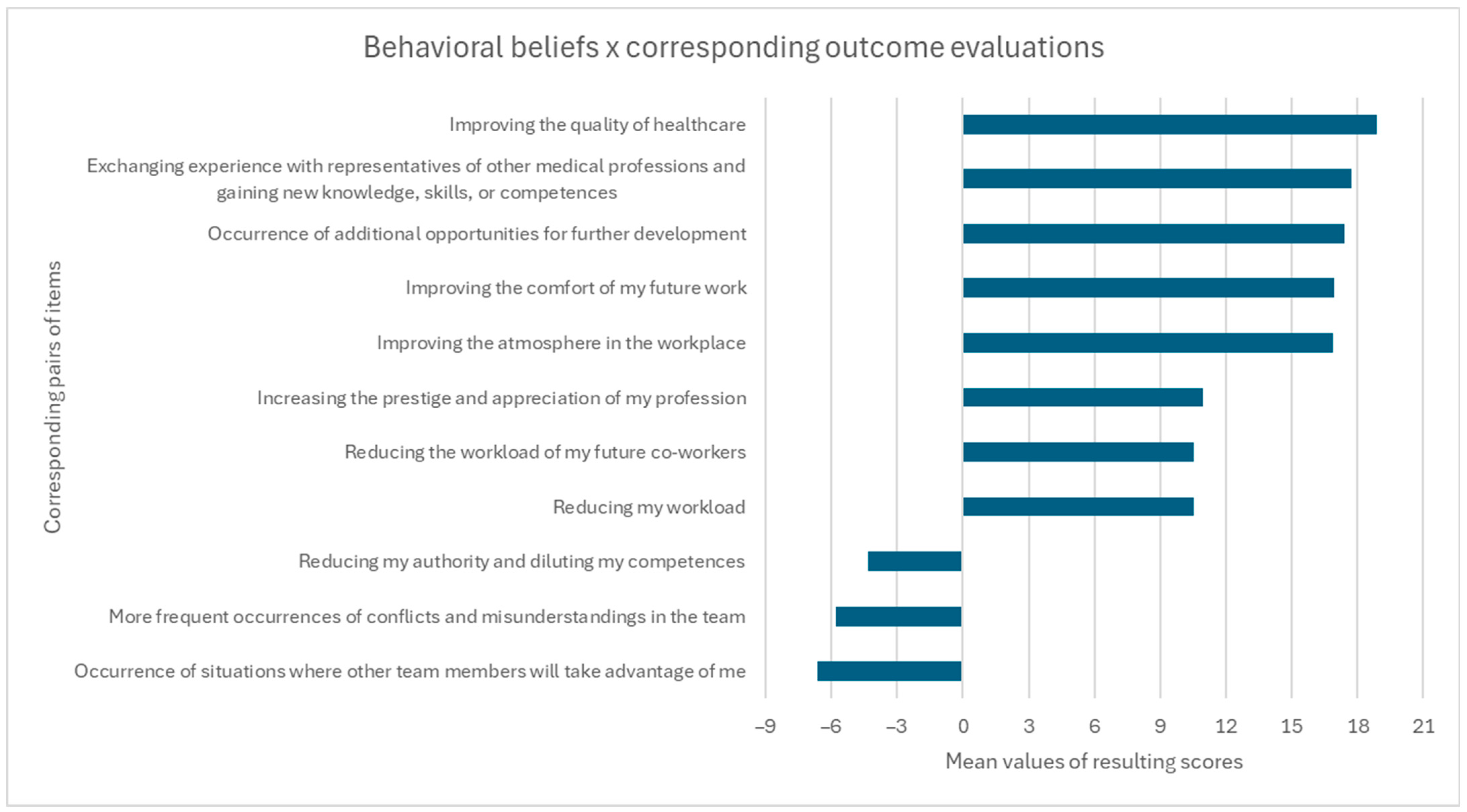
| Behavioral Beliefs × Corresponding Outcome Evaluations | n | Mean ± SD | M | Possible Score Range |
|---|---|---|---|---|
| Improving the quality of healthcare | 442 | 18.90 ± 0.50 | 21 | −21 to 21 |
| Exchanging experience with representatives of other medical professions and gaining new knowledge, skills, or competences | 442 | 17.72 ± 0.51 | 21 | −21 to 21 |
| Occurrence of additional opportunities for further development | 442 | 17.40 ± 0.65 | 21 | −21 to 21 |
| Improving the comfort of my future work | 442 | 16.95 ± 0.72 | 18 | −21 to 21 |
| Improving the atmosphere in the workplace | 442 | 16.90 ± 0.85 | 18 | −21 to 21 |
| More frequent occurrences of conflicts and misunderstandings in the team | 442 | −5.81 ± 2.10 | −6 | −21 to 21 |
| Reducing my workload | 442 | 10.52 ± 1.76 | 12 | −21 to 21 |
| Reducing the workload of my future co-workers | 442 | 10.53 ± 1.63 | 12 | −21 to 21 |
| Increasing the prestige and appreciation of my profession | 442 | 10.95 ± 1.91 | 12 | −21 to 21 |
| Reducing my authority and diluting my competences | 442 | −4.31 ± 1.93 | −3 | −21 to 21 |
| Occurrence of situations where other team members will take advantage of me | 442 | −6.63 ± 1.74 | −6 | −21 to 21 |
| Total attitude score | 442 | 103.13 ± 33.31 | 106.50 | −231 to 231 |
| Items Scale from 1 (Strongly Disagree) to 7 (Strongly Agree) | n | Mean ± SD | M |
|---|---|---|---|
| People who are important to me think that I should NOT undertake interprofessional collaboration * | 378 | 1.71 ± 1.19 | 1 |
| -results after recoding | 378 | 6.29 ± 1.19 | 7 |
| I feel under social pressure to undertake interprofessional collaboration in my future work | 378 | 2.70 ± 1.58 | 2 |
| It is expected of me that I undertake interprofessional collaboration in my future work | 377 | 4.32 ± 1.60 | 4 |
| Items Regarding Normative Beliefs Scale from −3 (Should Not) to 3 (Should) | n | Mean ± SD | M |
|---|---|---|---|
| Other students of my degree course think I … undertake interprofessional collaboration in my future work | 407 | 1.53 ± 1.26 | 2 |
| Representatives of my future profession think I … undertake interprofessional collaboration in my future work | 402 | 1.58 ± 1.32 | 2 |
| Representatives of other medical professions think I … undertake interprofessional collaboration in my future work | 396 | 1.22 ± 1.31 | 1 |
| Patients think I … undertake interprofessional collaboration in my future work | 395 | 1.39 ± 1.34 | 2 |
| Persons managing medical entities think I … undertake interprofessional collaboration in my future work | 395 | 1.18 ± 1.41 | 1 |
| My family thinks I … undertake interprofessional collaboration in my future work | 395 | 1.56 ± 1.28 | 2 |
| My friends and acquaintances think I … undertake interprofessional collaboration in my future work | 394 | 1.65 ± 1.19 | 2 |
| Society thinks I … undertake interprofessional collaboration in my future work | 396 | 1.29 ± 1.37 | 1 |
| Government authorities and politicians think I … undertake interprofessional collaboration in my future work | 395 | 0.31 ± 1.57 | 0 |
| Other Students of My Degree Course | rep. of My Profession | rep. of Other Professions | Patients | Persons Managing Medical Entities | My Family | My Friends and Acquaintances | Society | gov. Authorities and Politicians | |
|---|---|---|---|---|---|---|---|---|---|
| Other students of my degree course | - | ns | <0.001 | ns | <0.001 | ns | ns | 0.004 | <0.001 |
| Representatives of my profession | ns | - | <0.001 | 0.009 | <0.001 | ns | ns | <0.001 | <0.001 |
| Representatives of other professions | <0.001 | <0.001 | - | 0.013 | ns | <0.001 | <0.001 | ns | <0.001 |
| Patients | ns | 0.009 | 0.013 | - | 0.023 | 0.029 | 0.002 | ns | <0.001 |
| Persons managing medical entities | <0.001 | <0.001 | ns | 0.023 | - | <0.001 | <0.001 | ns | <0.001 |
| My family | ns | ns | <0.001 | 0.029 | <0.001 | - | ns | <0.001 | <0.001 |
| My friends and acquaintances | ns | ns | <0.001 | 0.002 | <0.001 | ns | - | <0.001 | <0.001 |
| Society | 0.004 | <0.001 | ns | ns | ns | <0.001 | <0.001 | - | <0.001 |
| Governmental authorities and politicians | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | - |
| Items Regarding Motivation to Comply Scale from 1 (Strongly Disagree) to 7 (Strongly Agree) | n | Mean ± SD | M |
|---|---|---|---|
| Doing what other students in my degree course think I should do is important to me | 386 | 4.13 ± 1.75 | 4 |
| Doing what representatives of my future profession think I should do is important to me | 386 | 5.14 ± 1.51 | 5 |
| Doing what representatives of other medical professions think I should do is important to me | 386 | 4.50 ± 1.57 | 5 |
| Doing what patients think I should do is important to me | 386 | 5.08 ± 1.49 | 5 |
| Doing what persons managing medical entities think I should do is important to me | 386 | 4.53 ± 1.56 | 5 |
| Doing what members of my family think I should do is important to me | 386 | 4.48 ± 1.76 | 5 |
| Doing what my friends and acquaintances think I should do is important to me | 386 | 4.39 ± 1.64 | 5 |
| Doing what society thinks I should do is important to me | 386 | 3.86 ± 1.67 | 4 |
| Doing what the governmental authorities and politicians think I should do is important to me | 386 | 2.83 ± 1.65 | 3 |
| Other Students of My Degree Course | rep. of My Profession | rep. of Other Professions | Patients | Persons Managing Medical Entities | My Family | My Friends and Acquaintances | Society | gov. Authorities and Politicians | |
|---|---|---|---|---|---|---|---|---|---|
| Other students of my degree course | - | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 | <0.001 |
| Representatives of my profession | <0.001 | - | <0.001 | ns | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Representatives of other professions | <0.001 | <0.001 | - | <0.001 | ns | ns | ns | <0.001 | <0.001 |
| Patients | <0.001 | ns | <0.001 | - | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Persons managing medical entities | <0.001 | <0.001 | ns | <0.001 | - | ns | ns | <0.001 | <0.001 |
| My family | <0.001 | <0.001 | ns | <0.001 | ns | - | ns | <0.001 | <0.001 |
| My friends and acquaintances | 0.001 | <0.001 | ns | <0.001 | ns | ns | - | <0.001 | <0.001 |
| Society | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | - | <0.001 |
| Governmental authorities and politicians | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | - |
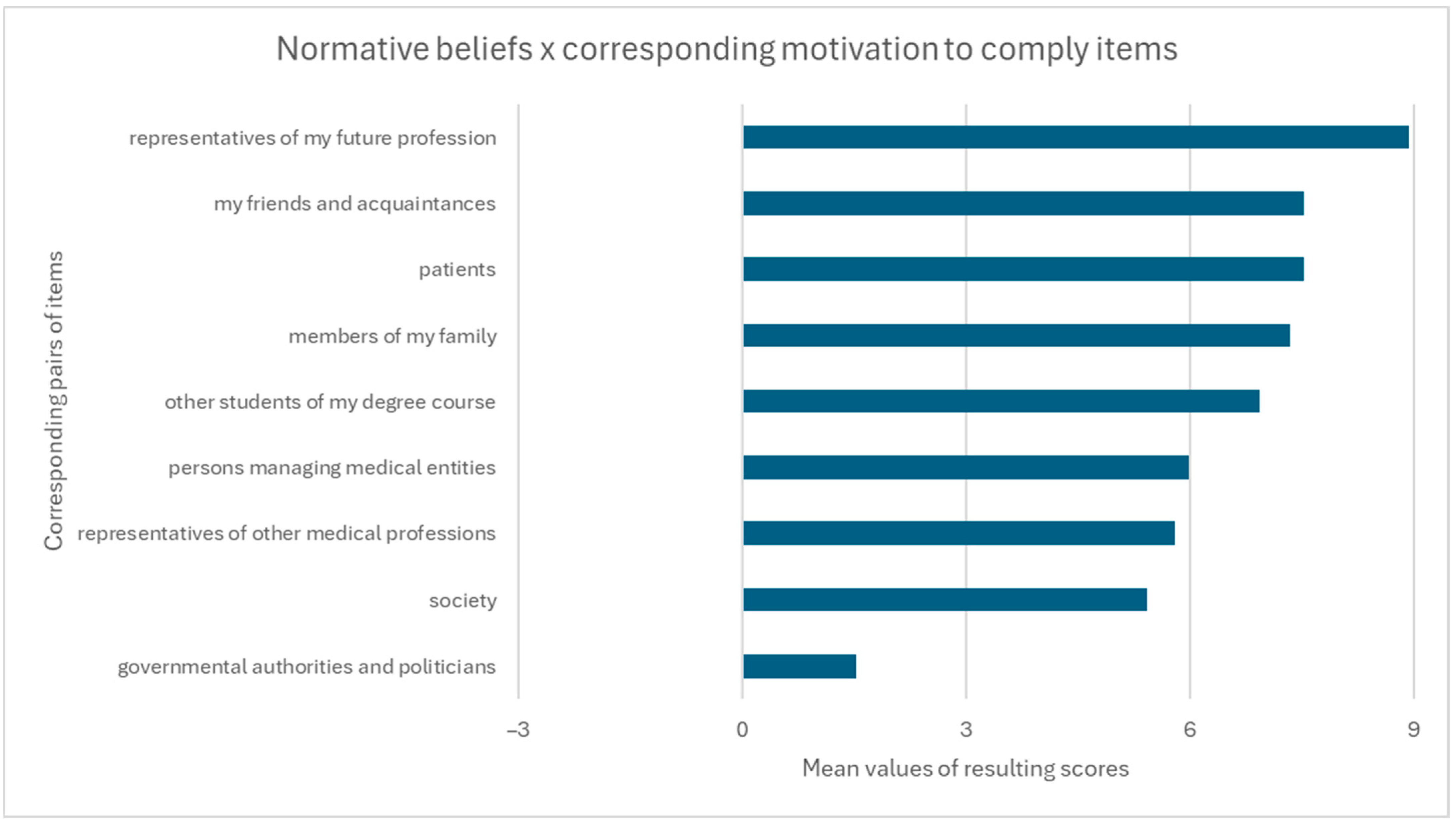
| Normative Beliefs × Corresponding Motivation to Comply Items | n | Mean ± SD | M | Possible Score Range |
|---|---|---|---|---|
| Other students of my degree course | 386 | 6.94 ± 6.78 | 6 | −21 to 21 |
| Representatives of my future profession | 386 | 8.94 ± 7.66 | 10 | −21 to 21 |
| Representatives of other medical professions | 386 | 5.79 ± 6.99 | 5 | −21 to 21 |
| Patients | 386 | 7.52 ± 7.74 | 6 | −21 to 21 |
| Persons managing medical entities | 386 | 5.99 ± 7.23 | 5 | −21 to 21 |
| Members of my family | 386 | 7.35 ± 6.83 | 6 | −21 to 21 |
| My friends and acquaintances | 386 | 7.53 ± 6.49 | 6 | −21 to 21 |
| Society | 386 | 5.42 ± 6.27 | 4 | −21 to 21 |
| Governmental authorities and politicians | 386 | 1.53 ± 5.47 | 0 | −21 to 21 |
| Total subjective norm score | 386 | 57.01 ± 42.98 | 52 | −189 to 189 |
| Item | n | Mean ± SD | M |
|---|---|---|---|
| I am confident that I can undertake interprofessional collaboration in my future work if I want to scale from 1 (strongly disagree) to 7 (strongly agree) | 378 | 5.47 ± 1.33 | 6 |
| Whether I undertake interprofessional collaboration in my future work is entirely up to me scale from 1 (strongly disagree) to 7 (strongly agree) | 378 | 4.01 ± 1.85 | 4 |
| For me to undertake interprofessional collaboration in my future work will be: scale from 1 (easy) to 7 (difficult) * | 378 | 3.50 ± 1.49 | 3 |
| -results after recoding | 378 | 4.50 ± 1.49 | 5 |
| * negatively worded item (recoded for clarity and consistency of presentation) | |||
| Items Regarding Control Beliefs Scale from 1 (Strongly Disagree) to 7 (Strongly Agree) | n | Mean ± SD | M |
|---|---|---|---|
| Mutual stereotypes and prejudices are present between different medical professions | 491 | 6.09 ± 1.01 | 6 |
| I have insufficient knowledge about the tasks and competencies of members of other medical professions | 490 | 4.81 ± 1.53 | 5 |
| I have insufficient knowledge about the possibilities of collaboration and the functioning of interprofessional teams | 486 | 4.96 ± 1.50 | 5 |
| During my studies, I had limited opportunities for contact with students of other degree courses and joint (interprofessional) classes | 484 | 5.52 ± 1.65 | 6 |
| Members of different healthcare professions work in separation from each other (e.g., separate offices, divergent work schedules) | 483 | 5.16 ± 1.50 | 5 |
| The number of medical personnel is insufficient in relation to the needs | 483 | 6.36 ± 1.06 | 7 |
| In everyday work, there is (will be) a lack of time for interprofessional collaboration | 482 | 4.83 ± 1.56 | 5 |
| There is a lack of legal regulations and systemic solutions regarding interprofessional collaboration | 481 | 5.32 ± 1.33 | 5 |
| There is a lack of incentives (gratifications) or factors motivating to undertake interprofessional collaboration | 480 | 5.37 ± 1.34 | 5.5 |
| The existing atmosphere and relationships in the team at the workplace influence the possibility of establishing interprofessional collaboration | 479 | 6.08 ± 1.15 | 6 |
| Members of other healthcare professions may not want to work together with me in my future work | 479 | 4.50 ± 1.65 | 5 |
| Items Regarding Control Belief Power Scale from −3 (Much More Difficult) to 3 (Much Easier) | n | Mean ± SD | M |
|---|---|---|---|
| Feeling that mutual stereotypes and prejudices are present between different medical professions would make undertaking interprofessional collaboration: | 380 | −1.91 ± 1.64 | −3 |
| Feeling that I have insufficient knowledge about the tasks and competencies of other medical professions would make undertaking interprofessional collaboration: | 380 | −1.67 ± 1.59 | −2 |
| Feeling that I have insufficient knowledge about the possibilities of collaboration and the functioning of interprofessional teams would make undertaking interprofessional collaboration: | 380 | −1.67 ± 1.61 | −2 |
| Limited opportunities for contact with students of other degree courses and joint (interprofessional) classes during studies would make undertaking interprofessional collaboration: | 380 | −1.72 ± 1.63 | −2 |
| Situations in which members of different healthcare professions work in separation from each other (e.g., separate offices, divergent work schedules) would make undertaking interprofessional collaboration: | 380 | −1.90 ± 1.36 | −2 |
| An insufficient number of medical personnel would make undertaking interprofessional collaboration: | 380 | −1.78 ± 1.59 | −2 |
| A feeling of a lack of time in everyday work in the future would make undertaking interprofessional collaboration: | 380 | −1.96 ± 1.40 | −2.5 |
| A feeling of lack of legal regulations and systemic solutions regarding interprofessional collaboration would make undertaking interprofessional collaboration: | 379 | −1.59 ± 1.43 | −2 |
| A feeling of a lack of incentives (gratifications) or motivating factors would make undertaking interprofessional collaboration: | 379 | −1.49 ± 1.35 | −2 |
| Good atmosphere and relationships in the team at the workplace would make undertaking interprofessional collaboration: | 379 | 2.40 ± 1.20 | 3 |
| Feeling that members of other healthcare professions may not want to work together with me would make undertaking interprofessional collaboration: | 379 | −2.01 ± 1.59 | −3 |
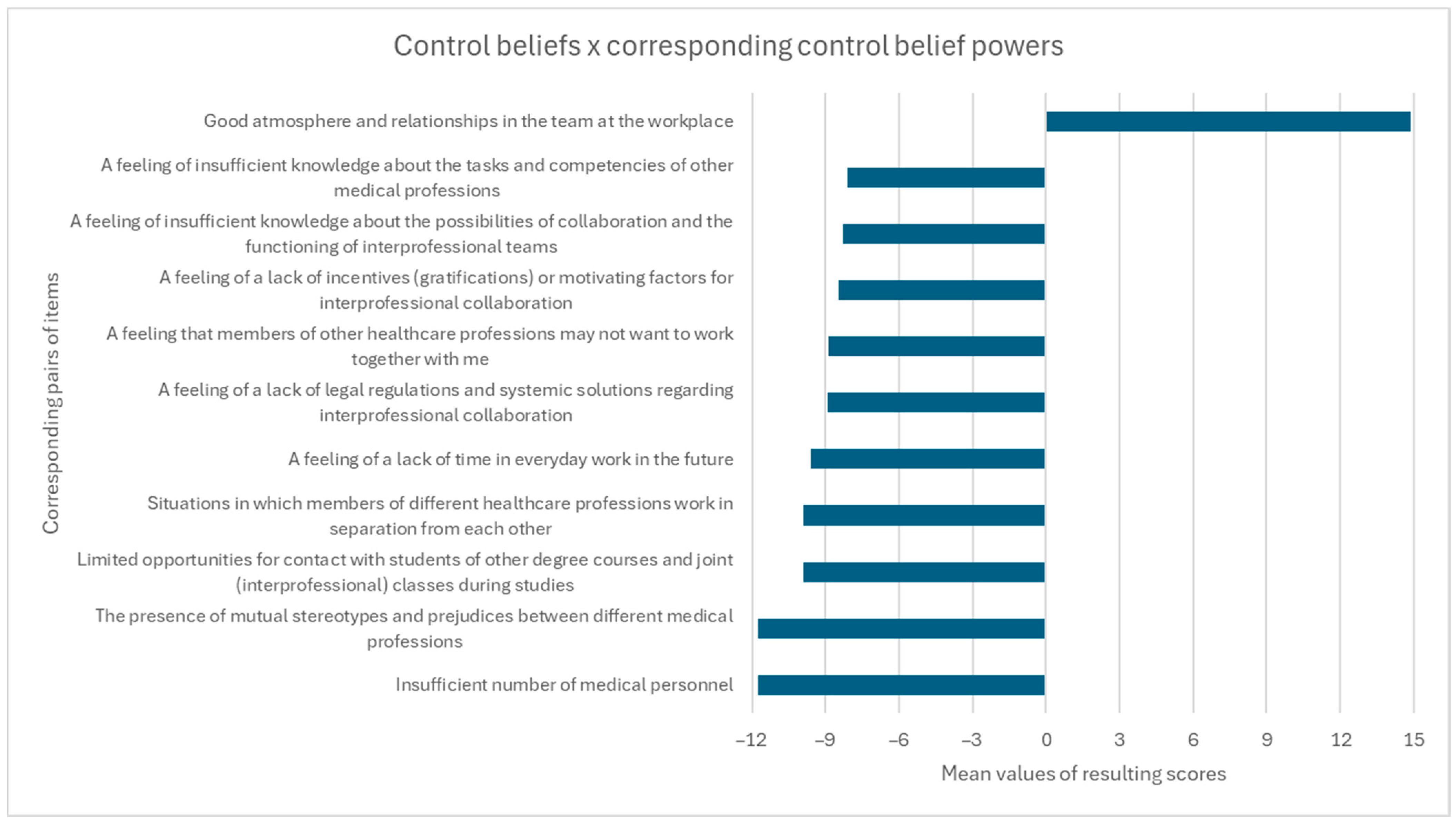
| Control Beliefs × Corresponding Control Belief Powers | n | Mean ± SD | M | Possible Score Range |
|---|---|---|---|---|
| The presence of mutual stereotypes and prejudices between different medical professions | 379 | −11.76 ± 10.57 | −15 | −21 to 21 |
| A feeling of insufficient knowledge about the tasks and competencies of other medical professions | 379 | −8.11 ± 8.64 | −10 | −21 to 21 |
| A feeling of insufficient knowledge about the possibilities of collaboration and the functioning of interprofessional teams | 379 | −8.32 ± 9.05 | −10 | −21 to 21 |
| Limited opportunities for contact with students of other degree courses and joint (interprofessional) classes during studies | 379 | −9.92 ± 10.07 | −12 | −21 to 21 |
| Situations in which members of different healthcare professions work in separation from each other | 379 | −9.90 ± 8.00 | −10 | −21 to 21 |
| Insufficient number of medical personnel | 379 | −11.78 ± 10.53 | −14 | −21 to 21 |
| A feeling of a lack of time in everyday work in the future | 379 | −9.59 ± 8.04 | −10 | −21 to 21 |
| A feeling of a lack of legal regulations and systemic solutions regarding interprofessional collaboration | 379 | −8.94 ± 8.46 | −10 | −21 to 21 |
| A feeling of a lack of incentives (gratifications) or motivating factors for interprofessional collaboration | 379 | −8.47 ± 8.27 | −8 | −21 to 21 |
| Good atmosphere and relationships in the team at the workplace | 379 | 14.89 ± 7.96 | 18 | −21 to 21 |
| A feeling that members of other healthcare professions may not want to work together with me | 379 | −8.89 ± 8.45 | −10 | −21 to 21 |
| Total perceived behavioural control score | 379 | −80.78 ± 59.21 | −87 | −231 to 231 |
| Items Scale from 1 (Strongly Disagree) to 7 (Strongly Agree) | n | Mean ± SD | M |
|---|---|---|---|
| I expect to undertake interprofessional collaboration in my future work | 378 | 5.80 ± 1.33 | 6 |
| I want to undertake interprofessional collaboration in my future work | 377 | 6.17 ± 1.07 | 7 |
| I intend to undertake interprofessional collaboration in my future work | 376 | 6.02 ± 1.06 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Przymuszała, P.; Chmielewski, A.; Zielińska-Tomczak, Ł.; Pieczyński, M.; Czudaj, P.; Cerbin-Koczorowska, M.; Marciniak, R. A Quantitative Cross-Sectional Study on the Behavioral Intentions of Polish Medical and Healthcare Students Regarding Interprofessional Collaboration in Their Future Clinical Practice. Educ. Sci. 2024, 14, 1142. https://doi.org/10.3390/educsci14111142
Przymuszała P, Chmielewski A, Zielińska-Tomczak Ł, Pieczyński M, Czudaj P, Cerbin-Koczorowska M, Marciniak R. A Quantitative Cross-Sectional Study on the Behavioral Intentions of Polish Medical and Healthcare Students Regarding Interprofessional Collaboration in Their Future Clinical Practice. Education Sciences. 2024; 14(11):1142. https://doi.org/10.3390/educsci14111142
Chicago/Turabian StylePrzymuszała, Piotr, Artur Chmielewski, Łucja Zielińska-Tomczak, Mateusz Pieczyński, Paweł Czudaj, Magdalena Cerbin-Koczorowska, and Ryszard Marciniak. 2024. "A Quantitative Cross-Sectional Study on the Behavioral Intentions of Polish Medical and Healthcare Students Regarding Interprofessional Collaboration in Their Future Clinical Practice" Education Sciences 14, no. 11: 1142. https://doi.org/10.3390/educsci14111142
APA StylePrzymuszała, P., Chmielewski, A., Zielińska-Tomczak, Ł., Pieczyński, M., Czudaj, P., Cerbin-Koczorowska, M., & Marciniak, R. (2024). A Quantitative Cross-Sectional Study on the Behavioral Intentions of Polish Medical and Healthcare Students Regarding Interprofessional Collaboration in Their Future Clinical Practice. Education Sciences, 14(11), 1142. https://doi.org/10.3390/educsci14111142