



Rotation of 3D Anatomy Models Is Associated with Underperformance of Students with Low Visual-Spatial Abilities: A Two-Center Randomized Crossover Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
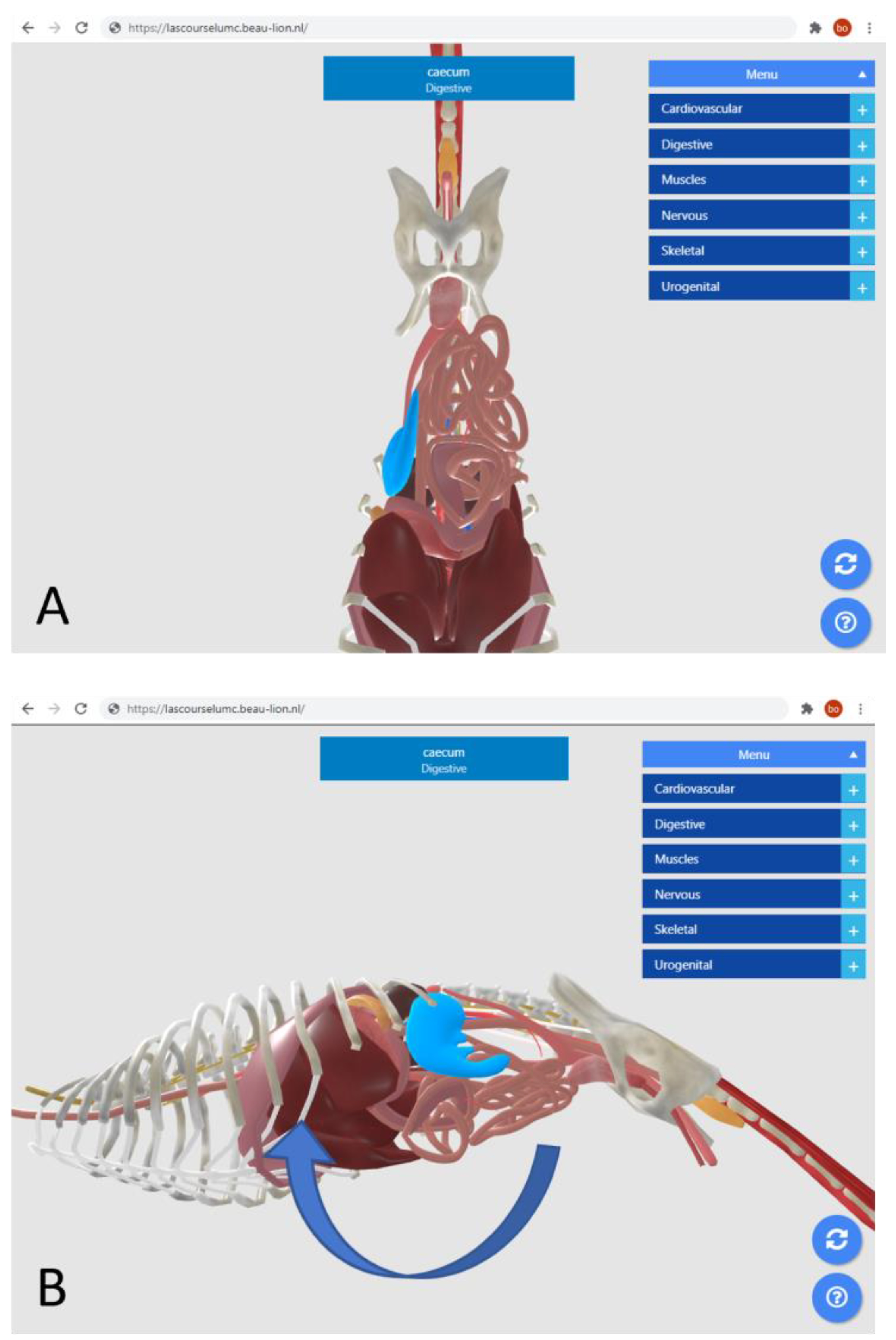
2.1. Interactive Monoscopic Two-Dimensional and Three-Dimensional Visualisation
2.2. Visual-Spatial Ability Test
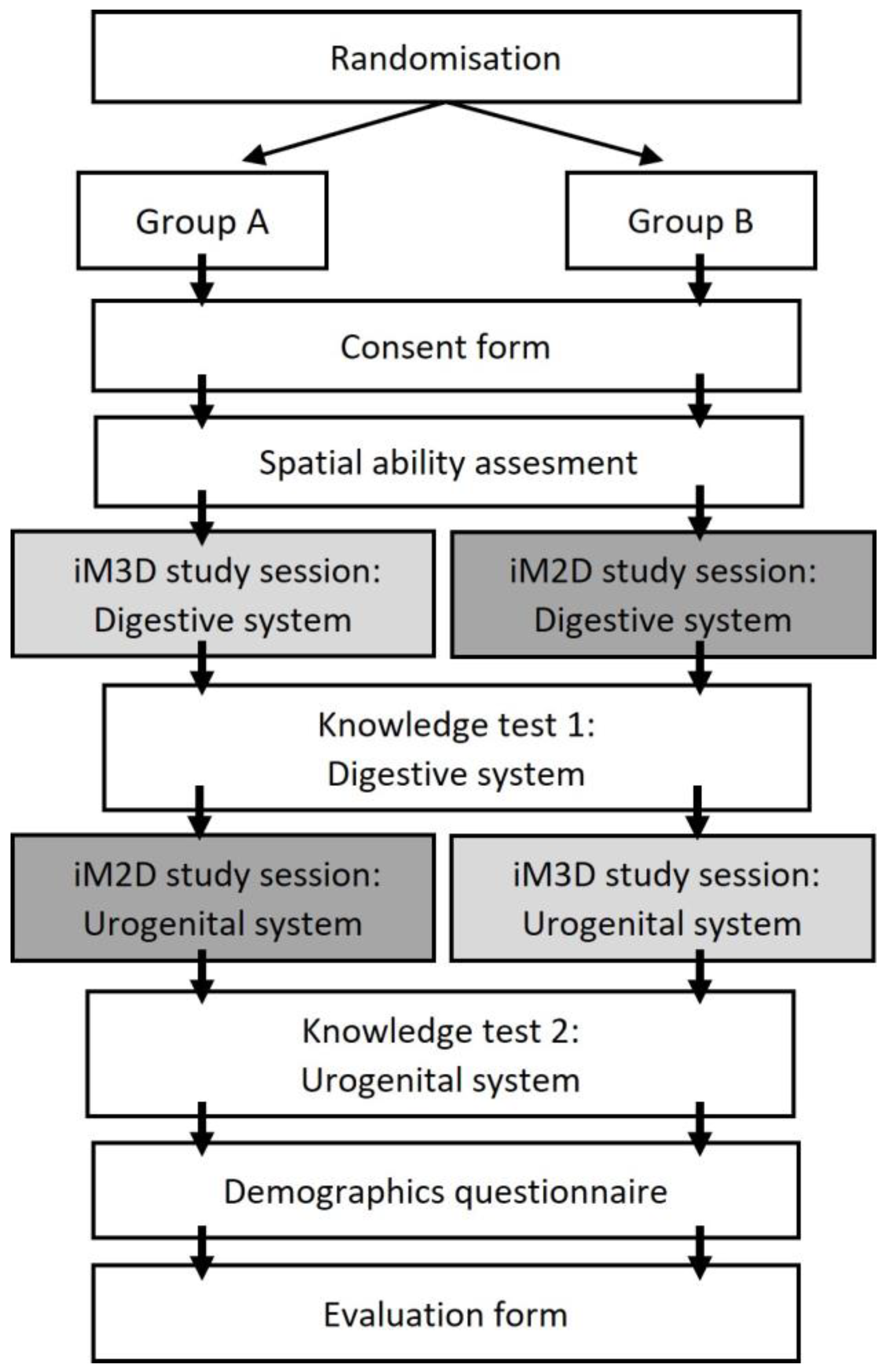
2.3. Study Design
2.4. Study Population
2.5. Randomisation and Pseudonymisation
2.6. Study Sessions and Knowledge Tests
2.7. Participant’s Demographics
2.8. Evaluation of Learning Experience
2.9. Experimental Environment
2.10. Statistical Analysis
3. Results
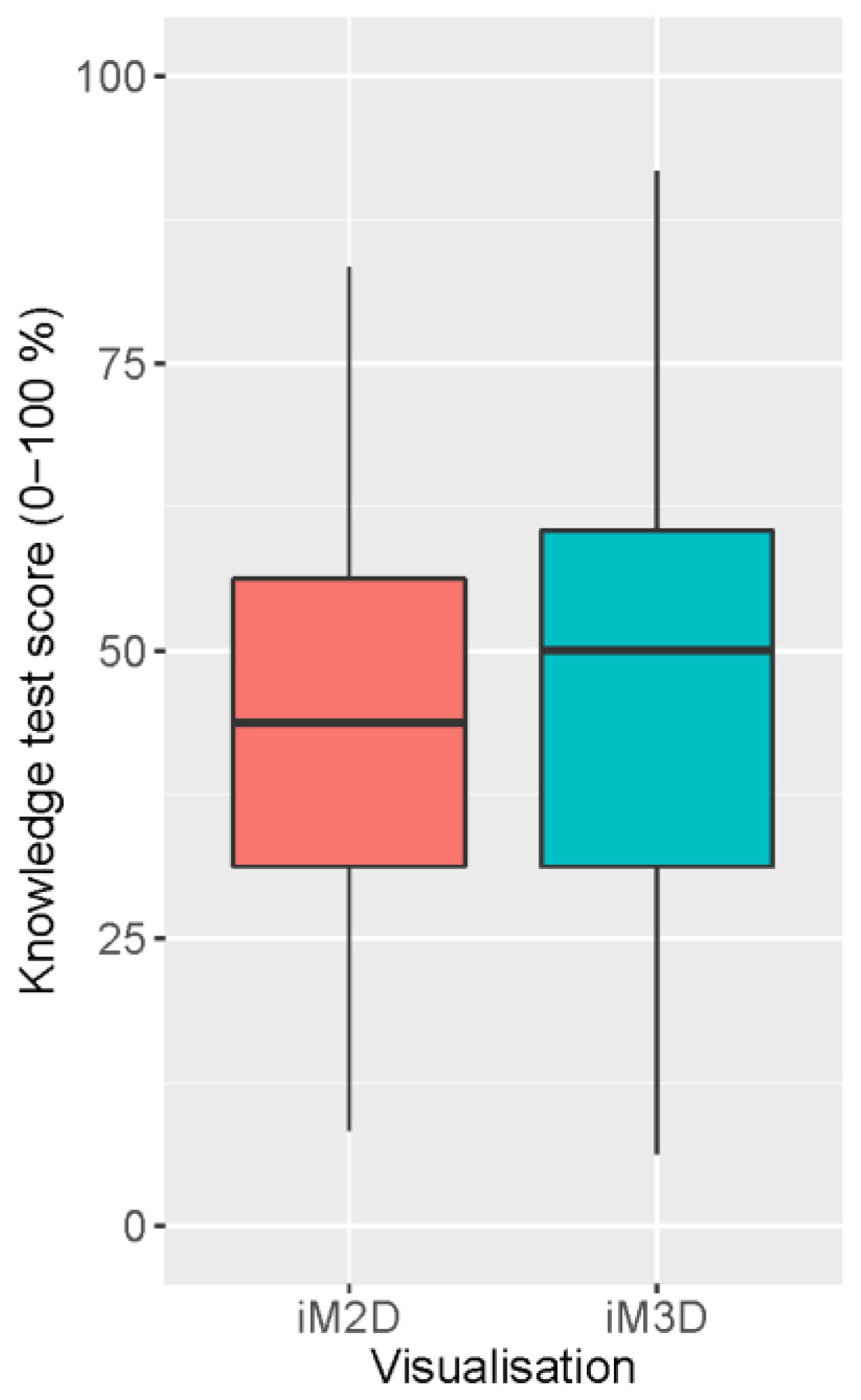
3.1. Overall Scores on the Anatomy Knowledge Test
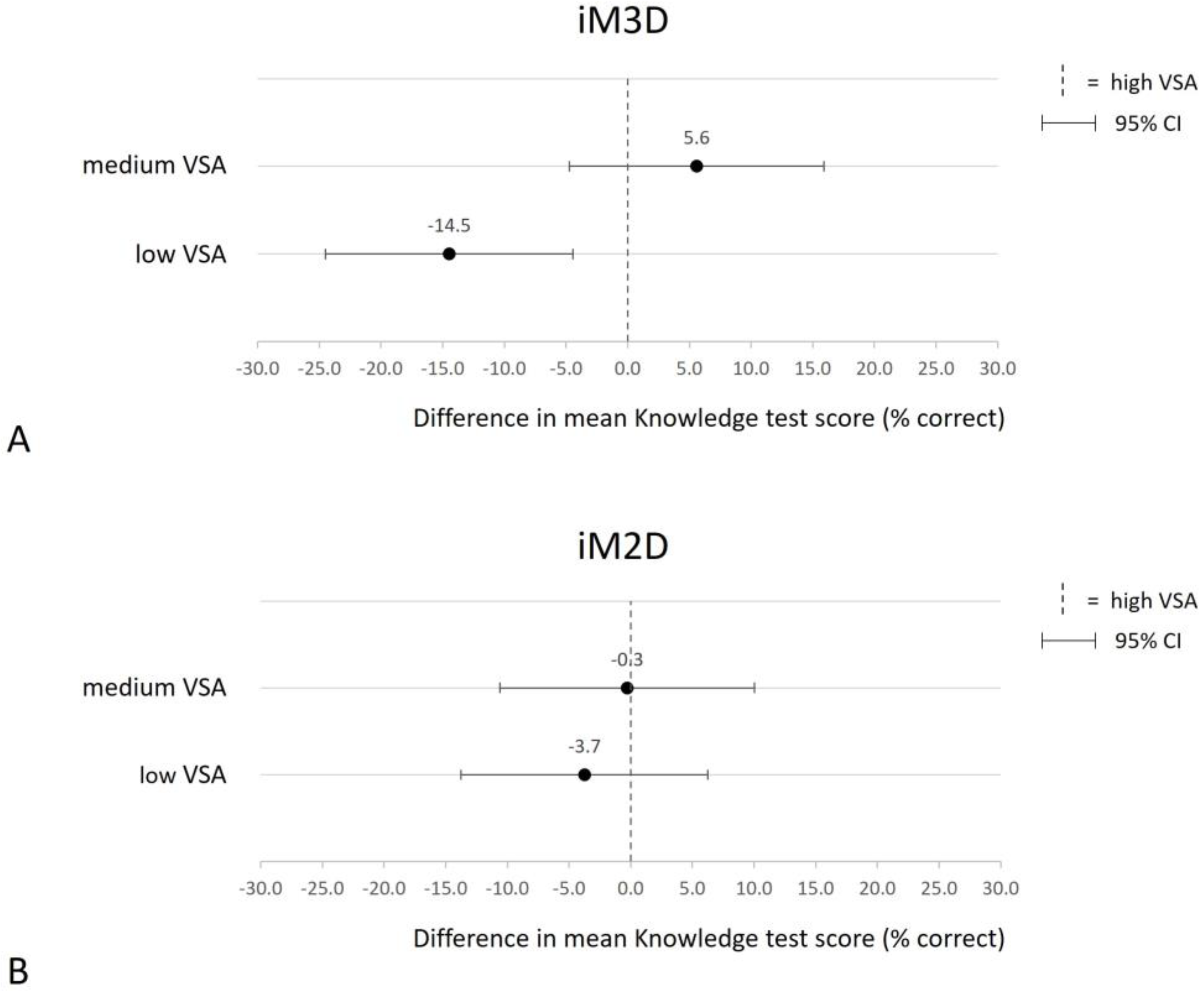
3.2. Effects of Study Parameters on Knowledge Test Scores
3.3. Participants Feedback
4. Discussion
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Learning Goals Digestive System At the End of the Learning Session, Students Should Be Able to: | |
|---|---|
| Identify the following structures: | Esophagus |
| Stomach | |
| Duodenum | |
| Jejunum | |
| Ileum | |
| Cecum | |
| Colon | |
| Liver | |
| Spleen | |
| Pancreas | |
| Caudal vena cava | |
| Aorta | |
| Cranial mesenteric artery | |
| Describe the course of the following structures: | Duodenum |
| Cecum | |
| Colon | |
| Caudal vena cava | |
| Aorta | |
| Cranial mesenteric artery | |
| Identify the organs that are in direct contact with the following structures (disregarding any possible mesenteric membranes): | Duodenum |
| Cecum | |
| Colon | |
| Pancreas | |
| Learning Goals Urogenital System of the Male Rat At the End of the Learning Session, Students Should Be Able to: | |
|---|---|
| Identify the following anatomical structures: | Testis |
| Epididymis | |
| Ductus deferens | |
| Prostate | |
| Vesicular glands | |
| Coagulating glands | |
| Penis | |
| Kidneys | |
| Adrenal glands | |
| Ureter | |
| Bladder | |
| Rectum | |
| Pelvic bone | |
| Determine the position of the following anatomical structures relative to the floor or bottom of the pelvic bone: | Rectum |
| Bladder | |
| Penis | |
| Kidneys | |
| Testis | |
| Identify the structures that are in direct contact with the following organs (disregarding any possible mesenteric membranes): | Vesicular gland Bladder |
| Describe the course of the following anatomical structures and how they run relative to each other: | Ductus deferens Ureter |
Appendix B
Appendix B.1. Knowledge Test 1
- Which part of the digestive tract enters (1) and which part leaves (2) the caecum? Additionally, on which side of the midline of the abdomen is the cecum located in the rat (3)?
- 2.
- The colon runs in a ................ (1) direction where it passes the cranial mesenteric artery to the left/right/cranial/caudal (2) side. Then, it runs in a ................ (3) direction where it passes the cranial mesenteric artery to the left/right/cranial/caudal (4) side. Lastly, it runs in a ................ (5) direction where it passes the cranial mesenteric artery to the left/right/cranial/caudal (6) side.
- 3.
- Which of these anatomical structures are in direct contact to the pancreas in the rat? (You can select multiple answers)
- 4.
- Where does the caudal vena cava enter the diaphragm? (1) Does the vena cava runs to the left/right/dorsal/ventral side or does it stay at the same course before entering the diaphragm? (2)
Appendix B.2. Knowledge Test 2
- Describe the position of the bulbourethral glands relative to the penis.
- 2.
- Describe the position of the testis (1) and the right and left kidneys (2) relative to the floor of the pelvic bone.
- 3.
- Describe in which direction the ductus deferens runs and how the ductus deferens crosses the ureter along its way to join the urethra.
- 4.
- Which of these anatomical structures are in direct contact to the bladder in the rat? (multiple answers can be selected)
Appendix C
Questionnaire
| Strongly Disagree | Disagree | Neither Agree Nor Disagree | Agree | Strongly Agree | |
| The 3D model allowed me to better understand spatial * relationships between anatomical structures than 2D views alone. | ○ | ○ | ○ | ○ | ○ |
| The 3D model allowed me to better understand the location of organs inside the animal as a whole. | ○ | ○ | ○ | ○ | ○ |
| I found it useful to be able to rotate and see the model from different viewpoints. | ○ | ○ | ○ | ○ | ○ |
| * spatial relationships is defined as how anatomical structures are located in the body relative to each other. | |||||
- ○
- Yes, please clarify:
- ○
- No
- ○
- Yes, please clarify:
- ○
- No
Appendix D
| Characteristic | Leiden University Medical Center (n = 49) | Utrecht University (n = 20) | Total (n = 69) | p-Value |
|---|---|---|---|---|
| Gender, n (%) | ||||
| Female | 36 (73) | 11 (55) | 47 (68.1) | 0.21 |
| Male | 12 (24) | 9 (45) | 21 (40.4) | |
| Unknown | 1 (2) | 0 (0) | 1 (1.4) | |
| Age, mean (±SD) | 26.0 (4.2) | 26.4 (5.8) | 26.1 (4.7) | 0.97 |
| Previous Education, n (%) | ||||
| ≤BSc | 23 (47) | 7 (35) | 30 (43.5) | 0.36 |
| ≥MSc | 26 (53) | 13 (65) | 39 (56.5) | |
| Mental Rotation Test, mean (±SD) | 16.2 (5.4) | 15.5 (5.6) | 16.0 (5.4) | 0.59 |
References
- Wheble, R.; Channon, S.B. What Use is Anatomy in First Opinion Small Animal Veterinary Practice? A Qualitative Study. Anat. Sci. Educ. 2021, 14, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Vdoviakova, K.; Petrovova, E.; Maloveska, M.; Kresakova, L.; Teleky, J.; Elias, M.Z.; Petrasova, D. Surgical Anatomy of the Gastrointestinal Tract and Its Vasculature in the Laboratory Rat. Gastroenterol. Res. Pract. 2016, 2016, 2632368. [Google Scholar] [CrossRef] [PubMed]
- Kararli, T.T. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharm. Drug Dispos. 1995, 16, 351–380. [Google Scholar] [CrossRef] [PubMed]
- Sugand, K.; Abrahams, P.; Khurana, A. The anatomy of anatomy: A review for its modernization. Anat. Sci. Educ. 2010, 3, 83–93. [Google Scholar] [CrossRef]
- Varner, C.; Dixon, L.; Simons, M.C. The Past, Present, and Future: A Discussion of Cadaver Use in Medical and Veterinary Education. Front. Vet. Sci. 2021, 8, 720740. [Google Scholar] [CrossRef]
- de Deus, J.; Santos, J.; de Haller, J.; Reiff, S.; Hardt, S.U.; Reginato, E.; Lupo, A.; Krajewski, R. Joint Statement EMOs—Use of Formaldehyde. Available online: https://www.uems.eu/__data/assets/pdf_file/0007/74851/Joint-statement-on-use-of-Formaldehyde-SEPT-2017.pdf (accessed on 26 June 2023).
- Knight, A. The Costs and Benefits of Animal Experiments, 1st ed.; Palgrave Macmillan: London, UK, 2011. [Google Scholar]
- Capaldo, T. The psychological effects on students of using animals in ways that they see as ethically, morally or religiously wrong. Altern. Lab. Anim. 2004, 32 (Suppl. S1B), 525–531. [Google Scholar] [CrossRef]
- Arluke, A.; Hafferty, F. From apprehension to fascination with “dog lab”: The use of absolutions by medical students. J. Contemp. Ethnogr. 1996, 25, 201–225. [Google Scholar] [CrossRef]
- Colombo, E.S.; Pelosi, A.; Prato-Previde, E. Empathy towards animals and belief in animal-human-continuity in Italian veterinary students. Anim. Welf. 2016, 25, 275–286. [Google Scholar] [CrossRef]
- Directive 2010/63/EU of the European Parliament and of the Council of 22 September 2010 on the Protection of Animals Used for Scientific Purposes. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32010L0063 (accessed on 26 June 2023).
- Statistics and Non-Technical Project Summaries. Improving Transparency through Open Access to Information on the Use of Animals for Scientific Purposes. Available online: https://environment.ec.europa.eu/topics/chemicals/animals-science/statistics-and-non-technical-project-summaries_en#statistical-database (accessed on 20 September 2023).
- Zemanova, M. Educational use of animals in Europe indicates a reluctance to implement alternatives. ALTEX 2021, 38, 490–506. [Google Scholar] [CrossRef]
- Ambition Statement on Innovation in Higher Education Using Fewer Laboratory Animals. Available online: https://www.nfu.nl/sites/default/files/2022-10/Streefbeeld_proefdiervrije_innovatie_in_het_postacademisch_onderwijs_0.pdf (accessed on 26 June 2023).
- Kumar, A.M.; Murtaugh, R.; Brown, D.; Ballas, T.; Clancy, E.; Patronek, G. Client donation program for acquiring dogs and cats to teach veterinary gross anatomy. J. Vet. Med. Educ. 2001, 28, 73–77. [Google Scholar] [CrossRef]
- Centre of Excellence for Plastination and Virtual Reality. Available online: https://www.uu.nl/en/organisation/faculty-of-veterinary-medicine/veterinary-research/research-centres-facilities/centre-of-excellence-for-plastination (accessed on 26 June 2023).
- Patronek, G.J.; Rauch, A. Systematic review of comparative studies examining alternatives to the harmful use of animals in biomedical education. J. Am. Vet. Med. Assoc. 2007, 230, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Knight, A. The effectiveness of humane teaching methods in veterinary education. Altex 2007, 24, 91–109. [Google Scholar] [CrossRef] [PubMed]
- Zemanova, M.; Knight, A. The Educational Efficacy of Humane Teaching Methods: A Systematic Review of the Evidence. Animals 2021, 11, 114. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.L.; Burnett, B.; Tunstall, R.G.; Abrahams, P.H. Complementing anatomy education using three-dimensional anatomy mobile software applications on tablet computers. Clin. Anat. 2014, 27, 313–320. [Google Scholar] [CrossRef]
- Little, W.B.; Artemiou, E.; Conan, A.; Sparks, C. Computer Assisted Learning: Assessment of the Veterinary Virtual Anatomy Education Software IVALA. Vet. Sci. 2018, 5, 58. [Google Scholar] [CrossRef]
- Linton, A.; Garrett, A.C.; Ivie, K.R., Jr.; Jones, J.D.; Martin, J.F.; Delcambre, J.J.; Magee, C. Enhancing Anatomical Instruction: Impact of a Virtual Canine Anatomy Program on Student Outcomes. Anat. Sci. Educ. 2022, 15, 330–340. [Google Scholar] [CrossRef]
- Badash, I.; Burtt, K.; Solorzano, C.A.; Carey, J.N. Innovations in surgery simulation: A review of past, current and future techniques. Ann. Transl. Med. 2016, 4, 453. [Google Scholar] [CrossRef]
- Pottle, J. Virtual reality and the transformation of medical education. Future Healthc. J. 2019, 6, 181–185. [Google Scholar] [CrossRef]
- Hackett, M.; Proctor, M. Three-Dimensional Display Technologies for Anatomical Education: A Literature Review. J. Sci. Educ. Technol. 2016, 25, 641–654. [Google Scholar] [CrossRef]
- Bulthoff, H.H.; Edelman, S.Y.; Tarr, M.J. How are three-dimensional objects represented in the brain? Cereb. Cortex 1995, 5, 247–260. [Google Scholar] [CrossRef]
- Kozhevnikov, M.; Hegarty, M. A dissociation between object manipulation spatial ability and spatial orientation ability. Mem. Cognit. 2001, 29, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, M. Components of Spatial Intelligence. In The Psychology of Learning and Motivation; Psychology of Learning and Motivation; Academic Press: Cambridge, MA, USA, 2010; Volume 52, pp. 265–297. [Google Scholar]
- Bogomolova, K.; van der Ham, I.J.M.; Dankbaar, M.E.W.; van den Broek, W.W.; Hovius, S.E.R.; van der Hage, J.A.; Hierck, B.P. The Effect of Stereoscopic Augmented Reality Visualization on Learning Anatomy and the Modifying Effect of Visual-Spatial Abilities: A Double-Center Randomized Controlled Trial. Anat. Sci. Educ. 2020, 13, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.X.; Norman, G.R.; Eva, K.W.; Spero, L.; Sharan, S. Is there any real virtue of virtual reality?: The minor role of multiple orientations in learning anatomy from computers. Acad. Med. 2002, 77, S97–S99. [Google Scholar] [CrossRef] [PubMed]
- Levinson, A.J.; Weaver, B.; Garside, S.; McGinn, H.; Norman, G.R. Virtual reality and brain anatomy: A randomised trial of e-learning instructional designs. Med. Educ. 2007, 41, 495–501. [Google Scholar] [CrossRef]
- Garg, A.X.; Norman, G.; Sperotable, L. How medical students learn spatial anatomy. Lancet 2001, 357, 363–364. [Google Scholar] [CrossRef]
- Johnston, E.B.; Cumming, B.G.; Landy, M.S. Integration of stereopsis and motion shape cues. Vis. Res. 1994, 34, 2259–2275. [Google Scholar] [CrossRef]
- Bogomolova, K.; Vorstenbosch, M.A.T.M.; El Messaoudi, I.; Holla, M.; Hovius, S.E.R.; Van Der Hage, J.A.; Hierck, B.P. Effect of binocular disparity on learning anatomy with stereoscopic augmented reality visualization: A double center randomized controlled trial. Anat. Sci. Educ. 2023, 16, 87–98. [Google Scholar] [CrossRef]
- Bogomolova, K.; Hierck, B.P.; Looijen, A.E.M.; Pilon, J.N.M.; Putter, H.; Wainman, B.; Hovius, S.E.R.; van der Hage, J.A. Stereoscopic three-dimensional visualisation technology in anatomy learning: A meta-analysis. Med. Educ. 2021, 55, 317–327. [Google Scholar] [CrossRef]
- Mather, G. Foundations of Sensation and Perception, 2nd ed.; Psychology Press: Hove, UK, 2009. [Google Scholar]
- Yammine, K.; Violato, C. A meta-analysis of the educational effectiveness of three-dimensional visualization technologies in teaching anatomy. Anat. Sci. Educ. 2015, 8, 525–538. [Google Scholar] [CrossRef]
- NVWA. Jaaroverzicht Dierproeven en Proefdieren van de Nederlandse Voedsel- en Warenautoriteit. Available online: https://www.nvwa.nl/documenten/dier/dierenwelzijn/zo-doende/publicaties/zo-doende-2019-jaaroverzicht-dierproeven-en-proefdieren (accessed on 26 June 2023).
- turbosquid.com 3D Rat Model. Available online: https://www.turbosquid.com/3d-models/dugm01-rat-anatomy-male-max/843255 (accessed on 26 June 2023).
- Blender Foundation. Blender, v2.8, Amsterdam, The Netherlands. Available online: https://www.blender.org/download/releases/2-80/ (accessed on 26 June 2023).
- Palmer, J. BlenderExporter, v6.4; Github: San Francisco, CA, USA, 2020. Available online: https://github.com/BabylonJS/BlenderExporter(accessed on 21 June 2023).
- Babylon.js, v5; Microsoft Corporation: Redmond, WA, USA. Available online: https://www.babylonjs.com/(accessed on 26 June 2023).
- Shepard, R.N.; Metzler, J. Mental rotation of three-dimensional objects. Science 1971, 171, 701–703. [Google Scholar] [CrossRef]
- Vandenberg, S.G.; Kuse, A.R. Mental rotations, a group test of three-dimensional spatial visualization. Percept. Mot. Ski. 1978, 47, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Laeng, B.; Latham, K.; Jackson, M.; Zaiyouna, R.; Richardson, C. A redrawn Vandenberg and Kuse mental rotations test: Different versions and factors that affect performance. Brain Cogn. 1995, 28, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Wet op de Dierproeven. Available online: https://wetten.overheid.nl/BWBR0003081/2021-07-01 (accessed on 26 June 2023).
- Laboratory Animal Science Course Utrecht University. Available online: https://www.uu.nl/en/professionals/programmes/laboratory-animal-science (accessed on 26 June 2023).
- Laboratory Animal Science Course Leiden University Medical Center. Available online: https://studiegids.universiteitleiden.nl/search?for=courses&q=&edition=2021-2022 (accessed on 26 June 2023).
- R Core Team. R: A Language and Environment for Statistical Computing, 4.1.3; R Foundation for Statistical Computing: Vienna, Austria, 2022. Available online: https://www.R-project.org(accessed on 26 June 2023).
- RStudio Team. RStudio, 2.1.461; Posit Software, PBC: Boston, MA, USA, 2022. Available online: https://posit.co/download/rstudio-desktop/(accessed on 20 June 2023).
- Pinheiro, J. nlme: Linear and Nonlinear Mixed Effects Models, v3.1-155; CRAN: Vianna, Austria, 2022. Available online: https://CRAN.R-project.org/package=nlme(accessed on 26 June 2023).
- Cui, D.; Wilson, T.D.; Rockhold, R.W.; Lehman, M.N.; Lynch, J.C. Evaluation of the effectiveness of 3D vascular stereoscopic models in anatomy instruction for first year medical students. Anat. Sci. Educ. 2017, 10, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Nelson, A.J.; Wilson, T.D. Computer visualizations: Factors that influence spatial anatomy comprehension. Anat. Sci. Educ. 2012, 5, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Norman, G.R.; Spero, L.; Maheshwari, P. Do virtual computer models hinder anatomy learning? Acad. Med. 1999, 74, S87–S89. [Google Scholar] [CrossRef]
- Huk, T. Who benefits from learning with 3D models? the case of spatial ability. J. Comput. Assist. Learn. 2006, 22, 392–404. [Google Scholar] [CrossRef]
- Khot, Z.; Quinlan, K.; Norman, G.R.; Wainman, B. The relative effectiveness of computer-based and traditional resources for education in anatomy. Anat. Sci. Educ. 2013, 6, 211–215. [Google Scholar] [CrossRef]
- Kirschner, P.A.; van Merriënboer, J.J.G. Do Learners Really Know Best? Urban Legends in Education. Educ. Psychol. 2013, 48, 169–183. [Google Scholar] [CrossRef]
- Cook, D.A. Avoiding confounded comparisons in education research. Med. Educ. 2009, 43, 102–104. [Google Scholar] [CrossRef]
- Linn, M.C.; Petersen, A.C. Emergence and characterization of sex differences in spatial ability: A meta-analysis. Child. Dev. 1985, 56, 1479–1498. [Google Scholar] [CrossRef]
- Voyer, D.; Voyer, S.; Bryden, M.P. Magnitude of sex differences in spatial abilities: A meta-analysis and consideration of critical variables. Psychol. Bull. 1995, 117, 250–270. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.M.; Son, T. Androgens and eye movements in women and men during a test of mental rotation ability. Horm. Behav. 2007, 52, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Moè, A.; Pazzaglia, F. Following the instructions! Learn. Individ. Differ. 2006, 16, 369–377. [Google Scholar] [CrossRef]
- Voyer, D. Time limits and gender differences on paper-and-pencil tests of mental rotation: A meta-analysis. Psychon. Bull. Rev. 2011, 18, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, M. Ability and sex differences in spatial thinking: What does the mental rotation test really measure? Psychon. Bull. Rev. 2018, 25, 1212–1219. [Google Scholar] [CrossRef]
- Stull, A.T.; Hegarty, M.; Mayer, R.E. Getting a Handle on Learning Anatomy With Interactive Three-Dimensional Graphics. J. Educ. Psychol. 2009, 101, 803–816. [Google Scholar] [CrossRef]
- Ziemek, T.; Creem-Regehr, S.; Thompson, W.; Whitaker, R. Evaluating the Effectiveness of Orientation Indicators with an Awareness of Individual Differences. Acm Trans. Appl. Percept. 2012, 9, 7. [Google Scholar] [CrossRef]
- Uttal, D.H.; Meadow, N.G.; Tipton, E.; Hand, L.L.; Alden, A.R.; Warren, C.; Newcombe, N.S. The malleability of spatial skills: A meta-analysis of training studies. Psychol. Bull. 2013, 139, 352–402. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.; Bellemare, C.; Toulouse, J.; Wells, G.A. Spatial Abilities Training in Anatomy Education: A Systematic Review. Anat. Sci. Educ. 2020, 13, 71–79. [Google Scholar] [CrossRef]
- Hegarty, M.; Keehner, M.; Cohen, C.; Montello, D.R.; Lippa, Y. The Role of Spatial Cognition in Medicine: Applications for Selecting and Training Professionals. In Applied Spatial Cognition: From Research to Cognitive Technology; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2007; pp. 285–315. [Google Scholar]
- Langlois, J.; Bellemare, C.; Toulouse, J.; Wells, G.A. Spatial abilities and technical skills performance in health care: A systematic review. Med. Educ. 2015, 49, 1065–1085. [Google Scholar] [CrossRef]


| Characteristic | Group A iM3D→iM2D (n = 37) | Group B iM2D→iM3D (n = 32) | Total (n = 69) | p-Value |
|---|---|---|---|---|
| Academic Institute, n (%) | ||||
| Leiden University Medical Center | 26 (70) | 23 (72) | 49 (71) | 0.88 |
| Utrecht University | 11 (30) | 9 (28) | 20 (29) | |
| Gender, n (%) | ||||
| Female | 27 (73) | 20 (62) | 47 (68.1) | 0.42 |
| Male | 10 (27) | 11 (34) | 21 (30.4) | |
| Unknown | 0 | 1 (3) | 1 (1.4) | |
| Age, mean (±SD) | 25.8 (4.7) | 26.5 (4.7) | 26.1 (4.7) | 0.63 |
| Previous Education, n (%) | ||||
| ≤BSc | 14 (38) | 16 (50) | 30 (43.5) | 0.31 |
| ≥MSc | 23 (62) | 16 (50) | 39 (56.5) | |
| Mental Rotation Test, mean (±SD) | 15.6 (5.3) | 16.5 (5.6) | 16.0 (5.4) | 0.39 |
| Statement | Mean (±SD) | n | VSA |
|---|---|---|---|
| The 3D model allowed me to better understand spatial * relationships between anatomical structures than 2D views alone. | 4.4 (±0.7) | 22 | high |
| 4.2 (±0.7) | 22 | medium | |
| 4.3 (±0.9) | 25 | low | |
| The 3D model allowed me to better understand the location of organs inside the animal as a whole. | 4.3 (±0.7) | 22 | high |
| 3.9 (±0.9) | 22 | medium | |
| 4.2 (±0.9) | 24 | low | |
| I found it useful to be able to rotate and see the model from different viewpoints. | 4.7 (±0.5) | 22 | high |
| 4.5 (±0.5) | 22 | medium | |
| 4.5 (±0.7) | 24 | low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leeuwen, B.S.v.; Dollé, A.E.D.; Vernooij, J.C.M.; Hierck, B.P.; Salvatori, D.C.F. Rotation of 3D Anatomy Models Is Associated with Underperformance of Students with Low Visual-Spatial Abilities: A Two-Center Randomized Crossover Trial. Educ. Sci. 2023, 13, 992. https://doi.org/10.3390/educsci13100992
Leeuwen BSv, Dollé AED, Vernooij JCM, Hierck BP, Salvatori DCF. Rotation of 3D Anatomy Models Is Associated with Underperformance of Students with Low Visual-Spatial Abilities: A Two-Center Randomized Crossover Trial. Education Sciences. 2023; 13(10):992. https://doi.org/10.3390/educsci13100992
Chicago/Turabian StyleLeeuwen, Bo S. van, Anna E. D. Dollé, Johannes C. M. Vernooij, Beerend P. Hierck, and Daniela C. F. Salvatori. 2023. "Rotation of 3D Anatomy Models Is Associated with Underperformance of Students with Low Visual-Spatial Abilities: A Two-Center Randomized Crossover Trial" Education Sciences 13, no. 10: 992. https://doi.org/10.3390/educsci13100992
APA StyleLeeuwen, B. S. v., Dollé, A. E. D., Vernooij, J. C. M., Hierck, B. P., & Salvatori, D. C. F. (2023). Rotation of 3D Anatomy Models Is Associated with Underperformance of Students with Low Visual-Spatial Abilities: A Two-Center Randomized Crossover Trial. Education Sciences, 13(10), 992. https://doi.org/10.3390/educsci13100992