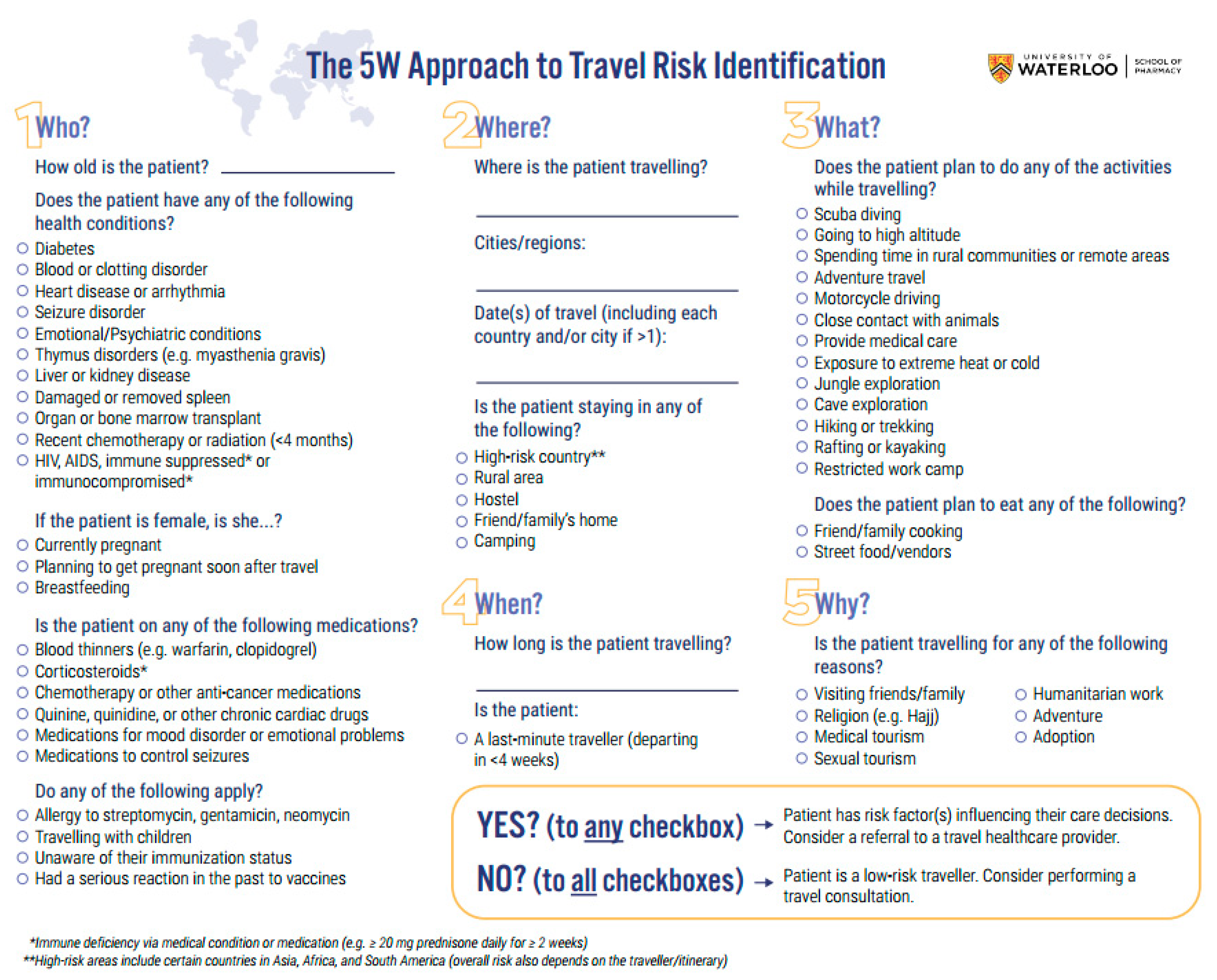
Development and Testing of a Clinical Practice Framework for Pharmacists to Assess Patients’ Travel-Related Risks: The 5W Approach to Travel Risk Identification



Abstract
1. Introduction
- Given the entry-level competencies required for pharmacists to practice, and lack of travel medicine training in pharmacy school curricula, most pharmacists without additional training or experience in travel medicine feel inadequately prepared to care for travelling patients. Further education and training regarding travel medicine for pharmacists are also often discussed as strategies to be explored by the studies with this theme [12,13,14].
2. Materials and Methods
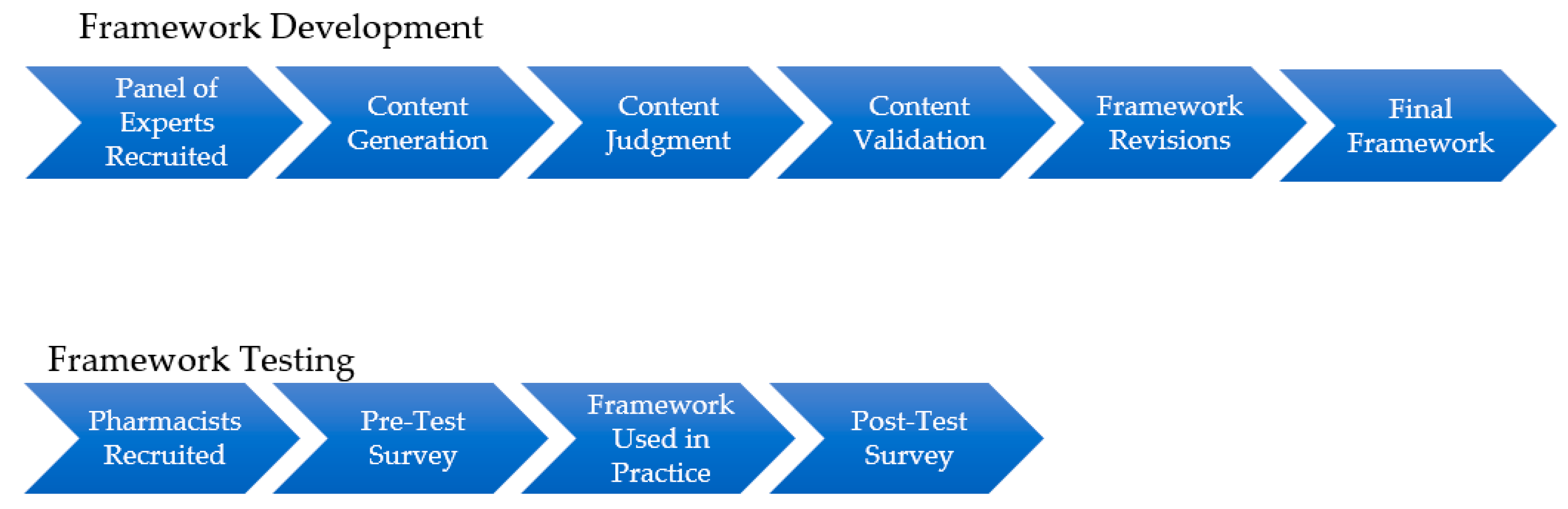
2.1. Framework Development
2.1.1. Content Generation
2.1.2. Content Judgement
2.1.3. Content Validation
2.1.4. Construction of The Framework
2.2. Framework Testing
2.2.1. Study Design and Recruitment
- Current practice is in a community pharmacy.
- Part A (able to provide direct patient care) licensure through the Ontario College of Pharmacists (OCP) or 4th year entry-to-practice PharmD student currently on clinical practice rotation.
- Does not currently hold CTH® designation from ISTM. This exclusion was applied as it is a global indicator that the individual has an advanced level of travel medicine knowledge [24], whereas this framework was developed specifically for pharmacists without experience or expertise in travel medicine.
2.2.2. Data Collection
3. Results
3.1. Framework Development
3.2. Framework Testing
3.2.1. Attitudes and Beliefs Towards Travel Medicine
3.2.2. Framework Feasibility
4. Discussion
4.1. Framework Development
4.2. Framework Testing
- Just because a pharmacy offers pretravel consultation services does not necessarily indicate that the pharmacists are actively performing them.
- Pharmacists may have differing definitions of what they consider to be a pretravel consultation.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Question | Answer Options |
|---|---|
| Screening | |
| Do you currently work in a community pharmacy practice setting? |
|
| Do you currently have an Ontario Part A license to practice pharmacy in the province? |
|
| Do you currently have the Certificate in Travel HealthTM from the International Society of Travel Medicine? |
|
| Demographics | |
| Which type of community pharmacy practice setting do you primarily work in? |
|
| What is your role in the community pharmacy practice setting you work in? |
|
| Are you the pharmacy’s designated manager? |
|
| Where is your community pharmacy practice setting located? |
|
| How many years have you worked in a community pharmacy practice setting? |
|
| On average, how many hours per week do you work in a community pharmacy practice setting? |
|
| Which gender do you most identify with? |
|
| Are you authorized to administer injections in Ontario? |
|
| What degrees/training have you received? Select all that apply. |
|
| Which of the following travel or travel-related vaccines have you personally administered since the expansion of Ontario pharmacists’ scope in December 2016? Select all that apply. |
|
| Does your pharmacy currently offer travel health services other than administration of travel vaccines (e.g., pretravel consultations)? |
|
| Pharmacy Practice | |
| What do you do when a patient presents to the pharmacy wondering what precautions they need for upcoming their travel destination? Select all that apply. |
|
| Please describe your current willingness to incorporate travel medicine services at your pharmacy. | Free-text response |
| Please describe the primary barrier(s) preventing your pharmacy from starting travel medicine services | Free-text response |
| Please describe the primary motivator(s) for your pharmacy wanting to start travel medicine services | Free-text response |
| Question | Answer Options |
|---|---|
| Practice Questions | |
| What do you do when a patient presents to the pharmacy wondering what precautions they need for upcoming their travel destination? Select all that apply. |
|
| Please describe your current willingness to incorporate travel medicine services at your pharmacy. | Free-text response |
| Please describe the primary barrier(s) preventing your pharmacy from starting travel medicine services. | Free-text response |
| Please describe the primary motivator(s) for your pharmacy wanting to start travel medicine services. | Free-text response |
| When and how do you currently offer travel consultations at your pharmacy? Select all that apply. |
|
| Does your pharmacy charge a fee to patients for a travel consultation? |
|
| Framework | |
| Please describe the main advantages of the framework. | Free-text response |
| Please describe the main disadvantages of the framework. | Free-text response |
| Please provide any suggestions, improvements, or clarifications needed for future editions of the framework | Free-text response |
Appendix B
| Domain: Who? | Essential (%, n) | Useful, but Not Essential (%, n) | Not Necessary (%, n) |
| Health Conditions | |||
| Diabetes* | 66.7% (6) | 11.1% (1) | 0% (0) |
| High blood pressure | 11.1% (1) | 55.6% (5) | 11.1% (1) |
| High cholesterol | 0% (0) | 66.7% (6) | 11.1% (1) |
| Blood or clotting disorder* | 77.8% (7) | 0% (0) | 0% (0) |
| Heart disease or arrhythmia* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Seizure disorder* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Emotional/psychiatric condition(s) * | 77.8% (7) | 0% (0) | 0% (0) |
| Lung condition (Asthma/COPD) | 44.4% (4) | 33.3% (3) | 0% (0) |
| Migraines or headaches | 0% (0) | 66.7% (6) | 11.1% (1) |
| Irritable Bowel Syndrome or digestive tract problems | 22.2% (2) | 44.4% (4) | 11.1% (1) |
| Inflammatory Bowel Disease* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Acid Reflux or heartburn | 33.3% (3) | 44.4% (4) | 0% (0) |
| Thymus disorders (e.g., myasthenia gravis) * | 66.7% (6) | 11.1% (1) | 0% (0) |
| Radical mastectomy or lymph-node dissection | 44.4% (4) | 33.3% (3) | 0% (0) |
| Liver or kidney disease* | 77.8% (7) | 0% (0) | 0% (0) |
| Damaged or removed spleen* | 77.8% (7) | 0% (0) | 0% (0) |
| Organ or bone marrow transplant* | 77.8% (7) | 0% (0) | 0% (0) |
| Recent chemotherapy or radiation (4 months) * | 77.8% (7) | 0% (0) | 0% (0) |
| HIV, AIDS, immune suppressed or immunocompromised* | 77.8% (7) | 0% (0) | 0% (0) |
| Psoriasis | 44.4% (4) | 33.3% (3) | 0% (0) |
| Ear/hearing problems | 0% (0) | 77.8% (7) | 0% (0) |
| Anemia | 11.1% (1) | 66.7% (6) | 0% (0) |
| Considerations for Females when Traveling | |||
| Currently pregnant* | 77.8% (7) | 0% (0) | 0% (0) |
| Planning to get pregnant soon after travel* | 77.8% (7) | 0% (0) | 0% (0) |
| Breastfeeding* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Date of last menstrual period | 22.2% (2) | 33.3% (3) | 22.2% (2) |
| Demographics | |||
| Age* | 77.8% (7) | 0% (0) | 0% (0) |
| Date of birth (for immunization purposes) * | 55.6% (5) | 22.2% (2) | 0% (0) |
| Medications | |||
| Blood thinners (e.g., warfarin, clopidogrel) * | 77.8% (7) | 0% (0) | 0% (0) |
| Corticosteroids* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Chemotherapy or other anti-cancer medications* | 77.8% (7) | 0% (0) | 0% (0) |
| Quinine, quinidine, or other cardiac drugs* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Antibiotics | 33.3% (3) | 44.4% (4) | 0% (0) |
| Medication for mood disorders or emotional problems* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Medications to control seizures* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Other prescription medications | 33.3% (3) | 44.4% (4) | 0% (0) |
| Allergy | |||
| Sulfa drugs | 22.2% (2) | 55.6% (5) | 0% (0) |
| Streptomycin, gentamicin or neomycin* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Penicillin | 22.2% (2) | 55.6% (5) | 0% (0) |
| Latex | 44.4% (4) | 33.3% (3) | 0% (0) |
| Yeast | 44.4% (4) | 33.3% (3) | 0% (0) |
| Gelatin | 33.3% (3) | 44.4% (4) | 0% (0) |
| Eggs or other foods | 44.4% (4) | 33.3% (3) | 0% (0) |
| Adhesive bandages | 16.7% (1) | 83.3% (5) | 0% (0) |
| Travel Companion | |||
| Alone | 33.3% (3) | 44.4% (4) | 0% (0) |
| With spouse/partner | 0% (0) | 66.7% (6) | 11.1% (1) |
| With a group | 0% (0) | 66.7% (6) | 11.1% (1) |
| With children* | 55.6% (5) | 22.2% (2) | 0% (0) |
| With an older/elderly person | 57.4% (4) | 33.3% (3) | 0% (0) |
| Immunization History | |||
| In what country were you born? | 44.4% (4) | 33.3% (3) | 0% (0) |
| If you were not born in Canada, at what age did you leave your country of birth?† | 55.6% (5) | 22.2% (2) | 0% (0) |
| Determining if the patient is aware of their immunization status* | 77.8% (7) | 0% (0) | 0% (0) |
| Has fainted or felt unwell after an injection | 33.3% (3) | 33.3% (3) | 11.1% (1) |
| Had a serious reaction in the past with vaccines* | 77.8% (7) | 0% (0) | 0% (0) |
| Had (or currently has) a fear of needles | 33.3% (3) | 44.4% (4) | 0% (0) |
| Carries an Epi-Pen | 33.3% (3) | 33.3% (3) | 11.1% (1) |
| Domain: Where? | Essential (%, n) | Useful, but not essential (%, n) | Not necessary (%, n) |
| Destination(s) | |||
| Country/Countries* | 77.8% (7) | 0% (0) | 0% (0) |
| Cities/Regions* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Dates of travel for each country and/or city (if more than one)* | 77.8% (7) | 0% (0) | 0% (0) |
| Rural/urban areas* | 77.8% (7) | 0% (0) | 0% (0) |
| Accommodations | |||
| Premium hotel | 44.4% (4) | 22.2% (2) | 11.1% (1) |
| Budget hotel | 44.4% (4) | 33.3% (3) | 0% (0) |
| Resort | 33.3% (3) | 44.4% (4) | 0% (0) |
| Cruise | 44.4% (4) | 33.3% (3) | 0% (0) |
| Hostel* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Friends/family’s home* | 77.8% (7) | 0% (0) | 0% (0) |
| Camping* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Dining | |||
| Local restaurants/bars | 33.3% (3) | 44.4% (4) | 0% (0) |
| Cooking themselves | 33.3% (3) | 44.4% (4) | 0% (0) |
| Friend/family cooking* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Street food and vendors* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Domain: When? | Essential (%, n) | Useful, but not essential (%, n) | Not necessary (%, n) |
| Timing | |||
| Departure/Arrival Dates* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Last minute traveler (<4 weeks before departure date)* | 77.8% (7) | 0% (0) | 0% (0) |
| Time of year | 44.4% (4) | 33.3% (3) | 0% (0) |
| Length of stay* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Domain: Why? | Essential (%, n) | Useful, but not essential (%, n) | Not necessary (%, n) |
| Reason(s) for Travel | |||
| Visiting friends/family* | 77.8% (7) | 0% (0) | 0% (0) |
| Business | 33.3% (3) | 44.4% (4) | 0% (0) |
| Athletic competition* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Religion (e.g., Hajj)* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Medical tourism* | 77.8% (7) | 0% (0) | 0% (0) |
| Sexual tourism* | 77.8% (7) | 0% (0) | 0% (0) |
| Humanitarian work* | 77.8% (7) | 0% (0) | 0% (0) |
| Vacation | 44.4% (4) | 33.3% (3) | 0% (0) |
| Adventure* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Research/Education* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Adoption* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Domain: What? | Essential (%, n) | Useful, but not essential (%, n) | Not necessary (%, n) |
| Planned Activities | |||
| Scuba diving* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Going to high altitude* | 77.8% (7) | 0% (0) | 0% (0) |
| Safari* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Spending time in rural communities or remote areas* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Adventure travel* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Close contact with animals* | 77.8% (7) | 0% (0) | 0% (0) |
| Providing medical care* | 77.8% (7) | 0% (0) | 0% (0) |
| Exposure to extreme heat or cold* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Jungle* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Cave exploration* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Hiking or trekking* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Rafting or kayaking* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Restricted work camp* | 66.7% (6) | 11.1% (1) | 0% (0) |
| Misc. excursion off resort | 44.4% (4) | 33.3% (3) | 0% (0) |
| Transportation | |||
| Train | 11.1% (1) | 66.7% (6) | 0% (0) |
| Rental car | 22.2% (2) | 55.6% (5) | 0% (0) |
| In-country flights | 11.1% (1) | 66.7% (6) | 0% (0) |
| Boat | 44.4% (4) | 33.3% (3) | 0% (0) |
| Motorcycle* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Type of Travel | |||
| Package | 22.2% (2) | 44.4% (4) | 11.1% (1) |
| Camping | 33.3% (3) | 44.4% (4) | 0% (0) |
| Self-organized | 22.2% (2) | 44.4% (4) | 11.1% (1) |
| Cruise ship | 33.3% (3) | 44.4% (4) | 0% (0) |
| Backpacking* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Trekking* | 55.6% (5) | 22.2% (2) | 0% (0) |
| Domain: How? | Essential (%, n) | Useful, but not essential (%, n) | Not necessary (%, n) |
| Travel Experience | |||
| New traveler | 33.3% (3) | 44.4% (4) | 0% (0) |
| Local trips only, never overseas | 22.2% (2) | 55.6% (5) | 0% (0) |
| Travelled overseas | 22.2% (2) | 55.6% (5) | 0% (0) |
| Experienced traveler | 22.2% (2) | 55.6% (5) | 0% (0) |
References
- Ministry of Health, Government of Ontario. Available online: https://news.ontario.ca/mohltc/en/2016/12/ontario-making-it-easier-to-get-your-travel-vaccines.html (accessed on 23 October 2019).
- Zaretsky, L. Is the Blueprint just old news? Can. Pharm. J. 2009, 142, 66–67. [Google Scholar] [CrossRef]
- Killeen, R. What will it take to make patient-centered care a reality? Can. Pharm. J. 2008, 141, 205–206. [Google Scholar] [CrossRef]
- Tsuyuki, R.T.; Schindel, T. Changing pharmacy practice: The leadership challenge. Can. Pharm. J. 2008, 141, 174–180. [Google Scholar] [CrossRef]
- Rosenthal, M.; Austin, Z.; Tsuyuki, R.T. Ontario pharmacists’ crisis over Bill 16: A missed opportunity? Can. Pharm. J. 2012, 145, 3539. [Google Scholar] [CrossRef]
- Houle, S.K.D.; Kozlovsky, K.; Fernandes, H.V.J.; Rosenberg-Yunger, Z. Uptake of travel health services by community pharmacies and patients following pharmacist immunization scope expansion in Ontario, Canada. Pharmacy 2019, 7, 35. [Google Scholar] [CrossRef]
- Durham, M.J.; Goad, J.A.; Neinstein, L.S.; Lou, M. A comparison of pharmacist travel-health specialists’ versus primary care providers’ recommendations for travel-related medications, vaccinations, and patient compliance in a college health setting. J. Travel Med. 2011, 18, 20–25. [Google Scholar] [CrossRef]
- Jackson, A.B.; Humphries, T.L.; Nelson, K.M.; Helling, D.K. Clinical pharmacy travel medicine services: A new frontier. Ann. Pharmacother. 2004, 38, 2160–2165. [Google Scholar] [CrossRef]
- Tran, D.; Gatewood, S.; Moczygemba, L.R.; Stanley, D.D.; Goode, J.V. Evaluating health outcomes following a pharmacist-provided comprehensive pretravel health clinic in a supermarket pharmacy. J. Am. Pharm. Assoc. 2015, 55, 143–152. [Google Scholar] [CrossRef]
- Hess, K.M.; Dai, C.W.; Garner, B.; Law, A.V. Measuring outcomes of a pharmacist-run travel health clinic located in an independent community pharmacy. J. Am. Pharm. Assoc. 2010, 50, 174–180. [Google Scholar] [CrossRef]
- Houle, S.K.D.; Bascom, C.S.; Rosenthal, M.M. Clinical outcomes and satisfaction with a pharmacist-managed travel clinic in Alberta, Canada. Travel Med. Infect. Dis. 2018, 23, 21–26. [Google Scholar] [CrossRef]
- Gilmartin, H.M. Provider-pharmacist education and adherence rates for the oral typhoid vaccine: A pilot study. J. Travel Med. 2005, 12, 113–114. [Google Scholar] [CrossRef][Green Version]
- Ross, R.S.; Wolters, B.; Viazov, S.O.; Roggendorf, M. Awareness of rabies risks and knowledge about preventive measures among experienced German travel health advisors. J. Travel Med. 2006, 13, 261–267. [Google Scholar] [CrossRef]
- Teodósio, R.; Gonçalves, L.; Imperatori, E.; Atouguia, J. Pharmacists and travel advice for tropics in lisbon (portugal). J. Travel Med. 2006, 13, 281–287. [Google Scholar] [CrossRef]
- Bascom, C.S.; Rosenthal, M.M.; Houle, S.K.D. Are pharmacists ready for a greater role in travel health? an evaluation of the knowledge and confidence in providing travel health advice of pharmacists practicing in a community pharmacy chain in Alberta, Canada. J. Travel Med. 2015, 22, 99–104. [Google Scholar] [CrossRef]
- Houle, S.K.D. Pharmacy travel health services: Current perspectives and future prospects. Integr. Pharm. Res. Pract. 2017, 7, 13–20. [Google Scholar] [CrossRef]
- Dang, R.; Goad, J.; Hess, K.; Zeind, C.; Machado, M.; Luo, S.; Law, A. Survey to determine travel medicine and immunization content in pharmacy school curricula. In Proceedings of the American Pharmacist Association Conference, Orlando, FL, USA, 28–31 March 2014. [Google Scholar]
- Spooner, L.; Abel, C.; Dunican, K.; Lynch, A.; Seed, S. Perception of the importance of a travel medicine curriculum and required immunization certification among students of pharmacy in different professional years of an accelerated doctor of pharmacy program. In Proceedings of the American Pharmacist Association Conference, New Orleans, LA, USA, 9–12 March 2012. [Google Scholar]
- Nakhla, N. Pharmacist assessment of the self-treating patient. In Canadian Pharmacists Association. Compendium of Therapeutics for Minor Ailments 2019; Canadian Pharmacists Association: Toronto, ON, Canada, 2019. [Google Scholar]
- Bates, B.P.; Bates, B.R.; Northway, D.I. PQRST: A mnemonic to communicate a change in condition. J. Am. Med. Dir. Assoc. 2002, 3, 23–25. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Yellow Book 2020: Health Information for International Travel; Oxford University Press: New York, NY, USA, 2019. [Google Scholar]
- Aw, B.; Boraston, S.; Botten, D.; Cherniwchan, D.; Fazal, H.; Kelton, T.; Libman, M.; Saldanha, C.; Scappatura, P.; Stowe, B. Travel medicine: what’s involved? When to refer? Can. Fam. Physician 2014, 60, 1091–1103. [Google Scholar]
- Sanford, C.; McConnell, A.; Osborn, J. The pretravel consultation. Am. Fam. Physician 2016, 94, 620–627. [Google Scholar]
- International Society of Travel Medicine. Certificate of Knowledge. Available online: https://www.istm.org/certificateofknowledge (accessed on 23 October 2019).
- Almanasreh, E.; Moles, R.; Chen, T.F. Evaluation of methods used for estimating content validity. Res. Social Adm. Pharm. 2019, 15, 214–221. [Google Scholar] [CrossRef]
- Rubio, D.M.; Berg-Weger, M.; Tebb, S.S.; Lee, E.S.; Rauch, S. Objectifying content validity: Conducting a content validity study in social work research. Soc. Work Res. 2003, 27, 94–104. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–386. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef]
- Government of Ontario. Available online: https://www.fin.gov.on.ca/en/economy/demographics/quarterly/dhiq1.html (accessed on 23 October 2019).
- American Pharmacist Association. Pharmacy Based Travel Health Services. Available online: https://www.pharmacist.com/pharmacy-based-travel-health-services (accessed on 23 October 2019).
- Hatz, C.; Chen, L.H. Pre-Travel Consultation. In Travel Medicine, 3rd ed.; Keystone, J.S., Freedman, D.O., Kozarsky, P.E., Connor, B.A., Nothdurft, H.D., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 31–36. [Google Scholar]
- Canadian Pharmacists Association. Pharmacists’ Expanded Scope of Practice. Pharmacists. Available online: https://www.pharmacists.ca/pharmacy-in-canada/scope-of-practice-canada/ (accessed on 30 August 2019).
- International Society of Travel Medicine. Pharmacist Professional Group. Available online: https://www.istm.org/pharmacistgroup (accessed on 30 August 2019).
- Cision. Survey says: Half of Canadians Take a Beach Holiday to Leave Behind the Winter Blues, While Others do so to Relax and Forget a Regular Routine. Available online: https://www.newswire.ca/news-releases/survey-says-half-of-canadians-take-a-beach-holiday-to-leave-behind-the-winter-blues-while-others-do-so-to-relax-and-forget-a-regular-routine-670876433.html (accessed on 23 October 2019).
- MacCallum, L.; Consiglio, G.; MacKeigan, L.; Dolovich, L. Uptake of community pharmacist-delivered MedsCheck Diabetes medication review service in Ontario between 2010 and 2014. Can. J. Diabetes 2017, 41, 253–258. [Google Scholar] [CrossRef]


| Panellist | Profession | Gender | Year of Licensure | Year CTH® Achieved | Practice Setting | Canadian Province of Practice |
|---|---|---|---|---|---|---|
| 1 | Physician | Female | 1999 | 2007 | Medical Clinic | Ontario |
| 2 | Physician | Male | 2011 | 2013 | Medical Clinic | Ontario |
| 3 | Pharmacist | Female | 2009 | 2017 | Community Pharmacy | British Columbia |
| 4 | Pharmacist | Female | 1999 | 2011 | Community Pharmacy | Nova Scotia |
| 5 | Pharmacist | Female | 1994 | 2015 | Community Pharmacy | Alberta |
| 6 | Pharmacist | Male | 1993 | 2015 | Consultant | Ontario |
| 7 | Pharmacist | Male | 2012 | 2014 | Community pharmacy | British Columbia |
| 8 | Pharmacist | Female | 1999 | 2011 | Travel Clinic | Alberta |
| 9 | Pharmacist | Female | 2013 | 2015 | Community Pharmacy | Ontario |
| Domain | Definition |
|---|---|
| Who? | Patient specific-factors (e.g., medical conditions) |
| What? | Itinerary-specific factors (e.g., activities planned during travel) |
| When? | Timeframe of travel (departure date, duration at destination) |
| Where? | Country(ies) and region(s) visited, including order if more than one |
| Why? | Motivation for travel (e.g., visiting friends and relatives) |
| How? | Travel style and history (e.g., previous travel experience) |
| Item | Not Relevant (%, n) | Somewhat Relevant (%, n) | Quite Relevant (%, n) | Highly Relevant (%, n) | I-CVI |
|---|---|---|---|---|---|
| Domain: Who? | |||||
| Diabetes | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Blood or clotting disorder | 11.1% (1) | 0% (0) | 22.2% (2) | 66.7% (6) | 0.89 |
| Heart disease or arrhythmia | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Seizure disorder | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Emotional/psychiatric condition(s) | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Inflammatory bowel disease | 0% (0) | 33.3% (3) | 22.2% (2) | 44.4% (4) | 0.67 |
| Thymus disorders (e.g., myasthenia gravis) | 0% (0) | 11.1% (1) | 11.1% (1) | 77.8% (7) | 0.89 |
| Liver or kidney disease | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Damaged or removed spleen | 0% (0) | 11.1% (1) | 22.2% (2) | 66.7% (6) | 0.89 |
| Organ or bone marrow transplant | 11.1% (1) | 0% (0) | 0% (0) | 88.9% (8) | 0.89 |
| Recent chemotherapy or radiation (<4 months) | 11.1% (1) | 0% (0) | 0% (0) | 88.9% (8) | 0.89 |
| HIV, AIDS, immune suppressed or immunocompromised | 11.1% (1) | 0% (0) | 0% (0) | 88.9% (8) | 0.89 |
| Currently pregnant | 0% (0) | 0% (0) | 0% (0) | 100% (9) | 1 |
| Planning to get pregnant soon after travel | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Breastfeeding | 0% (0) | 11.1% (1) | 55.6% (5) | 33.3% (3) | 0.89 |
| Blood thinners (e.g., warfarin, clopidogrel) | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Corticosteroids | 0% (0) | 0% (0) | 11.1% (1) | 88.9% (8) | 1 |
| Chemotherapy or other anti-cancer medications | 0% (0) | 0% (0) | 0% (0) | 100% (9) | 1 |
| Quinine, quinidine, or other cardiac drugs | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Medications for mood disorder or emotional problems | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Medications to control seizures | 0% (0) | 0% (0) | 66.7% (6) | 33.3% (3) | 1 |
| Age | 0% (0) | 0% (0) | 55.6% (5) | 44.4% (4) | 1 |
| Date of birth (for immunization purposes) | 0% (0) | 22.2% (2) | 55.6% (5) | 22.2% (2) | 0.78 |
| Allergy to streptomycin, gentamicin or neomycin etc. | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Traveling with children | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Awareness of immunization status | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Serious reaction in the past with vaccines | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Domain: Where? | |||||
| Country/Countries | 0% (0) | 0% (0) | 11.1% (1) | 88.9% (8) | 1 |
| Cities/Regions | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Dates for travel for each country and/or city (if more than one) | 0% (0) | 0% (0) | 77.8% (7) | 22.2% (2) | 1 |
| Rural/urban areas | 0% (0) | 0% (0) | 66.7% (6) | 33.3% (3) | 1 |
| Hostels | 0% (0) | 11.1% (1) | 55.6% (5) | 33.3% (3) | 0.89 |
| Friend/family’s home | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Camping | 0% (0) | 0% (0) | 55.6% (5) | 44.4% (4) | 1 |
| Domain: When? | |||||
| Departure/arrival dates | 0% (0) | 55.6% (5) | 22.2% (2) | 22.2% (2) | 0.44 |
| Last minute traveller (<4 weeks) | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Length of stay | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Domain: Why? | |||||
| Visiting friends/family | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Athletic competition | 0% (0) | 44.44% (4) | 33.33% (3) | 11.11% (1) | 0.44 |
| Religion (e.g., Hajj) | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Medical tourism | 0% (0) | 0% (0) | 11.1% (1) | 88.9% (8) | 1 |
| Sexual tourism | 0% (0) | 0% (0) | 11.1% (1) | 88.9% (8) | 1 |
| Humanitarian work | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Adventure | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Research/education | 0% (0) | 33.3% (3) | 66.7% (6) | 0% (0) | 0.67 |
| Adoption | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Domain: What? | |||||
| Scuba diving | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Going to high altitude | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Safari | 0% (0) | 33.3% (3) | 55.6% (5) | 11.1% (1) | 0.67 |
| Spending time in rural communities or remote areas | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Adventure travel | 0% (0) | 11.1% (1) | 55.6% (5) | 33.3% (3) | 0.89 |
| Close contact with animals | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Providing medical care | 0% (0) | 0% (0) | 11.1% (1) | 88.9% (8) | 1 |
| Exposure to extreme heat or cold | 0% (0) | 0% (0) | 44.4% (4) | 55.6% (5) | 1 |
| Jungle | 0% (0) | 11.1% (1) | 44.4% (4) | 44.4% (4) | 0.89 |
| Cave exploration | 0% (0) | 0% (0) | 66.7% (6) | 33.3% (3) | 1 |
| Hiking or trekking | 0% (0) | 11.1% (1) | 66.7% (6) | 22.2% (2) | 0.89 |
| Rafting or kayaking | 0% (0) | 22.2% (2) | 55.6% (5) | 22.2% (2) | 0.78 |
| Restricted work camp | 0% (0) | 22.2% (2) | 55.6% (5) | 22.2% (2) | 0.78 |
| Motorcycle | 0% (0) | 11.1% (1) | 33.3% (3) | 55.6% (5) | 0.89 |
| Backpacking | 0% (0) | 22.2% (2) | 33.3% (3) | 44.4% (4) | 0.78 |
| Trekking | 0% (0) | 33.3% (3) | 33.3% (3) | 33.3% (3) | 0.67 |
| Friend/family cooking | 0% (0) | 0% (0) | 22.2% (2) | 77.8% (7) | 1 |
| Street food and vendors | 0% (0) | 0% (0) | 33.3% (3) | 66.7% (6) | 1 |
| Ave-CVI = 0.91 | |||||
| Characteristic | Frequency (%) (n = 8) |
|---|---|
| Type of community pharmacy | |
| Chain | 4 (50.0%) |
| Independent | 1 (12.5%) |
| Banner | 3 (37.5%) |
| Role in pharmacy | |
| Staff pharmacist | 4 (50.0%) |
| Owner | 2 (25.0%) |
| Pharmacy student | 2 (25.0%) |
| Designated manager1 | 3 (37.5%) |
| Location in Ontario | |
| Central South | 1 (12.5%) |
| Central West | 1 (12.5%) |
| East | 1 (12.5%) |
| South West | 5 (62.5%) |
| Years in a community pharmacy practice (licensed pharmacists only, n = 6) | |
| Less than 1 | 1 (16.7%) |
| 11–20 | 4 (66.6%) |
| 21–30 | 1 (16.7%) |
| Average number of hours worked per week (licensed pharmacists only, n = 6) | |
| 8–16 | 2 (33.3%) |
| 25–32 | 1 (16.7%) |
| 33–40 | 2 (33.3%) |
| More than 40 | 1 (16.7%) |
| Gender | |
| Male | 3 (37.5%) |
| Female | 5 (62.5%) |
| Authorized to administer injections | |
| Yes | 8 (100.0%) |
| Education (licensed pharmacists only, n = 6), select all that apply | |
| BSc Pharmacy | 5 (83.3%) |
| Entry-to-practice PharmD | 1 (16.7%) |
| Date Used (YYYY/MM/DD) | Estimated Triage Time (mins) | Did You Refer the Patient? | What Was the Reason for Referring/Not Referring | If You Did Not Refer, What Was the Course of Action? |
|---|---|---|---|---|
| 2019/03/26 | 45* | Yes | “Needed yellow fever vaccine, proof of polio vaccination and malaria chemoprophylaxis” | |
| 2019/03/28 | 35* | Yes | “Needed yellow fever vaccine and proof of polio vaccination” | |
| 2019/04/20 | 15 | No | “Did not refer as not high risk” | “Patient had TwinRix® [combined hepatitis A and B vaccine] previously and decided to get Dukoral® [oral cholera vaccine]” |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, H.V.J.; Houle, S.K.D. Development and Testing of a Clinical Practice Framework for Pharmacists to Assess Patients’ Travel-Related Risks: The 5W Approach to Travel Risk Identification. Pharmacy 2019, 7, 159. https://doi.org/10.3390/pharmacy7040159
Fernandes HVJ, Houle SKD. Development and Testing of a Clinical Practice Framework for Pharmacists to Assess Patients’ Travel-Related Risks: The 5W Approach to Travel Risk Identification. Pharmacy. 2019; 7(4):159. https://doi.org/10.3390/pharmacy7040159
Chicago/Turabian StyleFernandes, Heidi V.J., and Sherilyn K.D. Houle. 2019. "Development and Testing of a Clinical Practice Framework for Pharmacists to Assess Patients’ Travel-Related Risks: The 5W Approach to Travel Risk Identification" Pharmacy 7, no. 4: 159. https://doi.org/10.3390/pharmacy7040159
APA StyleFernandes, H. V. J., & Houle, S. K. D. (2019). Development and Testing of a Clinical Practice Framework for Pharmacists to Assess Patients’ Travel-Related Risks: The 5W Approach to Travel Risk Identification. Pharmacy, 7(4), 159. https://doi.org/10.3390/pharmacy7040159