Managing Allergic Rhinitis in the Pharmacy: An ARIA Guide for Implementation in Practice

 ,
, 

 , ,
, , 

Abstract
1. Introduction
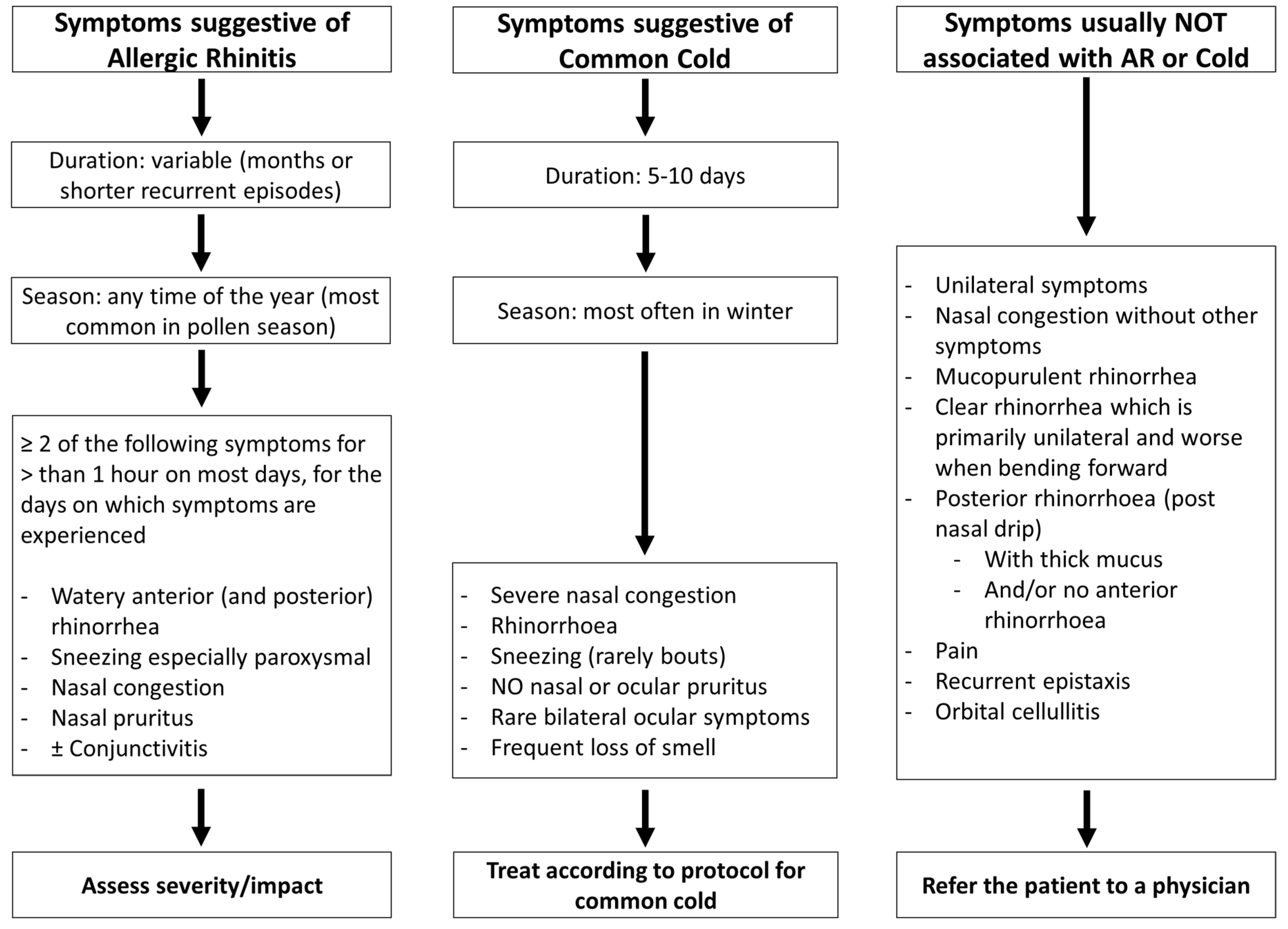
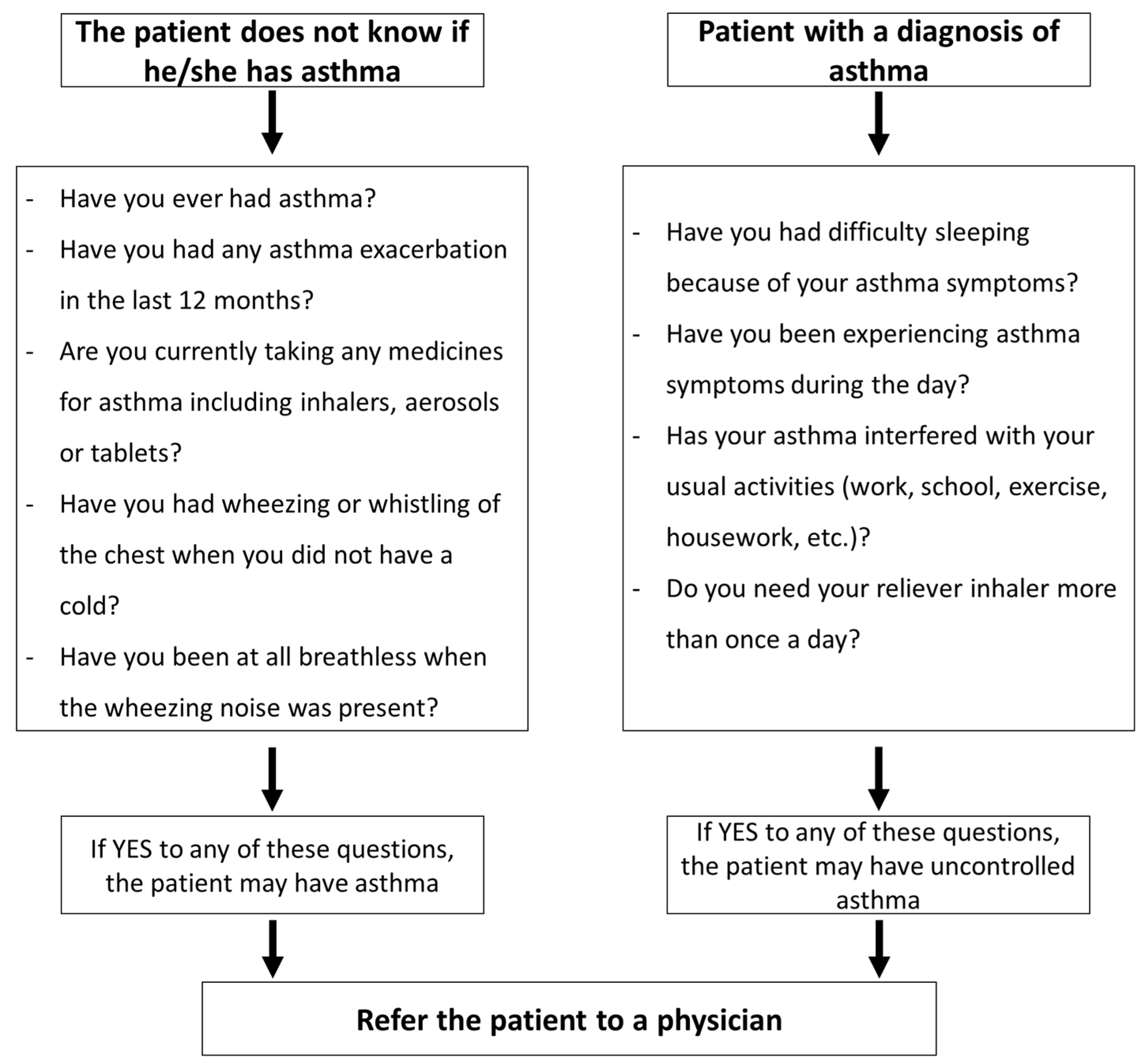
2. Is this Allergic Rhinitis?
3. Assessing the Severity of Allergic Rhinitis: Tools for the Pharmacist
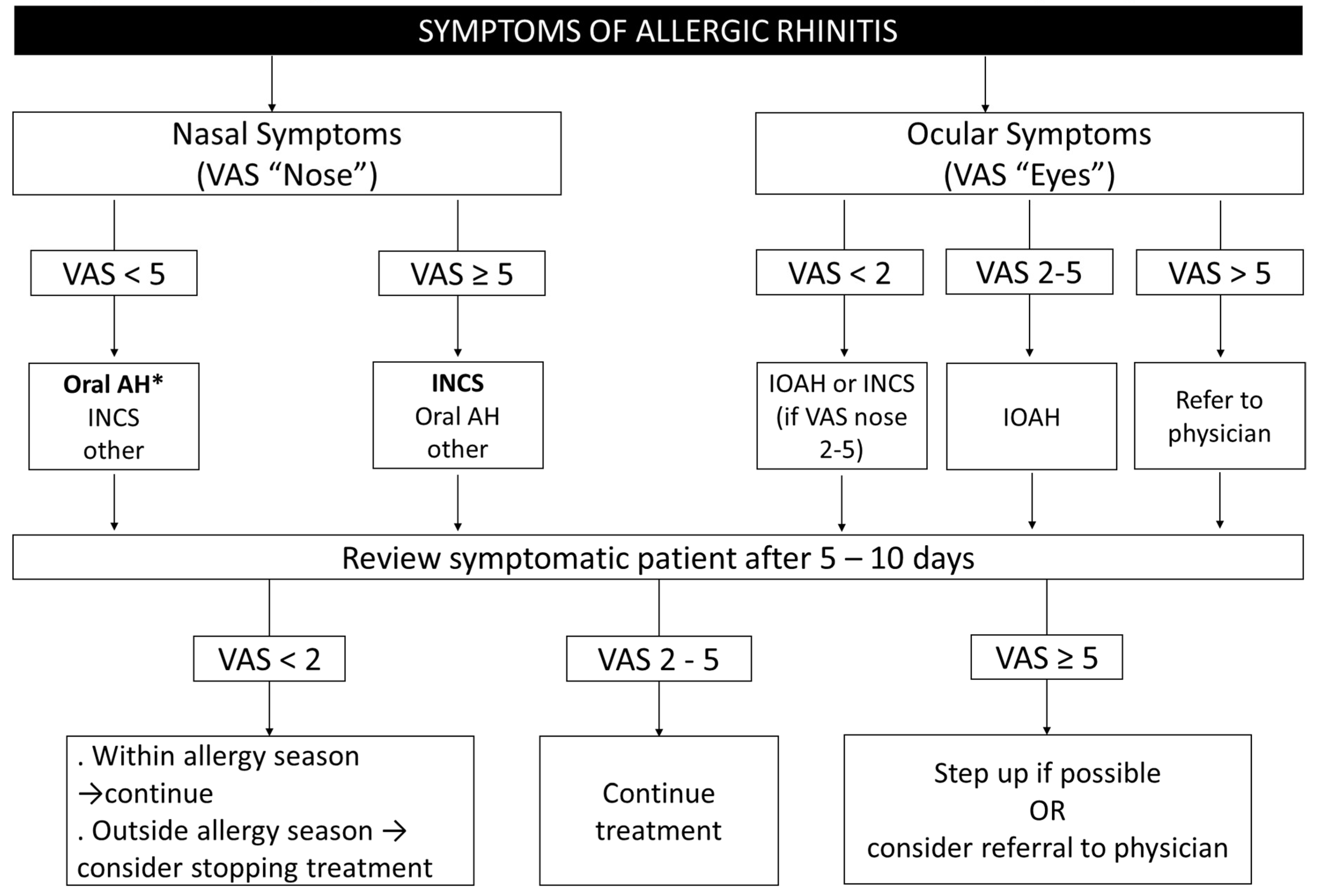
4. Treatment of Allergic Rhinitis in the Pharmacy
5. Counselling on Possible Side Effects of Medications
6. Patient’s Self-Management of AR and Patient Support
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mims, J.W. Epidemiology of allergic rhinitis. Int. Forum Allergy Rhinol. 2014, 4, S18–S20. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Blaiss, M.S.; Naclerio, R.M.; Stoloff, S.W.; Derebery, M.J.; Nelson, H.S.; Boyle, J.M.; Wingertzahn, M.A. Burden of allergic rhinitis: Allergies in America, Latin America, and Asia-Pacific adult surveys. Allergy Asthma Proc. 2012, 33, S113–S141. [Google Scholar] [CrossRef]
- Baptist, A.P.; Nyenhuis, S. Rhinitis in the elderly. Immunol. Allergy Clin. N. Am. 2016, 36, 343–357. [Google Scholar] [CrossRef]
- Hill, D.A.; Grundmeier, R.W.; Ram, G.; Spergel, J.M. The epidemiologic characteristics of healthcare provider-diagnosed eczema, asthma, allergic rhinitis, and food allergy in children: A retrospective cohort study. BMC Pediatr. 2016, 16, 133. [Google Scholar] [CrossRef] [PubMed]
- Brozek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines—2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, O.; Vinnikov, D.; Blanc, P.D.; Agache, I.; Bachert, C.; Bewick, M.; Cardell, L.O.; Cullinan, P.; Demoly, P.; Descatha, A.; et al. Impact of rhinitis on work productivity: A systematic review. J. Allergy Clin. Immunol. Pract. 2018, 6, 1274–1286.e1279. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Cano, R.; Ribo, P.; Araujo, G.; Giralt, E.; Sanchez-Lopez, J.; Valero, A. Severity of allergic rhinitis impacts sleep and anxiety: Results from a large Spanish cohort. Clin. Transl. Allergy 2018, 8, 23. [Google Scholar] [CrossRef]
- Hoehle, L.P.; Speth, M.M.; Phillips, K.M.; Gaudin, R.A.; Caradonna, D.S.; Gray, S.T.; Sedaghat, A.R. Association between symptoms of allergic rhinitis with decreased general health-related quality of life. Am. J. Rhinol. Allergy 2017, 31, 235–239. [Google Scholar] [CrossRef]
- Meltzer, E.O. Allergic rhinitis: Burden of illness, quality of life, comorbidities, and control. Immunol. Allergy Clin. N. Am. 2016, 36, 235–248. [Google Scholar] [CrossRef]
- Bachert, C.; Bousquet, J.; Hellings, P. Rapid onset of action and reduced nasal hyperreactivity: New targets in allergic rhinitis management. Clin. Transl. Allergy 2018, 8, 25. [Google Scholar] [CrossRef]
- Cvetkovski, B.; Kritikos, V.; Yan, K.; Bosnic-Anticevich, S. Tell me about your hay fever: A qualitative investigation of allergic rhinitis management from the perspective of the patient. NPJ Prim. Care Respir. Med. 2018, 28, 3. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Scadding, G. Is reliance on self-medication and pharmacy care adequate for rhinitis patients? Int. J. Clin. Pract. 2009, 63, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, B.L.; Abdulnour, S.; O’Dell, M.; Kyle, T.K. Understanding the role of the healthcare professional in patient self-management of allergic rhinitis. SAGE Open Med. 2015, 3, 2050312115595822. [Google Scholar] [CrossRef] [PubMed]
- Bosnic-Anticevich, S.; Kritikos, V.; Carter, V.; Yan, K.Y.; Armour, C.; Ryan, D.; Price, D. Lack of asthma and rhinitis control in general practitioner-managed patients prescribed fixed-dose combination therapy in Australia. J. Asthma 2018, 55, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Menditto, E.; Cahir, C.; Aza-Pascual-Salcedo, M.; Bruzzese, D.; Poblador-Plou, B.; Malo, S.; Costa, E.; Gonzalez-Rubio, F.; Gimeno-Miguel, A.; Orlando, V.; et al. Adherence to chronic medication in older populations: Application of a common protocol among three European cohorts. Patient Prefer. Adherence 2018, 12, 1975–1987. [Google Scholar] [CrossRef]
- Menditto, E.; Costa, E.; Midao, L.; Bosnic-Anticevich, S.; Novellino, E.; Bialek, S.; Briedis, V.; Mair, A.; Rajabian-Soderlund, R.; Arnavielhe, S.; et al. Adherence to treatment in allergic rhinitis using mobile technology. The MASK Study. Clin. Exp. Allergy 2019, 49, 442–460. [Google Scholar] [CrossRef]
- Bousquet, J.; Devillier, P.; Anto, J.M.; Bewick, M.; Haahtela, T.; Arnavielhe, S.; Bedbrook, A.; Murray, R.; van Eerd, M.; Fonseca, J.A.; et al. Daily allergic multimorbidity in rhinitis using mobile technology: A novel concept of the MASK study. Allergy 2018, 73, 1622–1631. [Google Scholar] [CrossRef]
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; van Weel, C.; et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008, 63, 8–160. [Google Scholar] [CrossRef]
- Bousquet, J.; Van Cauwenberge, P.; Khaltaev, N.; Aria Workshop, G.; World Health, O. Allergic rhinitis and its impact on asthma. J. Allergy Clin. Immunol. 2001, 108, S147–S334. [Google Scholar] [CrossRef]
- Brozek, J.L.; Bousquet, J.; Baena-Cagnani, C.E.; Bonini, S.; Canonica, G.W.; Casale, T.B.; van Wijk, R.G.; Ohta, K.; Zuberbier, T.; Schunemann, H.J.; et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 revision. J. Allergy Clin. Immunol. 2010, 126, 466–476. [Google Scholar] [CrossRef]
- Members of the Workshops. ARIA in the pharmacy: Management of allergic rhinitis symptoms in the pharmacy. Allergic rhinitis and its impact on asthma. Allergy 2004, 59, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Bosnic-Anticevich, S.; Costa, E.; Menditto, E.; Lourenco, O.; Novellino, E.; Bialek, S.; Briedis, V.; Buonaiuto, R.; Chrystyn, H.; Cvetkovski, B.; et al. ARIA pharmacy 2018 “Allergic rhinitis care pathways for community pharmacy”: AIRWAYS ICPs initiative (European Innovation Partnership on Active and Healthy Ageing, DG CONNECT and DG Sante) POLLAR (Impact of Air POLLution on Asthma and Rhinitis) GARD Demonstration project. Allergy 2019, 74, 1219–1236. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Hellings, P.W.; Agache, I.; Bedbrook, A.; Bachert, C.; Bergmann, K.C.; Bewick, M.; Bindslev-Jensen, C.; Bosnic-Anticevitch, S.; Bucca, C.; et al. ARIA 2016: Care pathways implementing emerging technologies for predictive medicine in rhinitis and asthma across the life cycle. Clin. Transl. Allergy 2016, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Arnavielhe, S.; Bedbrook, A.; Bewick, M.; Laune, D.; Mathieu-Dupas, E.; Murray, R.; Onorato, G.L.; Pepin, J.L.; Picard, R.; et al. MASK 2017: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma multimorbidity using real-world-evidence. Clin. Transl. Allergy 2018, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Bedbrook, A.; Czarlewski, W.; Onorato, G.L.; Arnavielhe, S.; Laune, D.; Mathieu-Dupas, E.; Fonseca, J.; Costa, E.; Lourenco, O.; et al. Guidance to 2018 good practice: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma. Clin. Transl. Allergy 2019, 9, 16. [Google Scholar] [CrossRef]
- European Innovation Partnership on Active and Healthy Ageing Action Plan B3; Mechanisms of the Development of Allergy WP10; Global Alliance against Chronic Respiratory Diseases; Bousquet, J.; Addis, A.; Adcock, I.; Agache, I.; Agusti, A.; Alonso, A.; Annesi-Maesano, I.; et al. Integrated care pathways for airway diseases (AIRWAYS-ICPs). Eur. Respir. J. 2014, 44, 304–323. [Google Scholar] [CrossRef]
- Bousquet, J.; Barbara, C.; Bateman, E.; Bel, E.; Bewick, M.; Chavannes, N.H.; Cruz, A.A.; Haahtela, T.; Hellings, P.W.; Khaltaev, N.; et al. AIRWAYS-ICPs (European Innovation Partnership on Active and Healthy Ageing) from concept to implementation. Eur. Respir. J. 2016, 47, 1028–1033. [Google Scholar] [CrossRef]
- Bousquet, J.J.; Schunemann, H.J.; Togias, A.; Erhola, M.; Hellings, P.W.; Zuberbier, T.; Agache, I.; Ansotegui, I.J.; Anto, J.M.; Bachert, C.; et al. Next-generation ARIA care pathways for rhinitis and asthma: A model for multimorbid chronic diseases. Clin. Transl. Allergy 2019, 9, 44. [Google Scholar] [CrossRef]
- Bousquet, J.; Schunemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I.; et al. Next-generation allergic rhinitis and its impact on asthma (ARIA) guidelines for allergic rhinitis based on grading of recommendations assessment, development and evaluation (GRADE) and real-world evidence. J. Allergy Clin. Immunol. 2019. [Google Scholar] [CrossRef]
- Bousquet, J.; Farrell, J.; Crooks, G.; Hellings, P.; Bel, E.H.; Bewick, M.; Chavannes, N.H.; de Sousa, J.C.; Cruz, A.A.; Haahtela, T.; et al. Scaling up strategies of the chronic respiratory disease programme of the European innovation partnership on active and healthy ageing (Action Plan B3: Area 5). Clin. Transl. Allergy 2016, 6, 29. [Google Scholar] [CrossRef]
- Bousquet, J.; Agache, I.; Aliberti, M.R.; Angles, R.; Annesi-Maesano, I.; Anto, J.M.; Arnavielhe, S.; Asayag, E.; Bacci, E.; Bedbrook, A.; et al. Transfer of innovation on allergic rhinitis and asthma multimorbidity in the elderly (MACVIA-ARIA)—EIP on AHA twinning reference site (GARD research demonstration project). Allergy 2018, 73, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Valiulis, A.; Bousquet, J.; Veryga, A.; Suprun, U.; Sergeenko, D.; Cebotari, S.; Borelli, D.; Pietikainen, S.; Banys, J.; Agache, I.; et al. Vilnius declaration on chronic respiratory diseases: Multisectoral care pathways embedding guided self-management, mHealth and air pollution in chronic respiratory diseases. Clin. Transl. Allergy 2019, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Hellings, P.W.; Agache, I.; Amat, F.; Annesi-Maesano, I.; Ansotegui, I.J.; Anto, J.M.; Bachert, C.; Bateman, E.D.; Bedbrook, A.; et al. Allergic rhinitis and its impact on asthma (ARIA) phase 4 (2018): Change management in allergic rhinitis and asthma multimorbidity using mobile technology. J. Allergy Clin. Immunol. 2019, 143, 864–879. [Google Scholar] [CrossRef]
- Wallace, D.V.; Dykewicz, M.S. Seasonal allergic rhinitis: A focused systematic review and practice parameter update. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Tan, R.; Cvetkovski, B.; Kritikos, V.; Price, D.; Yan, K.; Smith, P.; Bosnic-Anticevich, S. The burden of rhinitis and the impact of medication management within the community pharmacy setting. J. Allergy Clin. Immunol. Pract. 2018, 6, 1717–1725. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, P.J.; Bachert, C.; Canonica, G.W.; Casale, T.B.; Mullol, J.; Klossek, J.M.; Zuberbier, T.; Bousquet, J. Uncontrolled allergic rhinitis during treatment and its impact on quality of life: A cluster randomized trial. J. Allergy Clin. Immunol. 2010, 126, 666–668.e5. [Google Scholar] [CrossRef] [PubMed]
- Tan, R.; Cvetkovski, B.; Kritikos, V.; Price, D.; Yan, K.; Smith, P.; Bosnic-Anticevich, S. Identifying the hidden burden of allergic rhinitis (AR) in community pharmacy: A global phenomenon. Asthma Res. Pract. 2017, 3, 8. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012, 50, 1–12. [Google Scholar] [CrossRef]
- Shaaban, R.; Zureik, M.; Soussan, D.; Neukirch, C.; Heinrich, J.; Sunyer, J.; Wjst, M.; Cerveri, I.; Pin, I.; Bousquet, J.; et al. Rhinitis and onset of asthma: A longitudinal population-based study. Lancet 2008, 372, 1049–1057. [Google Scholar] [CrossRef]
- Bousquet, J.; Fokkens, W.; Burney, P.; Durham, S.R.; Bachert, C.; Akdis, C.A.; Canonica, G.W.; Dahlen, S.E.; Zuberbier, T.; Bieber, T.; et al. Important research questions in allergy and related diseases: Nonallergic rhinitis: A GA2LEN paper. Allergy 2008, 63, 842–853. [Google Scholar] [CrossRef]
- Leonardi, A.; Castegnaro, A.; Valerio, A.L.; Lazzarini, D. Epidemiology of allergic conjunctivitis: Clinical appearance and treatment patterns in a population-based study. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Navarro, A.; Valero, A.; Julia, B.; Quirce, S. Coexistence of asthma and allergic rhinitis in adult patients attending allergy clinics: ONEAIR study. J. Investig. Allergol. Clin. Immunol. 2008, 18, 233–238. [Google Scholar] [PubMed]
- Ciprandi, G.; Cirillo, I.; Signori, A. Impact of allergic rhinitis on bronchi: An 8-year follow-up study. Am. J. Rhinol. Allergy 2011, 25, e72–e76. [Google Scholar] [CrossRef] [PubMed]
- Clatworthy, J.; Price, D.; Ryan, D.; Haughney, J.; Horne, R. The value of self-report assessment of adherence, rhinitis and smoking in relation to asthma control. Prim. Care Respir. J. 2009, 18, 300–305. [Google Scholar] [CrossRef]
- Bousquet, J.; Pfaar, O.; Togias, A.; Schunemann, H.J.; Ansotegui, I.; Papadopoulos, N.G.; Tsiligianni, I.; Agache, I.; Anto, J.M.; Bachert, C.; et al. 2019 ARIA Care pathways for allergen immunotherapy. Allergy 2019. [Google Scholar] [CrossRef] [PubMed]
- Silverman, J.B.; Stapinski, C.D.; Huber, C.; Ghandi, T.K.; Churchill, W.W. Computer-based system for preventing adverse drug events. Am. J. Health Syst. Pharm. 2004, 61, 1599–1603. [Google Scholar] [CrossRef]
- Ajami, S.; Amini, F. Evaluate the ability of clinical decision support systems (CDSSs) to improve clinical practice. Med. Arch. 2013, 67, 126–130. [Google Scholar] [CrossRef]
- Hwang, S.H.; Lee, S.; Koo, H.K.; Kim, Y. Evaluation of a computer-based adverse-drug-event monitor. Am. J. Health Syst. Pharm. 2008, 65, 2265–2272. [Google Scholar] [CrossRef]
- Liu, Y.L.; Chu, L.L.; Su, H.C.; Tsai, K.T.; Kao, P.H.; Chen, J.F.; Hsieh, H.C.; Lin, H.J.; Hsu, C.C.; Huang, C.C. Impact of computer-based and pharmacist-assisted medication review initiated in the emergency department. J. Am. Geriatr. Soc. 2019, 67, 2298–2304. [Google Scholar] [CrossRef]
- Bertsche, T.; Nachbar, M.; Fiederling, J.; Schmitt, S.P.; Kaltschmidt, J.; Seidling, H.M.; Haefeli, W.E. Assessment of a computerised decision support system for allergic rhino-conjunctivitis counselling in German pharmacy. Int. J. Clin. Pharm. 2012, 34, 17–22. [Google Scholar] [CrossRef]
- Courbis, A.L.; Murray, R.B.; Arnavielhe, S.; Caimmi, D.; Bedbrook, A.; Van Eerd, M.; De Vries, G.; Dray, G.; Agache, I.; Morais-Almeida, M.; et al. Electronic clinical decision support system for allergic rhinitis management: MASK e-CDSS. Clin. Exp. Allergy 2018, 48, 1640–1653. [Google Scholar] [CrossRef] [PubMed]
- Demoly, P.; Bousquet, P.J.; Mesbah, K.; Bousquet, J.; Devillier, P. Visual analogue scale in patients treated for allergic rhinitis: An observational prospective study in primary care: Asthma and rhinitis. Clin. Exp. Allergy 2013, 43, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, P.J.; Demoly, P.; Devillier, P.; Mesbah, K.; Bousquet, J. Impact of allergic rhinitis symptoms on quality of life in primary care. Int. Arch. Allergy Immunol. 2013, 160, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, P.; Correia de Sousa, J.; Bousquet, J.; Bugalho-Almeida, A.; Del Giacco, S.R.; Demoly, P.; Haahtela, T.; Jacinto, T.; Garcia-Larsen, V.; van der Molen, T.; et al. Control of allergic rhinitis and asthma test (CARAT): Dissemination and applications in primary care. Prim. Care Respir. J. 2013, 22, 112–116. [Google Scholar] [CrossRef]
- Lourenco, O.; Calado, S.; Sa-Sousa, A.; Fonseca, J. Evaluation of allergic rhinitis and asthma control in a Portuguese community pharmacy setting. J. Manag. Care Spec. Pharm. 2014, 20, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Wise, S.K.; Lin, S.Y.; Toskala, E.; Orlandi, R.R.; Akdis, C.A.; Alt, J.A.; Azar, A.; Baroody, F.M.; Bachert, C.; Canonica, G.W.; et al. International consensus statement on allergy and rhinology: Allergic rhinitis. Int. Forum Allergy Rhinol. 2018, 8, 108–352. [Google Scholar] [CrossRef] [PubMed]
- Seidman, M.D.; Gurgel, R.K.; Lin, S.Y.; Schwartz, S.R.; Baroody, F.M.; Bonner, J.R.; Dawson, D.E.; Dykewicz, M.S.; Hackell, J.M.; Han, J.K.; et al. Clinical practice guideline: Allergic rhinitis. Otolaryngol. Head Neck Surg. 2015, 152, S1–S43. [Google Scholar] [CrossRef]
- Angier, E.; Willington, J.; Scadding, G.; Holmes, S.; Walker, S. Management of allergic and non-allergic rhinitis: A primary care summary of the BSACI guideline. Prim. Care Respir. J. 2010, 19, 217–222. [Google Scholar] [CrossRef]
- Roberts, G.; Xatzipsalti, M.; Borrego, L.M.; Custovic, A.; Halken, S.; Hellings, P.W.; Papadopoulos, N.G.; Rotiroti, G.; Scadding, G.; Timmermans, F.; et al. Paediatric rhinitis: Position paper of the European Academy of Allergy and Clinical Immunology. Allergy 2013, 68, 1102–1116. [Google Scholar] [CrossRef]
- Benninger, M.; Farrar, J.R.; Blaiss, M.; Chipps, B.; Ferguson, B.; Krouse, J.; Marple, B.; Storms, W.; Kaliner, M. Evaluating approved medications to treat allergic rhinitis in the United States: An evidence-based review of efficacy for nasal symptoms by class. Ann. Allergy Asthma Immunol. 2010, 104, 13–29. [Google Scholar] [CrossRef]
- May, J.R.; Dolen, W.K. Management of allergic rhinitis: A review for the community pharmacist. Clin. Ther. 2017, 39, 2410–2419. [Google Scholar] [CrossRef]
- Carter, A.; Dattani, N.; Hannan, S.A. Chronic rhinosinusitis. BMJ 2019, 364, l131. [Google Scholar] [CrossRef]
- Sher, E.R.; Ross, J.A. Intranasal corticosteroids: The role of patient preference and satisfaction. Allergy Asthma Proc. 2014, 35, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Yanez, A.; Dimitroff, A.; Bremner, P.; Rhee, C.S.; Luscombe, G.; Prillaman, B.A.; Johnson, N. A patient preference study that evaluated fluticasone furoate and mometasone furoate nasal sprays for allergic rhinitis. Allergy Rhinol. 2016, 7, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Ruud, K.W.; Ronningen, S.W.; Faksvag, P.K.; Ariansen, H.; Hovland, R. Evaluation of a structured pharmacist-led inhalation technique assessment service for patients with asthma and COPD in Norwegian pharmacies. Patient Educ. Couns. 2018, 101, 1828–1837. [Google Scholar] [CrossRef] [PubMed]
- Apikoglu-Rabus, S.; Yesilyaprak, G.; Izzettin, F.V. Drug-related problems and pharmacist interventions in a cohort of patients with asthma and chronic obstructive pulmonary disease. Respir. Med. 2016, 120, 109–115. [Google Scholar] [CrossRef]
- Tommelein, E.; Mehuys, E.; Van Hees, T.; Adriaens, E.; Van Bortel, L.; Christiaens, T.; Van Tongelen, I.; Remon, J.P.; Boussery, K.; Brusselle, G. Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): A randomized controlled trial. Br. J. Clin. Pharmacol. 2014, 77, 756–766. [Google Scholar] [CrossRef]
- McLean, W.M.; MacKeigan, L.D. When does pharmaceutical care impact health outcomes? A comparison of community pharmacy-based studies of pharmaceutical care for patients with asthma. Ann. Pharmacother. 2005, 39, 625–631. [Google Scholar] [CrossRef]
- Ganesh, V.; Banigo, A.; McMurran, A.E.L.; Shakeel, M.; Ram, B. Does intranasal steroid spray technique affect side effects and compliance? Results of a patient survey. J. Laryngol. Otol. 2017, 131, 991–996. [Google Scholar] [CrossRef]
- Williams, P.B.; Crandall, E.; Sheppard, J.D. Azelastine hydrochloride, a dual-acting anti-inflammatory ophthalmic solution, for treatment of allergic conjunctivitis. Clin. Ophthalmol. 2010, 4, 993–1001. [Google Scholar] [CrossRef]
- Berger, W.; Bousquet, J.; Fox, A.T.; Just, J.; Muraro, A.; Nieto, A.; Valovirta, E.; Wickman, M.; Wahn, U. Azelastine/fluticasone propionate(Dymista) for seasonal allergic rhinitis. Med. Lett. Drugs Ther. 2012, 54, 85–87. [Google Scholar]
- Bousquet, J.; Bachert, C.; Bernstein, J.; Canonica, G.W.; Carr, W.; Dahl, R.; Demoly, P.; Devillier, P.; Hellings, P.; Fokkens, W.; et al. Advances in pharmacotherapy for the treatment of allergic rhinitis; MP29-02 (a novel formulation of azelastine hydrochloride and fluticasone propionate in an advanced delivery system) fills the gaps. Expert Opin. Pharmacother. 2015, 16, 913–928. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.; Musicco, E.; Rastrelli, F.; Bettoncelli, G.; Passalacqua, G.; Canonica, G.W. The patient with rhinitis in the pharmacy. A cross-sectional study in real life. Asthma Res. Pract. 2015, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Church, M.K.; Maurer, M.; Simons, F.E.; Bindslev-Jensen, C.; van Cauwenberge, P.; Bousquet, J.; Holgate, S.T.; Zuberbier, T.; Global Allergy and Asthma European Network. Risk of first-generation H(1)-antihistamines: A GA(2)LEN position paper. Allergy 2010, 65, 459–466. [Google Scholar] [CrossRef]
- Van Driel, M.L.; Scheire, S.; Deckx, L.; Gevaert, P.; De Sutter, A. What treatments are effective for common cold in adults and children? BMJ 2018, 363, k3786. [Google Scholar] [CrossRef]
- Wallace, D.V.; Dykewicz, M.S.; Bernstein, D.I.; Blessing-Moore, J.; Cox, L.; Khan, D.A.; Lang, D.M.; Nicklas, R.A.; Oppenheimer, J.; Portnoy, J.M.; et al. The diagnosis and management of rhinitis: An updated practice parameter. J. Allergy Clin. Immunol. 2008, 122, S1–S84. [Google Scholar] [CrossRef]
- Graf, P. Rhinitis medicamentosa: A review of causes and treatment. Treat. Respir. Med. 2005, 4, 21–29. [Google Scholar] [CrossRef]
- Ramey, J.T.; Bailen, E.; Lockey, R.F. Rhinitis medicamentosa. J. Investig. Allergol. Clin. Immunol. 2006, 16, 148–155. [Google Scholar]
- Mehuys, E.; Gevaert, P.; Brusselle, G.; Van Hees, T.; Adriaens, E.; Christiaens, T.; Van Bortel, L.; Van Tongelen, I.; Remon, J.P.; Boussery, K. Self-medication in persistent rhinitis: Overuse of decongestants in half of the patients. J. Allergy Clin. Immunol. Pract. 2014, 2, 313–319. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Caballero, F.; Fromer, L.M.; Krouse, J.H.; Scadding, G. Treatment of congestion in upper respiratory diseases. Int. J. Gen. Med. 2010, 3, 69–91. [Google Scholar] [CrossRef]
- Rachelefsky, G.; Farrar, J.R. Are you comfortable with over-the-counter intranasal steroids for children? A call to action. J. Allergy Clin. Immunol. Pract. 2014, 2, 271–274. [Google Scholar] [CrossRef] [PubMed]
- van Cauwenberge, P.; Bachert, C.; Passalacqua, G.; Bousquet, J.; Canonica, G.W.; Durham, S.R.; Fokkens, W.J.; Howarth, P.H.; Lund, V.; Malling, H.J.; et al. Consensus statement on the treatment of allergic rhinitis. European Academy of Allergology and Clinical Immunology. Allergy 2000, 55, 116–134. [Google Scholar] [CrossRef] [PubMed]
- Cardell, L.O.; Olsson, P.; Andersson, M.; Welin, K.O.; Svensson, J.; Tennvall, G.R.; Hellgren, J. TOTALL: High cost of allergic rhinitis-a national Swedish population-based questionnaire study. NPJ Prim. Care Respir. Med. 2016, 26, 15082. [Google Scholar] [CrossRef] [PubMed]
- Pinnock, H. Supported self-management for asthma. Breathe 2015, 11, 98–109. [Google Scholar] [CrossRef]
- Lenferink, A.; Brusse-Keizer, M.; van der Valk, P.D.; Frith, P.A.; Zwerink, M.; Monninkhof, E.M.; van der Palen, J.; Effing, T.W. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 8, CD011682. [Google Scholar] [CrossRef]
- Grady, P.A.; Gough, L.L. Self-management: A comprehensive approach to management of chronic conditions. Am. J. Public Health 2014, 104, e25–e31. [Google Scholar] [CrossRef]
- Andrews, K.L.; Jones, S.C.; Mullan, J. Asthma self management in adults: A review of current literature. Collegian 2014, 21, 33–41. [Google Scholar] [CrossRef]
- O’Connor, J.; Seeto, C.; Saini, B.; Bosnic-Anticevich, S.; Krass, I.; Armour, C.; Smith, L. Healthcare professional versus patient goal setting in intermittent allergic rhinitis. Patient Educ. Couns. 2008, 70, 111–117. [Google Scholar] [CrossRef]
- McCabe, C.; McCann, M.; Brady, A.M. Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 5, CD011425. [Google Scholar] [CrossRef]
- Makhinova, T.; Barner, J.C.; Richards, K.M.; Rascati, K.L. Asthma controller medication adherence, risk of exacerbation, and use of rescue agents among Texas medicaid patients with persistent asthma. J. Manag. Care Spec. Pharm. 2015, 21, 1124–1132. [Google Scholar] [CrossRef]
- Hasford, J.; Uricher, J.; Tauscher, M.; Bramlage, P.; Virchow, J.C. Persistence with asthma treatment is low in Germany especially for controller medication—A population based study of 483,051 patients. Allergy 2010, 65, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.; Kurup, R.; Laba, T.L.; Santo, K.; Thiagalingam, A.; Rodgers, A.; Woodward, M.; Redfern, J.; Chow, C.K. Mobile telephone text messaging for medication adherence in chronic disease: A meta-analysis. JAMA Intern. Med. 2016, 176, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Santo, K.; Richtering, S.S.; Chalmers, J.; Thiagalingam, A.; Chow, C.K.; Redfern, J. Mobile phone apps to improve medication adherence: A systematic stepwise process to identify high-quality apps. JMIR mHealth uHealth 2016, 4, e132. [Google Scholar] [CrossRef] [PubMed]
- Milosavljevic, A.; Aspden, T.; Harrison, J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: A systematic review. Int. J. Pharm. Pract. 2018, 26, 387–397. [Google Scholar] [CrossRef]
- Bousquet, J.; Bewick, M.; Arnavielhe, S.; Mathieu-Dupas, E.; Murray, R.; Bedbrook, A.; Caimmi, D.P.; Vandenplas, O.; Hellings, P.W.; Bachert, C.; et al. Work productivity in rhinitis using cell phones: The MASK pilot study. Allergy 2017, 72, 1475–1484. [Google Scholar] [CrossRef]
- Bousquet, J.; Arnavielhe, S.; Bedbrook, A.; Fonseca, J.; Morais Almeida, M.; Todo Bom, A.; Annesi-Maesano, I.; Caimmi, D.; Demoly, P.; Devillier, P.; et al. The allergic rhinitis and its impact on asthma (ARIA) score of allergic rhinitis using mobile technology correlates with quality of life: The MASK study. Allergy 2018, 73, 505–510. [Google Scholar] [CrossRef]
- Bourret, R.; Bousquet, J.; Mercier, J.; Camuzat, T.; Bedbrook, A.; Demoly, P.; Caimmi, D.; Laune, D.; Arnavielhe, S. MASK-rhinitis, a single tool for integrated care pathways in allergic rhinitis. World Hosp. Health Serv. 2015, 51, 36–39. [Google Scholar]
- Bousquet, P.J.; Combescure, C.; Neukirch, F.; Klossek, J.M.; Mechin, H.; Daures, J.P.; Bousquet, J. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy 2007, 62, 367–372. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions Helping to Identify Allergic Rhinitis |
|---|
| What is your main symptom? (Check for rhinorrhea, sneezing, itchy nose, nasal congestion, watery or itchy eyes.) |
| How long have you had these symptoms? |
| Do you have the symptoms all the time or do they come and go? |
| Are you aware of anything that seems to bring the symptoms on, such as being outdoors, pollen seasons, contact with animals, something you handle at work or at home? |
| Has a doctor ever diagnosed you with hay fever, allergic rhinitis, or asthma? |
| Is your nasal discharge clear and watery? (purulent discharge suggests infection) |
| Are you experiencing any wheezing or shortness of breath? (“Yes” may indicate asthma.) |
| Do you have an earache or any pain in your face? (“Yes” may indicate otitis media or sinusitis.) |
| Questions helping to identify allergic conjunctivitis |
| What is your main symptom? (Check for bilateral eye symptoms, eye itching, watery eyes, red eyes) |
| Do you have allergic rhinitis? |
| Do your eyes burn? (“Yes” may indicate disease other than allergic rhinitis) |
| Do you have dry eyes? (“Yes” may indicate disease other than allergic rhinitis) |
| Do you have photophobia? (“Yes” may indicate disease other than allergic rhinitis and the patient should be referred to a doctor) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lourenço, O.; Bosnic-Anticevich, S.; Costa, E.; Fonseca, J.A.; Menditto, E.; Cvetkovski, B.; Kritikos, V.; Tan, R.; Bedbrook, A.; Scheire, S.; et al. Managing Allergic Rhinitis in the Pharmacy: An ARIA Guide for Implementation in Practice. Pharmacy 2020, 8, 85. https://doi.org/10.3390/pharmacy8020085
Lourenço O, Bosnic-Anticevich S, Costa E, Fonseca JA, Menditto E, Cvetkovski B, Kritikos V, Tan R, Bedbrook A, Scheire S, et al. Managing Allergic Rhinitis in the Pharmacy: An ARIA Guide for Implementation in Practice. Pharmacy. 2020; 8(2):85. https://doi.org/10.3390/pharmacy8020085
Chicago/Turabian StyleLourenço, Olga, Sinthia Bosnic-Anticevich, Elísio Costa, João A. Fonseca, Enrica Menditto, Biljana Cvetkovski, Vicky Kritikos, Rachel Tan, Anna Bedbrook, Sophie Scheire, and et al. 2020. "Managing Allergic Rhinitis in the Pharmacy: An ARIA Guide for Implementation in Practice" Pharmacy 8, no. 2: 85. https://doi.org/10.3390/pharmacy8020085
APA StyleLourenço, O., Bosnic-Anticevich, S., Costa, E., Fonseca, J. A., Menditto, E., Cvetkovski, B., Kritikos, V., Tan, R., Bedbrook, A., Scheire, S., Bachert, C., Białek, S., Briedis, V., Boussery, K., Canonica, G. W., Haahtela, T., Kuna, P., Novellino, E., Samoliński, B., ... Bousquet, J. (2020). Managing Allergic Rhinitis in the Pharmacy: An ARIA Guide for Implementation in Practice. Pharmacy, 8(2), 85. https://doi.org/10.3390/pharmacy8020085