
Outcomes of a National, Cross-Sector Antimicrobial Stewardship Training Initiative for Pharmacists in England



Abstract
1. Introduction
2. Materials and Methods
2.1. Funding, Training Design, and Delivery
2.2. Learners, Tutors, and Assessors
2.3. Data Collection and Evaluation
2.4. Ethics Approval
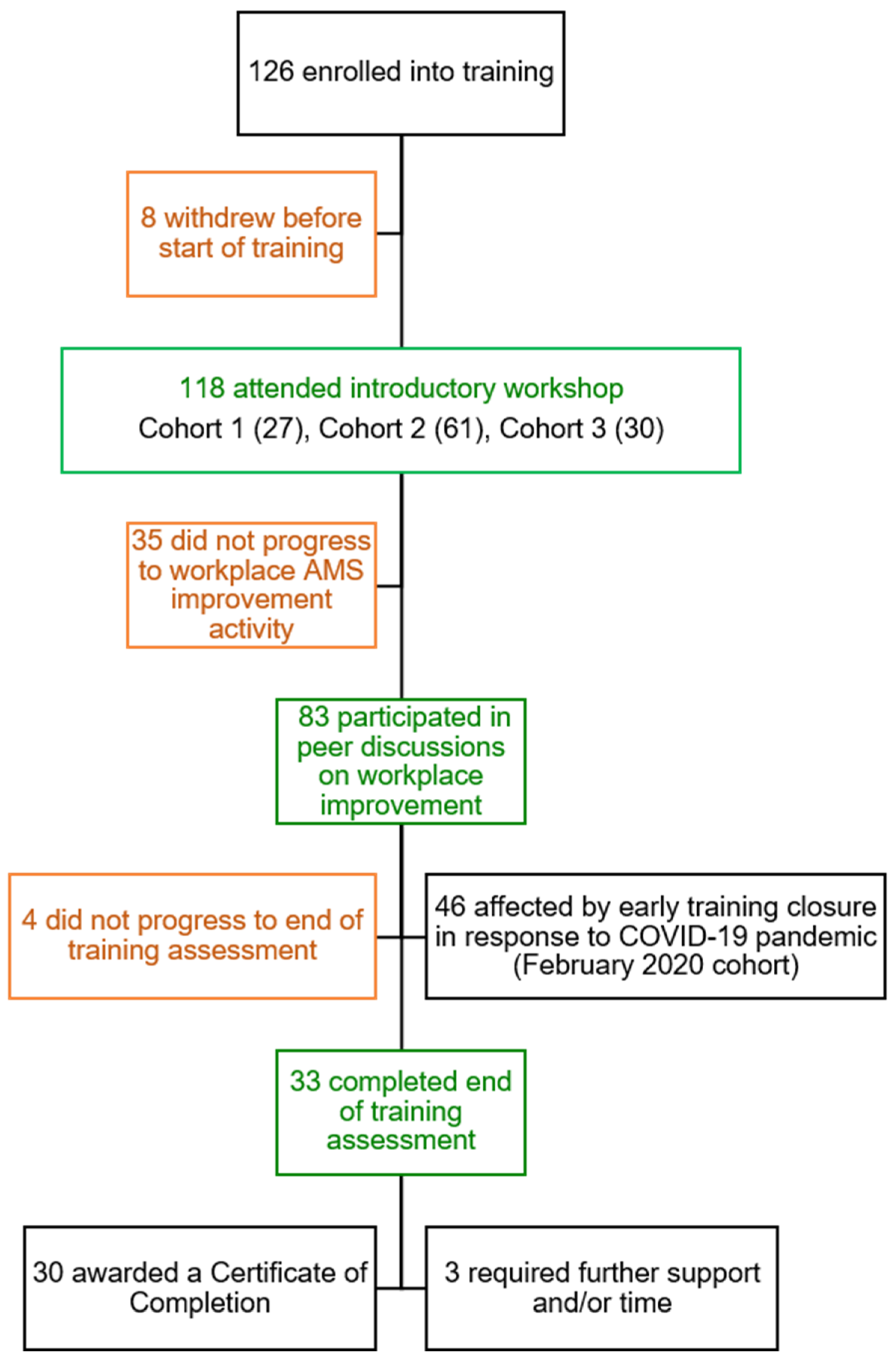
3. Results
3.1. Learner Demographics
3.2. Knowledge Quiz
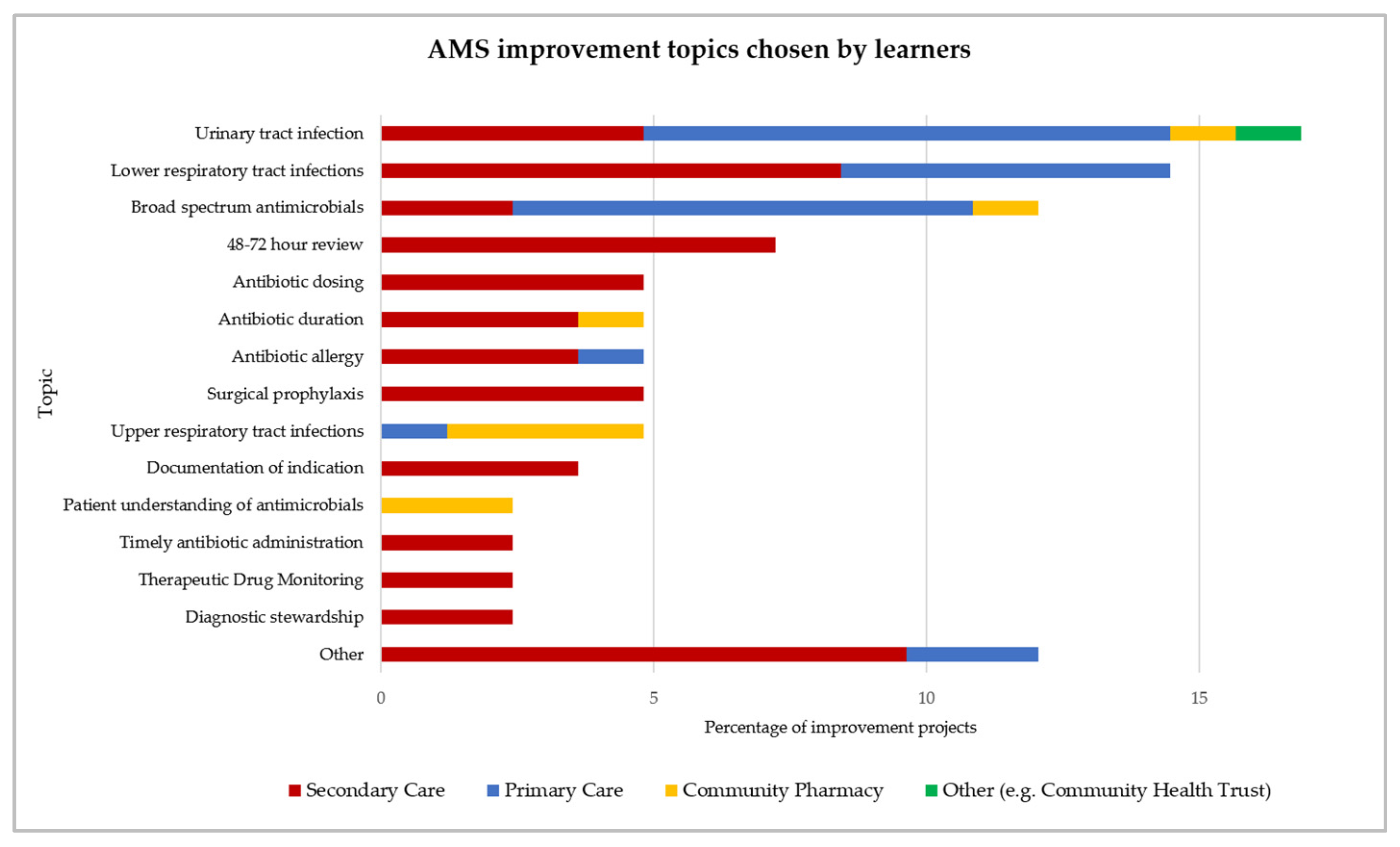
3.3. Analysis of Learner Improvement Projects
3.4. Learner Feedback and Follow-Up Surveys
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Neill, J.; UK Trust; UK Government. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. The Review on Antimicrobial Resistance. Tackling Drug-Resistant Infections Globally. Available online: https://wellcomecollection.org/works/rdpck35v (accessed on 9 August 2021).
- World Health Organisation. Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/publications-detail-redirect/9789241509763 (accessed on 9 August 2021).
- Department of Health and Social Care. UK 20-Year Vision for Antimicrobial Resistance. Available online: https://www.gov.uk/government/publications/uk-20-year-vision-for-antimicrobial-resistance (accessed on 24 August 2021).
- Department of Health and Social Care. UK 5 Year Antimicrobial Resistance Strategy 2013 to 2018. Available online: https://www.gov.uk/government/publications/uk-5-year-antimicrobial-resistance-strategy-2013-to-2018 (accessed on 17 May 2021).
- Department of Health and Social Care. UK 5-Year Action Plan for Antimicrobial Resistance 2019 to 2024. Available online: https://www.gov.uk/government/publications/uk-5-year-action-plan-for-antimicrobial-resistance-2019-to-2024 (accessed on 17 May 2021).
- General Pharmaceutical Council. GPhC Survey of Registered Pharmacy Professionals 2019. Available online: https://www.pharmacyregulation.org/about-us/research/gphc-survey-registered-pharmacy-professionals-2019 (accessed on 24 August 2021).
- Liaskou, M.; Duggan, C.; Joynes, R.; Rosado, H. Pharmacy’s Role in Antimicrobial Resistance and Stewardship. Clin. Pharm. 2018, 10. [Google Scholar] [CrossRef]
- Gilchrist, M.; Wade, P.; Ashiru-Oredope, D.; Howard, P.; Sneddon, J.; Whitney, L.; Wickens, H. Antimicrobial Stewardship from Policy to Practice: Experiences from UK Antimicrobial Pharmacists. Infect. Dis. Ther. 2015, 4, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Wickens, H.J.; Farrell, S.; Ashiru-Oredope, D.A.I.; Jacklin, A.; Holmes, A.; Antimicrobial Stewardship Group of the Department of Health Advisory Committee on Antimicrobial Resistance and Health Care Associated Infections (ASG-ARHAI); Cooke, J.; Sharland, M.; Ashiru-Oredope, D.; McNulty, C.; et al. The Increasing Role of Pharmacists in Antimicrobial Stewardship in English Hospitals. J. Antimicrob. Chemother. 2013, 68, 2675–2681. [Google Scholar] [CrossRef] [PubMed]
- Ashiru-Oredope, D.; Budd, E.L.; Bhattacharya, A.; Din, N.; McNulty, C.A.M.; Micallef, C.; Ladenheim, D.; Beech, E.; Murdan, S.; Hopkins, S.; et al. Implementation of Antimicrobial Stewardship Interventions Recommended by National Toolkits in Primary and Secondary Healthcare Sectors in England: TARGET and Start Smart Then Focus. J. Antimicrob. Chemother. 2016, 71, 1408–1414. [Google Scholar] [CrossRef] [PubMed]
- Hancock, L.J.; Mellor, C. An evaluation of antimicrobial stewardship in community pharmacy. Fields: J. Hudders. Stud. Res. 2016, 2. [Google Scholar] [CrossRef]
- Wilcock, M.; Wisner, K.; Lee, F. Community Pharmacists and Antimicrobial Stewardship—What Is Their Role? J. Med. Optim. 2017, 3, 4. [Google Scholar]
- Tonna, A.P.; Weidmann, A.E.; Sneddon, J.; Stewart, D. Views and Experiences of Community Pharmacy Team Members on Antimicrobial Stewardship Activities in Scotland: A Qualitative Study. Int. J. Clin. Pharm. 2020, 42, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Allison, R.; Chapman, S.; Howard, P.; Thornley, T.; Ashiru-Oredope, D.; Walker, S.; Jones, L.F.; McNulty, C.A.M. Feasibility of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI): An Innovative Approach to Improve Patients’ Understanding of Their Antibiotics. JAC-Antimicrob. Resist. 2020, 2. [Google Scholar] [CrossRef]
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2019 to 2020. Available online: https://www.gov.uk/government/publications/english-surveillance-programme-antimicrobial-utilisation-and-resistance-espaur-report (accessed on 16 May 2021).
- Majumder, M.A.A.; Singh, K.; Hilaire, M.G.-S.; Rahman, S.; Sa, B.; Haque, M. Tackling Antimicrobial Resistance by Promoting Antimicrobial Stewardship in Medical and Allied Health Professional Curricula. Expert Rev. Anti Infect. Ther. 2020, 18, 1245–1258. [Google Scholar] [CrossRef] [PubMed]
- Castro-Sánchez, E.; Drumright, L.N.; Gharbi, M.; Farrell, S.; Holmes, A.H. Mapping Antimicrobial Stewardship in Undergraduate Medical, Dental, Pharmacy, Nursing and Veterinary Education in the United Kingdom. PLoS ONE 2016, 11, e0150056. [Google Scholar] [CrossRef] [PubMed]
- Ashiru-Oredope, D.; Cookson, B.; Fry, C. Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection Professional Education Subgroup Developing the First National Antimicrobial Prescribing and Stewardship Competences. J. Antimicrob. Chemother. 2014, 69, 2886–2888. [Google Scholar] [CrossRef] [PubMed]
- Royal Pharmaceutical Society. Post-Registration Foundation Curriculum. Available online: https://www.rpharms.com/development/credentialing/foundation/post-registration-foundation-curriculum (accessed on 26 September 2021).
- Royal Pharmaceutical Society. RPS Advanced Pharmacy Framework. Available online: https://www.rpharms.com/resources/frameworks/advanced-pharmacy-framework-apf (accessed on 18 August 2021).
- Sneddon, J.; Gilchrist, M.; Wickens, H. Development of an Expert Professional Curriculum for Antimicrobial Pharmacists in the UK. J. Antimicrob. Chemother. 2015, 70, 1277–1280. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Roque, F.; Herdeiro, M.T.; Soares, S.; Teixeira Rodrigues, A.; Breitenfeld, L.; Figueiras, A. Educational Interventions to Improve Prescription and Dispensing of Antibiotics: A Systematic Review. BMC Public Health 2014, 14, 1276. [Google Scholar] [CrossRef]
- Weier, N.; Nathwani, D.; Thursky, K.; Tängdén, T.; Vlahović-Palčevski, V.; Dyar, O.; Beović, B.; Levy Hara, G.; Patel, R.; Pulcini, C.; et al. An International Inventory of Antimicrobial Stewardship (AMS) Training Programmes for AMS Teams. J. Antimicrob. Chemother. 2021, 76, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Marwick, C.; Scott, C.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.; Ramsay, C.; Michie, S. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Behaviour Change and Antibiotic Prescribing in Healthcare Settings: Literature Review and Behavioural Analysis. Available online: https://www.gov.uk/government/publications/antibiotic-prescribing-and-behaviour-change-in-healthcare-settings. (accessed on 27 August 2021).
- The Lancet NICE Antimicrobial Stewardship: Right Drug, Dose, and Time? Lancet 2015, 386, 717. [CrossRef]
- National Institute for Health and Care Excellence. Antimicrobial Stewardship: Changing Risk-Related Behaviours in the General Population (NICE Guideline 63). Available online: https://www.nice.org.uk/guidance/ng63/chapter/Recommendations (accessed on 16 May 2021).
- NHS England. The NHS Long Term Plan. Available online: https://www.longtermplan.nhs.uk/ (accessed on 20 May 2021).
- Michie, S.; van Stralen, M.M.; West, R. The Behaviour Change Wheel: A New Method for Characterising and Designing Behaviour Change Interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- NHS Research Authority. Do I Need NHS Ethics Approval? Available online: http://www.hra-decisiontools.org.uk/ethics/ (accessed on 21 August 2021).
- Latif, A.; Gulzar, N.; Lowe, F.; Ansong, T.; Gohil, S. Engaging Community Pharmacists in Quality Improvement (QI): A Qualitative Case Study of a Partnership between a Higher Education Institute and Local Pharmaceutical Committees. BMJ Open Qual. 2021, 10, e001047. [Google Scholar] [CrossRef] [PubMed]
- Royal Pharmaceutical Society. RPS to Offer Free Clinical Consultation Skills Training to Community Pharmacists in England. Available online: https://pharmaceutical-journal.com/article/news/rps-to-offer-free-clinical-consultation-skills-training-to-community-pharmacists-in-england (accessed on 26 September 2021).
- McNicholas, C.; Lennox, L.; Woodcock, T.; Bell, D.; Reed, J.E. Evolving Quality Improvement Support Strategies to Improve Plan–Do–Study–Act Cycle Fidelity: A Retrospective Mixed-Methods Study. BMJ Qual. Saf. 2019, 28, 356. [Google Scholar] [CrossRef] [PubMed]
- The Health Foundation. Quality Improvement Training for Healthcare Professionals. Available online: https://www.health.org.uk/publications/quality-improvement-training-for-healthcare-professionals (accessed on 27 August 2021).
- NHS England. CCG CQUIN 2019/20 Indicators Specifications. Available online: https://www.england.nhs.uk/publication/ccg-cquin-2019-20-indicators-specifications/ (accessed on 26 August 2021).
- NHS England. Technical Guidance for Refreshing NHS Plans 2018/19 Annex A: Commissioning for Quality and Innovation (CQUIN) Indicator Specification 2017-2019. Available online: https://www.england.nhs.uk/publication/cquin-indicator-specification/ (accessed on 26 August 2021).
- NHS England. Quality Premium. Available online: https://www.england.nhs.uk/ccg-out-tool/qual-prem/ (accessed on 26 August 2021).




{kind=link}
{kind=link}
{kind=link}
| Number of Learners (% of Sub-Group) | ||
|---|---|---|
| Demographic | Started the Training | Certificate of Completion |
| Region | ||
| North | 15 (12%) | 5 (16%) |
| Midlands | 15 (13%) | 2 (7%) |
| East | 16 (14%) | 2 (7%) |
| London | 36 (30%) | 9 (30%) |
| Southwest | 8 (7%) | 0 (0%) |
| Southeast | 28 (24%) | 12 (40%) |
| Sector | ||
| Hospital | 64 (54%) | 19 (63%) |
| CCG | 25 (21%) | 5 (16%) |
| GP/PCN | 16 (14%) | 2 (7%) |
| Community pharmacy | 10 (8%) | 2 (7%) |
| Community health trust | 3 (3%) | 2 (7%) |
| Years of experience | ||
| <5 years | 31 (26%) | 9 (30%) |
| 5–10 years | 42 (36%) | 9 (30%) |
| >10 years | 45 (38%) | 12 (40%) |
| Workplace roles | ||
| Clinical pharmacist | 62 (53%) | 18 (60%) |
| Antimicrobial pharmacist | 23 (19%) | 4 (13%) |
| Prescribing advisor | 11 (9%) | 2 (7%) |
| Pharmacy manager | 9 (8%) | 3 (10%) |
| Medicines optimisation | 9 (8%) | 3 (10%) |
| Community pharmacist | 4 (3%) | 0 (0%) |
| Total | 118 (100%) | 30 (100%) |
| Quiz Section | Sample | Mean Score (%) | SD | t | p-Value |
|---|---|---|---|---|---|
| All questions | pre | 67.7 | 10.4 | −5.43 | <0.0001 |
| post | 81.1 | 14.4 | |||
| AMS and infection management | pre | 65.0 | 10.3 | −6.09 | <0.0001 |
| post | 79.4 | 14.4 | |||
| Quality improvement and behaviour change | pre | 76.8 | 19.5 | −2.26 | 0.03 |
| post | 86.7 | 19.3 |
| Activity | Number of Learners | |||
|---|---|---|---|---|
| Cohort 1 | Cohort 2 | Cohort 3 | Total (% of 118 Learners) | |
| Identified improvement topic | 19 (16%) | 45 (38%) | 19 (16%) | 83 (70%) |
| Secured stakeholder engagement | 19 (16%) | 25 (21%) | 13 (11%) | 57 (48%) |
| Improved understanding of problem through data collection | 10 (9%) | 4 (3%) | 15 (13%) | 29 (25%) |
| Devised an improvement intervention | 19 (16%) | 34 (29%) | 14 (12%) | 67 (57%) |
| Conducted a test of change | 17 (14%) | 0 (0%) | 5 (4%) | 22 (18%) |
| Promoted improvement initiative | 15 (13%) | 9 (8%) | 12 (10%) | 36 (31%) |
| Provided education to colleagues | 10 (8%) | 1 (1%) | 9 (8%) | 20 (17%) |
| Characteristics of Interventions | Number of Interventions (% of Interventions) | PDSA Cycle Completed (% of Interventions) |
|---|---|---|
| Proposed intervention type: | ||
| Guideline or procedure | 14 (20%) | 4 (6%) |
| Prospective audit and feedback | 11 (16%) | 4 (6%) |
| Use of practice aids | 12 (18%) | 4 (6%) |
| Education and promotion | 13 (19%) | 3 (4%) |
| Prompts and reminders | 8 (12%) | 2 (3%) |
| Restriction | 5 (7%) | 3 (4%) |
| Electronic prescribing functions | 1 (2%) | 1 (2%) |
| Role modelling | 1 (2%) | 1 (2%) |
| Peer group benchmarking | 1 (2%) | 0 (0%) |
| Clinical decision support | 1 (2%) | 0 (0%) |
| Behavioural determinants addressed: | ||
| Capability | 24 (36%) | 5 (7%) |
| Opportunity | 19 (28%) | 9 (13%) |
| Motivation | 9 (13%) | 2 (3%) |
| Combination of capability, opportunity and/or motivation | 15 (23%) | 6 (10%) |
| Total number of interventions | 67 (100%) | 22 (33%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, V.; Ashiru-Oredope, D.; Rosado, H.; Ward, B. Outcomes of a National, Cross-Sector Antimicrobial Stewardship Training Initiative for Pharmacists in England. Pharmacy 2021, 9, 165. https://doi.org/10.3390/pharmacy9040165
Ng V, Ashiru-Oredope D, Rosado H, Ward B. Outcomes of a National, Cross-Sector Antimicrobial Stewardship Training Initiative for Pharmacists in England. Pharmacy. 2021; 9(4):165. https://doi.org/10.3390/pharmacy9040165
Chicago/Turabian StyleNg, Vincent, Diane Ashiru-Oredope, Helena Rosado, and Beth Ward. 2021. "Outcomes of a National, Cross-Sector Antimicrobial Stewardship Training Initiative for Pharmacists in England" Pharmacy 9, no. 4: 165. https://doi.org/10.3390/pharmacy9040165
APA StyleNg, V., Ashiru-Oredope, D., Rosado, H., & Ward, B. (2021). Outcomes of a National, Cross-Sector Antimicrobial Stewardship Training Initiative for Pharmacists in England. Pharmacy, 9(4), 165. https://doi.org/10.3390/pharmacy9040165