A Continuing Professional Development Program for Pharmacists Implementing Pharmacogenomics into Practice

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Phase 1—Pharmacogenomics CPD Program
2.1.1. Recruitment Procedures
2.1.2. CPD Program Design and Curriculum
2.2. Phase 2—Pharmacogenomics Implementation in Practice
2.3. Outcomes
2.3.1. Participant Satisfaction Questionnaire
2.3.2. Knowledge Test
2.3.3. Self-Assessment Survey
2.3.4 Semi-Structured Interviews
2.4. Data Analysis
3. Results
3.1. Training Program Participants
3.2. Moore’s Expanded Outcome Framework
3.2.1. Level 1: Participation
3.2.2. Level 2: Satisfaction
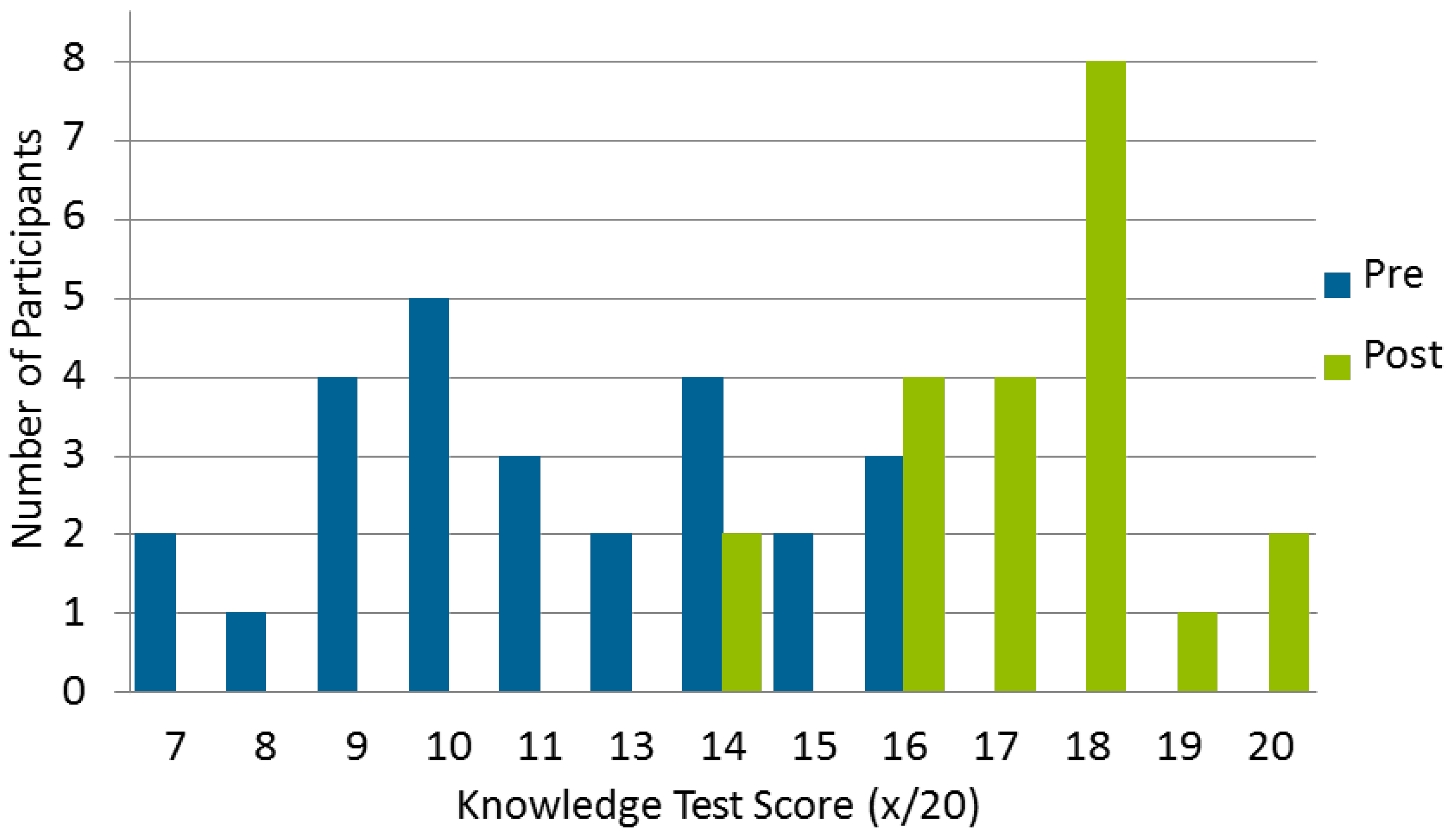
3.2.3. Level 3: Declarative and Procedural Knowledge
3.2.4. Level 4: Competence
3.2.5. Level 5: Performance
“I feel that I definitely have a better understanding than I had before. I definitely have more resources that I’ve learned about through this process. So if I were to be asked a question, I think I can be able to find the right resources to provide some opinion.”
“Especially with some of the first patients that I had, it just took me a while to feel comfortable myself with all of that. So let alone, sort of potential knowledge gaps that I had too. So not only getting comfortable in understanding what the results mean and how to apply that to the patient but also the knowledge gaps with regards to... I mean, like CANMAT [Canadian Network for Mood and Anxiety Treatments, parentheses added] guidelines for anxiety and depression and all of those subcategories, I found that I really had to refresh myself. Obviously wanting to recommend what was first line.”
“Well, I can tell you that I got three more referrals from that physician. So I think once you kind of see some of that success that also kind of buys into the approach as well.”
“I think I would want to personally study a little bit more now that I have an understanding. I think I have a very general understanding and have been able to at least talk about the reports. But if I were doing it on my own, I would want to be a little bit more up-to-date. Like…because you know, being part of the study, I always felt that if I had any questions, I can reach out to somebody who is an expert. But if I were doing it on my own then I would expect that my level of understanding should be higher.”
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
- Daniel Mueller, Arun Tiwani, Natalie Freeman for their teaching contributions during the in-person component of the CPD program.
- Ryan Keay and Sara Karlsson for coordinating the logistics of the in-person component of the program. Melissa Baranski for her assistance with submission for research ethics board approval.
- Josie Chundamala, Thomas Boyang Huang, Jessica John, and Dana Wall-Bryce for their contributions to quantitative data management and preliminary analysis.
- Nina Krupetsky and Clara Korenvain for data collection and analysis of the qualitative interviews.
Conflicts of Interest
References
- Murphy, J.E.; Green, J.S.; Adams, L.A.; Squire, R.B.; Kuo, G.M.; McKay, A. Pharmacogenomics in the curricula of colleges and schools of pharmacy in the United States. Am. J. Pharm. Educ. 2010, 74, 7. [Google Scholar] [CrossRef] [PubMed]
- Haga, S.B.; Moaddeb, J. Pharmacogenomics courses in pharmacy school curricula. Pharmacogenomics 2019, 20, 625–630. [Google Scholar] [CrossRef] [PubMed]
- De Denus, S.; Letarte, N.; Hurlimann, T.; Lambert, J.-P.; Lavoie, A.; Robb, L.; Sheehan, N.L.; Turgeon, J.; Vadnais, B. An evaluation of pharmacists’ expectations towards pharmacogenomics. Pharmacogenomics 2013, 14, 165–175. [Google Scholar] [CrossRef] [PubMed]
- McCullough, K.B.; Formea, C.M.; Berg, K.D.; Burzynski, J.A.; Cunningham, J.L.; Ou, N.N.; Rudis, M.I.; Stollings, J.L.; Nicholson, W.T. Assessment of the Pharmacogenomics Educational Needs of Pharmacists. Am. J. Pharm. Educ. 2011, 75, 51. [Google Scholar] [CrossRef] [PubMed]
- Obreli-Neto, P.R.; Marques dos Reis, T.; Guidoni, C.M.; Girotto, E.; Guerra, M.L.; de Oliveira Baldoni, A.; Leira Pereira, L.R. A Systematic Review of the Effects of Continuing Education Programs on Providing Clinical Community Pharmacy Services. Am. J. Pharm. Educ. 2016, 80, 88. [Google Scholar] [CrossRef]
- Wheeler, J.S.; Chisholm-Burns, M. The Benefit of Continuing Professional Development for Continuing Pharmacy Education. Am. J. Pharm. Educ. 2018, 82, 6461. [Google Scholar] [CrossRef]
- Moore, D.E.; Green, J.S.; Gallis, H.A. Achieving desired results and improved outcomes: Integrating planning and assessment throughout learning activities: J. Contin. Educ. Health Prof. 2009, 29, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Weitzel, K.W.; Aquilante, C.L.; Johnson, S.; Kisor, D.F.; Empey, P.E. Educational strategies to enable expansion of pharmacogenomics-based care. Am. J. Health. Syst. Pharm. 2016, 73, 1986–1998. [Google Scholar] [CrossRef] [PubMed]
- Merrill, M.D.; Twitchell, D. Instructional Design Theory; Educational Technology Publications: Englewood Cliffs, NJ, USA, 1994; ISBN 978-0-87778-275-9. [Google Scholar]
- Haga, S.; Burke, W.; Ginsburg, G.; Mills, R.; Agans, R. Primary care physicians’ knowledge of and experience with pharmacogenetic testing: Primary care physicians’ and pharmacogenetic testing. Clin. Genet. 2012, 82, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Stanek, E.J.; Sanders, C.L.; Taber, K.A.J.; Khalid, M.; Patel, A.; Verbrugge, R.R.; Agatep, B.C.; Aubert, R.E.; Epstein, R.S.; Frueh, F.W. Adoption of Pharmacogenomic Testing by US Physicians: Results of a Nationwide Survey. Clin. Pharmacol. Ther. 2012, 91, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Roederer, M.W.; Kuo, G.M.; Kisor, D.F.; Frye, R.F.; Hoffman, J.M.; Jenkins, J.; Weitzel, K.W. Pharmacogenomics competencies in pharmacy practice: A blueprint for change. J. Am. Pharm. Assoc. 2017, 57, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Diamantouros, A.; Marchesano, R.; Geerts, W.H.; Pennefather, P.; Zwarenstein, M.; Austin, Z. Development and evaluation of a continuing pharmacy education (CPE) program in thrombosis management. Curr. Pharm. Teach. Learn. 2017, 9, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Wilbur, K.; Shabana, S.; Maraghi, F.; ElMubark, A.; Kheir, N. An evaluation of the translation of continuing education into diabetes public health care by pharmacists. Int. J. Clin. Pharm. 2017, 39, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Formea, C.M.; Nicholson, W.T.; McCullough, K.B.; Berg, K.D.; Berg, M.L.; Cunningham, J.L.; Merten, J.A.; Ou, N.N.; Stollings, J.L. Development and Evaluation of a Pharmacogenomics Educational Program for Pharmacists. Am. J. Pharm. Educ. 2013, 77, 10. [Google Scholar] [CrossRef] [PubMed]
- Kuo, G.M.; Lee, K.C.; Ma, J.D. Implementation and outcomes of a live continuing education program on pharmacogenomics. Pharmacogenomics 2013, 14, 885–895. [Google Scholar] [CrossRef] [PubMed]
- Kisor, D.F.; Bright, D.R.; Chen, J.; Smith, T.R. Academic and professional pharmacy education: A pharmacogenomics certificate training program. Pers. Med. 2015, 12, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Formea, C.M.; Nicholson, W.T.; Vitek, C.R.; Wix, K.K.; McCullough, K.B.; Cunningham, J.L.; Zeuli, J.D.; Matey, E.T.; Merten, J.A.; Richardson, D.M.; et al. Implementation of a pharmacogenomics education program for pharmacists. Am. J. Health. Syst. Pharm. 2018, 75, 1939–1946. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institute of Health Information Pharmacists, Health Workforce Database. Available online: https://www.cihi.ca/en/pharmacists-2015-health-workforce-information (accessed on 27 February 2020).
- Berenbrok, L.A.; Hart, K.M.; McGrath, S.H.; Coley, K.C.; Somma McGivney, M.A.; Empey, P.E. Community pharmacists’ educational needs for implementing clinical pharmacogenomic services. J. Am. Pharm. Assoc. 2019, 59, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.E.; Chappell, K.; Sherman, L.; Vinayaga-Pavan, M. A conceptual framework for planning and assessing learning in continuing education activities designed for clinicians in one profession and/or clinical teams. Med. Teach. 2018, 40, 904–913. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Moore’s Framework | Description | Study Outcomes |
|---|---|---|
| Level 1: Participation | Number of pharmacists who participated in the activity | Training program attendance and completion |
| Level 2: Satisfaction | The degree to which the expectations of the participations about the setting and delivery of the CE activity were met | Training Program Participant Satisfaction Questionnaire |
| Level 3A: Declarative knowledge | The degree to which participants state what the CE activity intended them know | Objective: Pre-Post Knowledge Test Subjective: Self-Assessment Survey, Part B |
| Level 3B: Procedural knowledge | The degree to which participants state how to do what the CE activity intended them know how to do | |
| Level 4: Competence | The degree to which participants show in an educational setting how to do what the CE activity intended them to be able to do | Objective: Individual and global feedback on the patient case workups submitted by participants Subjective: Self-Assessment Survey, Part C |
| Level 5: Performance | The degree to which participants do what the CE activity intended them to be able to do in their practices | Objective: Patient enrollment in PRIME Subjective: semi-structured pharmacist interviews with thematic analysis |
| Characteristic | Category | n (%) |
|---|---|---|
| Age (years) | 20–39 | 11 (42%) |
| 40–59 | 15 (58%) | |
| Gender | Women | 15 (58%) |
| Men | 11 (42%) | |
| Primary Practice Setting | Community Pharmacy | 18 (69%) |
| Primary Care Clinics | 8 (31%) | |
| Years in Practice | <5 | 6 (23%) |
| 5–9 | 4 (15%) | |
| 10 or more | 16 (62%) | |
| Highest Pharmacy-Related Education | Bachelor of Science in Pharmacy | 18 (69%) |
| Advanced Academic/Research (MSc, MBA) | 4 (15%) | |
| Residency Trained | 1 (4%) | |
| Doctor of Pharmacy | 3 (12%) |
| Item | Pre-Program Mean (SD) 1 | Post-Program Mean (SD) 1 | p-value 2 |
|---|---|---|---|
| Part B – Self Reported Knowledge | |||
| I am adequately informed about the availability of genetic testing. | 1.6 (0.7) | 3.9 (0.8) | <0.001 |
| I am adequately informed about applying pharmacogenetics in the context of selecting medication therapy. | 1.6 (0.7) | 4.1 (0.3) | <0.001 |
| I am adequately informed about applying pharmacogenetics in the context of dosing medication therapy. | 1.7 (0.7) | 3.8 (0.7) | <0.001 |
| I feel comfortable recommending medication therapy with my current knowledge of pharmacogenetics. | 1.7 (0.7) | 3.7 (1.0) | <0.001 |
| I feel comfortable recommending medication doses with my current knowledge of pharmacogenetics. | 1.7 (0.7) | 3.3 (1.0) | 0.002 |
| Part C – Intention to change, Self-reported competence | |||
| Pharmacogenetics will be an important component of pharmacy practice in the future. | 4.5 (0.5) | 4.8 (0.4) | 0.13 |
| As a pharmacist I am well positioned to interpret pharmacogenetics testing information for my patients. | 4.0 (1.4) | 4.4 (0.5) | 0.39 |
| Pharmacogenetics is relevant to my clinical practice. | 4.1 (0.9) | 4.3 (0.5) | 0.45 |
| I can identify medications for which pharmacogenetics testing may be considered. | 2.5 (1.2) | 4.2 (0.4) | <0.001 |
| I feel comfortable recommending medication therapy with my current knowledge of pharmacogenetics. | 1.7 (0.7) | 3.7 (1.0) | <0.001 |
| I can accurately apply pharmacogenetics concepts to medication therapy selection for my patients. | 1.7 (0.7) | 4.1 (0.4) | <0.001 |
| I feel comfortable recommending medication doses with my current knowledge of pharmacogenetics. | 1.7 (0.7) | 3.3 (1.0) | 0.002 |
| I can accurately apply pharmacogenetics concepts to medication therapy dosing for my patients. | 1.7 (0.7) | 3.7 (0.8) | <0.001 |
| I can provide information about how pharmacogenetics affects the efficacy of medication therapy for my patients. | 3.1 (1.5) | 4.2 (0.9) | 0.02 |
| I can provide information about how pharmacogenetics affects the safety of medication therapy for my patients. | 3.0 (1.3) | 4.0 (0.8) | 0.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crown, N.; Sproule, B.A.; Luke, M.J.; Piquette-Miller, M.; McCarthy, L.M. A Continuing Professional Development Program for Pharmacists Implementing Pharmacogenomics into Practice. Pharmacy 2020, 8, 55. https://doi.org/10.3390/pharmacy8020055
Crown N, Sproule BA, Luke MJ, Piquette-Miller M, McCarthy LM. A Continuing Professional Development Program for Pharmacists Implementing Pharmacogenomics into Practice. Pharmacy. 2020; 8(2):55. https://doi.org/10.3390/pharmacy8020055
Chicago/Turabian StyleCrown, Natalie, Beth A. Sproule, Miles J. Luke, Micheline Piquette-Miller, and Lisa M. McCarthy. 2020. "A Continuing Professional Development Program for Pharmacists Implementing Pharmacogenomics into Practice" Pharmacy 8, no. 2: 55. https://doi.org/10.3390/pharmacy8020055
APA StyleCrown, N., Sproule, B. A., Luke, M. J., Piquette-Miller, M., & McCarthy, L. M. (2020). A Continuing Professional Development Program for Pharmacists Implementing Pharmacogenomics into Practice. Pharmacy, 8(2), 55. https://doi.org/10.3390/pharmacy8020055