Abstract
safeMedicate was developed as an English-language web-based system designed to support learning and competence development in solving medication dosage problems. Our purpose was to identify the adaptations necessary to implement safeMedicate for use in Brazil, with an explorative, qualitative design using an adapted Participatory and Iterative Process Framework for Language Adaptation (PIPFLA) process and the Delphi technique with online focus groups. Focus group transcripts were analyzed using content analysis. The main themes were language, visual content, programing, data, and strength. safeMedicate was considered to be acceptable for use in Brazil. Participants perceived that it would be welcomed by faculty and students as a way to address current teaching and practice gaps. Cultural and political barriers should be identified and addressed when adapting material for use in different national contexts.
1. Introduction
This qualitative study explores the adaptation of safeMedicate (a virtual learning environment for medication dosage calculation problem solving (MDC-PS)) for use in Brazil based on the Delphi technique with nursing professors, practicing nurses, and nursing students by identifying the changes necessary to adapt the educational software.
Medication administration is an important, essential nursing function, with the potential for dangerous consequences if errors occur. Competency-based education for personnel charged with medication administration may minimize this threat. Most errors in Brazil relate to prescribing, preparing, and administering medications. These include incorrect doses/overdose (13.2%), the incorrect administration route (11.4%), inadequate drug storage (11.4%), and the incorrect dosage form (e.g., tablets, capsules, ampoules, intravenous infusion crystalloid solutions) (8.8%) [1]. An overdose is the excessive administration of a drug due to incorrect prescription use or incorrect dose preparation or a combination of the two. The error frequency increases close to shift change times, specifically 07.00–08.00 and 19.00–20.00 [2].
These errors illustrate the need to systematically address MDC-PS and drug administration errors. This study addresses this problem through the cross-cultural adaptation of safeMedicate, an evidence-based virtual learning environment. It was developed via sequential translational research and is used worldwide [3]. Translational research links basic research and its clinical application by addressing gaps in knowledge/technology transfer and health professional evaluation [4] using real-world data [5].
UK and USA nursing students using safeMedicate achieved significant improvements in constructing conceptual and calculation competence in MDC-PS [6,7,8,9,10,11]. The authentic learning environment supports a spectrum of mathematics learning styles by tailoring and expanding mathematical skills through mental computation, arithmetic, geometry/visual, and algebra [8,12]. The need for an evidence-driven cross-cultural Brazilian safeMedicate adaptation is clear.
Cross-cultural adaptation is more than word-for-word direct translation. A decentering technique is used to interpret meaning [13]. Translation moves beyond grammatical rules and writing conventions to an interpretation informed by socio-cultural and contextual factors [14,15]. We used a combined emic (within-culture) and etic (across-culture) cross-cultural adaptation process [16,17,18,19].
safeMedicate is a teaching/learning software with multiple modules and materials. An iterative, multiple step process such as the Participatory and Iterative Process Framework for Language Adaptation (PIPFLA) process is more suitable for adapting educational training as it considers the needs of time, resource constraints, and additional harmonization steps [13,18,20].
Nursing professors, practicing nurses, and nursing students were asked via the Delphi technique to evaluate whether safeMedicate meets Brazilian professional practice, regulation, and political requirements. The Delphi technique is an iterative process using structured group communication to establish a participant consensus [21,22]. We used RealTime Delphi to present participants’ judgements as real-time online feedback [23] to adapt safeMedicate by addressing the following research question: “Which are the adaptations necessary in safeMedicate for use in Brazil?”
2. Methods
2.1. Design
An explorative, qualitative design was used with an adapted Participatory and Iterative Process Framework for Language Adaptation (PIPFLA) approach. The PIPFLA process is a cross-cultural equivalence model that combines the emic (perspective from inside the system/culture) and etic (viewpoint from outside the system) perspectives. A cross-cultural emic–etic paradigm considers the multiple linguistic and socio-cultural factors. Additionally, PIPFLA considers the different needs in translating an intervention versus a measurement tool [13,18]. The process was adapted to translation sciences recommendations of, instead of back-translation, focusing on the best translation by looking at the two source language texts and evaluating the translation in the target language [24].
Video conferences sought to clarify the teaching video purpose, i.e., to teach students how to access the safeMedicate virtual learning environment and see assessments. This should be done before users finish the evaluation. Semantic and cultural modifications are common in cross-cultural studies, commonly performing psychometric analysis [13,25]. Psychometric analysis is not necessary here because this is not an assessment-scale adaptation but a content analysis exploring the pedagogical changes necessary for safeMedicate usage in Brazil.
Data collection was performed via online Zoom focus groups due to the international nature of the project (United Kingdom, United States, and Brazil). This is an affordable, easy-to-use, video-, voice-, and screen-sharing platform with mobile app access. Participants chose a time most convenient to them considering worldwide time zone differences. This method has been widely adopted after the COVID-19 pandemic outbreak [26,27].
The semi-structured narrative interview guide was adjusted via an iterative process based on new insights from ongoing data analysis throughout data collection. The interview guidelines also varied according to focus group characteristics (language adaptation team, participant panel). Protocols focused on identifying changes necessary for safeMedicate use in Brazil, and participants’ general perceptions of the virtual learning environment (see Table 1 and Table 2).

Table 1.
Interview guide for language adaptation team.
Table 2.
Interview guide for panel of experts and student/nurse panel.
2.2. Participants and Recruitment
Inclusion criteria to participate included the following:
- Bilingual committee: Bilingual professionals with healthcare experience (nurses) and a professional translator.
- Panel of Experts: University nurse professors working for at least 4 years preferably in MDC-PS, and/or clinical practice supervisors and/or clinical nurses.
- Student/Nurse Panel: Students already undertaking MDC-PS classes or nurses working in clinical practice.
Participants were recruited by convenience sampling via university dean networks, principal researchers’ professional networks, snowball sampling, and social media. A Google form was available for potential participants to answer questions and link their Lattes platform curriculum (Brazilian government information system, www.lattes.cnpq.br, accessed on 22 December 2017). There was an initial sample of 22 nurses and professors for the panel of experts and 45 students/nurses for the student panel. The potential panel of experts’ form responses and curriculum were evaluated against the study inclusion criteria. Fifteen nurses and professors were invited by e-mail. Upon confirmation, an e-mail to identify availability for video conference dates was sent. English fluency was not required for this group. Student panel participants were drawn from a list provided by the panel of experts. Each expert indicated three students and one nurse; 18 students and 6 nurses were invited to the student panel. The first three students and first nurse who committed to participate had access to the safeMedicate Brazilian version. After last-minute cancelations, two members participated (one student and one recently graduated nurse). English fluency was not required.
Six bilingual participants were invited to form the bilingual committee: four professional translators and two nursing professors. One English–Portuguese professional translator and two bilingual nurse professors committed to participate in the safeMedicate adaptation process. A bilingual committee approach was used to develop the best possible translation. This allowed for mistakes from one committee member to be recognized and corrected by other members [13,28]. Participants knew that the primary investigator was a doctoral candidate developing an international partnership for the virtual learning environment adaptation. Some expert committee members had heard about each other or had worked together. Only participants and researchers were present at the focus groups, which were recorded using Zoom.
2.3. Data Collection
Participants were allocated according to focus group purposes. The bilingual committee’s objective was to produce the best possible translation (English–Portuguese) by merging professional translator and nurse translation documents, and prioritizing an adaptation to Portuguese (target language) considering Brazilian socio-cultural factors. The panel of experts’ objective was to evaluate the translation produced in Portuguese (target language) via critique and suggestions, using governmental and professional guidelines, articles, and standardized medical language. The panel of students/nurses provided a general evaluation of safeMedicate and supplied user feedback and suggestions.
Ideally, focus groups should have 6–10 members, but can range from 4 to 12 [29]. Groups were scheduled with a higher number of invitees but final numbers were smaller than intended. A possible negative focus group outcome is groupthink, when stronger members control or influence other members’ verbalization. It can be overcome by focusing on the potential for learning about the focus and the group [30].
All focus groups showed productive results. Members interacted comfortably to build a consensus through iteration and controlled Delphi feedback [21,22]. The bilingual committee (N = 3) and panel of experts focus group (N = 4) met twice to reach a consensus; the student/professional panel (N = 2) met once. The mean duration of meetings was 68 min. Field notes were made during and after the focus groups. Transcripts were returned to participants for comments and changes. The panel of experts had 16 years of Brazilian nursing work experience, 9.6 years as clinical supervisors of nursing students, and 11 years as nursing professors. Focus groups were conducted between December 2017 and May 2018. Participants received links to the Zoom video conference, safeMedicate material for analysis, and participation instructions. The principal investigator acted as a moderator to ensure participant engagement and asked questions to clarify and validate participants’ comments; this often stimulated feedback or further explanation. Paraphrasing was used to ensure that the data reflected participants’ perspectives as accurately as possible. The investigator was a doctoral candidate at the time, trained in qualitative research and interviewing, and had previously taught Brazilian nursing students for five years.
Saturation was reached at the professors’ second video conference. Their suggestions were either accepted by the software developers or explanations of safeMedicate functions were requested prior to changes. For example, participants suggested a numerical value to indicate student performance to guide both student and professor. The software produces a final report percentage so that students and professors may see how many calculations were made and the calculation error frequency. Participants agreed that this fulfilled the “percentage, numeric” need on the assessment data report.
2.4. Data Analysis
A directed content analysis approach was used on the group video conference call transcripts. Theory or relevant findings guided initial code production in a directed approach [31]. The analysis strategy followed the CDC codebook development method. Coding was done at dispersed locations by two or more individuals [32]. This provided a stable framework for contextual data analysis. Team-based code development supports improved intercoder agreement in adapting and implementing the virtual learning environment.
The primary investigator developed the codebook and, with a secondary coder, independently coded the transcripts. Both identified and sorted statements answering the research question, “Which are the adaptations necessary in safeMedicate for use in Brazil?” Where there was disagreement about a statement’s placement, the primary and secondary investigators recoded the relevant text referencing Brazilian regulatory documents on medication training information.
The codes were derived from a priori and emergent themes. A priori is what researchers expect from the research questions. Emergent themes are codes emerging after data collection, leading to codebook review according to emergent themes and consistency in line with the CDC coding flow diagram [32]. Participant names were protected via assigned pseudonyms during Zoom conference calls (see Table 3 for final themes and subthemes).
Table 3.
Adaptation process codebook.
2.5. Ethical Considerations
The University of South Florida Institutional Review Board (USF IRB) identified the study as a program evaluation method, quality improvement, and/or needs analysis. It was conducted in compliance with the USF IRB Not Human Subjects Research Policy.
3. Results
The main themes were language, visual content, programing, data, and strength (see Figure 1).
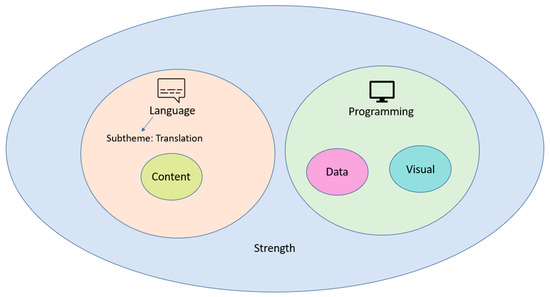
Figure 1.
Themes diagram for the cross-cultural adaptation of safeMedicate.
Participants made efforts throughout the video conferences to actively collaborate with other participants. Participants clearly perceived it as a collaborative process for all voices to be heard. The researcher asked explicitly about areas for improvement during participant debriefing on using video conferences for focus groups. There was a very positive validation from participants about the process and software used:
No. I thought it was pretty good. It was the first time I used this [Zoom] software and it gives to interact well, see several things at the same time, the chat, the person… I have not used before and I thought it is fantastic. No specific detail… You were extremely thoughtful, when I entered you were already online in the room…. I opened the doors with you. It was very quiet [smooth]. I have nothing to suggest (Betony).
3.1. Language
The translation language varied between a succinct format and more detailed format using more words and technical healthcare words. Using a diverse bilingual committee to choose appropriate wording produced the best translated Portuguese version. Portuguese is a dynamic language and the professional translator ensured that translation differences did not interfere with content comprehension.
The translator is more succinct and more direct. [but the nurse] had some technical words and a tendency to explain more detailed (Tulip).
It has to be translated by the word that conveys the necessary understanding, so it’s correct. Does not change in anything the meaning of the phrase, it just gets elegant […] It got more concise, but it didn’t change. I grant to you [both], because you have the knowledge of the practical language (Violet).
The safeMedicate video material was in Portuguese, but showed how to access the assessment in the website via icons in English. Video conference participants mentioned website and icon language adaptation as crucial for safeMedicate usage in Brazil.
[Check with the software developers on the] possibility of translating this material into Portuguese altogether, [translating the website]. I think it’s suitable the way it is [with the content translated and adapted]. With the exception of that issue of the translation of the [website and icons from English to] Portuguese (Sunflower).
Until these [English] icons are translated. I see a bit difficult at first by having many sectors in English (Lily).
3.2. Language Subtheme: Translation
Video conference discussions explored various specific terms for translation, and focused on wording fitting the reality of Brazilian teaching and practice. The principal investigator clarified the original material’s meaning, differences, and content. Feedback included the following:
Change those names “domain” into “ability” (Betony).
I’m confused about “injectable” and “IV infusions” (Sunflower).
Concerns were raised about including medical terms used in everyday healthcare practice. The translated material was not perceived as an incorrect translation, but it was noted that the language should be tailored for public comprehension and the practice context.
She [professional translator] uses the term “medication request” I would follow more the translation by the nurse who says “ medical prescription”. […] I agree more with “measuring device”. I like it better. Not that it’s wrong, but “instrument” is general. […] Yes, “no rounding required”. I liked the way the nurse put it, because she used the language she uses in her everyday life [in the healthcare environment]. […] I would suggest putting “routine medicine”. To be clear the translation is not wrong, it is only the use of language (Tulip).
They also expanded the language comprehension to technical nursing students, and used language that would follow technology development.
Here there is the technical level of nursing that also works with medications. So the clearest and simplest so everyone can understand. […] [I suggest using a language like] “take the cursor” […] [because] I guess “pass the mouse” will be obsolete [since people are already stopping to use the “computer mouse”] (Tulip).
3.3. Visual
Participants provided a general visual perspective on safeMedicate videos regarding content visualization. They wanted better video quality or more information on the content shown.
Even placing in full screen, it was hard to read (Coneflower).
Replacing the color with symbols or numeric categories (Sunflower).
Oh… how cute… very interesting [When seeing the syringe plunger move] (Violet).
We do not see the question to know how really is. […] What is the style of the question. […] He did not bother to show us the question, but rather the operation as a whole (Jasmine).
They recommended including a results overview on the same screen so that students could see which part was incorrect (calculation, device choice, or device measurement).
For him to know the point he missed, not need to open…at the first view, he would know where the error is (Marguerite).
3.4. Content
Further pharmacology information in safeMedicate was requested to align with Brazilian professional practice guidelines and respond to Brazilian professional development needs.
Both in undergraduate and specialization, we perceive a fragility in pharmacology training. […] Add an informative balloon of pharmacology. (Coneflower)
Having a balloon that the student clicked, stating the indication. […] The indication of the medication as an extra option. […] is he [the student] wants he watches, if he already dominates the content: he goes into the calculation (Marguerite).
Adding extra materials for consultation in the virtual learning environment was beneficial for safeMedicate users. It reminded them of the Brazilian guidelines, public perceptions of how safeMedicate aligns, and class-taught materials, e.g., the nine rights of medication administration.
I thought on when start the software have an introductory video listing protocol, only as a reminder to the student (Coneflower).
Is there any part of the software that could have these protocols? […] it’s not a fundamental thing, but it would be a plus […] because if he [the student] has a doubt, he goes there [click in the material] and studies (Marguerite).
We use the international protocols anyway […] including the right nine [in safeMedicate system], would be closer to the reality of our students here in Brazil (Sunflower).
Not clear to us [whether the software follows] the Brazilian guidelines (Jasmine).
3.5. Programming
Participants suggested how safeMedicate could be adapted to appeal to future users.
We need to think about leaving the product attractive to the student so that he walks in the process and this does not get tiresome, boring. […] increasing the numbers of problems and the degree of difficulty (Coneflower).
Intelligent test. That will increase the difficulty and stay on top of the mistakes to test you [test the user of the software] (Marguerite).
Video conferences highlighted the need for safeMedicate to use resources flexibly and align with diverse technological contexts in Brazilian universities and healthcare facilities.
Hospital units [are] more accessible in terms of resources available because there are already computers [in the site]. Diversification to be acceptable depending on the university situation for teaching. (different technology platforms favors access) (Tulip).
Concern about peoples’ ability to use the technology was raised, as well as making the virtual learning environment available as a mobile app.
But not everyone has facility in technology [deal with technology easily]. By cell phone would be something…easier to access. A more portable way. […] computer is much more complex and involves a lot more system stuff than software as an app. Having the software on the cell phone would help these people who don’t have this technological handling because it’s an easier tool to use. We live in a totally technological era. And tends to increase. So even people who are not adept at technology end up having to undergo technology [use] even for their own survival, either for academic or work reasons. People with smartphone use that technology every day to call a child or husband (Jasmine).
I have some doubts about the software not accompanying the smartphone (Lily).
The principal investigator explained that the virtual learning environment could be accessed via a cell phone web browser. This raised speed and data usage concerns.
There is no way to pick up a software and reduce it in a short time, but it would be a very valid option. […] We know that it can be accessed through the internet by the smartphone, but we also know that the internet of the smartphone is not as effective as an app regarding data usage […] … is completely different. Even because if it is something very heavy you take a lot of time to download and etc. So this question has to be well studied, because it runs the risk [of software coming] and not be so accessed or well accepted by the difficulty that would have in accessing it. Even because not everyone has a computer under the arm, not everyone has a data package [on the smartphone] with a reasonably accessible speed to sites that size. Among other things (Jasmine).
This concern is valid for target population access and the use of safeMedicate considering Brazilian data usage and charges. Reducing tabs or having an intuitive menu with images would avoid the “pass the mouse, open the menu” function, and increase user satisfaction.
There are so many tabs in the menu…if it didn’t have so many subfolders. I believe that even being in Portuguese still would have some difficulty. Implementation of images to the menu get more didactic and easy. Be something more objective so that you can access what is your goal faster [reach the tab you intend to access faster]. […] this software is coming to be a facilitator, so this needs to be quick and easy to reach the goal more effectively. sometimes we can have ten links, but if they are focused it turns out well without difficulty (Jasmine).
In some applications [programs] this part of you just passing the mouse over gives some bugs [problems] […] being unnecessary stress (Lily).
3.6. Data
The theme came from suggestions about the software display of performance statistics to align user comprehension and expectations and allow easy follow-up on students’ main needs.
In the Brazilian reality, the Brazilian students are stuck to the grade (Coneflower).
I wouldn’t put as color, I would put as a numerical scale from zero to ten. […] either in percentage or numerical scale. as much feedback to the student and to us [the teacher]. We have to know “this student is having difficulty at this point” (Marguerite).
3.7. Strength
safeMedicate’s strengths and positive perspectives were a frequent emerging theme incorporated into the codebook after coder review. The video format used to present content was considered beneficial to users’ comprehension, aligned with the authentic virtual environment for syringe choice and usage.
Found the entire tool [safeMedicate] easy to access (Coneflower).
Good visualization of [syringe] graduation number. I think [the video] is very clear, very explanatory, the voice of narration is good, the diction is good. […] The same observation of the other video because one complements the other (Marguerite).
Technology being used much more often in the classrooms. This tool [safeMedicate] can be even an ally of the teacher within the classroom. […] It seems you are handling the syringe (Betony).
I really liked the appearance, the syringe, the plunger, the ease of you seeing the syringe units, choosing the ideal syringe, the medication, the dosage and all (Sunflower).
I really liked [safeMedicate] I think it will be very useful (Tulip).
[safeMedicate] was very well thought out and planned aiming at the study of [drug calculation] skills (Jasmine).
But the [opportunity to] practice generates the possibility of performing with a greater ease to improve customer service and avoid mistakes. Used within the institutions as a new discipline […] along with semiology and semitechnical (Lyli).
The availability of the problem and tools in one screen was also mentioned.
Can see everything that will be necessary for the realization of the calculation (Betony).
Product suitability for Brazil was frequently mentioned, particularly regarding learning opportunities beyond classrooms, allowing for calculation skills repetition. Opportunity for repetition was a positive safeMedicate characteristic in all video conferences. Using technology to teach MDC-PS skills was seen as a way to address current teaching method gaps, particularly as the implementation of nurse prescribing is being considered in Brazil.
Suitable for use in Brazil, it is a tool that facilitates learning not only in the classroom as other spaces (Betony).
We are seeing that [our classroom, traditional teaching methods] are not responding to the problems of our students, they feel the need to build their own knowledge and I think the arrival of these applications [software] only tends to enrich our methodology (Sunflower).
I think showing the necessity here […] the gap exists. Especially that nursing that is planned to install in Brazil requires the pharmaceutical prescription. So knowledge in the area of pharmacology and medication calculation only comes to add (Tulip).
We only pay [register in discipline] that has this calculation in one or two disciplines of the university […] then it becomes vacant, because whether you want or not everything that involves mathematics is practical…you have to be there practicing daily (Jasmine).
safeMedicate would also stimulate users’ independence for knowledge development. Introducing the virtual aid tool concept to teachers and students was considered important.
Also to make our students become more independent is the search for their own knowledge and we really work and participate as facilitator of this process (Sunflower).
I already see a very strong viability, but it’s because I’m already getting to know how to use it. […] there’s a certain lack of notion what a virtual aid is (Tulip).
Finally, safeMedicate’s potential importance to different healthcare professionals was acknowledged.
Very good teaching and practice tool for those who are working in that area. Be it doctors, residents, nurses, nursing assistants… people who need to practice something and have no opportunity to do it firsthand (Violet).
4. Discussion
This participatory and iterative process focused on identifying the adaptations necessary in the software that provides a virtual learning environment for medication calculation and problem solving (safeMedicate) for use in Brazil. The participants identified changes related to language, visual content, programming, and strength. These findings will guide the adaptations of the remaining modules, material, website, and icons related to other care environments. Examples would be pediatric dosage calculations, oncology dose calculation and proportion, and other content requiring titration.
These results also suggest areas that other virtual learning programs should consider for improvement. This is because solemn translations are insufficient to address the user’s needs, improve their understanding, and make the program relevant to their professional practice [18,20]. The suggestion of adapting the grading system in safeMedicate to Brazil, for example, was a cultural recommendation. This improves users’ understanding of the software feedback on assessment data reports, as the majority of students and teachers are used to a numerical 0–10 or 0–100 system.
These findings also show that, in addition to linguistic and cultural translation, the specialized viewpoint provides an invaluable technical perspective. While one translation document was developed by a nurse following established nomenclature guidelines from the government and professional associations, the second translation version was created by a professional translator (who was not a healthcare professional). Both versions were assessed side-by-side with the source language texts by the bilingual committee. The bilingual committee agreed that the standardized nomenclature used by the nurse was preferred over the language-equivalent translation. However, the semantics used by the professional translator made the text easier to read. Merging both created the best translation from the source document: a text with semantics for easy understanding and appropriate technical nomenclature. This adapted PIPFLA process supports the translation sciences’ suggestion to focus on a target language translation rather than back-translation [24], as well as previous evidence that an expert committee helps to ensure accurate content [33].
safeMedicate can be used by multiple professions, such as pharmacologists and dentists. The committee of experts also saw in the software an opportunity to address gaps in nursing education to improve drug calculation skills. This is because advanced practice nursing programs are undergoing expansion in Brazil [34,35].
A challenge that safeMedicate could face is being formally recognized by professional associations. In order to overcome this barrier, the expert committee recommended using safeMedicate in conjunction with classroom education (not in place of classroom time). Their concern about emphasizing this message aligns with the trend in Brazil of questioning distance education for the nursing profession. To clarify, although distance education is an emerging trend globally, especially after the pandemic, the Federal Board of Nursing of Brazil unanimously rejects distance nursing education. In an official letter published in April 2022, the Federal Board of Nursing clarified that emergency remote teaching is provisional, limited to the period of the health crisis, which is different from distance education, because it transfers face-to-face activities to a virtual environment for a specific time, prioritizing the dialogical relationship between teacher and student [36].
Therefore, the term “Emergency Remote Teaching” (Ensino Remoto Emergencial, ERE) was crafted to differentiate from “Distance Education” (Ensino a Distância, EaD) due to differences in legislation, planning, investments, and the training of teachers in digital technologies [37]. During Emergency Response Teaching, students stated that they missed the in-person exchange of experiences. However, they were split between returning to in-person classes and engaging in a hybrid format [38], which shows a preference for virtual usage.
safeMedicate favors accessibility and repetition, aligning with the usage of web-based software to facilitate teaching and research [39], similar to other educational [40] and therapeutic [41] experiences developed during the pandemic in Brazil. However, the pandemic also reinforced the importance of virtual accessibility to ensure access to education, as there is still a digital gap in Brazil’s urban and rural areas [42,43]. Therefore, safeMedicate and other online software programs need to consider data usage as a limiting user factor, which can be overcome by developing an app with offline access to exercises (as suggested by the student/nurse panel).
5. Conclusions
Beyond reporting safeMedicate as acceptable in Brazil, members welcomed it as a way to address current teaching and practice gaps for professional nursing development. It is important to consider that cultural and political barriers will exist when adapting material between different nations. It is therefore crucial to not only observe the standardized language and protocols established by the government and professional associations of the country, but also consider how they regulate healthcare and education so that software (e.g., safeMedicate) is adapted/used accordingly.
Study Strengths and Limitations
Technical difficulties arose during the video conference, with one participant unable to turn on the microphone due to computer technical problems. However, by sending voice messages to the principal investigator to communicate with the group, he ensured his participation. Providing access to video prior to translating written documents is important for proper word choices applicable to the software. Hence, the importance of alignment with software developers is highlighted.
Author Contributions
Conceptualization, S.V.O.D., K.W. and J.M.C.; methodology, S.V.O.D., V.C., K.W. and J.M.C.; software, K.W., D.P. and J.M.C.; validation, S.V.O.D., V.C. and J.M.C.; formal analysis, S.V.O.D., V.C. and J.M.C.; investigation, S.V.O.D. and J.M.C.; resources, S.V.O.D., V.C., K.W., D.P. and J.M.C.; data curation, S.V.O.D.; writing—original draft preparation, S.V.O.D., K.W. and J.M.C.; writing—review and editing, S.V.O.D., V.C., K.W., D.P. and J.M.C.; visualization, S.V.O.D., V.C., K.W. and J.M.C.; supervision, K.W. and J.M.C.; project administration, S.V.O.D., K.W. and J.M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the study being identified as a program evaluation method, quality improvement, and/or needs analysis by the University of South Florida Institutional Review Board.
Informed Consent Statement
Informed consent was waived due to the study being identified as a program evaluation method, quality improvement, and/or needs analysis.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to individual privacy. The study protocol of the current research can be found at: https://www.mdpi.com/2227-7102/13/3/237 (accessed on 27 February 2023).
Conflicts of Interest
The authors declare no conflict of interest.
References
- dos Santos, L.; Winkler, N.; dos Santos, M.A.; Martinbiancho, J.K. Description of medication errors detected at a drug information centre in Southern Brazil. Pharm. Pract. 2015, 13, 524. [Google Scholar] [CrossRef]
- Isaacs, A.N.; Ch’Ng, K.; Delhiwale, N.; Taylor, K.; Kent, B.; Raymond, A. Hospital medication errors: A cross-sectional study. Int. J. Qual. Health Care 2020, 33, mzaa136. [Google Scholar] [CrossRef]
- Authentic World. Institution Administrator: User Guide; SafeMedicate: Cardiff, UK, 2009. [Google Scholar]
- Young, S.; Weeks, K.W.; Hutton, B.M. Safety in numbers 1: Essential numerical and scientific principles underpinning medication dose calculation. Nurse Educ. Pract. 2013, 13, e11–e22. [Google Scholar] [CrossRef]
- Marchiano, R.D.M.; Di Sante, G.; Piro, G.; Carbone, C.; Tortora, G.; Boldrini, L.; Pietragalla, A.; Daniele, G.; Tredicine, M.; Cesario, A.; et al. Translational Research in the Era of Precision Medicine: Where We Are and Where We Will Go. J. Pers. Med. 2021, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, K.; Weeks, K.W.; Moseley, L. Safety in numbers 6: Tracking pre-registration nursing students’ cognitive and functional competence development in medication dosage calculation problem-solving: The role of authentic learning and diagnostic assessment environments. Nurse Educ. Pract. 2013, 13, e66–e77. [Google Scholar] [CrossRef] [PubMed]
- Sabin, M.; Weeks, K.W.; Rowe, D.A.; Hutton, B.M.; Coben, D.; Hall, C.; Woolley, N. Safety in numbers 5: Evaluation of computer-based authentic assessment and high fidelity simulated OSCE environments as a framework for articulating a point of registration medication dosage calculation benchmark. Nurse Educ. Pract. 2013, 13, e55–e65. [Google Scholar] [CrossRef] [PubMed]
- Weeks, K.W.; Clochesy, J.M.; Hutton, B.M.; Moseley, L. Safety in numbers 4: The relationship between exposure to authentic and didactic environments and Nursing Students’ learning of medication dosage calculation problem solving knowledge and skills. Nurse Educ. Pract. 2013, 13, e43–e54. [Google Scholar] [CrossRef] [PubMed]
- Weeks, K.W.; Hutton, B.M.; Coben, D.; Clochesy, J.M.; Pontin, D. Safety in numbers 3: Authenticity, Building knowledge & skills and Competency development & assessment: The ABC of safe medication dosage calculation problem-solving pedagogy. Nurse Educ. Pract. 2013, 13, e33–e42. [Google Scholar] [CrossRef]
- Weeks, K.W.; Higginson, R.; Clochesy, J.M.; Coben, D. Safety in Numbers 7: Veni, vidi, duci: A grounded theory evaluation of nursing students’ medication dosage calculation problem-solving schemata construction. Nurse Educ. Pract. 2013, 13, e78–e87. [Google Scholar] [CrossRef]
- Weeks, K.W.; Hutton, B.M.; Young, S.; Coben, D.; Clochesy, J.M.; Pontin, D. Safety in numbers 2: Competency modelling and diagnostic error assessment in medication dosage calculation problem-solving. Nurse Educ. Pract. 2013, 13, e23–e32. [Google Scholar] [CrossRef]
- Weeks, K.W.; Coben, D.; O’Neill, D.; Jones, A.; Weeks, A.; Brown, M.; Pontin, D. Developing and integrating nursing competence through authentic technology-enhanced clinical simulation education: Pedagogies for reconceptualising the theory-practice gap. Nurse Educ. Pract. 2019, 37, 29–38. [Google Scholar] [CrossRef]
- Brislin, R.W.; Lonner, W.J.; Thorndike, R.M. Cross-Cultural Research Methods; John Wiley: New York, NY, USA, 1973; Volume 11. [Google Scholar]
- Alegria, M.; Vila, D.; Woo, M.; Canino, G.; Takeuchi, D.; Vera, M.; Febo, V.; Guarnaccia, P.; Aguilar-Gaxiola, S.; Shrout, P. Cultural relevance and equivalence in the NLAAS instrument: Integrating etic and emic in the development of cross-cultural measures for a psychiatric epidemiology and services study of Latinos. Int. J. Methods Psychiatr. Res. 2004, 13, 270–288. [Google Scholar] [CrossRef]
- Bravo, M.; Woodbury-Farina, M. The Spanish translation and cultural adaptation of the diagnostic interview schedule for children. Cult. Med. Psychiatry 1993, 17, 329. [Google Scholar] [CrossRef]
- Matías-Carrelo, L.E.; Chávez, L.M.; Negrón, G.; Canino, G.; Aguilar-Gaxiola, S.; Hoppe, S. The Spanish Translation and Cultural Adaptation of Five Mental Health Outcome Measures. Cult. Med. Psychiatry 2003, 27, 291–313. [Google Scholar] [CrossRef]
- Berry, J.W. Emics and Etics: A Symbiotic Conception. Cult. Psychol. 1999, 5, 165–171. [Google Scholar] [CrossRef]
- Maríñez-Lora, A.M.; Boustani, M.; Del Busto, C.T.; Leone, C. A Framework for Translating an Evidence-Based Intervention from English to Spanish. Hisp. J. Behav. Sci. 2016, 38, 117–133. [Google Scholar] [CrossRef]
- Gromkowska-Melosik, A. Cross-Cultural Research: Insider/Outsider Dichotomy Reconsidered. Przegląd Badań Eduk. (Educ. Stud. Rev.) 2021, 1, 205–214. [Google Scholar] [CrossRef]
- van der Wel, M.; van der Smissen, D.; Dierickx, S.; Cohen, J.; Hudson, P.; De Vleminck, A.; Tutt, L.; Scott, D.; Di Leo, S.; Arnfeldt, C.M.; et al. Systematic translation and adaptation of the FOCUS program, a USA-based supportive intervention for persons with cancer and their family caregivers, for use in six European countries. Support. Care Cancer 2022, 30, 9763–9770. [Google Scholar] [CrossRef]
- Häder, M. Delphi-Befragungen: Ein Arbeitsbuch; Springer VS: Wiesbaden, Germany, 2009. [Google Scholar]
- Turoff, M.; Linstone, H.A. The Delphi Method-Techniques and Applications; Addison-Wesley: Boston, MA, USA, 2002. [Google Scholar]
- Aengenheyster, S.; Cuhls, K.; Gerhold, L.; Heiskanen-Schüttler, M.; Huck, J.; Muszynska, M. Real-Time Delphi in practice—A comparative analysis of existing software-based tools. Technol. Forecast. Soc. Chang. 2017, 118, 15–27. [Google Scholar] [CrossRef]
- Harkness. VIII. Translation. Available online: http://ccsg.isr.umich.edu/translation.cfm#r14 (accessed on 10 April 2017).
- Silveira, L.C.J.; Rabelo-Silva, E.R.; Ávila, C.W.; Moreira, L.B.; Dickson, V.V.; Riegel, B. Cross-cultural Adaptation of the Self-care of Hypertension Inventory Into Brazilian Portuguese. J. Cardiovasc. Nurs. 2018, 33, 289–295. [Google Scholar] [CrossRef]
- Zwaanswijk, M.; van Dulmen, S. Advantages of asynchronous online focus groups and face-to-face focus groups as perceived by child, adolescent and adult participants: A survey study. BMC Res. Notes 2014, 7, 756. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Marques, I.C.; Theiss, L.M.; Johnson, C.Y.; McLin, E.; Ruf, B.A.; Vickers, S.M.; Fouad, M.N.; Scarinci, I.C.; Chu, D.I. Implementation of virtual focus groups for qualitative data collection in a global pandemic. Am. J. Surg. 2021, 221, 918–922. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Krueger, R.A. Focus Groups: A Practical Guide for Applied Research; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Speziale, H.S.; Carpenter, D.R. Qualitative Research in Nursing; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- MacQueen, K.M.; McLellan-Lemal, E.; Kay, K.; Milstein, B. Codebook Development for Team-Based Qualitative Analysis. CAM J. 1998, 10, 31–36. [Google Scholar] [CrossRef]
- Epstein, J.; Osborne, R.H.; Elsworth, G.R.; Beaton, D.E.; Guillemin, F. Cross-cultural adaptation of the Health Education Impact Questionnaire: Experimental study showed expert committee, not back-translation, added value. J. Clin. Epidemiol. 2013, 68, 360–369. [Google Scholar] [CrossRef]
- Love, R.; Santana, R.F. Advanced nursing practice training: The reality of the United States and the first steps of Brazil. Rev. Esc. Enferm. USP 2022, 56. [Google Scholar] [CrossRef]
- Poveda, V.d.B.; Nogueira, L.d.S. Advanced Nursing Practice: The Next Achievement of Brazilian Nursing. Rev. Esc. Enferm. USP 2022, 56. [Google Scholar] [CrossRef] [PubMed]
- Conselho Federal de Enfermagem. Carta Aberta Explica Posição do Cofen sobre EaD: Ensino Remoto Emergencial e Ensino a Distância: Entenda o Porquê de não Apoiarmos o EaD no Ensino de Graduação e na Formação Técnica em Enfermagem. Available online: http://www.cofen.gov.br/carta-aberta-explica-posicao-do-cofen-sobre-ead_97472.html (accessed on 23 July 2022).
- Joye, C.R.; Moreira, M.M.; Rocha, S.S.D. Educação a Distância ou Atividade Educacional Remota Emergencial: Em busca do elo perdido da educação escolar em tempos de COVID-19. Res. Soc. Dev. 2020, 9, e521974299. [Google Scholar] [CrossRef]
- Baggenstoss, S.; Sznitowski, A.M.; Camyla Piran Stiegler, L.; Lima, A. O Ensino Remoto Emergencial e seu Legado no Ensino Superior: Contribuições e Perspectivas; UFSC: São Carlos, Brazil, 2023. [Google Scholar]
- Dutra, S.; Kumar, K.; Clochesy, J. Instruction strategies for drug calculation skills: A systematic review of the literature. Nurse Educ. Today 2022, 111, 105299. [Google Scholar] [CrossRef]
- Teixeira Netto, J.; Andrade, Z.P.; Romano, M.R.R. Inclusão digital e literacia em saúde: Uma experiência educativa em tempos de pandemia do COVID-19. Res. Soc. Dev. 2022, 11, e11011326415. [Google Scholar] [CrossRef]
- Pereira Neto, A.; Ribeiro, B.D.; Guljor, A.P.F.; Barbosa, L.; Sampaio, C.M.A.; Castro, C.A.d.; Amarante, P. Eu quero entrar na rede: Análise de uma experiência de inclusão digital com usuários do Caps. Saúde Debate 2021, 44, 58–69. [Google Scholar] [CrossRef]
- Moreira, F.G.; De Oliveira, D.B. Direito à educação: Acesso à internet e o mínimo existencial. Braz. J. Dev. 2023, 9, 1968–1980. [Google Scholar] [CrossRef]
- Cavalcante, A.M.; Marquezini, M.V.; Mendes, L.; Moreno, C.S. 5G for Remote Areas: Challenges, Opportunities and Business Modeling for Brazil. IEEE Access 2021, 9, 10829–10843. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).