Abstract
The long period of tuberculosis treatment causes patients to have a high risk of forgetting or stopping the medication altogether, which increases the risk of oral anti-tuberculosis drug resistance. The patient’s knowledge and perception of the disease affect the patient’s adherence to treatment. This research objective was to determine the impact of educational videos in the local language on the level of knowledge, perception, and adherence of tuberculosis patients in the Regional General Hospital (RSUD) Bangil. This quasi-experimental study design with a one-month follow-up allocated 62 respondents in the intervention group and 60 in the control group. The pre- and post-experiment levels of knowledge and perception were measured with a validated set of questions. Adherence was measured by pill counts. The results showed that the intervention increases the level of knowledge of the intervention group higher than that of the control group (p-value < 0.05) and remained high after one month of follow-up. The perceptions domains that changed after education using Javanese (Ngoko) language videos with the Community Based Interactive Approach (CBIA) method were the timeline, personal control, illness coherence, and emotional representations (p-value < 0.05). More than 95% of respondents in the intervention group take 95% of their pill compared to 58% of respondents in the control group (p-value < 0.05). Utilization of the local languages for design a community-based interactive approach to educate and communicate is important and effective.
1. Introduction
Tuberculosis (TB) is an infectious disease of international concern and is prevalent in Indonesia. In 2050, it is estimated that deaths due to anti-TB drug resistance will be 10 million more than from cancer [1]. The total global losses incurred due to anti-TB drug resistance may reach US$100 trillion. The World Health Organization (WHO) Global Report 2019 states that the total number of TB cases identified in Indonesia rose from 331,703 in 2015 to 563,879 in 2018 (+70%); a 28% increase happened between 2017 and 2018 [2]. In 2016, 110,000 people, or 42 per 100,000 population, died of TB of which 32,000 (12 per 100,000 population) were caused by Multi-Drug-Resistant Tuberculosis (MDR-TB) [3]. Pasuruan Regency is among the five cities/districts with the highest number of TB cases in East Java. In 2013, the number of TB cases in Pasuruan Regency was 964, which declined to 886 cases in 2014 and rose to 1693 cases in 2015 [4]. In the Regional General Hospital (RSUD) Bangil, there were 100 tuberculosis outpatients at the pulmonary clinic each month from January to June 2018. If the number of tuberculosis patients continues to rise, Indonesia would fail to achieve the TB control targets of the 2020–2024 National Medium-Term Development Plan (RPJMN), Millennium Development Goals (MDGs), and Sustainable Development Goals (SDGs).
Tuberculosis treatment lasts at least 6 months, depending on the clinical presentation in each patient, which causes patients to be at high risk of forgetting to take medication or dropping out of treatment. Medication non-adherence will prolong therapy duration, and increase the risk of drug resistance, morbidity, and mortality [5,6]. Resistance cannot be eliminated but can be controlled with the appropriate use of anti-TB drugs. Furthauer et al. (2013) argued that factors causing non-adherence include patients’ lack of knowledge about their health, the patient’s weak relationship with medical personnel, and the drugs’ side effects [7].
According to Regulation of the Minister of Health No. 72 of 2016, one of the roles of clinical pharmacists in controlling anti-TB drug resistance is to provide education to patients and the public about tuberculosis and the judicious use of anti-TB drugs, in the hope of increasing patients’ knowledge, which in turn shapes correct perceptions about the disease, encourages adherence and controls the number of drug resistance cases [8]. Videos in the Javanese (Ngoko) language were chosen as an instrument because a person can absorb information best and highest through sight and hearing senses; video educational material more effective than text-only [9]. A video educational tool was effective for increasing the level of outpatients’ knowledge [10,11] and remained significant after three months [10]. The study was conducted at the Regional General Hospital (RSUD) Bangil because the hospital is a referral hospital in Pasuruan Regency with a high number of TB cases. Secondary data from Patient and Family Education in the pulmonary clinic of the Regional General Hospital (RSUD) Bangil in October 2017 showed educational achievements by the health personnel were not yet optimal. This was confirmed by the pharmacist at the outpatient pharmacy, who reported that many tuberculosis patients who were following treatments at the Regional General Hospital (RSUD) Bangil did not adhere to the scheduled patients’ routine visits and no record was written on the pharmacy’s education register. This study aimed to assess the impact of a local language educational video on the level of knowledge, perception, and adherence of tuberculosis patients in the Regional General Hospital (RSUD) Bangil.
2. Materials and Methods
Before the Javanese (Ngoko) videos were created, the researcher performed a needs assessment and education plan for respondents so that contents could be suited to the needs of tuberculosis outpatients in the Regional General Hospital (RSUD) Bangil. The Javanese (Ngoko) language was adopted because the majority of patients use the Javanese (Ngoko) language daily. The design of this research was quasi-experimental with a control group and an intervention group. The control group and the intervention group were followed for 30 days. Data collection began by screening the medical records of prospective respondents. Prospective respondents who fulfilled the inclusion and exclusion criteria were visited, and the researcher explained the purpose of the study along with giving an informed consent form to be signed by the respondents as evidence of volunteerism. Respondents who were willing to take part in the study were allocated into a control group and intervention group with a simple random sample using a lottery method. Afterward, on day-1 and 30, respondents were given questionnaires to test their levels of knowledge and perception (Figure 1). Questions on knowledge level were adapted from several studies [12,13,14,15], guideline published by Ministry of Health Indonesia [16,17] and WHO [18]. The expected achievements on knowledge level were based on Bloom’s Revised Cognitive Domain [19,20], which were knowing, understanding, and applying. Questions on perception were adapted from The Revised Illness Perception Questionnaire [21]. The expected result was a change from negative perception to positive perception. The same questions (Appendix A) were given twice to the control group on day 1 and day 30, and three times to the intervention group on day 1 (before and after being provided with education) and day 30. The researcher performed tests on knowledge and perception during patients’ routine visits at Bangil District Public Hospital. An educational video in the local language about tuberculosis disease, anti-TB drugs administration, and their adverse drug events was given to educate the community (TB outpatients) in a small discussion group, named Community-Based Interactive Approach (CBIA), at the pulmonary clinic of the Regional General Hospital (RSUD) Bangil.
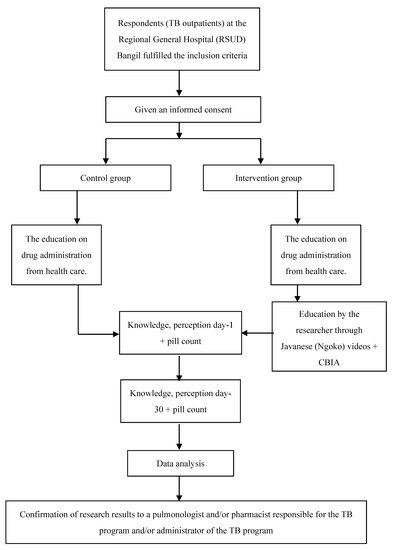
Figure 1.
The Scheme of Research Work.
2.1. Respondents
Data collection for the study sample was performed from October to December 2018 at the pulmonary clinic of the Regional General Hospital (RSUD) Bangil, Pasuruan Regency (Figure 1). The recruitment flow of TB respondents can be seen in Figure 2. Inclusion criteria were tuberculosis patients >14 years who received anti-TB drug category one and two, while exclusion criteria were tuberculosis patients who were currently following the Directly Observed Treatment Short-Course (DOTS) program, patients diagnosed with schizophrenia, blindness, or deafness.
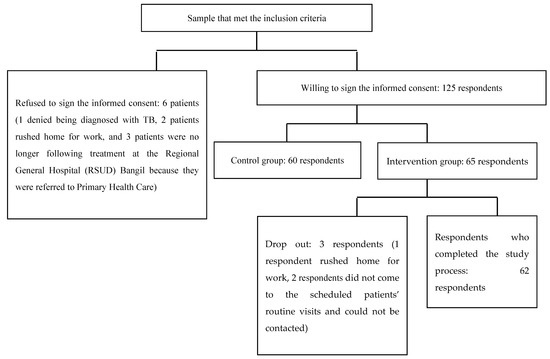
Figure 2.
The Flow of TB Respondents’ Recruitment at the Pulmonary Outpatient Clinic in the Regional General Hospital (RSUD) Bangil.
Education was given by the researcher to the intervention group through videos in Javanese (Ngoko) language with a CBIA approach upon the completion of their clinic visit on day 1. The educational video (CBIA) duration was six minutes. It covered information about tuberculosis disease, tuberculosis treatment (including duration, the risk of drug resistance, and adverse drug events), a reminder system, and non-pharmacology aspects. The control group received standard care, education on drug administration from health care. CBIA was done through small group discussions between 6 and 8 respondents; each group was accompanied by a counselor who facilitated the discussions. Respondents were encouraged to be more active in expressing opinions and asking questions of the informant about the discussion material, and the outcome of these small group discussions was ultimately presented to all groups. During the implementation, every CBIA education session (the control group and the intervention group), was assisted by a group of 3–4 people, comprising of a physician, pharmacist, pharmacy student, and/or medical student who had previously been briefed. To anticipate respondents forgetting the educational material, each respondent was provided with videos on his or her mobile phone. The videos were transferred from the researcher to the respondent’s mobile devices (with Bluetooth, Share It, WhatsApp, or LINE platform).
To understand the effect of education on adherence, adherence to treatment in the control group and intervention group was measured by pill counts on day-1 and 30; the number of drugs taken by the patients with counting the remaining units (drugs consumed) divided by the number of drugs prescribed (prescribed drugs). The pill count calculation formula is as follows:
Pill count = Σ Drugs consumed/Σ Prescribed drugs × 100%
Adherence to medications on day-1 was assessed by looking at the number of drugs and medication instructions, attendance at the previously scheduled appointment as specified on the patient’s identity card, Hospital Management Information System, and/or medication collection card. On day-1, the patient’s medication was examined and recorded. Meanwhile, adherence to medications from day-1 to day-30 was assessed by making records on the number of drugs received by the respondent up to day-30; the remaining medications were counted by the researcher on day-30. A day before the scheduled patients’ routine visits on day-30, the researcher reminded respondents via phone calls, as well as chats on WhatsApp or LINE, to bring their medications. If the respondent did not come to the scheduled appointment, the researcher would contact them by phone, as well as chat on WhatsApp or LINE. Nonetheless, if the respondent was still unable to be reached and did not attend the patients’ routine visits, he or she was moved to the drop-out category. Respondents were considered to have a high level of adherence to medications if the pill count was ≥95%, and low if it was <95% [22]. The study results were then reported to a pulmonologist and/or pharmacist responsible for the TB program and/or administrator of the TB program, to inform and ask for suggestions relating to the results.
2.2. Data Validity Test
A needs assessment and education planning were carried out through a preliminary study in 30 respondents who met the inclusion and exclusion criteria (excluding the research sample). Accordingly, statements or terms that were unclear to the respondents were discussed together. A difficulty index analysis was used for knowledge questions. Questions number 4 (question-related to tuberculosis disease) and 7 (question-related to anti-tuberculosis drugs administration) were considered as ‘easy’ within the difficulty index (at least 70% of respondents answer it correctly), while questions number 1, 3, 5, 6, 9, 10, 11, and 12 belong to the ‘moderate’ group (40–60% of respondents answer it correctly). Meanwhile, questions number 2 (question-related to tuberculosis disease) and 8 (question-related to anti-tuberculosis drugs administration) were considered as ‘difficult’ within the difficulty index (only 30% of respondents answer it correctly). Construct validation was done on perception. A questionnaire regarding perception consisted of 15 questions grouped into 7 domains: timeline, illness coherence, consequences, treatment control, personal control, timeline cyclical, and emotional representations. All perception questions were valid, as the product-moment correlation coefficient was above 0.3, and reliable because the Cronbach’s α test was 0.791. The Javanese (Ngoko) language on the video’s script was proofread with experts and validated by tuberculosis patients who were not respondents in the research.
2.3. Statistical Analysis
To compare the level of knowledge and the level of perception among the control group and intervention group, the Mann–Whitney test was used. The Wilcoxon Signed-Rank test was used to compare the level of knowledge and the level of perception per domain in each group. The level of adherence to medications in the control group and the intervention group were compared using the chi-square test, as were the relationships between respondents’ demographic factors and the level of adherence to medications in the control group and the intervention group.
2.4. Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Politeknik Kesehatan Kementerian Kesehatan Surabaya (the Health Research Ethics Commission of the Health Polytechnic of the Ministry of Health Surabaya), Number 025/S/KEPK/V/2017. This study acquired a research permit from Badan Kesatuan Bangsa dan Politik (the National Unity and Politics Agency) Number 072/940/424.104/SUR/RES/2018 and the Regional General Hospital (RSUD) Bangil Number 445.1/2175/424.202/2018.
3. Results
The characteristic demographic patients in the intervention group were similar to patients in the control group (Table 1). There was a significant difference between the knowledge level of the control group and that of the intervention group in the knowledge of tuberculosis disease, anti-tuberculosis drug administration, and anti-tuberculosis drug adverse drug events, with a p-value of less than 0.05 (Table 2). The consistency of improved knowledge was maintained for one month after the intervention.

Table 1.
Baseline characteristic.
Table 2.
Average Score of Respondent’s Knowledge and Perception after intervention, day-30.
Perception domains that were changed due to education through Javanese (Ngoko) videos with the CBIA method were a timeline, personal control, illness coherence, and emotional representations (p-value < 0.05) (Table 2). Perception domains that did not change after education was given were the consequence, treatment control, and timeline cyclical (p-value > 0.05).
With regards to adherence, additional education from the researcher increased the number of respondents who take 95% of their pill in the intervention group (37% increases) three times higher than in the number of the respondent in the control group (12% increases) (Table 3). There was no relationship found between respondents’ demographic factors (gender, age, level of education, and occupation) and the level of adherence to medications in the control group and the intervention group (p-value > 0.05) but this may be because the group size was modest.
Table 3.
Percentage of respondents’ adherence after a 30-days follow-up.
4. Discussion
Many factors influenced the successful delivery of this education. First, respondents had a strong desire to recover, and this heightened their need to obtain correct information about the disease. Second, placing the video on each respondent’s mobile phone enabled patients to watch the videos again if they had forgotten. Other factors that may have affected knowledge include education level, information source, economic level, age, and occupation. An education increases adherence [23]. There is a positive relationship between knowledge level and adherence to taking anti-TB drugs [24,25,26,27]. Patients with a high level of knowledge had a greater chance of being adherent to medications compared to those having a low level of knowledge. A survey by Wandwalo and Morkve (2000) with regards to patients’ knowledge about tuberculosis revealed that only 43.9% of patients knew the cause of tuberculosis, 54.9% of patients knew how Mycobacterium tuberculosis bacteria are transmitted, 82% of patients assumed that tuberculosis disease could be cured, 44.3% thought that tuberculosis disease could be prevented, 50.7% of patients knew the duration of tuberculosis treatment, and 29% of patients knew the side effects of anti-TB drugs [28].
Knowledge influences perception [29,30,31,32]. Perception about illness is the patient’s experience with the disease suffered and that experience will be applied to his or her condition [33,34,35]. There is a positive correlation between perception and adherence to taking anti-TB drugs [36,37,38,39,40], and Pasek et al. (2013) found that 94% of patients with positive perception adhere to their treatment, whereas only 13% of patients with negative perception adhere to their treatment. There are 33 out of 40 tuberculosis patients (82.5%) who had a positive perception and 27 out of 40 tuberculosis patients (67.5%) had good knowledge [41].
A greater increase of respondent’s knowledge and perception in this study not only because of using a video but also because of using the local language. Language concordance will improve patient understanding, trust in the healthcare, and adherence to their treatment [42]. The implementation limitation of this study was not every healthcare had local language proficiency.
5. Conclusions
The use of videos with the local language, Javanese (Ngoko), as an educational tool effective increasing knowledge of tuberculosis disease, anti-TB drug administration, and anti-TB drug adverse drug events; understanding, and implicating as described in Bloom’s taxonomy; turning negative perceptions of timeline, personal control, illness coherence, and emotional representations into positives perceptions; and increasing the adherence to tuberculosis medications.
Author Contributions
Conceptualization, F.H. and R.Y.; methodology, F.H. and A.; software, Y.M.; validation, F.H., Y.M., and A.; formal analysis, Y.M., F.H., and R.A.; investigation, Y.M.; resources, A.; data curation, Y.M.; writing—original draft preparation, F.H.; writing—review and editing, F.H. and R.A.; supervision, R.A. and R.Y.; project administration, R.Y.; funding acquisition, R.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Ministry of Research, Technology, and Higher Education of the Republic of Indonesia, grant number No. 036/SP-Lit/LPPM-01/RistekBRIN/Mono/FF/III/2020.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to restrictions (privacy).
Acknowledgments
The authors would like to thank the Director of the Private Hospital for allowing us to research their hospital. We would like to thank David Scott, Pharmacy Department, the Cardiff University, UK for reviewing, editing, and proofreading the manuscript.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Appendix A
Knowledge questionnaire.
SOAL PENGETAHUAN TUBERKULOSIS (TBC)
Penyakit TBC (total poin = 100)
- TBC iku mlebu penyakit nular opo gak?
- ☐
- Lara sing nular (poin = 1)
- ☐
- Dudu lara sing nular (poin = 0)
- ☐
- Gak ngerti utawa bingung (poin = 0)
- Lara TBC iki sebabe opo?
- ☐
- Bakteri Mycobacterium tuberculosis (poin = 1)
- ☐
- Jamur (poin = 0)
- ☐
- Virus (poin = 0)
- ☐
- Parasit (poin = 0)
- ☐
- Gak ngerti utawa bingung (poin = 0)
- Tondo-tondo TBC iku opo? Tau ngalami dewe? ...... Sak piro suwene? .......(lek jawaban bener ≥3 = poin 1; jawaban bener <3 = 0)
- ☐
- Metu kringet adem lek bengi
- ☐
- Lemah, lemes, lepok
- ☐
- Ambekan sesek lan dodo lara koyok disuduk
- ☐
- Panas sak wulan luwih
- ☐
- Bobote mudhun
- ☐
- Nafsu mangan mudun
- ☐
- Watuk riak’en rong minggu luwih lan onok getih e
- Coro TBC nular yo opo? (lek jawaban bener ≥2 = poin 1; jawaban bener <2 = 0)
- ☐
- Watuk ☐ Anginlek ☐ Wahing ☐ Ngidu ☐ Nafas
Coro Ngombe OAT (total poin = 100)
- Biasane sampeyan cara ngombe obate yo opo? (lek jawaban bener ≥1 = poin 1)
- ☐
- Sak-elinge
- ☐
- Diombe lek wayahe watuk tok, utawa panas tok
- ☐
- Isuk utawa bengi, sak jam sadurunge mangan (bener)
- ☐
- Isuk utawa bengi, rong jam sak wise mangan (bener)
- ☐
- Pas waktune utawa tetep waktune utawa pancet waktune ben dino e (bener)
- ☐
- Gak ngerti utawa lali utawa bingung
- Sampeyan tau lali ngombe obat TBC? (lek jawaban bener ≥1 = poin 1)
- ☐
- Tau →Langsung ngombe dobel obat e saka biasae
- ☐
- Tau →Langsung ngombe pas eling (bener)
- ☐
- Tau →Kandha dokter (bener)
- ☐
- Tau →Gak ngombe obat sampe wayahe kontrol maneh
- ☐
- Gak tau lali (bener)
- ☐
- Bingung
Lek tau lali, opo sing sampeyan lakukno ben gak gampang lali? (data deskriptif) - Jare dokter, sak piro suwene sampeyan kudu ngombe obat TBC iki? (jawaban bener poin = 1)
- ☐
- Rong minggu luwih (poin = 0)
- ☐
- 1 wulan (poin = 0)
- ☐
- 2 wulan (poin = 0)
- ☐
- 3 wulan (poin = 0)
- ☐
- 6 wulan utawa luwih tergantung penyakite (poin = 1)
- Opo ae macem e obat TBC sing sampeyan ombe? ngerti jeneng e? (lek jawaban bener ≥2 = poin 1; jawaban bener <2 = 0)
- ☐
- Isoniazid (INH) ☐ Pirazinamid
- ☐
- Rifampisin ☐ Streptomisin injeksi
- ☐
- Etambutol
Efek Samping (total poin = 100)
- Tondo-tondo opo ae sing perlu diwaspadai marine ngombe obat TBC? (lek jawaban bener ≥2 = poin 1; jawaban bener <2 = 0)
- ☐
- Uyuh e abang ☐lara weteng ☐gringgingen
- ☐
- muneg-muneg lan muntah ☐ora nafsu mangan ☐nyeri sendi
- ☐
- budeg ☐gatel-gatel lan abang-abang nde kulit
- ☐
- kuning ☐mripat e bureng
- Opo sing sampeyan lakukno lek onok keluhan koyok muneg-muneg lan muntah, lara weteng, gak nafsu mangan marine ngombe obat? (jawaban bener 2 = poin 1; jawaban bener <2 = 0)
- ☐
- Mandeg ngombe obat, wes gak gelem ngombe obat maneh sateruse
- ☐
- Ganti ngombe obat herbal
- ☐
- Ganti obat liyane ora kandha dokter
- ☐
- Diombe isuk utawa bengi sakwise mangan (bener)
- ☐
- Kandha dokter (bener)
- Lek uyuh e abang sakwise ngombe obat, sampeyan ngerti penyebabe obat opo?
- ☐
- Rifampisin (poin = 1)
- ☐
- Isoniazid (poin = 0)
- ☐
- Etambutol (poin = 0)
- ☐
- Pirazinamid (poin = 0)
- ☐
- Streptomisin (poin = 0)
- Opo akibat e lek ngombe obat TBC gak teratur? (lek jawaban bener ≥2 = poin 1; jawaban bener <2 = 0)
- ☐
- Ngulang pengobatane utawa tambah suwe waras e (bener)
- ☐
- Obat e gak mempan maneh (bener)
- ☐
- Penyakit e tambah akeh (bener)
- ☐
- Gak ngerti utawa bingung
References
- de Kraker, M.E.A.; Stewardson, A.J.; Harbarth, S. Will 10 million people die a year due to antimicrobial resistance by 2050? PLoS Med. 2016, 13, e1002184. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report: Executive Summary 2019; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/tb/publications/global_report/GraphicExecutiveSummary.pdf (accessed on 12 April 2021).
- Surya, A.; Setyaningsih, B.; Nasution, H.S.; Parwati, C.G.; Yuzwar, Y.E.; Osberg, M.; Hanson, C.L.; Hymoff, A.; Mingkwan, P.; Makayova, J.; et al. Quality tuberculosis care in Indonesia: Using Patient Pathway Analysis to optimize public–private collaboration. J. Infect. Dis. 2017, 216, S724–S732. (accessed on 29 August 2019). [Google Scholar] [CrossRef] [PubMed]
- Pasuruan Regency Health Office. Profil Kesehatan Kabupaten Pasuruan Tahun. 2015. Available online: http://www.depkes.go.id/resources/download/profil/PROFIL_KAB_KOTA_2015/3514_Jatim_Kab_Pasuruan_2015.pdf (accessed on 29 August 2019).
- Pradipta, I.S.; Houtsma, D.; van Boven, J.F.M.; Alffenaar, J.-W.C.; Hak, E. Interventions to improve medication adherence in tuberculosis patients: A systematic review of randomized controlled studies. NPJ Prim. Care Respir. Med. 2020, 30, 21. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, L.A.; Zamzami, M.; Aldin, S.; Pazdirek, J. Clinical consequences of non-compliance with directly observed therapy short course (DOTS): Story of a recurrent defaulter. Int. J. Mycobacteriol. 2012, 1, 99–103. [Google Scholar] [CrossRef]
- Fürthauer, J.; Flamm, M.; Sönnichsen, A. Patient and physician related factors of adherence to evidence based guidelines in diabetes mellitus type 2, cardiovascular disease and prevention: A cross sectional study. BMC Fam. Pract. 2013, 14, 47. [Google Scholar] [CrossRef]
- Indonesian Ministry of Health (IMOH). Peraturan Menteri Kesehatan Republik Indonesia Nomor 72 Tahun 2016 tentang Standar Pelayanan Kefarmasian di Rumah Sakit; Direktorat Jenderal Bina Kefarmasian dan Alat–Kesehatan Kementerian Kesehatan RI: Jakarta, Indonesia, 2016; Available online: http://farmalkes.kemkes.go.id/?wpdmact=process&did=NDA5LmhvdGxpbms= (accessed on 29 August 2019).
- Clark, R.C.; Mayer, R.E. E-Learning and the Science of Instruction: Proven Guidelines for Consumers and Designers of Multimedia Learning, 4th ed.; John Wiley &Sons Inc: Hoboken, NJ, USA, 2016. [Google Scholar]
- Hendricks, M.; Nair, G.; Staunton, C.; Pather, M.; Garrett, N.; Baadjies, D.; Kidd, M.; Moodley, K. Impact of an educational video as a consent tool on knowledge about cure research among patients and caregivers at HIV clinics in South Africa. J. Virus Erad. 2018, 4, 103–107. [Google Scholar] [CrossRef]
- Al Owaifeer, A.M.; Alrefaie, S.M.; Alsawah, Z.M.; Al Taisan, A.A.; Mousa, A.; Ahmad, S.I. The effect of a short animated educational video on knowledge among glaucoma patients. Clin. Ophthalmol. 2018, 12, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Wieland, M.L.; Nelson, J.; Palmer, T.; O’Hara, C.; Weis, J.A.; Nigron, J.A.; Sia, I.G. Evaluation of a tuberculosis education video among immigrants and refugees at an adult education center: A community-based participatory approach. J. Health Commun. 2013, 18, 343–353. [Google Scholar] [CrossRef]
- Reeves, H.; Grandjean Lapierre, S.; Razafindrina, K.; Andriamiadanarivo, A.; Rakotosamimanana, N.; Razafindranaivo, T.; Seimon, T.; Blalock, B.; Bello-Bravo, J.; Pittendrigh, B.; et al. Evaluating the use of educational videos to support the tuberculosis care cascade in remote Madagascar. Int. J. Tuberc. Lung Dis. 2020, 24, 28–35. [Google Scholar] [CrossRef]
- Wilson, J.W.; Ramos, J.G.; Castillo, F.; Castellanos, E.F.; Escalante, P. Tuberculosis patient and family education through videography in El Salvador. J. Clin. Tuberc. Other Mycobact. Dis. 2016, 4, 14–20. [Google Scholar] [CrossRef]
- Ramadhany, S.; Achmad, H.; Singgih, M.F.; Ramadhany, Y.F.; Inayah, N.H.; Mutmainnah, N. A review: Knowledge and attitude of society toward tuberculosis disease in Soppeng District. Sys. Rev. Pharm. 2020, 11, 57–62. [Google Scholar]
- Indonesian Ministry of Health (IMOH). Keputusan Menteri Kesehatan Republik Indonesia Nomor HK.01.07/MENKES/755/2019 tentang Pedoman Nasional Pelayanan KedokteranTata Laksana Tuberkulosis; Direktorat Jenderal Bina Kefarmasian dan Alat–Kesehatan Kementerian Kesehatan RI: Jakarta, Indonesia, 2019. [Google Scholar]
- Departemen Kesehatan Republik Indonesia. Pedoman Nasional Penanggulangan Tuberkulosis, 2nd ed.; Departemen Kesehatan Republik Indonesia: Jakarta, Indonesia, 2007.
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Adams, N.E. Bloom’s taxonomy of cognitive learning objectives. J. Med. Libr. Assoc. 2015, 103, 152–153. [Google Scholar] [CrossRef] [PubMed]
- Orgill, B.D.; Nolin, J. Learning Taxonomies in Medical Simulation; StatPearls Publishing: Treasure Islands, FL, USA, 2021; Available online: https://www.ncbi.nlm.nih.gov/books/NBK559109/ (accessed on 21 January 2021).
- Moss-Morris, R.; Petrie, J.W.K.; Horne, R.; Cameron, L.; Buick, D. The revised illness perception questionnaire (IPQ-R). Psychol. Health 2002, 17, 1–16. [Google Scholar] [CrossRef]
- Achappa, B.; Madi, D.; Bhaskaran, U.; Ramapuram, J.T.; Rao, S.; Mahalingam, S. Adherence to antiretroviral therapy among people living with HIV. N. Am. J. Med. Sci. 2013, 5, 220–223. [Google Scholar]
- Alipanah, N.; Jarlsberg, L.; Miller, C.; Linh, N.N.; Falzon, D.; Jaramillo, E.; Nahid, P. Adherence interventions and outcomes of tuberculosis treatment: A systematic review and meta-analysis of trials and observational studies. PLoS Med. 2018, 15, e1002595. [Google Scholar] [CrossRef]
- Sukartini, T.; Widianingrum, T.R.; Yasmara, D. The relationship of knowledge and motivation with anti tuberculosis drugs compliance in tuberculosis patients. Syst. Rev. Pharm. 2020, 11, 603–606. [Google Scholar]
- Nezenega, Z.S.; Perimal-Lewis, L.; Maeder, A.J. Factors influencing patient adherence to tuberculosis treatment in Ethiopia: A literature review. Int. J. Environ. Res. Public Health 2020, 17, 5626. [Google Scholar] [CrossRef]
- Swarjana, K.D.; Sukartini, T.; Makhfudli, M. Level of attitude, medication adherence, and quality of life among patients with tuberculosis. J. Nurs. Healthc. Res. 2019, 2, 334–339. [Google Scholar]
- Tesfahuneygn, G.; Medhin, G.; Legesse, M. Adherence to anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC Res. Notes 2015, 8, 503. [Google Scholar] [CrossRef] [PubMed]
- Wandwalo, E.R.; Morkve, O. Knowledge of disease and treatment among tuberculosis patients in Mwanza, Tanzania. Int. J. Tuberc. Lung Dis. 2000, 4, 1041–1046. [Google Scholar] [PubMed]
- Ramsey, R.; Hamilton, A.F. How does your own knowledge influence the perception of another person’s action in the human brain? Soc. Cogn. Affect. Neurosci. 2012, 7, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Min, J.; Chung, C.; Jung, S.S.; Park, H.K.; Lee, S.-S.; Lee, K.M. Understanding illness perception in pulmonary tuberculosis patients: One step towards patient-centered care. PLoS ONE 2019, 14, e0218106. [Google Scholar] [CrossRef]
- Putera, I.; Pakasi, T.A.; Karyadi, E. Knowledge and perception of tuberculosis and the risk to become treatment default among newly diagnosed pulmonary tuberculosis patients treated in primary health care, East Nusa Tenggara: A retrospective study. BMC Res. Notes 2015, 8, 238. [Google Scholar] [CrossRef] [PubMed]
- Nyasulu, P.; Sikwese, S.; Chirwa, T.; Makanjee, C.; Mmanga, M.; Babalola, J.O.; Mpunga, J.; Banda, H.T.; Muula, A.S.; Munthali, A.C. Knowledge, beliefs, and perceptions of tuberculosis among community members in Ntcheu district, Malawi. J. Multidiscip. Healthc. 2018, 11, 375–389. [Google Scholar] [CrossRef]
- Mohammed, S.; Nagla, S.; Morten, S.; Asma, E.; Arja, A. Illness perceptions and quality of life among tuberculosis patients in Gezira, Sudan. Afr. Health Sci. 2015, 15, 385–393. [Google Scholar] [CrossRef]
- Jamaludin, T.S.S.; Ismail, N.; Saidi, S. Knowledge, awareness, and perception towards tuberculosis disease among International Islamic University Malaysia Kuantan students. Enferm. Clin. 2019, 29, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Dodor, E.A. The feelings and experiences of patients with tuberculosis in the Sekondi-Takoradi Metropolitan District: Implications for TB Control Efforts. Ghana Med. J. 2012, 46, 211–218. [Google Scholar] [PubMed]
- Zainal, S.M.; Sapar; Syafruddin; Irwandy. The effect of patients’ perception about tuberculosis (TB) against treatment compliance. Enferm. Clin. 2020, 30, 416–419. [Google Scholar] [CrossRef]
- van den Boogaard, J.; Msoka, E.; Homfray, M.; Kibiki, G.S.; Heldens, J.J.H.M.; Felling, A.J.A.; Aarnoutse, R.E. An exploration of patient perceptions of adherence to tuberculosis treatment in Tanzania. Qual. Health Res. 2012, 22, 835–845. [Google Scholar] [CrossRef]
- Diesty, U.A.F.; Tjekyan, R.M.S.; Zulkarnain, M. Medical compliance determinants for tuberculosis patients in Palembang. J. Ilmu Kesehat. Masy. 2020, 11, 272–284. [Google Scholar] [CrossRef]
- Lestari, A.P.; Fathana, P.B.; Affarah, W.S. The correlations of knowledge, attitude and practice with compliance in treatment of pulmonary tuberculosis patients in Puskesmas Cakranegara. J. Biol. Trop. 2021, 21, 65–71. [Google Scholar]
- Tang, Y.; Zhao, M.; Wang, Y.; Gong, Y.; Yin, X.; Zhao, A.; Zheng, J.; Liu, Z.; Jian, X.; Wang, W.; et al. Non-adherence to anti-tuberculosis treatment among internal migrants with pulmonary tuberculosis in Shenzhen, China: A cross-sectionalstudy. BMC Public Health 2015, 15, 474. [Google Scholar] [CrossRef]
- Pasek, M.S.; Suryani, N.; Murdani, P. Hubungan persepsi dan tingkat pengetahuan penderita tuberkulosis dengan kepatuhan pengobatan di wilayah kerja puskesmas buleleng I. J. Magister Kedokt. Kel. 2013, 1, 14–23. Available online: https://media.neliti.com/media/publications/13494-ID-hubungan-persepsi-dan-tingkat-pengetahuan-penderita-tuberkulosis-dengan-kepatuha.pdf (accessed on 29 August 2019).
- Molina, R.L.; Kasper, J. The power of language-concordant care: A call to action for medical schools. BMC Med. Educ. 2019, 19, 378. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).