
NikshayChain: A Blockchain-Based Proposal for Tuberculosis Data Management in India




Abstract
1. Introduction
1.1. Related Works and Main Contributions
- Discussion and analysis of the working of Nikshay Poshan Yojana, the responsibilities and challenges faced by different stakeholders, and the data management issues associated with this novel scheme.
- Proposing a method based on blockchain for smart healthcare and understanding how a blockchain-based architecture can help build patient-centric and efficient data-sharing with a specific example of the TB scheme.
- Proposing the architecture for implementing the blockchain-based model for the NPY scheme, which can be extended to any public health scheme.
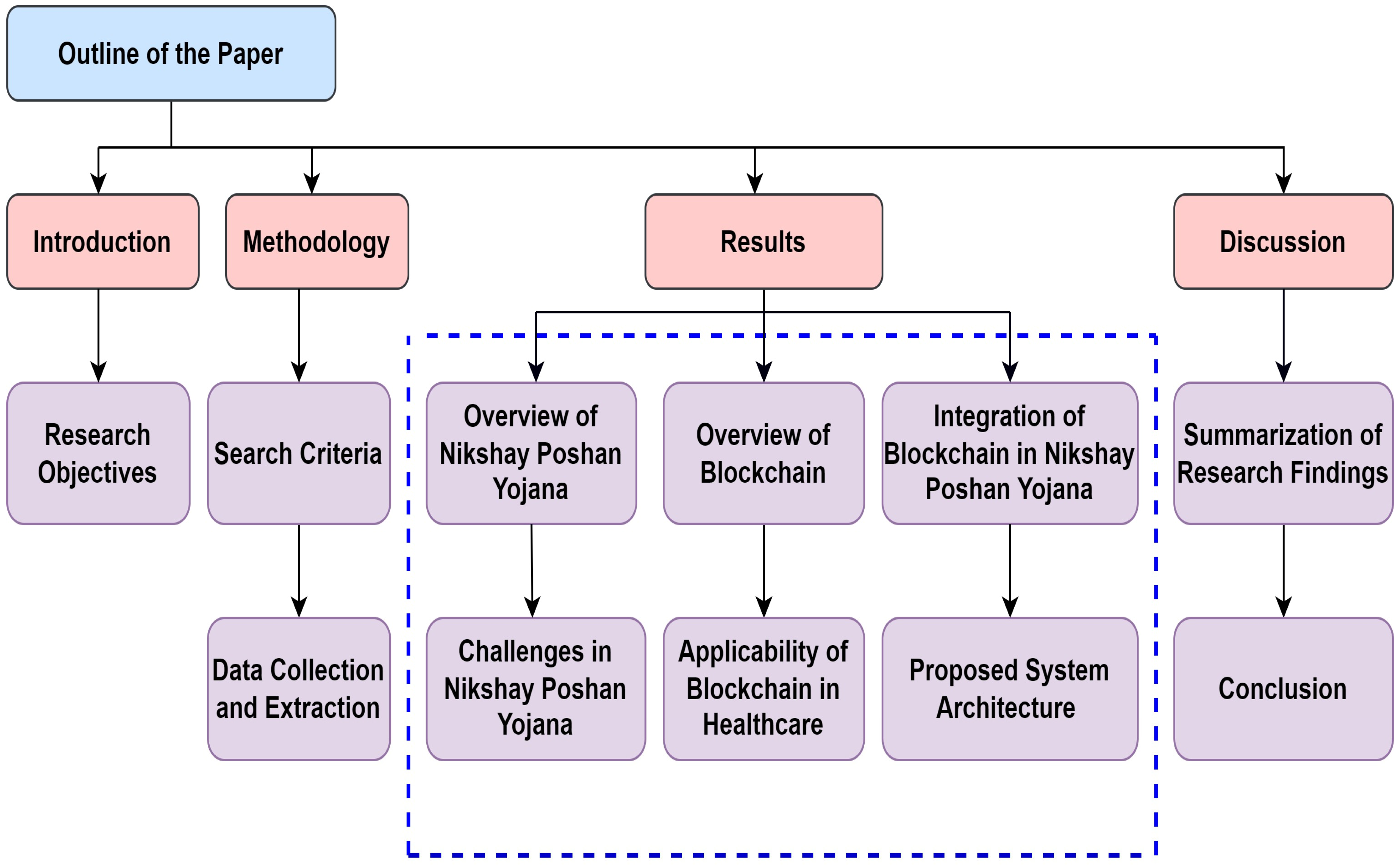
1.2. The Paper Organization
2. Materials and Methods
2.1. Search Criteria
2.2. Data Collection and Extraction
3. The Proposed Blockchain-Based NPY System
3.1. Nikshay Poshan Yojana (NPY)
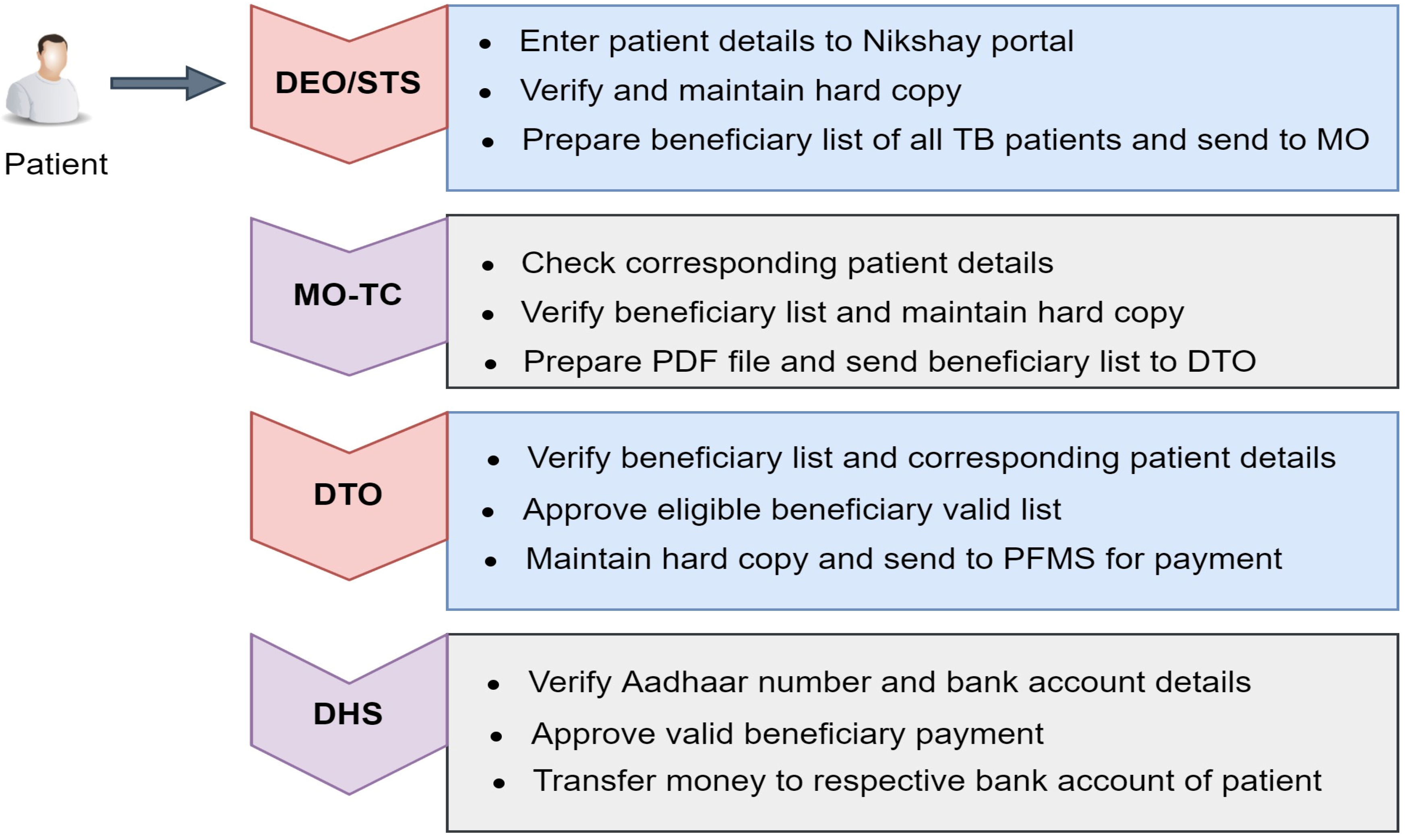
3.1.1. Stakeholders Involved in NPY Scheme
3.1.2. Role and Responsibility of Stakeholders
- Data Entry Operator (DEO):
- Senior TB Supervisor (STS):
- Medical Officer-TB Control (MO-TC):
- District TB Officer (DTO):
- State TB Officer (STO):
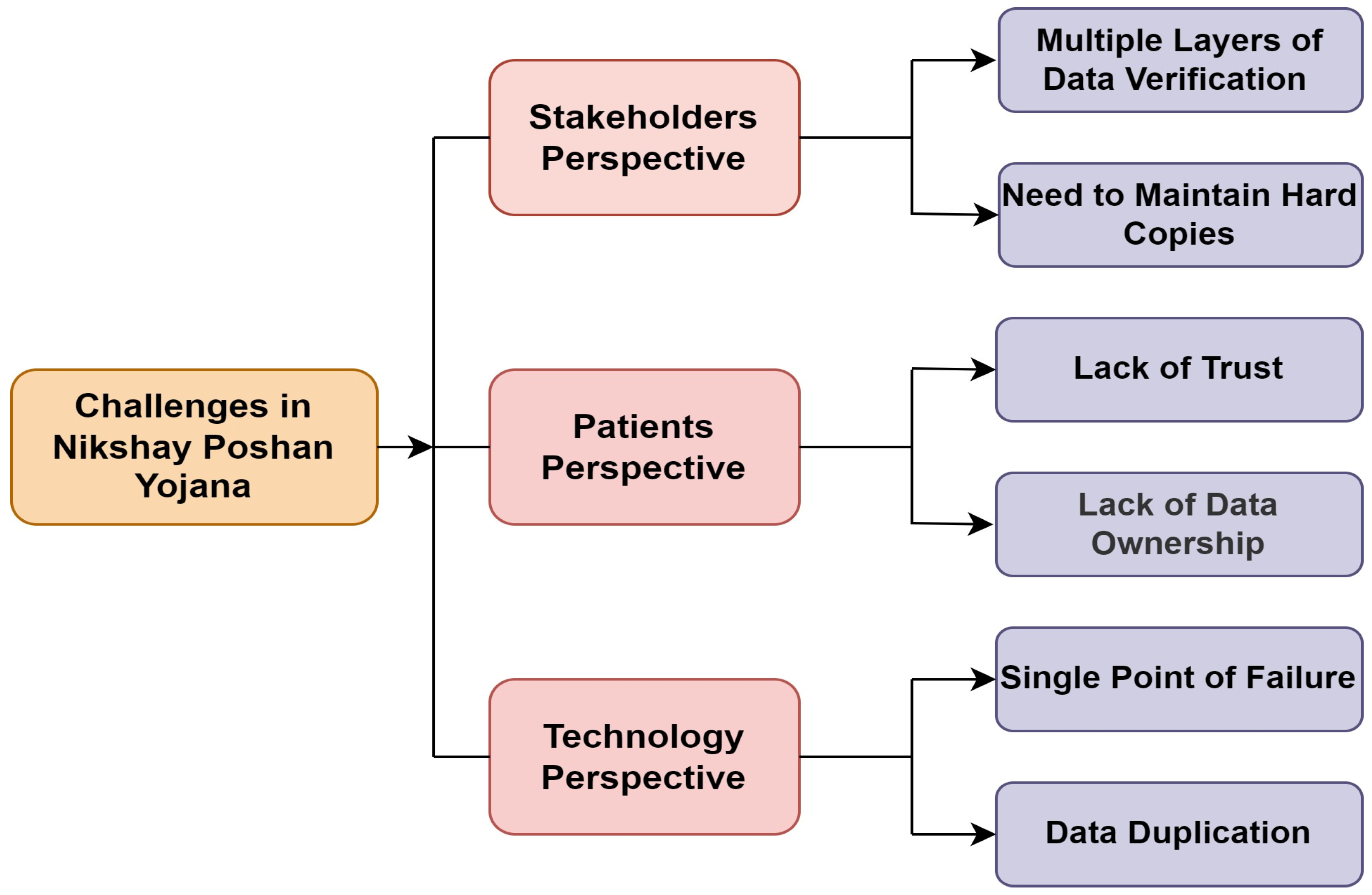
3.2. Challenges in the NPY Scheme
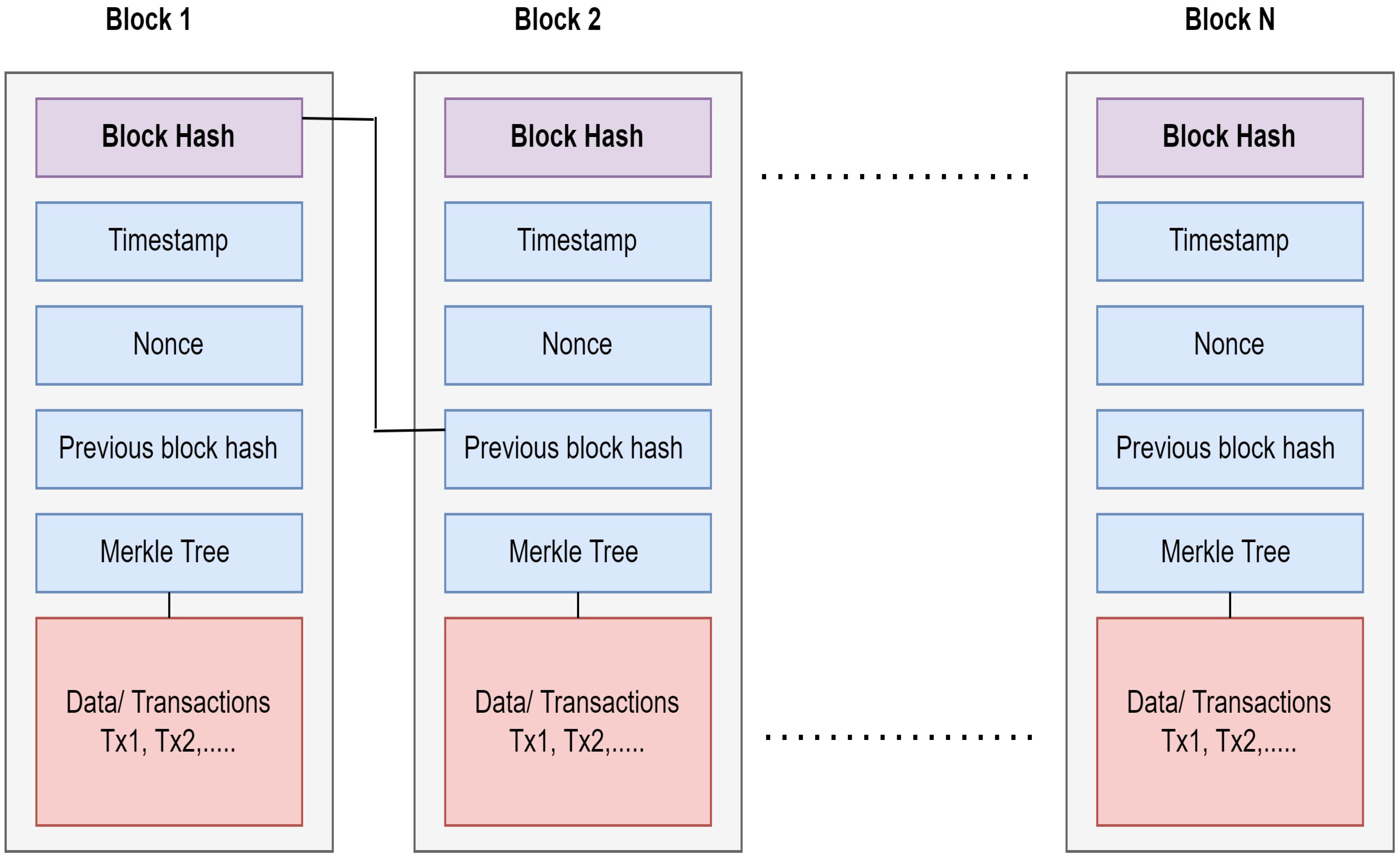
3.3. Overview of Blockchain in Healthcare Scenario
Key Features of Blockchain
- Decentralize: Most healthcare systems rely on centralized repositories to store sensitive medical data. The main issue with a centralized repository is a single point of failure that can destroy the entire network. In such cases, the decentralized nature of blockchain helps overcome the problem of a single point of failure.
- Immutable: When a transaction is validated and recorded on the blockchain, it becomes impossible to change this validated data. Thus, it helps to record immutable agreements between various untrusted nodes and enhances business growth, ensuring data quality and integrity.
- Trust and Transparency: Blockchain network is trustworthy. It uses consensus mechanisms and cryptography techniques to store data in the network. The consent of the majority of participating nodes is needed to keep data in the network. Blockchain develops transparency and trust among participating healthcare stakeholders to share patient-sensitive medical data with these two mechanisms.
- Eliminating Middleman: Blockchain has great potential to overcome the need for intermediaries. Smart contracts enable different stakeholders to communicate and transact directly on a peer-to-peer basis [27].
- Smart Contract Logic: It is one of the fascinating features of blockchain [28]. With smart contracts, blockchain overlaps traditional paper-based contracts and converts them into digital agreements [29]. Smart contracts provide network automation and enable codifying the digital agreement between untrusted parties without central supervision [30]. Smart contract verifiability and auto-enforcing ability facilitate the execution of predefined business rules in a distributed network, where each participating node is equal to predefined authority. Smart contract code, once executed on the blockchain, no one can modify or change that code. Multiple blockchain platforms support smart contract execution by using numerous programming languages. In Ethereum, solidity is a well-known language. In Hyperledger Fabric, Go, JavaScript, and Java are major programming languages. Regardless of blockchain type, smart contracts help to encode business logic. Smart contracts are self-executing and tamper-proof programming codes that are responsible for reshaping business processes. Smart contracts embedded in blockchain enable predefined conditions of the agreement to be executed automatically without any third-party intervention. As a result, it can reduce administration costs and improve the efficiency of the process [30].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Authors | Key Findings | Limitation |
|---|---|---|---|
| 1 | S. Bhattacharya et al., 2019 [35] | With blockchain’s help, the surveillance system can become more effective and faster than traditional surveillance in terms of coverage, durability, consensus, selective privacy, uniqueness, and timing. The blockchain avoids data duplication and improves patient-provider communication. | Lack of frameworks for implementation and regulation, concerns for cost-effectiveness and interoperability. |
| 2 | Vijay Kumar Chattu et al., 2019 [36] | This paper explores the basics of blockchain, its applications, quality of experience, and advantages in disease surveillance over the other widely used real-time and machine-learning techniques. The blockchain helps to achieve data integrity. | There is a need to address security and scalability issues. |
| 3 | Filipe Bernardi et al., 2019 [5] | This paper presents a blockchain-based TB network proposal to share tuberculosis data between several stakeholders. Due to permissioned blockchain networks, stakeholders guarantee security and auditability to transmit or receive data; they can manage their data access levels, users, and privacy. | Lack of scalability, interoperability |
| 4 | Cichosz et al., 2018 [32] | Authors propose using NEM Blockchain to develop patient-centered governance of health data, multi-signature contracts for access control of data management, and data encryption to allow privacy and control of health care data. | Lack of scalability |
| 5 | Jie Xu et al., 2019 [37] | The authors propose a health chain, a large-scale health data privacy-preserving scheme, and encrypted health data to conduct fine-grained access control in this paper. Privacy is maintained; users can effectively revoke or add authorized doctors by leveraging user transactions for key management. | Interoperability, lack of open standards, trust between all parties, and data integration |
| 6 | S. Tanwar et al., 2020 [38] | The authors propose a system architecture and algorithm for a patient-centered approach to providing an access control policy with symmetric key cryptography to a different healthcare provider. | There is a need to address the privacy issue |
| 7 | Peng Zhang et al., 2018 [39] | It enables scalable and secure clinical data sharing with established trusts, providing clinicians with secure and scalable collaborative care decision support. | High deployment cost, interoperability |
| 8 | Asma Khatoon et al., 2020 [40] | This paper proposes using a smart contract from the Ethereum platform to build record ownership, permission, data integrity, and patient-provider coordination. Smart contracts have been designed for different medical workflows and managing data access permission between various entities in the healthcare ecosystem. | The cost of deployment of the smart contracts is higher |
| 9 | Lee et al., 2020 [41] | This paper designed an Ethereum-based blockchain model for health data exchange to guarantee data availability and integrity. | Data Privacy |
| 10 | Rahman et al. [42] | The authors designed private blockchain-based architecture for cancer patients to provide secure data exchange among healthcare stakeholders. | Lack of Scalability |
| 11 | Dib et al. [43] | In this paper, the authors created a Hyperledger fabric blockchain-based model to develop a user-centric network for effective data sharing between patients and stakeholders. | Lack of Scalability |
| 12 | EI Mojdoubie et al. [44] | The authors proposed a blockchain-based smart healthcare model to share data in a privacy-preserving manner. | Interoperability |
| 13 | Yazdinejad et al. [31] | Blockchain creates a decentralized network for remote patient monitoring with valid access policies and secure data transmission. | Lack of Scalability |
| 14 | Singh et al. [45] | The authors present a novel blockchain-enabled patient-oriented framework for healthcare applications. This Hyperledger-based architecture provides a secure data-sharing platform for stakeholders of the healthcare domain. | - |
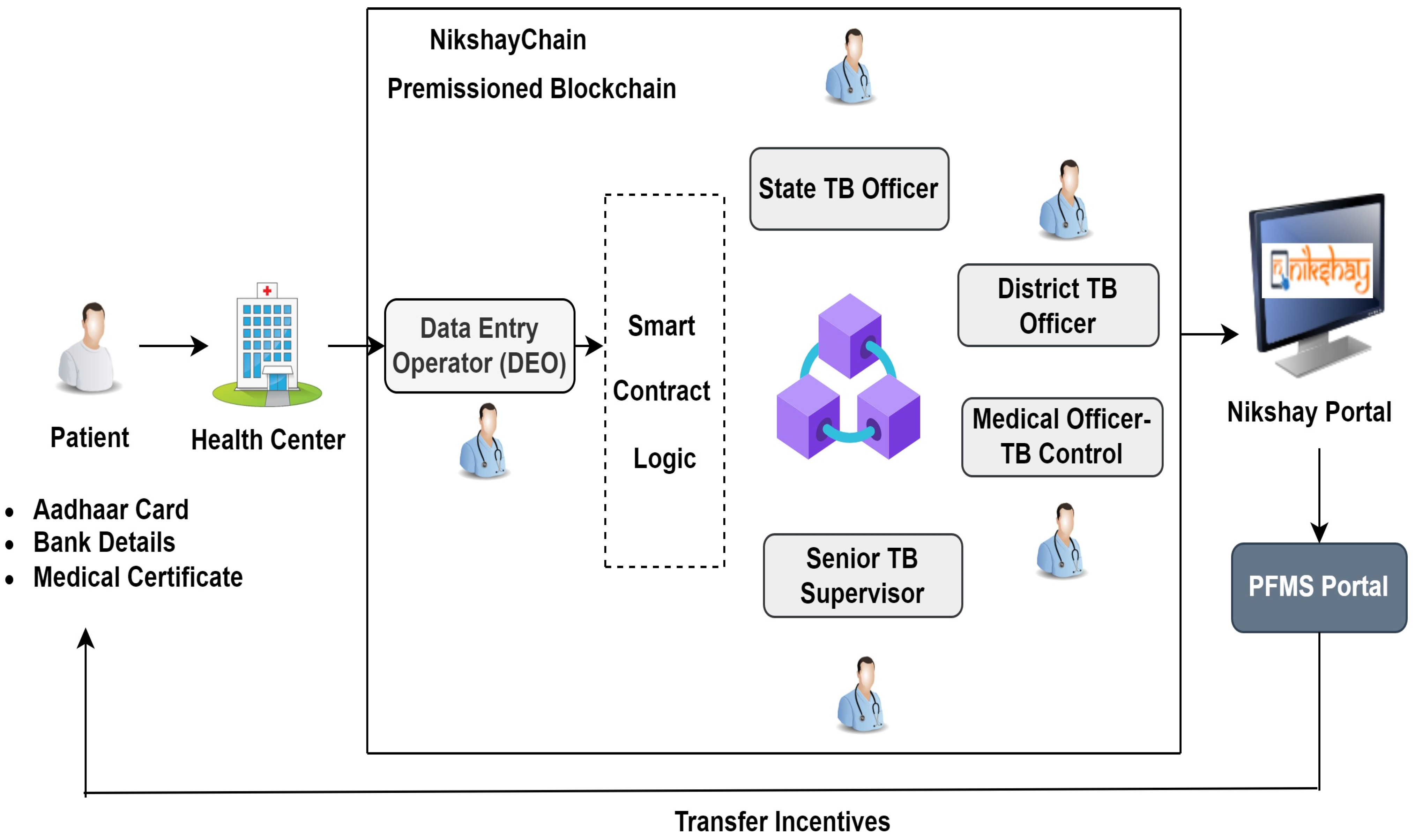
3.4. NikshayChain: A Proposed Blockchain-Based NPY Architecture
3.4.1. System Overview
3.4.2. A Proposed System Architecture
4. Discussion
- It will strengthen the overall national TB surveillance system in India.
- With the blockchain, the process of data verification and transfer of incentive takes place automatically and efficiently. The NPY process can become simpler, faster, and more transparent.
- It will improve service quality and will increase operational efficiency. It will eliminate the need for multiple layers of approver to reduce the delay in verification and transfer of incentive to the respective bank account of the patient.
- This framework can transfer incentive to a beneficiary on time, improving transparency, efficiency, and accountability in the TB surveillance system.
- It will reduce the overburden on all TB stakeholders and eventually boost the DBT process, and no need to maintain extensive paper-based documentation.
- Increase the trust among the patient to share their document, and provide personalized care to TB patients.
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Umair, M.; Cheema, M.A.; Cheema, O.; Li, H.; Lu, H. Impact of COVID-19 on IoT Adoption in Healthcare, Smart Homes, Smart Buildings, Smart Cities, Transportation and Industrial IoT. Sensors 2021, 21, 3838. [Google Scholar] [CrossRef] [PubMed]
- Hiwale, S.; Ulman, S.; Subbaraman, K.; Hiwale, S.; Ulman, S.; Subbaraman, K. Barriers to Adoptions of IoT-Based Solutions for Disease Screening. Available online: https://www.igi-global.com/gateway/chapter/215040 (accessed on 24 November 2021).
- Bhushan, B.; Khamparia, A.; Sagayam, K.M.; Sharma, S.K.; Ahad, M.A.; Debnath, N.C. Blockchain for Smart Cities: A Review of Architectures, Integration Trends and Future Research Directions. Sustain. Cities Soc. 2020, 61, 102360. [Google Scholar] [CrossRef]
- Hiwale, M.; Phanasalkar, S.; Kotecha, K. Using Blockchain and Distributed Machine Learning to Manage Decentralized but Trustworthy Disease Data. Sci. Technol. Libr. 2021, 40, 190–213. [Google Scholar] [CrossRef]
- Bernardi, F.; Lima, V.; Pellison, F.; de Azevedo Marques, P.M.; Rijo, R.; Galliez, R.M.; Kritski, A.; Alves, D. Blockchain Based Network for Tuberculosis: A Data Sharing Initiative in Brazil. Stud. Health Technol. Inform. 2019, 262, 264–267. [Google Scholar] [CrossRef]
- Chakaya, J.; Khan, M.; Ntoumi, F.; Aklillu, E.; Fatima, R.; Mwaba, P.; Kapata, N.; Mfinanga, S.; Hasnain, S.E.; Katoto, P.D.M.C.; et al. Global Tuberculosis Report 2020—Reflections on the Global TB Burden, Treatment and Prevention Efforts. Int. J. Infect. Dis. 2021, 113, S7–S12. [Google Scholar] [CrossRef]
- Global Tuberculosis Report 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 18 November 2022).
- Vashi, K.; Pathak, Y.V.; Patel, J. Understanding the Gaps in Elimination of Tuberculosis in India. Indian J. Tuberc. 2021, 68, 114–118. [Google Scholar] [CrossRef]
- Dias, H.M.Y.; Pai, M.; Raviglione, M.C. Ending Tuberculosis in India: A Political Challenge & an Opportunity. Indian J. Med. Res. 2018, 147, 217–220. [Google Scholar] [CrossRef]
- Sj, M.; Ep, S. Malnutrition and Associated Disorders in Tuberculosis and Its Therapy. J. Diet. Suppl. 2019, 16, 602–610. [Google Scholar] [CrossRef]
- World Health Organization. Compendium of WHO Guidelines and Associated Standards: Ensuring Optimum Delivery of the Cascade of Care for Patients with Tuberculosis, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-151410-1. [Google Scholar]
- Kumar, R.; Khayyam, K.U.; Singla, N.; Anand, T.; Nagaraja, S.B.; Sagili, K.D.; Sarin, R. Nikshay Poshan Yojana (NPY) for Tuberculosis Patients: Early Implementation Challenges in Delhi, India. Indian J. Tuberc. 2020, 67, 231–237. [Google Scholar] [CrossRef]
- Hölbl, M.; Kompara, M.; Kamišalić, A.; Nemec Zlatolas, L. A Systematic Review of the Use of Blockchain in Healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef]
- Agbo, C.C.; Mahmoud, Q.H.; Eklund, J.M. Blockchain Technology in Healthcare: A Systematic Review. Healthcare 2019, 7, 56. [Google Scholar] [CrossRef]
- Durneva, P.; Cousins, K.; Chen, M. The Current State of Research, Challenges, and Future Research Directions of Blockchain Technology in Patient Care: Systematic Review. J. Med. Internet Res. 2020, 22, e18619. [Google Scholar] [CrossRef] [PubMed]
- Ni-Kshay Poshan Yojana: Central TB Division. Available online: https://tbcindia.gov.in/index1.php?lang=1&level=1&sublinkid=5275&lid=3385 (accessed on 18 November 2022).
- Gupta, D. Strategy and Way Forward for TB Elimination. Indian J. Tuberc. 2018, 65, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.H.; Jeyashree, K.; Chinnakali, P.; Vijayageetha, M.; Mehta, K.G.; Modi, B.; Chavda, P.D.; Dave, P.V.; Zala, C.C.; Shewade, H.D.; et al. Cash Transfer Scheme for People with Tuberculosis Treated by the National TB Programme in Western India: A Mixed Methods Study. BMJ Open 2019, 9, e033158. [Google Scholar] [CrossRef] [PubMed]
- India TB Report 2022: Central TB Division. Available online: https://tbcindia.gov.in/index1.php?lang=1&level=1&sublinkid=5613&lid=3658 (accessed on 18 November 2022).
- Nirgude, A.S.; Kumar, A.M.V.; Collins, T.; Naik, P.R.; Parmar, M.; Tao, L.; Akshaya, K.M.; Raghuveer, P.; Yatnatti, S.K.; Nagendra, N.; et al. ‘I Am on Treatment since 5 Months but I Have Not Received Any Money’: Coverage, Delays and Implementation Challenges of ‘Direct Benefit Transfer’ for Tuberculosis Patients—A Mixed-Methods Study from South India. Glob. Health Action 2019, 12, 1633725. [Google Scholar] [CrossRef]
- Thakur, G.; Thakur, S.; Thakur, H. Status and Challenges for Tuberculosis Control in India—Stakeholders’ Perspective. Indian J. Tuberc. 2021, 68, 334–339. [Google Scholar] [CrossRef]
- Sachdeva, K.S. Accelerating Progress towards Ending Tuberculosis in India. Indian J. Med. Res. Suppl. 2020, 151, 266–268. [Google Scholar] [CrossRef]
- Nakamoto, S. Bitcoin: A Peer-to-Peer Electronic Cash System. Available online: https://bitcoin.org/bitcoin.pdf (accessed on 18 November 2022).
- Leeming, G.; Ainsworth, J.; Clifton, D.A. Blockchain in Health Care: Hype, Trust, and Digital Health. Lancet 2019, 393, 2476–2477. [Google Scholar] [CrossRef]
- Pandey, P.; Litoriya, R. Implementing Healthcare Services on a Large Scale: Challenges and Remedies Based on Blockchain Technology. Health Policy Technol. 2020, 9, 69–78. [Google Scholar] [CrossRef]
- Hasselgren, A.; Kralevska, K.; Gligoroski, D.; Pedersen, S.A.; Faxvaag, A. Blockchain in Healthcare and Health Sciences—A Scoping Review. Int. J. Med. Inform. 2020, 134, 104040. [Google Scholar] [CrossRef]
- Abu-elezz, I.; Hassan, A.; Nazeemudeen, A.; Househ, M.; Abd-alrazaq, A. The Benefits and Threats of Blockchain Technology in Healthcare: A Scoping Review. Int. J. Med. Inform. 2020, 142, 104246. [Google Scholar] [CrossRef] [PubMed]
- Hewa, T.; Ylianttila, M.; Liyanage, M. Survey on Blockchain Based Smart Contracts: Applications, Opportunities and Challenges. J. Netw. Comput. Appl. 2020, 177, 102857. [Google Scholar] [CrossRef]
- Sookhak, M.; Jabbarpour, M.R.; Safa, N.S.; Yu, F.R. Blockchain and Smart Contract for Access Control in Healthcare: A Survey, Issues and Challenges, and Open Issues. J. Netw. Comput. Appl. 2021, 178, 102950. [Google Scholar] [CrossRef]
- Khan, S.N.; Loukil, F.; Ghedira-Guegan, C.; Benkhelifa, E.; Bani-Hani, A. Blockchain Smart Contracts: Applications, Challenges, and Future Trends. Peer-to-Peer Netw. Appl. 2021, 14, 2901–2925. [Google Scholar] [CrossRef]
- Yazdinejad, A.; Srivastava, G.; Parizi, R.M.; Dehghantanha, A.; Choo, K.-K.R.; Aledhari, M. Decentralized Authentication of Distributed Patients in Hospital Networks Using Blockchain. IEEE J. Biomed. Health Inform. 2020, 24, 2146–2156. [Google Scholar] [CrossRef]
- Cichosz, S.L.; Stausholm, M.N.; Kronborg, T.; Vestergaard, P.; Hejlesen, O. How to Use Blockchain for Diabetes Health Care Data and Access Management: An Operational Concept. J. Diabetes Sci. Technol. 2018, 13, 248–253. [Google Scholar] [CrossRef]
- Dagher, G.G.; Mohler, J.; Milojkovic, M.; Marella, P.B. Ancile: Privacy-Preserving Framework for Access Control and Interoperability of Electronic Health Records Using Blockchain Technology. Sustain. Cities Soc. 2018, 39, 283–297. [Google Scholar] [CrossRef]
- Cernian, A.; Tiganoaia, B.; Sacala, I.; Pavel, A.; Iftemi, A. PatientDataChain: A Blockchain-Based Approach to Integrate Personal Health Records. Sensors 2020, 20, 6538. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Singh, A.; Hossain, M.M. Strengthening Public Health Surveillance through Blockchain Technology. AIMS Public Health 2019, 6, 326–333. [Google Scholar] [CrossRef]
- Chattu, V.K.; Nanda, A.; Chattu, S.K.; Kadri, S.M.; Knight, A.W. The Emerging Role of Blockchain Technology Applications in Routine Disease Surveillance Systems to Strengthen Global Health Security. Big Data Cogn. Comput. 2019, 3, 25. [Google Scholar] [CrossRef]
- Xu, J.; Xue, K.; Li, S.; Tian, H.; Hong, J.; Hong, P.; Yu, N. Healthchain: A Blockchain-Based Privacy Preserving Scheme for Large-Scale Health Data. IEEE Internet Things J. 2019, 6, 8770–8781. [Google Scholar] [CrossRef]
- Tanwar, S.; Parekh, K.; Evans, R. Blockchain-Based Electronic Healthcare Record System for Healthcare 4.0 Applications. J. Inf. Secur. Appl. 2020, 50, 102407. [Google Scholar] [CrossRef]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G.; Rosenbloom, S.T. FHIRChain: Applying Blockchain to Securely and Scalably Share Clinical Data. Comput. Struct. Biotechnol. J. 2018, 16, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Khatoon, A. A Blockchain-Based Smart Contract System for Healthcare Management. Electronics 2020, 9, 94. [Google Scholar] [CrossRef]
- Lee, H.-A.; Kung, H.-H.; Udayasankaran, J.G.; Kijsanayotin, B.; B Marcelo, A.; Chao, L.R.; Hsu, C.-Y. An Architecture and Management Platform for Blockchain-Based Personal Health Record Exchange: Development and Usability Study. J. Med. Internet Res. 2020, 22, e16748. [Google Scholar] [CrossRef]
- Rahman, M.A.; Rashid, M.; Barnes, S.; Hossain, M.S.; Hassanain, E.; Guizani, M. An IoT and Blockchain-Based Multi-Sensory In-Home Quality of Life Framework for Cancer Patients. In Proceedings of the 2019 15th International Wireless Communications Mobile Computing Conference (IWCMC), Tangier, Morocco, 24–28 June 2019; pp. 2116–2121. [Google Scholar]
- Dib, O.; Huyart, C.; Toumi, K. A Novel Data Exploitation Framework Based on Blockchain. Pervasive Mob. Comput. 2020, 61, 101104. [Google Scholar] [CrossRef]
- El Majdoubi, D.; El Bakkali, H.; Sadki, S. SmartMedChain: A Blockchain-Based Privacy-Preserving Smart Healthcare Framework. J. Healthc. Eng. 2021, 2021, 4145512. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.P.; Pradhan, N.R.; Luhach, A.K.; Agnihotri, S.; Jhanjhi, N.Z.; Verma, S.; Kavita; Ghosh, U.; Roy, D.S. A Novel Patient-Centric Architectural Framework for Blockchain-Enabled Healthcare Applications. IEEE Trans. Ind. Inf. 2021, 17, 5779–5789. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiwale, M.; Varadarajan, V.; Walambe, R.; Kotecha, K. NikshayChain: A Blockchain-Based Proposal for Tuberculosis Data Management in India. Technologies 2023, 11, 5. https://doi.org/10.3390/technologies11010005
Hiwale M, Varadarajan V, Walambe R, Kotecha K. NikshayChain: A Blockchain-Based Proposal for Tuberculosis Data Management in India. Technologies. 2023; 11(1):5. https://doi.org/10.3390/technologies11010005
Chicago/Turabian StyleHiwale, Madhuri, Vijayakumar Varadarajan, Rahee Walambe, and Ketan Kotecha. 2023. "NikshayChain: A Blockchain-Based Proposal for Tuberculosis Data Management in India" Technologies 11, no. 1: 5. https://doi.org/10.3390/technologies11010005
APA StyleHiwale, M., Varadarajan, V., Walambe, R., & Kotecha, K. (2023). NikshayChain: A Blockchain-Based Proposal for Tuberculosis Data Management in India. Technologies, 11(1), 5. https://doi.org/10.3390/technologies11010005