
Medication Utilisation Program, Quality Improvement and Research Pharmacist—Implementation Strategies and Preliminary Findings



Abstract
:1. Introduction
- Safe, avoiding injuries to patients from the care that is intended to help them.
- Effective, providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit (avoiding underuse and overuse, respectively).
- Patient-centred, providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.
- Timely, reducing waits and sometimes harmful delays for both those who receive and those who give care.
- Efficient, avoiding waste, including waste of equipment, supplies, ideas and energy.
- Equitable, providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location and socioeconomic status.
- When the benefit of the medication is unknown;
- When there are little data available to influence choice;
- When there is a need to analyse the process of medication management including prescribing, preparation, dispensing, administration and monitoring.
- Authoritative medical staff support;
- Clear structure and leadership with clear definition of roles, responsibilities and accountabilities;
- Excellent communication and the importance of involvement of key stakeholders;
- Excellent documentation summarising findings and outlining an action plan;
- An interdisciplinary approach;
- Follow up and evaluation of initial actions, flexibility to adjust the action plan if necessary and keeping sight of improvement goals;
- Education regarding not only how to conduct these studies but also education when implementing new processes.
2. Materials and Methods
2.1. Establishment of the Role
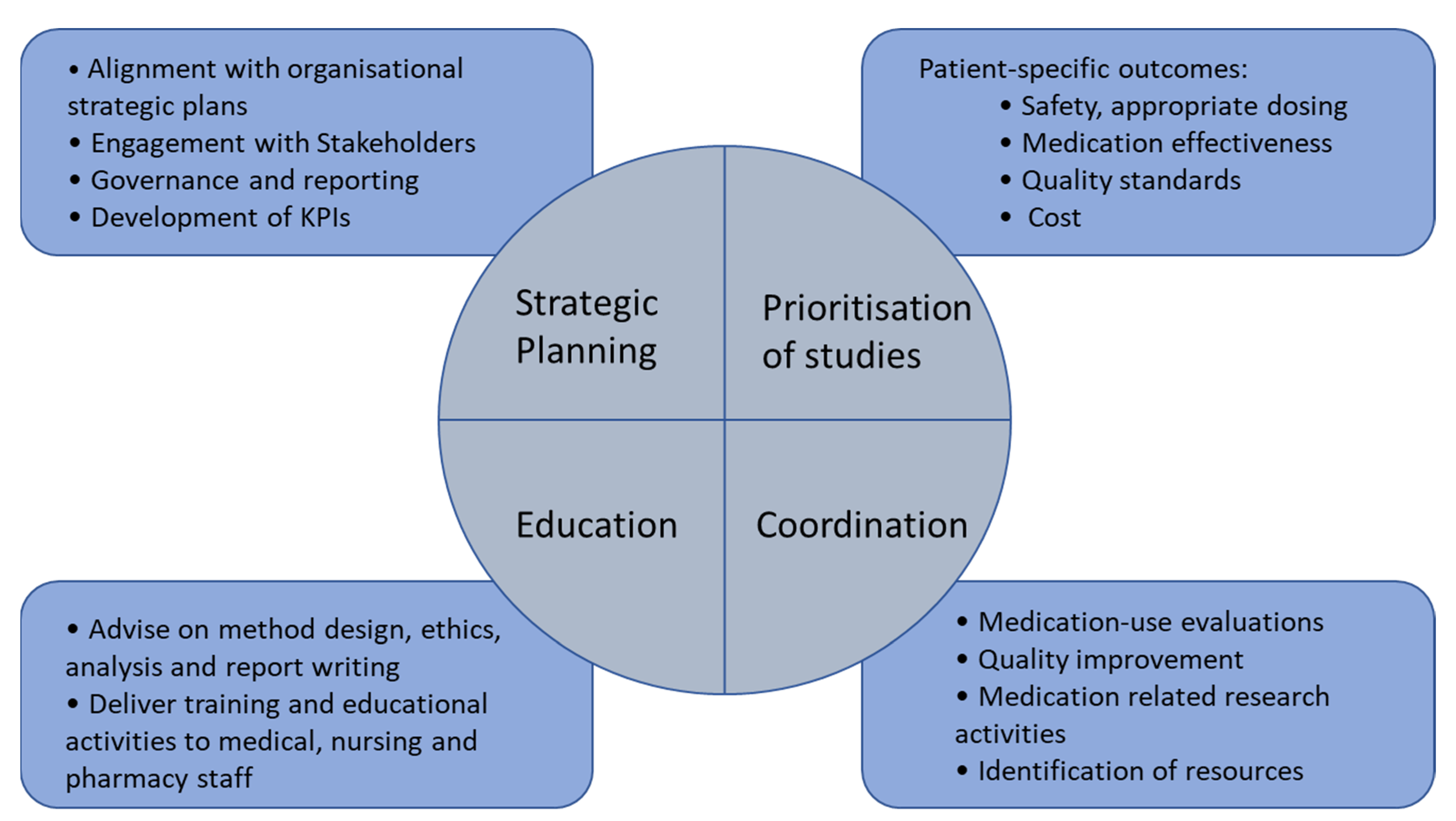
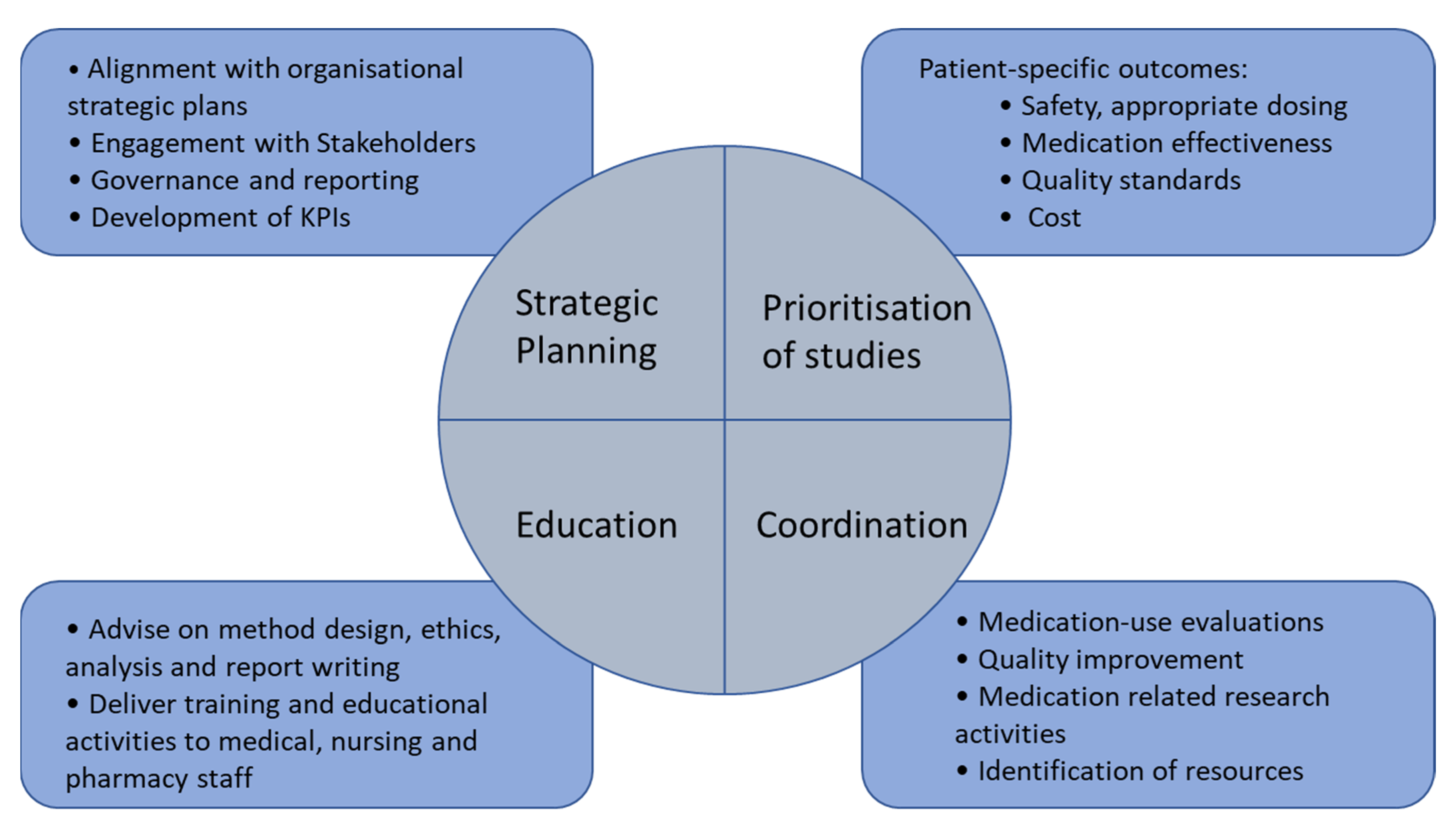
2.2. Purpose of the Role
- To lead the strategic planning and implementation of a Medication Utilisation Program to include medication quality improvement and medication related research activities.
- To coordinate medication-use evaluations, quality improvement and medication related research activities including: the evidence-based review of medicines use, review of medication expenditure, and the implementation and evaluation of interventions to change practice in collaboration with medical, pharmacy and nursing staff across all service lines of the hospital.
- To apply, implement and evaluate the Medication Utilisation Program in cost-effectiveness and patient outcomes, in alignment with the Australian Commission’s National Safety and Quality Health Service Standards.
- To implement the Medication Utilisation Program with a focus on high cost, high usage and high-risk medications to ensure cost-effective, evidence-based medication use is implemented to optimise patient outcomes.
- To develop and deliver training and educational activities associated with medication utilisation review, quality improvement and research activities to medical, nursing and pharmacy staff.
2.3. Governance Structure
2.4. Cost Containment Activities
2.5. Dissemination of Study Findings
3. Results
3.1. Strategic Planning
3.2. Development of MUP Studies
3.3. Cost Containment Activities
3.4. Educational Activities
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Government Department of Health. What is Quality Use of Medicines? 2020. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/nmp-quality.htm (accessed on 23 October 2021).
- Wilks, C.; Krisle, E.; Westrich, K.; Lunner, K.; Muhlestein, D.; Dubois, R. Optimization of Medication Use at Accountable Care Organizations. J. Manag. Care Spec. Pharm. 2017, 23, 1054–1064. [Google Scholar] [PubMed]
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academy of Sciences: Washington, DC, USA, 2001.
- Vest, T.A.; Gazda, N.P.; Schenkat, D.H.; Eckel, S.F. Practice-enhancing publications about the medication-use process in 2018. Am. J. Health Syst. Pharm. 2020, 77, 759–770. [Google Scholar] [CrossRef] [PubMed]
- Afanasjeva, J.; Burk, M.; Cunningham, F.; Fanikos, J.; Gabay, M.; Hayes, G.; Masters, P.L.; Rodriguez, R.; Sinnett, M.J. ASHP Guidelines on Medication-Use Evaluation. Am. J. Health Pharm. 2021, 78, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Fanikos, J.; Jenkins, K.L.; Piazza, G.; Connors, J.; Goldhaber, S.Z. Medication use evaluation: Pharmacist rubric for performance improvement. Pharmacotherapy 2014, 34 (Suppl. 1), 5s–13s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Drug and Therapeutics Committees: A Practical Guide. 2003. Available online: https://apps.who.int/iris/handle/10665/68553 (accessed on 23 October 2021).
- Jones, B.; Vaux, E.; Olsson-Brown, A. How to get started in quality improvement. BMJ 2019, 364, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregory, K.E. Differentiating Between Research and Quality Improvement. J. Périnat. Neonatal Nurs. 2015, 29, 100–102. [Google Scholar] [CrossRef] [PubMed]
- International Pharmacuetical Federation. FIP Global Advanced Development Framework—Supporting the advancement of the profession. 2019. Available online: https://www.fip.org/file/4331 (accessed on 23 October 2021).
- Galbraith, K.; Coombes, I.; Matthews, A.; Rowett, D.; Bader, L.R.; Bates, I. Advanced pharmacy practice: Aligning national action with global targets. J. Pharm. Pract. Res. 2017, 47, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Helou, N.; Talhouedec, D.; Zumstein-Shaha, M.; Zanchi, A. A Multidisciplinary Approach for Improving Quality of Life and Self-Management in Diabetic Kidney Disease: A Crossover Study. J. Clin. Med. 2020, 9, 2160. [Google Scholar] [CrossRef] [PubMed]
- Mieiro, D.B.; De Oliveira Érica, B.C.; Da Fonseca, R.E.P.; Mininel, V.A.; Zem-Mascarenhas, S.H.; Machado, R.C. Strategies to minimize medication errors in emergency units: An integrative review. Rev. Bras. Enferm. 2019, 72, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lincoln, E.W.; Reed-Schrader, E.; Jarvis, J.L. EMS Quality Improvement Programs; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK536982/#!po=91.6667 (accessed on 4 November 2021).
- Downen, J.; Jaeger, C. Quality improvement of intravenous to oral medication conversion using Lean Six Sigma methodologies. BMJ Open Qual. 2020, 9, e000804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prosci. What Is the ADKAR Model? 2018. Available online: http://www.prosci.com/adkar/adkar-model (accessed on 23 October 2021).
- Wong, Q.; Lacombe, M.; Keller, R.; Joyce, T.; O’Malley, K. Leading change with ADKAR. Nurs. Manag. 2019, 50, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Kotter, J.P. Accelerate! Harv. Bus. Rev. 2012, 90, 149. [Google Scholar]
- Barrow, J.M.; Annamaraju, P.; Toney-Butler, T.J. Change Management; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459380/ (accessed on 4 November 2021).
- Kumar, A.; Nesbitt, K.M.; Bakkum-Gamez, J.N. Quality improvement in gynecologic oncology: Current successes and future promise. Gynecol Oncol. 2019, 152, 486–491. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Objective 1 To Always Put People First. | Objective 2 To Improve Health Equity, Access, Quality, Safety and Health Outcomes. | Objective 3 To Deliver Value-Based Health Services through a Culture of Research, Education, Learning and Innovation. | Objective 4 To be Accountable for Delivery of Sustainable Services, High Performance and Excellent Patient Outcomes. |
|---|---|---|---|
|
|
|
|
| Key Performance Indicators | |||
|
|
|
|
| MUE and Rationale | Outcome | Objective Alignment |
|---|---|---|
| Poractant Alfa use in Neonatal Intensive Care High-cost medication and adherence to guidelines |
| 1.2, 2.7, 3.1 |
| Tapentadol use in admitted patients Opioid stewardship and adherence to local hospital formulary |
| 1.2, 2.2, 2.7 |
| Botulinum Toxin type A use High-cost medication and adherence to local hospital restrictions |
| 1.2, 3.1 |
| Intravenous aciclovir High-cost medication and adherence to local hospital restrictions |
| 1.2, 2.2, 3.1 |
| Nebulised pentamidine in cancer care for PJP prophylaxis High-cost medication and appropriate use |
| 1.2, 3.1 |
| Melatonin use in admitted adolescents (mental health ward) Adherence to interim hospital approval in select adolescent patients |
| 1.2 |
| Intravenous fluid use High-cost medications and adherence to local hospital formulary |
| 1.2, 3.1 |
| Study | Rationale | Potential Outcomes | Objective Alignment |
|---|---|---|---|
| Evaluation of the correlation, preventability and severity of hospital acquired complications. specifically hemorrhage from anticoagulant medications | Retrospective study of patients with a hospital acquired complication (HAC) coded in relation to anticoagulation medications. This is a high-risk medication. Adverse effects contribute to poorer clinical outcomes for patients, and often increase length of stay in hospital, increasing financial burden on the health system. | Identification of common underlying causes for hemorrhagic hospital acquired complications from anticoagulants. Identification of the appropriateness of hospital acquired complication (HAC) coding in relation to anticoagulants. | 2.1, 2.2 |
| To evaluate the use of LAMA * and LABA ** inhaler therapy following temporary hospital approval for continuation of therapy in admitted patients | LAMA * and LABA ** are expensive inhalers and not currently hospital approved. Interim alternative inhalers are supplied for admitted patients who do not bring in their own inhalers to hospital. This can result in confusion to patients and wastage. | To determine if the implementation of a hospital approval for continuing supply of LAMA * and LABA ** inhalers for admitted patients has resulted in a reduction in cost and wastage associated with interim and or alternative hospital approved inhalers. | 3.1 |
| To evaluate pharmacist confidence in documenting recommendations in patient clinical notes in a digital hospital compared to a paper-based hospital | Anecdotal evidence suggests documenting recommendations in the patient clinical notes by pharmacists is inconsistent. | Identification of any differences between pharmacists’ confidence documenting in patient clinical notes, at digital or paper-based site, and if so the barriers and enablers for this. | 1.2, 1.3 |
| To examine health care staff communication, knowledge and practices regarding medication management of patients with dysphagia | This is a collaborative study involving pharmacy and speech pathology. The effective management of patients with dysphagia rely on collaboration between the multidisciplinary team. The study will examine the current practice of the multidisciplinary team in the medication management of patients with dysphagia. | Identification of any gaps in staff communication, knowledge and practices regarding medication management of patients with dysphagia and development of interventions to address these. | 1.2, 2.1, 2.6 |
| To determine the use and effectiveness of antihypertensive medications currently used in Neonatal Intensive Care | This is a collaborative study looking at current antihypertensive agents used in critically ill infants to manage hypertensive episodes. Limited evidence is available to guide practice. | Identification of effectiveness of current medications to manage hypertension and any associated adverse events. | 1.2, 2.1, 2.2, 2.3 |
| To determine anti-arrhythmic medications prescribed in the peri-procedural and post-procedural period to reduce the risk of arrythmia recurrence | This is a collaborative study to explore the range of anti-arrhythmic medications currently prescribed and the monitoring undertaken compared to current local and international guidelines. | Identification if appropriate monitoring of anti-arrhythmic medications is taking place post discharge; and to identify any associated problems and address if required. | 1.2, 2.1, 2.3 |
| Therapeutic Drug Monitoring analysis | As an intervention Therapeutic Drug Monitoring has been shown to improve patient responses to important life-sustaining medications and to decrease adverse drug reactions. Therapeutic Drug Monitoring can have positive economic outcomes; however, these are negated if inappropriate and wasteful testing is undertaken. | Identification of the quantity and range of Therapeutic Drug Monitoring performed and evaluate the usefulness of the result when compared with current guidelines. Identification if appropriate dose adjustment made was appropriate and evaluate any waste. | 1.2, 2.2, 3.1, 4.1 |
| To develop and evaluate a tool to efficiently and reproducibly track the cost of claimable and non-claimable medication dispensed within the hospital | Tracking costs of non-claimable medicines and reviewing use that falls outside the Pharmaceutical Benefits Scheme (PBS) indication ensures optimal patient care and financial sustainability of medication use. | Development of a tool to allow efficient, timely analysis of non-claimed and claimed high-cost medicines, projection of high-cost medicine expenses and evaluation of cost changes associated with changes in mediation supply. | 3.1 |
| Study | Objective Alignment |
|---|---|
| Strategies to investigate oral mucositis prevention in patients undergoing haematopoietic stem cell transplantation (HSCT) | 1.2, 1.4, 2.2, 3.3 |
| Investigation to evaluate the impact of a pharmacist-led Therapeutic Drug Monitoring optimisation | 1.2, 1.4, 2.2, 3.3 |
| Development and implementation of a risk assessment tool of poisoned patients by non-expert clinicians in Emergency Departments | 1.2, 1.4, 2.2, 3.3 |
| Investigation of the impact of a pharmacist in the medication management of patients post bariatric surgery | 1.1 1.2, 1.4, 3.3 |
| Investigation of the impact of a multidisciplinary team in the medication optimisation of diabetic patient prior to surgery | 1.1, 1.2, 2.2, 1.4, 3.3 |
| Investigation of the impact of a pharmacist in early cardiac patient follow up after hospital discharge | 1.1, 1.2, 1.4, 3.3 |
| Characteristics of readmitted patients reviewed by a high-risk discharge pharmacist | 1.2, 1.4, 3.3 |
| Key Performance Indicator | Comment |
|---|---|
| 1.1 Demonstrate at least three codesigned MUP initiatives with consumers per annum | Not achieved |
| 1.2 Demonstrate staff participation in MUP activities | Achieved |
| 1.3 Demonstrate MUP educational activities for staff | Achieved |
| 2.1 Conduct 5 MUEs per year | Achieved |
| 2.2 Conduct 3 MUEs activities related to high-risk medications per year | Not achieved |
| 3.1 Demonstrate at least three cost-effective initiatives per annum | Achieved |
| 3.2 Demonstrate involvement in staff pursuing a higher degree | Achieved |
| 4.1 Achieve sustainable positive financial results | Achieved |
| 4.2 Demonstrate projects that have a robust evaluation framework | Achieved |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whitfield, K.; Coombes, I.; Denaro, C.; Donovan, P. Medication Utilisation Program, Quality Improvement and Research Pharmacist—Implementation Strategies and Preliminary Findings. Pharmacy 2021, 9, 182. https://doi.org/10.3390/pharmacy9040182
Whitfield K, Coombes I, Denaro C, Donovan P. Medication Utilisation Program, Quality Improvement and Research Pharmacist—Implementation Strategies and Preliminary Findings. Pharmacy. 2021; 9(4):182. https://doi.org/10.3390/pharmacy9040182
Chicago/Turabian StyleWhitfield, Karen, Ian Coombes, Charles Denaro, and Peter Donovan. 2021. "Medication Utilisation Program, Quality Improvement and Research Pharmacist—Implementation Strategies and Preliminary Findings" Pharmacy 9, no. 4: 182. https://doi.org/10.3390/pharmacy9040182
APA StyleWhitfield, K., Coombes, I., Denaro, C., & Donovan, P. (2021). Medication Utilisation Program, Quality Improvement and Research Pharmacist—Implementation Strategies and Preliminary Findings. Pharmacy, 9(4), 182. https://doi.org/10.3390/pharmacy9040182