Abstract
Neck pain is a significant global health concern and a leading cause of disability. Conventional clinical neck assessments often rely on maximal Cervical Range of Motion (CROM) measurements, which may not accurately reflect functional limitations experienced during activities of daily living (ADLs). This study introduces a novel approach to evaluate neck functional status by employing a virtual reality (VR) environment to simulate an apple-harvesting task. Three-dimensional head kinematics were continuously recorded in 60 participants (30 with clinically significant neck pain and 30 asymptomatic) as they performed the task. Spectral analysis of the data revealed that individuals with neck pain exhibited slower head rotation speed, particularly in the transverse and frontal planes, compared to the pain-free group, as evidenced by higher spectral power in the low-frequency band [0, 0.1] Hz and lower power in the [0.1, 0.5] Hz band. Furthermore, participants with neck pain required significantly more time to complete the apple-harvesting task. The VR system demonstrated high usability (SUS score = 84.21), and no adverse effects were reported. These findings suggest that VR-based assessment during simulated ADLs can provide valuable information about the functional impact of neck pain beyond traditional CROM measurements, potentially enabling remote evaluation and personalized telerehabilitation strategies.
1. Introduction
Global estimates suggest that approximately 1.71 billion individuals are affected by musculoskeletal disorders [1]. Musculoskeletal conditions account for a substantial proportion of years lived with disability (YLDs), particularly among adults of working age (20–54 years). As this age group represents the period of highest economic and social productivity, disability during these years can lead to significant losses in human capital. This burden is increasingly acknowledged in international policy frameworks due to its wide-ranging societal impact [2].
Women have a higher prevalence of musculoskeletal disorders than men across all age groups, with peak incidence between 40 and 44 years [3]. Regionally, the highest incidence and age-adjusted YLD rates were reported in North Africa and the Middle East, with Iran having the highest burden, while New Zealand had the lowest. Spain experienced the greatest decline in these rates between 1990 and 2021 [3]. Although a slight reduction in adjusted rates is projected, the absolute number of cases is expected to continue to rise due to population aging, with a projected 269 million people affected by 2050 [4].
Neck pain is one of the most common musculoskeletal disorders, representing a significant source of disability [1]. Neck pain presents a substantial public health burden, impacting an estimated 222 million individuals and contributing to 22 million years lived with disability (YLDs) [5]. The lifetime prevalence of neck pain is considerable, with 30% to 50% of the general population reporting experiencing this condition [6]. Suboptimal management of neck pain is a leading cause of disability within musculoskeletal disorders, ranking fourth and often leading to chronic pain syndromes that pose considerable clinical management challenges [7].
The increasing prevalence of musculoskeletal disorders, including neck pain, is compounded by population aging and the adoption of sedentary lifestyles [8]. These conditions constitute the foremost contributor to YLDs worldwide, accounting for approximately 149 million YLDs, or 17% of the global burden. Neck pain affects individuals across their lifespans, from young adulthood to advanced age, highlighting its extensive societal impact [1].
Clinical assessment of individuals presenting with neck pain commonly involves the evaluation of Cervical Range of Motion (CROM) to quantify the range of neck movement in various planes [9]. CROM is frequently employed as a baseline measurement prior to treatment planning, as well as for longitudinal monitoring of patient progress [10]. Individuals experiencing neck pain often have restricted CROM and may exhibit pain at the limits of motion [11]. Furthermore, these individuals may present compensatory trunk movements, either conscious or unconscious, in response to limited or painful neck movement [12].
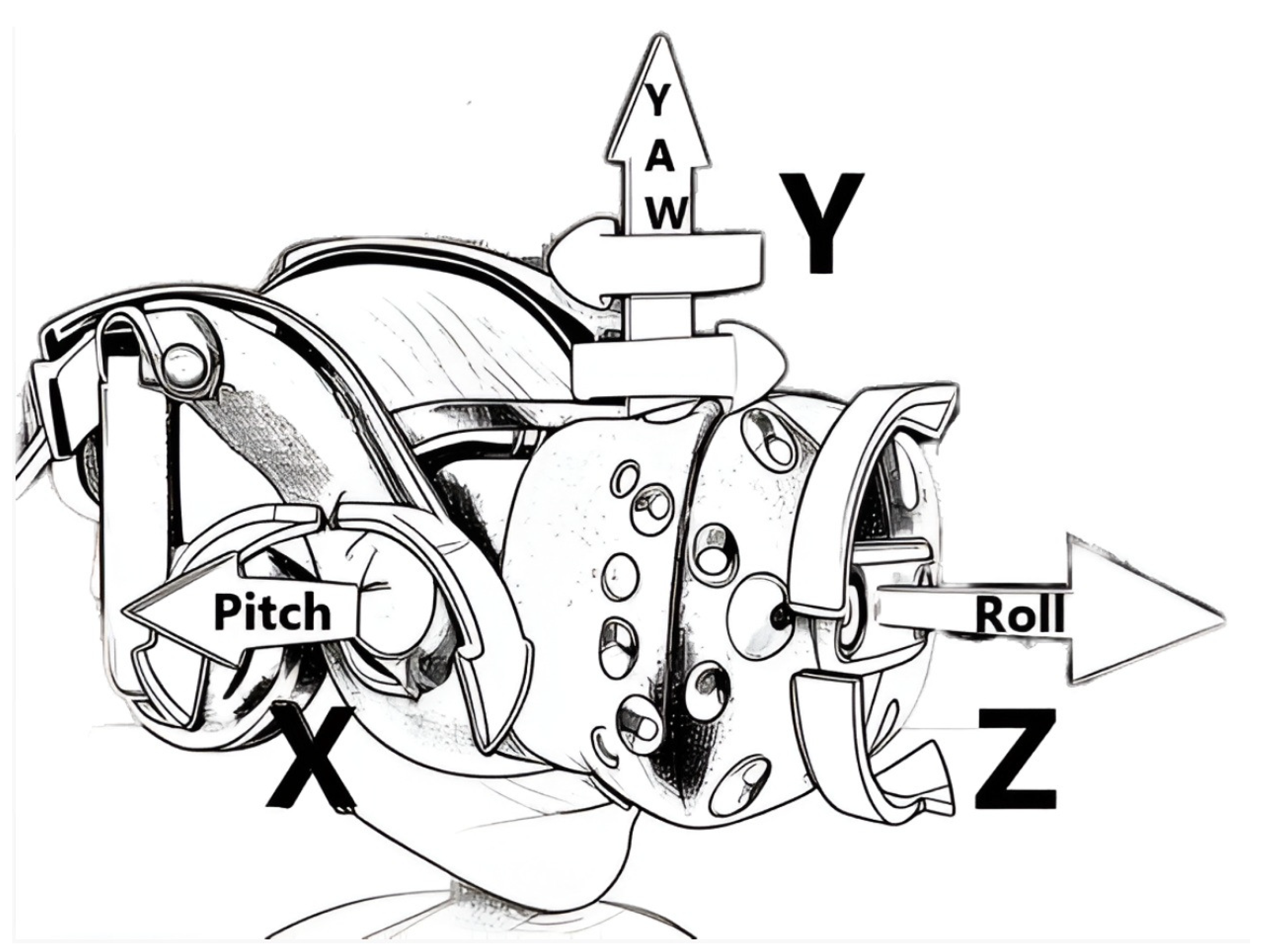
CROM assessment quantifies the angular displacement of the neck within its planes of motion. Specifically, the sagittal plane, which bisects the body into left and right halves, encompasses flexion (anterior movement of the head, approximating the chin to the chest) and extension (posterior movement of the head, directing the gaze upwards). Angular measurement within this plane is commonly designated as pitch (see Figure 1). The transverse plane, dividing the body into superior and inferior segments, corresponds to rotational movement (axial rotation of the head to the left or right). Angular measurement within this plane is commonly designated as yaw (see Figure 1). Finally, the frontal plane, which partitions the body into anterior and posterior aspects, allows for lateral flexion (abduction of the head, approximating the ear to the shoulder). Angular measurement within this plane is commonly known as roll (see Figure 1).
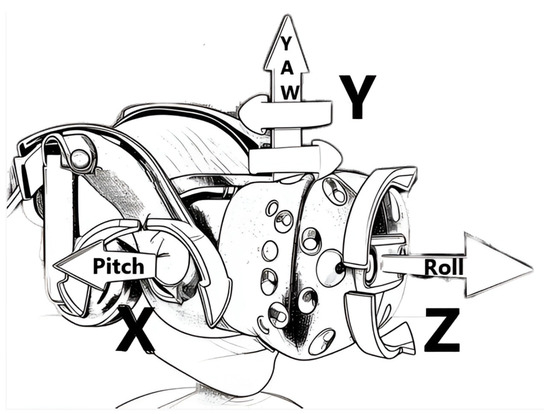
Figure 1.
The assessment of Cervical Range of Motion (CROM) quantifies the angular displacement of the neck across its planes of movement. The Head-Mounted Display (HMD) supporting six degrees of freedom can capture movement along the X, Y, and Z axes, as well as rotation around each axis, commonly referred to as pitch (nodding), yaw (turning), and roll (tilting).
Several instruments and methodologies are used to quantify cervical impairment. The goniometer remains a prevalent tool in clinical practice due to its portability, affordability, and ease of application [13]. This instrument facilitates the measurement of angular displacement within the sagittal (flexion–extension), transverse (rotation), and frontal (lateral flexion) planes. Despite the increasing availability of more advanced measurement systems, the goniometer continues to be widely used, especially in routine clinical assessments and in settings with limited access to high-cost equipment [14,15]. However, its inter-rater and intra-rater reliability has been reported to be moderate, with Intraclass Correlation Coefficient (ICC) values typically around 0.85 across movement directions [13,16].
Alternative methodologies for CROM assessment include inclinometers, which operate by quantifying the angle of inclination relative to the vertical plane during cervical movements. These devices, available in both manual and digital configurations, provide a numerical representation of angular displacement across multiple planes [17,18]. Inertial measurement units (IMUs) have emerged as a promising technology for CROM assessment [19,20]. These compact, wireless sensors integrate accelerometers, gyroscopes, and magnetometers to track head kinematics and orientation in three-dimensional space. IMUs offer enhanced measurement reliability compared to goniometers and can be integrated into clinical protocols to quantify movement within the sagittal, transverse, and frontal planes. Furthermore, specialized CROM devices [17,21,22,23,24], incorporating integrated inclinometers and magnetometers, provide measurements of cervical motion across all planes.
Inertial sensors [19,20], electromagnetic tracking systems [25], and CROM devices [22] have demonstrated higher reproducibility and measurement precision. Inertial sensors have shown ICC values above 0.95 in most cases [20], while CROM devices present slightly more variable results, with reported ICCs ranging from 0.83 (for flexion–extension) to over 0.89 (for rotation and lateral flexion) [22]. These instruments offer greater reliability but also involve higher costs and operational complexity. Inclinometers [17] and electronic goniometers are also used in clinical and research settings, with digital versions generally offering improved performance. Reported ICCs for inclinometers range from 0.68 to 0.80 [17], while digital inclinometers tend to yield values above 0.85, showing better consistency [26]. Furthermore, photogrammetry techniques [27] and radiographic imaging [28] have been employed primarily in research environments due to their high cost, lack of portability, and need for complex setups. More recently, virtual reality (VR)-based systems have gained attention for their potential to combine immersive environments with accurate motion tracking [29,30,31]. These systems have shown high reliability in CROM assessment, with ICC values comparable to those of inertial systems (e.g., 0.94 for flexion–extension, 0.96 for rotation, and 0.91 for lateral flexion [31]), supporting their use in both clinical and experimental contexts.
The majority of prior investigations on the neck’s functional status have primarily focused on evaluating the maximal cervical excursions exhibited by participants, representing the full active range of motion (ROM) [20,32,33,34]. While total ROM serves as a practical and straightforward metric for movement analysis, it offers a limited representation of functional capacity, as most activities of daily living (ADLs) do not necessitate maximal ROM [35]. For instance, previous research has questioned the clinical relevance of reductions in total ROM following cervical spine fusion with respect to ADLs and overall quality of life (QoL). The movement amplitudes required for ADLs are generally considered to be substantially lower than the full active ROM. Moreover, despite the utility of conventional methodologies in quantifying cervical movement, they frequently fail to capture clinically pertinent aspects such as movement speed, smoothness, trajectory, and compensatory trunk movements (consciously or unconsciously executed to alleviate pain or facilitate movement). Consequently, the diagnostic utility of CROM assessment as an isolated metric has been challenged, as some studies have provided limited evidence supporting its role in the diagnosis of specific cervical pathologies. This has fueled a growing interest in the development of alternative approaches that provide a more comprehensive representation of cervical spine function in real-world contexts [35,36,37].
CROM has been documented during various ADLs, including door manipulation, desk-based writing, and telephone usage. However, these findings were derived from a limited cohort of healthy university students utilizing multiple head-mounted inclinometers during experimental trials. The manual operation of these devices required the interruption of participant movements to allow the observer to take readings from the device indicators, thereby restricting data acquisition to static neck positions at the end of each activity [33]. In a more recent study, CROM was assessed during ADLs in 60 asymptomatic subjects aged 20 to 75 years. Using a noninvasive electrogoniometer and torsiometer, the full and functional Cervical ROM required to complete these simulated ADLs was measured. The results showed that, overall, ADLs require a relatively small percentage of total Cervical ROM. For example, when backing up a car, 32% of sagittal motion, 26% of lateral motion, and 92% of rotation were used. Activities related to personal hygiene, such as washing hands and hair, shaving, and applying makeup, involved significantly higher ROM compared to locomotor activities such as walking and ascending or descending stairs. These findings provide reference data that can allow clinicians to accurately assess the impact of the functional status of the neck on ADLs and to design therapies more focused on improving a patient’s performance when performing ADLs and therefore a patient’s quality of life [35].
A VR Head-Mounted Display (HMD) facilitates the continuous tracking of three-dimensional head position and rotation over time [38]. This tracking system provides six degrees of freedom (6DoF), encompassing both translational and rotational kinematics of the HMD (see Figure 1). The kinematic data, including three-dimensional position, orientation, and temporal timestamps, can be recorded continuously throughout the virtual reality experience. This methodology enables the uninterrupted measurement of CROM while participants engage in ADLs within a virtual environment (VE), thereby eliminating the need for movement interruption during data acquisition.
VR environments offer a unique advantage: they enable immersive and standardized assessment protocols that can be executed autonomously. In such systems, the VR experience guides users through specific cervical movements while simultaneously capturing motion data [31]. Through this motion data capture, it is possible to ensure that controlled repetitive movements of the neck joints during rehabilitation are performed properly, allowing recovery times to be shortened and improving the success of treatment [10].
These capabilities significantly enhance the potential of VR for telematic applications, including remote assessment, diagnosis, rehabilitation, and follow-up of cervical impairments. Recent studies have demonstrated the efficacy of VR-based interventions in improving Cervical Range of Motion, reducing pain, and enhancing functional outcomes in patients with chronic neck pain [39,40]. These findings underscore the viability of VR as a comprehensive tool in the telemanagement of cervical conditions.
Previous studies have demonstrated that VR setups are a reliable tool for measuring maximum CROM [31,41]. One of the advantages of VR technology is its relatively flat learning curve, allowing individuals with or without prior anatomical knowledge to use an HMD for cervical spine assessment. The objective of this observational cross-sectional study was to compare head kinematics between patients with chronic neck pain and asymptomatic participants during the performance of functional tasks in an immersive VR environment. To achieve this objective, we aimed to design a novel VR immersive experience to allow for the analysis of head kinematics during the performance of a whole-body functional task. Specifically, participants were required to retrieve virtual apples from simulated trees within a VE, utilizing natural head and neck movements to complete the task. The apple-harvesting task was chosen because it involves multiplanar movements, including whole-body movements in response to external stimuli for a duration that lasts a few minutes. This allows for a functional assessment that more closely resembles the ADLs a subject performs in their everyday life and aligns with previous recommendations for further research to examine neck kinematics for additional functional tasks [42].
Apples are located at various heights in the trees, and some may have fallen to the ground. The user is surrounded by trees; thus, she needs to search around for apples, pick them, and put them in a basket. We recorded the three-dimensional head kinematics of 60 participants (30 with clinically significant neck pain and 30 asymptomatic) during the apple retrieval task. Subsequently, we conducted a comparative analysis utilizing spectrograms generated from the head movement in its three motion planes to investigate whether participants with pain exhibited diminished movement speed compared to the pain-free cohort. The analysis shows that subjects without neck pain performed faster movements and required less time to complete the task compared to those with neck pain; these differences were statistically significant.
2. Materials and Methods
2.1. Participants
This was a descriptive, observational, cross-sectional study. It was conducted at CEU San Pablo University and received approval from the CEU San Pablo University Ethics Committee (approval code: 495/21/39). The study involved 60 participants, 30 individuals with neck pain and 30 asymptomatic individuals. They were recruited from the university’s student and faculty population, as well as from patients at the university’s polyclinic.
The inclusion criteria for the neck pain group required self-reported non-specific mechanical cervical pain of at least 3 months’ duration and a pain intensity rating of 4 or higher on the 10-point numerical rating Visual Analogue Scale (VAS) [43] (see Section 2.4 for details). This cut-off value was selected to exclude patients with no pain or mild levels of pain, as usually pain intensity lower than 4/10 in VAS is considered mild [44,45]. Participants in the neck pain group were permitted to report concomitant headaches or upper cervical/shoulder discomfort. Exclusion criteria included a history of craniocervical surgery; bony deformities in the thoracic, cervical, or cranial region; vertigo/dizziness; and complex regional syndrome. Participants in the pain group had a mean neck pain intensity of on the VAS at the time of evaluation. The asymptomatic group consisted of participants reporting no cervical pain within the preceding three months and no history of neck pain treatment.
2.2. Experimental Setup
For this study, we utilized the HTC Vive Pro Eye™HMD (HTC Corporation, Taoyuan, Taiwan), a high-end VR system. The device features a dual OLED display with a combined resolution of 2880 × 1600 pixels (1440 × 1600 per eye). It offers a 110-degree field of view and a refresh rate of 90 Hz. The system includes SteamVR™ 2.0 tracking with two Lighthouse™ v2 base stations (Valve Corporation, Bellevue, WA, USA), which allow for precise 6DoF motion tracking, enabling accurate head movement recording.
The VR environment was powered by an HP OMEN™ laptop (HP Inc., Palo Alto, CA, USA) equipped with an Intel® Core™ i7-10750H processor, 16GB of RAM, and an 8GB NVIDIA® GeForce® RTX™ 2070 Super GPU. The system operated on Windows® 10 and ran the VR environment using SteamVR™. The experimental setup included a custom-developed VR application designed to simulate an apple-harvesting task described in the next section.
The Lighthouse™ v2 (Valve Corporation, USA) base stations provide precise positional and orientational tracking of the HMD. By detecting the temporal disparities in the illumination of photodiodes on the HMD and hand controllers via a sweeping laser array, these base stations provide the three-dimensional spatial data. This technology enhances the precision in capturing subtle and rapid user kinematics, thereby improving immersion through the accurate registration of virtual elements, such as picking apples in the apple-harvesting task within the VE. The configuration of the virtual scene is predicated solely on the initial physical position of the HMD, thereby ensuring a consistent and immersive representation of the simulated environment. An earlier study by the authors utilizing this same virtual reality equipment showed that, when used to assess maximum CROM in each plane, this setup had more reliability than a traditional goniometer [31].
2.3. Task Design
The Virtual Reality Toolkit (VRTK) is a collection of solutions to assist in the creation of VR applications [46]. As part of its demonstration capabilities, the VRTK includes a “Farmyard” example that showcases various locomotion systems, interaction paradigms, and control methodologies. This example features a range of activities set within a farmyard environment, such as a workshop scenario where users are required to place tools in their designated positions. It also incorporates diverse movement modalities and interactive objects, including a manipulable and fireable pistol, alongside several other items enabling user interaction.
The virtual reality application employed in this study is a modified version of VRTK v4 Beta’s Farmyard example, specifically adapted to focus on the retrieval of apples from different trees. This version was developed using the Unity® 2018.4.33 engine.
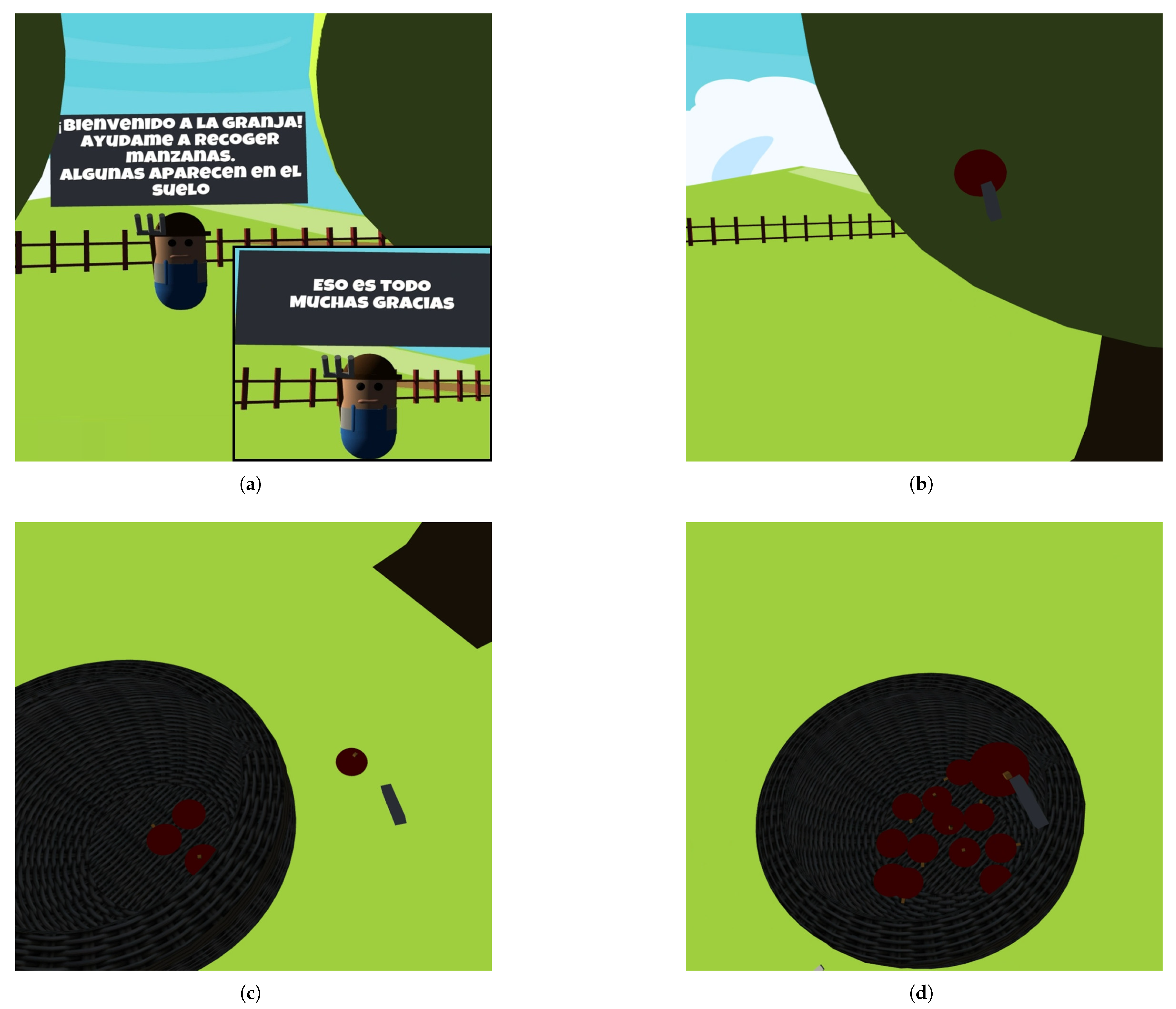
At the beginning of the activity, the participant is positioned at the center of a virtual orchard consisting of three apple trees arranged in a triangular formation, one located anterior-right, one anterior-left, and one posterior. Each tree is located approximately 1.5 m from a central basket placed on the ground that is also placed near the participant, serving as the receptacle for the collected apples (see Figure 2d). A non-player character (NPC), represented as a farmer and positioned in front of the participant, provides visual instructions via floating text in Spanish (see Figure 2a). The NPC first welcomes the participant and explains the task, noting that some apples may also appear on the ground. Participants are instructed to collect the apples—using the grip button on either VR controller—and place them in the basket. Upon successful placement of an apple in the basket, another apple will spawn in a different location, and this process is repeated until a total of sixteen apples have been collected. Once all sixteen apples have been deposited, the NPC signals the completion of the task and expresses gratitude (see Figure 2a).
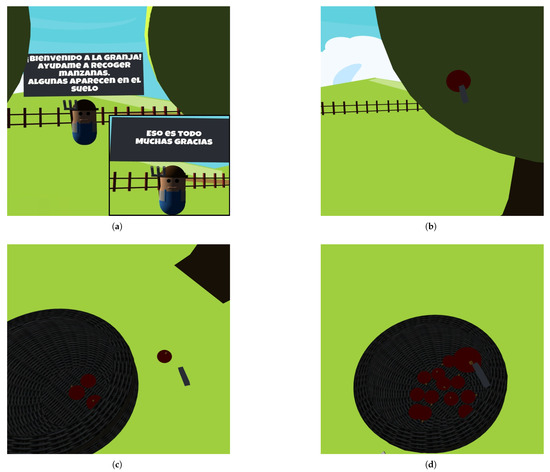
Figure 2.
Images from the apple harvesting app used: (a) A farmer holding a sign that indicates the start and end of the task and provides instructions (In Spanish: “Welcome to the Farm! Help me collect apples. Some may appear on the ground.” & “That’s all, thank you very much.”) for carrying out the task. (b) An apple that appears on a tree. (c) An apple that appears on the ground. (d) The basket where harvested apples are stored. Once an apple is placed in the basket, a new apple appears in one of the trees surrounding the user or on the ground.
The apple spawning sequence is predefined and identical for all participants to ensure experimental consistency. As part of an initial familiarization phase, the first four apples appear in each of the four possible locations: the first on the anterior-right tree (see Figure 2b), the second on the anterior-left tree, the third on the posterior tree, and the fourth on the ground (see Figure 2c). After this initial phase, the remaining twelve apples appear in varying order across the same four locations, ensuring that each tree and the ground hosts a total of four apples by the end of the task. Although the complete spawning sequence does not follow an obvious pattern (thus minimizing learning effects), all participants encounter the same distribution and order throughout the session. The positions of all apples are fixed and predefined in a comma-separated value (CSV) configuration file.
To ensure that all apples are within reach, the system calculates the user’s initial head position using the HMD at the start of the session. Apple positions are then determined by applying fixed normalized vectors relative to this reference point. For arboreal apples, these vectors are anchored at the center of each tree’s foliage, placing the apples visibly within the canopy and oriented toward the participant. Apples that spawn on the ground appear near the user’s starting position. This approach ensures a standardized, visible, and accessible configuration for all users.
2.4. Data Collection and Measurement
Data collection was carried out in two different locations: in a lab at CEU San Pablo University and at its university polyclinic. This approach aimed to increase the sample size and ensure a more diverse participant pool. To standardize the setup across locations and minimize environmental variability, a 2 × 2 m area was marked on the floor at both sites. The VR base stations were placed in opposite corners of this area (front-left and back-right) to maximize motion capture coverage and ensure consistent tracking of head and neck movements across all participants (see Figure 3).

Figure 3.
The image depicts a user performing the apple-harvesting task in the VE. The user is wearing an HMD and holding controllers within the designated measurement area, a 2 × 2 m open space. This area was physically marked at the measurement site. In the corner, one of the base stations can be seen, enabling precise tracking within the environment.
All participants provided their informed consent prior to the assessment. Subsequently, they completed a Visual Analogue Scale (VAS) questionnaire to assess pain levels [43]. VAS is a validated tool for assessing both acute and chronic pain. Participants indicate their pain intensity by placing a handwritten mark on a 10-centimeter line, which represents a continuum ranging from “no pain” to “worst pain imaginable”. This method allows for a nuanced representation of pain levels, capturing the subjective experience of pain in a straightforward and effective manner. The information gathered from this questionnaire was used to classify participants into the appropriate study groups based on their reported neck pain at the time of measurement.
Before placing the HMD on the participant, a brief explanation of the task was provided. Participants were informed that they would be required to collect apples using the VR controllers and that the grip button on either hand should be used to grab each apple. No time constraints or speed-related goals were given, and participants were instructed to perform the task at their own pace and to move freely within the environment to reach the apples. The game mechanics appeared to be intuitive and engaging, allowing participants to complete the task without requiring additional instructions [47]. This ensured that movements performed during the task were as natural as possible, facilitating the assessment of functional Cervical ROM.
The HTC Vive Pro Eye™ continuously recorded head position and orientation during the task, capturing movements across the three CROM axes (see Figure 1). Headset and hand positions and rotations were tracked and saved at a sampling frequency of 50 Hz. The system uses Valve’s SteamVR™ Lighthouse technology. The Lighthouse base stations emit structured infrared signals and sweeping laser beams, which are detected by photodiodes embedded on the surface of the HMD, controllers, and, when available, additional trackers. The timing differences in laser detection across photodiodes allow the system to calculate the position and orientation of the HMD and controllers in space, providing six degrees of freedom (three translational and three rotational). Additionally, the timestamps of when the apples are picked up and placed in the basket were also recorded for later analysis. To maintain consistency, the system was calibrated before each session, setting a neutral head position as the baseline reference. By allowing continuous motion recording throughout the task, this approach eliminated the need for manual readings or static postures [33], providing a more realistic and functional evaluation of cervical mobility.
The recorded sessions, encompassing the entirety of each evaluation, were stored in 60 CSV files [48]. These are divided into two groups: “Group A” for asymptomatic participants and “Group B” for participants experiencing neck pain. Each file has a variable length, reflecting the differing durations of the session of each subject, and contains the following data elements: sample index, timestamp, device identifier (denoted as “H” for the Head-Mounted Display (HMD), “L” for the left controller, and “R” for the right controller), three-dimensional spatial coordinates in meters (designated as “X”, “Y”, “Z”), rotation quaternion components (“qX”, “qY”, “qZ”, “qW”), and corresponding Euler angles for orientation (“x”, “y”, “z”). Furthermore, the instantiation and collection of virtual apples within the simulation were logged in this format: sample index, timestamp, and apple event (indicated as either “spawned” or “stored”, along with a numerical identifier ranging from 0 to 15). All data processing was performed using MATLAB™ R2023b. A GitHub® repository containing the raw data from the 60 participants in the study, as well as the code to analyze the data, can be found at [48].
2.5. Spectral Analysis
The objective of spectral analysis is to quantify the number of slower, smoother movements and faster, more abrupt movements that each subject performs during the apple-harvesting task. Our hypothesis is that subjects with neck pain will perform slower movements than healthy subjects. To quantify the number of slow movements, spectral power will be calculated in the [0, 0.1] band, and for fast movements, spectral power will be calculated in the [0.1, 0.5] band. These two spectral power bands fall within the frequency ranges clearly associated with voluntary motor control [49]. Movements occurring outside the subjects’ voluntary motor control will also be quantified by calculating the spectral power in the [0.5, 5] band [50]. All these calculations will be performed for each of the three planes of motion (frontal, transverse, and sagittal planes), as well as for the total three-dimensional movement. The detailed methodology for these calculations is explained below.
The data from the HMD and the apple positions were extracted from the CSV files. To prevent the time series of angles from containing fluctuations between and degrees, which correspond to small movements around that position, a wrap angle function was applied such that mapped to and also mapped to . Based on the angle of rotation in each plane, the magnitude of the three-dimensional head rotation was also computed for each subject.
For each recording, four spectrograms were computed: one for the movement in each plane and one for the total movement. A spectrogram depicts the frequency spectrum of a signal over time, with three axes: time, frequency, and magnitude (or power) at specific time-frequency points, calculated using the Short-Time Fourier Transform (STFT). Prior to spectrogram computation, the mean value was subtracted from each time series. To calculate the spectrogram, the signal was segmented into 512-sample sections (approximately 10 s in duration). A Hamming window function was applied to each of these segments. Subsequently, the Fast Fourier Transform (FFT) was calculated for each windowed section, thus obtaining the frequency content of that portion of the signal. This process was repeated throughout the entire signal, shifting the window by 128 samples at each step (approximately 2.5 s), which corresponds to a 384-sample overlap between consecutive segments. The result is a representation of how the signal’s power spectral density varies in time and frequency. To obtain the spectral power in each band, the average of the absolute value of the spectrogram’s spectral components falling within each band’s ranges was calculated.
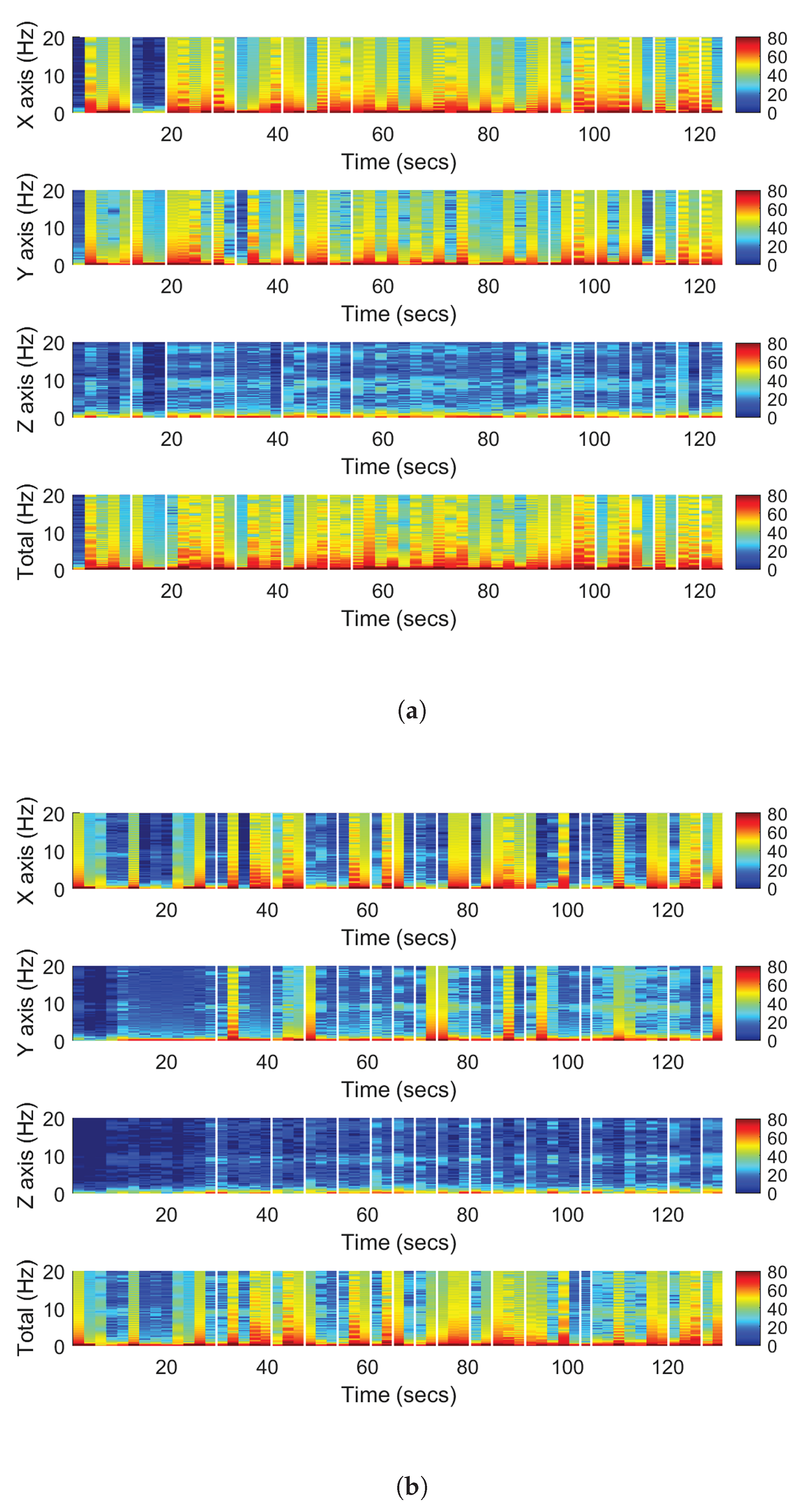
A custom function, “CustomPlotSpectrogram”, was developed to visualize the results in a 2D top-down view, with color limits set between −10 and 90 decibels to facilitate magnitude comparisons across subjects [48]. By default, MATLAB™ adjusts the color scale used in spectrogram visualization based on the minimum and maximum power values present in that spectrogram. This prevents direct visual comparisons between two spectrograms. Our custom function fixes these limits to constant values for all spectrograms of all subjects, thus allowing the comparison of spectrograms from different subjects. The custom function also adds white vertical lines to mark the moments when apples were stored. As explained in the previous section, the log generated by the virtual reality application includes “apple stored” events, along with a timestamp indicating when each event occurred. This timestamp is used to draw the white vertical lines on the spectrogram’s temporal axis to mark the moments when apples were stored. Figure 4 shows the spectrograms of a healthy subject and of a pain-affected subject. The axes units are time (seconds), frequency (Hz), and magnitude (dB/Hz).
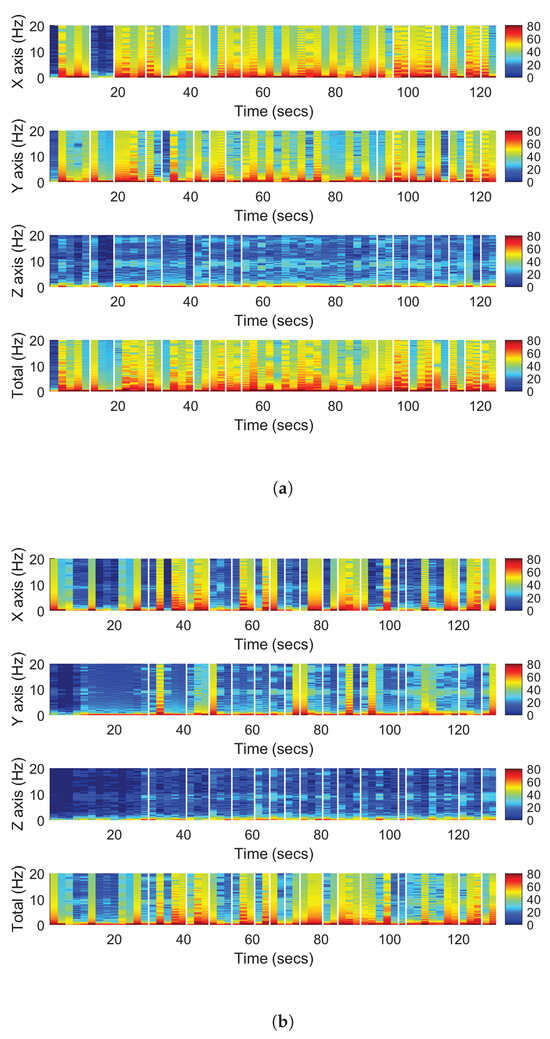
Figure 4.
(a) The spectrogram of a healthy subject. (b) The spectrogram of a pain-affected subject. The vertical white lines correspond to the moments when apples are stored. The spectrograms show more power in the higher spectral components in the patients without neck pain.
2.6. Statistical Analysis
A statistical analysis was performed to characterize and quantify the variations in spectral power derived from the spectrogram data. From the spectrograms, the average spectral power for each subject was computed for three distinct frequency bands. The first band, spanning [0, 0.1] Hz, corresponds to relatively slow movements. The second band encompasses the range [0.1, 0.5] Hz, including rapid movements. These two frequency bands correspond to voluntary movements under the conscious control of the subject [49]. The third band extends from [0.5, 5] Hz and includes high-frequency movements outside the domain of voluntary postural control [50]. The initial 30 s of each spectrogram were excluded to mitigate the influence of quiescent periods, as these segments likely represent the participants’ acclimation phase to the virtual reality environment and do not accurately reflect their natural movement kinematics. In Figure 4 it can be seen how at the beginning of the task, in all planes of movement and in the total movement, there is a greater prevalence of low frequencies (blue color) than for the rest of the task for both the subject with pain and the subject without pain.
To ascertain the presence of statistically significant differences in average spectral power between the two groups across the various frequency bands, a statistical analysis was conducted. First, the assumption of normality for the spectral power data within each group and for each frequency band was assessed using the Anderson–Darling test. This test was chosen for its sensitivity in detecting deviations from normality, particularly at the tails of the distribution. The null hypothesis for this test is that the data follow a normal distribution. If the Anderson–Darling test indicated that the data from both groups for a given frequency band were normally distributed, an independent-sample t-test was employed. Conversely, if the data in one or both groups for a given frequency band significantly deviated from a normal distribution, the non-parametric Mann–Whitney U test was utilized.
This methodology was applied to each of the three frequency bands for each of the four time series of head rotation (rotation in each of the three planes and total rotation). This involves the application of a total of 12 statistical tests. To mitigate the risk of spurious findings arising from multiple statistical comparisons, the False Discovery Rate (FDR) correction was applied to the resultant p-values obtained across all statistical tests [51]. This correction ranks the p-values in ascending order and then compares each p-value to a critical value that depends on its rank and the total number of tests. This method controls the expected proportion of significant results that are false positives, providing a set of FDR-adjusted p-values. This approach ensures greater validity and reliability of the findings, particularly in exploratory analyses involving numerous comparisons, as is the case of the analysis presented in this study.
The same procedure of normality testing and hypothesis evaluation was applied to the analysis of recording duration, to test for statistically significant differences in the time required by the subjects with and without pain to complete the apple-harvesting task.
2.7. System’s Usability
To evaluate the usability of the VR experience, the Spanish version of the System Usability Scale (SUS) was employed [52]. This tool provides a straightforward method for users and researchers to evaluate usability, generating a single, easily interpretable score [53].
The SUS consists of ten alternating positive and negative statements, which participants rate from 1 (“Strongly Disagree”) to 5 (“Strongly Agree”). The scores are calculated by adjusting the ratings for odd-numbered (positive) and even-numbered (negative) items, resulting in a total score ranging from 0 to 40. This total is then multiplied by 2.5 to create a scale from 0 to 100 [54]. A score between 68 and 84 indicates acceptable usability, while scores above 85 reflect excellent usability [52]. After completing the apple-harvesting task, participants anonymously filled out the SUS questionnaire to provide feedback on their VR experience.
3. Results
Table 1 shows the demographic characteristics of the participants in Groups A and B, with a total of 60 individuals included in the study. Group A consists of 14 women with an average age of years, a height of cm, and a weight of kg, alongside 16 men with a mean age of years, a height of cm, and a weight of kg. Group B comprises 21 women with a mean age of years, a height of cm, and a weight of kg, along with 9 men averaging years of age, cm in height, and kg in weight.

Table 1.
Demographic characteristics of participants in Groups A and B.
Table 2 shows the average spectral power for the 30 subjects without neck pain, for each of the three frequency bands, for each of the three planes of motion, and for the total movement. Table 3 shows the same information for the 30 subjects suffering from neck pain. The p-values of the statistical comparisons, after applying the FDR correction, can be found in Table 4.
Table 2.
Average spectral power and standard deviation for subjects without neck pain.
Table 3.
Average spectral power and standard deviation for subjects with neck pain.
Table 4.
Corrected p-values (using FDR) for each spectral band from the statistical tests assessing differences in average spectral power between subjects with neck pain and subjects without neck pain.
The p-values presented in Table 4 indicate statistically significant differences in spectral power for the [0.1, 0.5] Hz band along the y-axis and the z-axis, as well as for total movement (p = 0.0384 in all the cases). These findings reveal that movements within this frequency range differ significantly between subjects with and without pain. No statistically significant differences were observed for any of the movement planes or for the total movement within the [0, 0.1] Hz and [0.5, 5] Hz frequency bands.
The average time to accomplish the task for subjects with neck pain was seconds compared to () seconds for those without pain. The Mann–Whitney U test indicated a statistically significant difference in task duration (p-value of 0.039) between the groups.
The usability assessment using the SUS yielded an overall score of , indicating a high level of user satisfaction with the virtual reality system used for the apple-harvesting task. This score falls between acceptable and excellent usability, suggesting that participants found the system intuitive and effective [52].
To study the possible influence of age on the usability of the virtual reality system, participants were divided into three age groups: young adults (18–25 years, n = 26), adults (26–45 years, n = 20), and individuals in later adulthood (46–65 years, n = 14). The normality assessment test indicated that the SUS score did not follow a normal distribution in all groups. Therefore, the non-parametric Kruskal–Wallis test was used to compare the medians of the SUS score between groups. The results indicated that there were no significant differences (p-value = 0.903). The means and standard deviations of the SUS scores were 84.1 ± 10.6 for the young group, 83.4 ± 9.7 for the adult group, and 85.5 ± 7.7 for the older group. These results indicate that the usability of the virtual reality experience is not affected by the user’s age.
4. Discussion and Conclusions
The results of this study show that subjects with chronic neck pain exhibit consistently lower average spectral power in the [0.1, 0.5] Hz band for the y (transverse plane) and z (frontal plane) planes of motion and for the total movement when compared to asymptomatic controls (see Table 2 and Table 3). These findings indicate that subjects without neck pain perform faster head movements in the frontal and transverse planes when performing a whole-body functional task. However, such a difference between groups was not observed for the sagittal plane. Table 2 and Table 3 also show that the average spectral power in the [0, 0.1] Hz band is higher in subjects with neck pain for each of the three planes of motion compared to subjects without neck pain; however, these differences are not statistically significant (see Table 4). One interpretation of these data could be that subjects with neck pain, when rotating their heads to locate apples in the virtual trees, tend to do so more slowly than subjects without neck pain due to the pain they experience or the fear that the movement will induce pain.
The reduced head velocity seems to be aligned with previous evidence that has suggested that people with neck pain may have a slower head kinematics compared to asymptomatic individuals during functional movements [42]. However, there is little research analyzing functional tasks in individuals with neck pain that we could compare with our results. Moreover, to the best of our knowledge, there are no studies that share the same method of an immersive VR experience specifically designed for analyzing head kinematics during the performance of a complex whole-body functional task. Previous studies in the field have included analysis of neck or head motion during tasks such as walking [55], a typing task in sitting position [56], a VR game focused on isolated neck movements [57], or the task of transferring a weight with the upper limb [25].
The [0.5, 5] Hz frequency band captures very rapid movements outside the range of voluntary motor control. In this band, participants without neck pain again exhibit greater spectral power in the three planes of motion and in total movement, but these differences are not statistically significant (see Table 4). The meaning of this power band is difficult to interpret; however, a potential cause for these very rapid movements could be oscillations of the HMD due to a non-perfect fixation to the user’s head. The HTC Vive Pro Eye™ is a relatively bulkier HMD, weighing 800 g with a somewhat uneven weight distribution, being significantly front-heavy. This can induce a high torque during the subject’s rotational movements, potentially causing the HMD to continue rotating when the subject stops turning their neck in one direction [58]. The high torque caused by the weight and uneven weight distribution may lead to the HMD slipping relative to the subject’s cranium, rotating more than the cranium, and subsequently returning to the original position due to the HMD’s straps, causing vibrations and high-frequency movements. The fact that participants without neck pain exhibit faster movements (see Table 2 and Table 3) would make this effect more pronounced in this group.
Subjects with neck pain required more time to collect the 16 apples in the virtual reality experience than subjects without neck pain ( s vs s), and this difference was statistically significant. This finding further suggests a greater slowness in the movements of subjects with neck pain and at the same time reflects a lower performance in the task of these subjects.
Regarding system usability, the SUS score obtained indicates that the experience is simple and intuitive. None of the subjects who used the experience reported adverse effects. This suggests that this virtual reality experience could be employed in the assessment of neck functional status without the need for assistance from a technician or a health professional. This could open doors to the use of the experience from a patient’s home, allowing for remote assessment sessions as part of a virtual reality-based telerehabilitation program that integrates rehabilitation exercises and evaluation sessions for status monitoring and for adapting the rehabilitation exercises [59].
Currently, the evaluation of neck functional status is primarily based on the measurement of maximum ROM in the different planes. This assessment has little relation to the impact on a patient’s ADLs [35,36,37], hence the interest in conducting assessments based on the quantification of metrics during the performance of ADLs, as proposed in this work. Although other studies have attempted to assess the neck during ADLs, these studies have used manual measurements that required the subject to stop at a point during task performance [33] or have employed electrogoniometers and torsiometers [35], which are more complex to use than a VR setup and require the use of physical objects and environments for patient assessment. The use of a VR experience allows for the simulation of these environments and objects, enabling activities (such as harvesting apples) that would not be feasible in a clinical setting or the patient’s home. Furthermore, the use of VR provides an immersive and engaging environment that favors patient adherence to the treatment [60,61]. Although the current study included healthy individuals and participants with neck pain, the apple-harvesting task may be adapted for more impaired populations—such as frail older adults or individuals recovering from surgery—by modifying parameters like the location of the apples, required range of motion, or task duration. Future studies should explore the feasibility and usability of the system in these populations.
In this work, the spectral analysis has been proposed as a tool to assess kinematic differences between subjects with and without pain. This is based on the researchers’ hypothesis that neck pain will influence movement smoothness, and thus acceleration, more than other metrics like velocity or range of motion. Nevertheless, it would be interesting to analyze in the future whether other types of metrics, different from spectral analysis, allow for a better functional assessment of the subjects.
The main limitation of the present study is the lack of quantification of compensatory movements performed with the trunk or the whole body [12]. It is possible that if compensatory movements had been captured and if the actual neck movement had been calculated by subtracting trunk rotation data from neck rotation data, there would have been more relevant differences in the spectral bands or more pronounced differences. In a future study, we intend to replicate the present study, employing a tracker on the subject’s back to be able to analyze these compensatory movements. Furthermore, the differences in head kinematics between populations were analyzed through a cross-sectional study, so no inferences could be made in terms of causality. Future longitudinal research could provide more evidence on the possible causal direction of the relationship between head kinematics and the occurrence of the symptoms of neck pain.
Author Contributions
Conceptualization, R.G.-C., A.O. and A.M.-P.-Z.; methodology, R.G.-C., A.O. and A.M.-P.-Z.; software, Á.S.-P.; investigation, J.A.S.-P., E.B.-C. and F.M.; resources, R.G.-C. and A.O.; data curation, J.A.S.-P.; writing—original draft preparation, J.A.S.-P., R.G.-C. and A.O.; writing—review and editing, all the authors; supervision, R.G.-C. and A.O.; project administration, R.G.-C. and A.O.; funding acquisition, R.G.-C., A.O. and A.M.-P.-Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Spanish Ministry of Science, Innovation, and University under the grant European Regional Development Fund (ERDF), with project references IDI-20191120 and PID2021-127096OB-I00.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (Ethics Committee) of the University San Pablo CEU (approval code: 495/21/39 on 22 March 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data and code supporting the results of this study are available at the following link: https://github.com/AbrahamOtero/FunctionalAssessmentOfTheNeck, accessed on 28 April 2025.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 6DoF | six degrees of freedom |
| ADLs | activities of daily living |
| CROM | Cervical Range of Motion |
| CSV | comma-separated value |
| ERDF | European Regional Development Fund |
| FDR | False Discovery Rate |
| FFT | Fast Fourier Transform |
| HMD | Head-Mounted Display |
| ICC | Intraclass Correlation Coefficient |
| IMUs | inertial measurement units |
| NPC | non-player character |
| QoL | quality of life |
| ROM | range of motion |
| STFT | Short-Time Fourier Transform |
| SUS | System Usability Scale |
| VAS | Visual Analogue Scale |
| VE | virtual environment |
| VR | virtual reality |
| VRTK | Virtual Reality ToolKit |
| YLDs | years lived with disability |
References
- World Health Organization. Musculoskeletal Conditions. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 28 April 2025).
- Disease, G.; Incidence, I.; Collaborators, P. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858, Erratum in: Lancet 2019, 393, e44. https://doi.org/10.1016/S0140-6736(19)31047-5. [Google Scholar] [CrossRef]
- Wu, H.; Li, Y.; Zou, C.; Guo, W.; Han, F.; Huang, G.; Sun, L. Global burden of neck pain and its gender and regional inequalities from 1990–2021: A comprehensive analysis from the Global Burden of Disease Study 2021. BMC Musculoskelet. Disord. 2025, 26, 94. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Neck Pain Collaborators. Global, regional, and national burden of neck pain, 1990–2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2024, 6, e142–e155. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Barendregt, J.; Blore, J.; Murray, C.; et al. The global burden of neck pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef]
- Hogg-Johnson, S.; van der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E.; et al. The burden and determinants of neck pain in the general population: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J. Manip. Physiol. Ther. 2009, 32, S46–S60. [Google Scholar] [CrossRef]
- Cohen, S.P. Epidemiology, diagnosis, and treatment of neck pain. Mayo Clin. Proc. 2015, 90, 284–299. [Google Scholar] [CrossRef]
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.; Kolahi, A.A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 26. [Google Scholar] [CrossRef]
- Sarig-Bahat, H.; Weiss, P.L.; Laufer, Y. Neck pain assessment in a virtual environment. Spine 2010, 35, E105–E112. [Google Scholar] [CrossRef]
- Mareş, S.; Deaconescu, A.; Deaconescu, T. Pneumatically Actuated Rehabilitation Equipment for the Sagittal and Frontal Plane Movements of the Neck Joint. Technologies 2025, 13, 39. [Google Scholar] [CrossRef]
- Stenneberg, M.S.; Rood, M.; de Bie, R.; Schmitt, M.A.; Cattrysse, E.; Scholten-Peeters, G.G. To what degree does active cervical range of motion differ between patients with neck pain, patients with whiplash, and those without neck pain? A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2017, 98, 1407–1434. [Google Scholar] [CrossRef]
- Van der Kruk, E.; Silverman, A.K.; Koizia, L.; Reilly, P.; Fertleman, M.; Bull, A.M.J. Age-related compensation: Neuromusculoskeletal capacity, reserve & movement objectives. J. Biomech. 2021, 122, 110385. [Google Scholar] [CrossRef]
- Swinkels, R.A.; Swinkels-Meewisse, I.E. Normal values for cervical range of motion. Spine 2014, 39, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.; Marsh, D.; Koller, H.; Zenenr, J.; Bannister, G. Cervical range of movement in relation to neck dimension. Eur. Spine J. 2009, 18, 863–868. [Google Scholar] [CrossRef]
- Williams, M.A.; McCarthy, C.J.; Chorti, A.; Cooke, M.W.; Gates, S. A systematic review of reliability and validity studies of methods for measuring active and passive cervical range of motion. J. Manip. Physiol. Ther. 2010, 33, 138–155. [Google Scholar] [CrossRef]
- Luedtke, K.; Schoettker-Königer, T.; Hall, T.; Enns, C.; Grassold, M.; Hasselhoff-Styhler, P.; Reimer, C. Concurrent validity and reliability of measuring range of motion during the cervical flexion rotation test with a novel digital goniometer. BMC Musculoskelet. Disord. 2020, 21, 535. [Google Scholar] [CrossRef]
- Ghorbani, F.; Kamyab, M.; Azadinia, F. Smartphone applications as a suitable alternative to CROM device and inclinometers in assessing the cervical range of motion in patients with nonspecific neck pain. J. Chiropr. Med. 2020, 19, 38–48. [Google Scholar] [CrossRef]
- Prushansky, T.; Deryi, O.; Jabarreen, B. Reproducibility and validity of digital inclinometry for measuring cervical range of motion in normal subjects. Physiother. Res. Int. 2010, 15, 42–48. [Google Scholar] [CrossRef]
- Chalimourdas, A.; Dimitriadis, Z.; Kapreli, E.; Strimpakos, N. Test-re-test reliability and concurrent validity of cervical active range of motion in young asymptomatic adults using a new inertial measurement unit device. Expert Rev. Med. Devices 2021, 18, 1029–1037. [Google Scholar] [CrossRef]
- Raya, R.; Garcia-Carmona, R.; Sanchez, C.; Urendes, E.; Ramirez, O.; Martin, A.; Otero, A. An inexpensive and easy to use cervical range of motion measurement solution using inertial sensors. Sensors 2018, 18, 2582. [Google Scholar] [CrossRef]
- Feng, M.; Liang, L.; Sun, W.; Liu, G.W.; Yin, X.; Han, T.; Wei, X.; Zhu, L. Measurements of cervical range of motion using an optical motion capture system: Repeatability and validity. Exp. Ther. Med. 2019, 18, 4193–4202. [Google Scholar] [CrossRef]
- Oliveira-Souza, A.I.S.; Carvalho, G.F.; Florêncio, L.L.; Fernández-de Las-Peñas, C.; Dach, F.; Bevilaqua-Grossi, D. Intrarater and interrater reliability of the flexion rotation test and cervical range of motion in people with migraine. J. Manip. Physiol. Ther. 2020, 43, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Wolan-Nieroda, A.; Guzik, A.; Mocur, P.; Druzbicki, M.; Maciejczak, A. Assessment of Interrater and Intrarater Reliability of Cervical Range of Motion (CROM) goniometer. BioMed Res. Int. 2020, 2020, 8908035. [Google Scholar] [CrossRef] [PubMed]
- Lutke Schipholt, I.J.; Scholten-Peeters, G.G.M.; Logghe, S.; Koop, M.; Donders, S.; Stenneberg, M.S.; Coppieters, M.W. The CROM-VAS Test: A novel and reliable clinical test to assess immediate pain relief following treatment for movement-evoked neck pain. Musculoskelet. Sci. Pract. 2024, 74, 103191. [Google Scholar] [CrossRef] [PubMed]
- Tsang, S.M.; Szeto, G.P.; Lee, R.Y. Altered spinal kinematics and muscle recruitment pattern of the cervical and thoracic spine in people with chronic neck pain during functional task. J. Electromyogr. Kinesiol. 2014, 24, 104–113. [Google Scholar] [CrossRef]
- Law, E.Y.; Chiu, T.T. Measurement of cervical range of motion (CROM) by electronic CROM goniometer: A test of reliability and validity. J. Back Musculoskelet. Rehabil. 2013, 26, 141–148. [Google Scholar] [CrossRef]
- Janjua, M.B.; Zhou, P.L.; Vasquez-Montes, D.; Moskovich, R. Photogrammetric analysis: An objective measure to assess the craniocervical range of motion after cervical laminoplasty surgeries. J. Clin. Neurosci. 2020, 71, 76–83. [Google Scholar] [CrossRef]
- Rousseau, M.A.; Laporte, S.; Chavary-Bernier, E.; Lazennec, J.Y.; Skalli, W. Reproducibility of measuring the shape and three-dimensional position of cervical vertebrae in upright position using the EOS stereoradiography system. Spine 2007, 32, 2569–2572. [Google Scholar] [CrossRef]
- Kiper, P.; Baba, A.; Alhelou, M.; Pregnolato, G.; Maistrello, L.; Agostini, M.; Turolla, A. Assessment of the cervical spine mobility by immersive and nonimmersive virtual reality. J. Electromyogr. Kinesiol. 2020, 51, 102397. [Google Scholar] [CrossRef]
- Xu, X.; Chen, K.B.; Lin, J.H.; Radwin, R.G. The accuracy of the Oculus Rift virtual reality head-mounted display during cervical spine mobility measurement. J. Biomech. 2015, 48, 721–724. [Google Scholar] [CrossRef]
- Santos-Paz, J.A.; Sánchez-Picot, Á.; Rojo, A.; Martín-Pintado-Zugasti, A.; Otero, A.; Garcia-Carmona, R. A novel virtual reality application for autonomous assessment of cervical range of motion: Development and reliability study. PeerJ 2022, 10, e14031. [Google Scholar] [CrossRef]
- De Loose, V.; Van den Oord, M.; Burnotte, F.; Van Tiggelen, D.; Stevens, V.; Cagnie, B.; Danneels, L.; Witvrouw, E. Functional assessment of the cervical spine in F-16 pilots with and without neck pain. Aviat. Space Environ. Med. 2009, 80, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.E.; Schenk, R.J.; Simmons, E.D. Active Range of Motion Utilized in the Cervical Spine to Perform Daily Functional Tasks. J. Spinal Disord. Tech. 2002, 15, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Janczyk, R.; Janczyk, M.; Sibiński, M.; Drobniewski, M. Functional assessment and evaluation of health problems with the cervical spine among dental assistants and hygienists. PostęPy Psychiatr. Neurol. 2023, 32, 68–75. [Google Scholar] [CrossRef]
- Bible, J.E.; Biswas, D.; Miller, C.P.; Whang, P.G.; Grauer, J.N. Normal functional range of motion of the cervical spine during 15 activities of daily living. J. Spinal Disord. Tech. 2010, 23, 15–21. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Slater, M.; Sanchez-Vives, M.V. Impact of virtual embodiment and exercises on functional ability and range of motion in orthopedic rehabilitation. Sci. Rep. 2022, 12, 5046. [Google Scholar] [CrossRef]
- Flores-Cortes, M.; Guerra-Armas, J.; Pineda-Galan, C.; La Touche, R.; Luque-Suarez, A. Sensorimotor uncertainty of immersive virtual reality environments for people in pain: Scoping review. Brain Sci. 2023, 13, 1461. [Google Scholar] [CrossRef]
- Lim, C.H.; Lee, S.C. The Effects of Degrees of Freedom and Field of View on Motion Sickness in a Virtual Reality Context. Int. J. Hum.-Comput. Interact. 2023, 40, 5884–5896. [Google Scholar] [CrossRef]
- Guo, Q.; Zhang, L.; Han, L.; Gui, C.; Chen, G.; Ling, C.; Wang, W.; Gao, Q. Effects of Virtual Reality Therapy Combined With Conventional Rehabilitation on Pain, Kinematic Function, and Disability in Patients With Chronic Neck Pain: Randomized Controlled Trial. JMIR Serious Games 2024, 12, e42829. [Google Scholar] [CrossRef]
- Nusser, M.; Kramer, M.; Knapp, S.; Krischak, G. Effects of virtual reality-based neck-specific sensorimotor training in patients with chronic neck pain compared with general sensorimotor training and a standard rehabilitation programme: A randomized controlled pilot trial. J. Rehabil. Med. 2021, 53, jrm00151. [Google Scholar] [CrossRef]
- Trinidad-Fernández, M.; Bossavit, B.; Salgado-Fernández, J.; Abbate-Chica, S.; Fernández-Leiva, A.J.; Cuesta-Vargas, A.I. Head-Mounted Display for Clinical Evaluation of Neck Movement Validation with Meta Quest 2. Sensors 2023, 23, 3077. [Google Scholar] [CrossRef]
- Moghaddas, D.; de Zoete, R.M.J.; Edwards, S.; Snodgrass, S.J. Differences in the kinematics of the cervical and thoracic spine during functional movement in individuals with or without chronic neck pain: A systematic review. Physiotherapy 2019, 105, 421–433. [Google Scholar] [CrossRef] [PubMed]
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring With a Traditional Paper-based Visual Analog Scale in Adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.M.; Preuper, H.R.S.; Balk, G.A.; Stewart, R.E. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 2014, 155, 2545–2550. [Google Scholar] [CrossRef] [PubMed]
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995, 61, 277–284. [Google Scholar] [CrossRef]
- Quan, W.; Liu, S.; Cao, M.; Zhao, J. A comprehensive review of virtual reality technology for cognitive rehabilitation in patients with neurological conditions. Appl. Sci. 2024, 14, 6285. [Google Scholar] [CrossRef]
- Abbasi, M.; Váz, P.; Silva, J.; Martins, P. Enhancing Visual Perception in Immersive VR and AR Environments: AI-Driven Color and Clarity Adjustments Under Dynamic Lighting Conditions. Technologies 2024, 12, 216. [Google Scholar] [CrossRef]
- Santos-Paz, J.A.; Sánchez-Picot, Á.; Bocos-Corredor, E.; Moggioli, F.; Martín-Pintado-Zugasti, A.; García-Carmona, R.; Otero, A. GitHub Repository Containing the Raw Data from the 60 Participants in the Study, as Well as the Code to Analyze It. 2025. Available online: https://github.com/AbrahamOtero/FunctionalAssessmentOfTheNeck (accessed on 28 April 2025).
- Stensdotter, A.K.; Meisingset, I.; Pedersen, M.D.; Vasseljen, O.; Stavdahl, Ø. Frequency-dependent deficits in head steadiness in patients with nonspecific neck pain. Physiol. Rep. 2019, 7, e14013. [Google Scholar] [CrossRef]
- Gresty, M.A.; Halmagyi, G.M. Abnormal head movements. J. Neurol. Neurosurg. Psychiatry 1979, 42, 705–714. [Google Scholar] [CrossRef]
- Ni, Y.; Seffernick, A.E.; Onar-Thomas, A.; Pounds, S.B. Computing power and sample size for the false discovery rate in multiple applications. Genes 2024, 15, 344. [Google Scholar] [CrossRef]
- Sevilla-Gonzalez, M.D.R.; Moreno Loaeza, L.; Lazaro-Carrera, L.S.; Bourguet Ramirez, B.; Vázquez, R.A.; Peralta-Pedrero, M.L.; Almeda-Valdes, P. Spanish version of the system usability scale for the assessment of electronic tools: Development and validation. JMIR Hum. Factors 2020, 7, e21161. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J.-Hum.-Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A Quick and Dirty Usability Scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., McClelland, I.L., Weerdmeester, B., Eds.; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Falla, D.; Gizzi, L.; Parsa, H.; Dieterich, A.; Petzke, F. People with chronic neck pain walk with a stiffer spine. J. Orthop. Sport. Phys. Ther. 2017, 47, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Szeto, G.P.; Straker, L.M.; O’Sullivan, P.B. A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work—2: Neck and shoulder kinematics. Man. Ther. 2005, 10, 281–291. [Google Scholar] [CrossRef]
- Bahat, H.S.; Weiss, P.L.; Laufer, Y. The effect of neck pain on cervical kinematics, as assessed in a virtual environment. Arch. Phys. Med. Rehabil. 2010, 91, 1884–1890. [Google Scholar] [CrossRef]
- Astrologo, A.N.; Nano, S.; Klemm, E.M.; Shefelbine, S.J.; Dennerlein, J.T. Determining the effects of AR/VR HMD design parameters (mass and inertia) on cervical spine joint torques. Appl. Ergon. 2024, 116, 104183. [Google Scholar] [CrossRef]
- Cerda, I.H.; Therond, A.; Moreau, S.; Studer, K.; Donjow, A.R.; Crowther, J.E.; Mazzolenis, M.E.; Lang, M.; Tolba, R.; Gilligan, C.; et al. Telehealth and Virtual Reality Technologies in Chronic Pain Management: A Narrative Review. Curr. Pain Headache Rep. 2024, 28, 83–94. [Google Scholar] [CrossRef]
- Stasolla, F.; Passaro, A.; Curcio, E.; Di Gioia, M.; Zullo, A.; Dragone, M.; Martini, E. Combined deep and reinforcement learning with gaming to promote healthcare in neurodevelopmental disorders: A new hypothesis. Front. Hum. Neurosci. 2025, 19, 1557826. [Google Scholar] [CrossRef]
- Alazba, A.; Al-Khalifa, H.; AlSobayel, H. RabbitRun: An immersive virtual reality game for promoting physical activities among people with low back pain. Technologies 2018, 7, 2. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).