Co-Morbidities as Predictors of Airflow Limitation among Smokers in England



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Questionnaire
2.3. Data Analysis
2.4. Ethical Consideration
3. Results
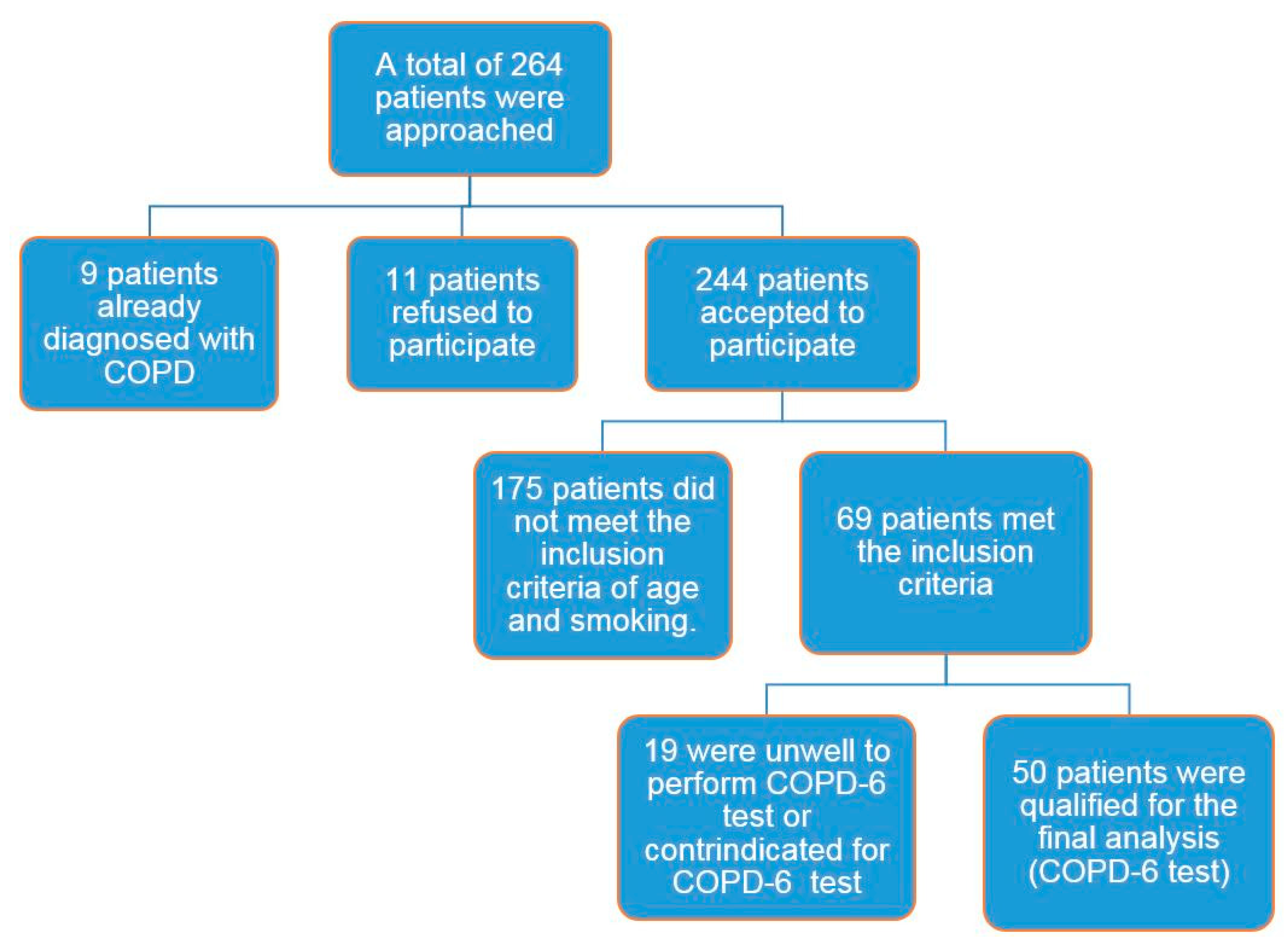
3.1. Participants’ Characteristics
3.2. COPD-6 Screening
3.3. Predictive Factors of Airflow Limitation
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A. Study Questionnaire
| Name: | |
| Date Of Birth: | |
| Age: | |
| Phone number: | |
| Ward: |
| Height: | |
| MRC: | 1/2/3/4/5 |
| Smoking status: | Y/N |
| Pack years: |
| Current or suspected respiratory infection | Y/N |
| Any antibiotics/prednisolone within the last 6 weeks | Y/N |
| Aneurysm (not treated) | Y/N |
| Unwell today, i.e., nausea, vomiting or pain | Y/N |
| Uncontrolled blood pressure | Y/N |
| Communication problems, i.e., dementia | Y/N |
| Ear problems, i.e., ear infection | Y/N |
| Eye problems, i.e., glaucoma | Y/N |
| Pregnancy | Y/N |
| Collapsed lung | Y/N |
| Haemoptysis of unknown cause | Y/N |
| Myocardial infarction or unstable heart condition | Y/N |
| Abdominal, chest, ear or eye surgery | Y/N |
| PE or Blood clot on the lung | Y/N |
| Stroke | Y/N |
| FEV1 | FEV1% Pred | FEV6 | FEV6% Pred | Ratio | |
| Effort 1 | |||||
| Effort 2 | |||||
| Effort 3 |
References
- Hesso, I.; Gebara, S.N.; Kayyali, R. Impact of community pharmacists in COPD management: Inhalation technique and medication adherence. Respir. Med. 2016, 118, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Depatment of Health (DH). An Outcomes Strategy for Chronic Obstructive Pulmonary Disease (COPD) and Asthma in England; Depatment of Health & Social Care: London, UK, 2011.
- Celli, B.R.; MacNee, W. ATS/ERS task force: Standards for the diagnosis and treatment of patients with COPD: A summary of the ATS/ERS position paper. Eur. Respir. J. 2004, 23, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Global Srategy for the Diagnosis Management and Prevention of Chronic Obstructive Pulmonary Disease, Updated 2015. Available online: http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf (accessed on 7 January 2018).
- Kayyali, R.; Odeh, B.; Frerichs, I.; Davies, N.; Perantoni, E.; D’arcy, S. COPD care delivery pathways in five European Union countries: Mapping and health care professionals’ perceptions. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2831. [Google Scholar] [CrossRef] [PubMed]
- Löfdahl, C. COPD and co-morbidities, with special emphasis on cardiovascular conditions. Clin. Respir. J. 2008, 2, 59–63. [Google Scholar] [CrossRef] [PubMed]
- MacNee, W. Systemic inflammatory biomarkers and co-morbidities of chronic obstructive pulmonary disease. Ann. Med. 2013, 45, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, H.; Watz, H. Systemic inflammation in chronic obstructive pulmonary disease and asthma: Relation with comorbidities. Proc. Am. Thorac. Soc. 2009, 6, 648–651. [Google Scholar] [CrossRef] [PubMed]
- COPD Strategy Group. Chronic Obstructive Pulmonary Disease (COPD) Strategy 2010–2015. Available online: www.cress.bics.nhs.uk/EasySiteWeb/GatewayLink.aspx?alId=1907 (accessed on 17 January 2018).
- NICE. Chronic Obstructive Pulmonary Disease—Casting Report—Implementing NICE Guidelines; NICE: London, UK, 2011. [Google Scholar]
- Stenton, C. The MRC breathlessness scale. Occup. Med. (Lond.) 2008, 58, 226–227. [Google Scholar] [CrossRef] [PubMed]
- Rosa, F.W.; Perez-Padilla, R.; Camelier, A.; Nascimento, O.A.; Menezes, A.M.B.; Jardim, J.R. Efficacy of the FEV1/FEV6 ratio compared to the FEV1/FVC ratio for the diagnosis of airway obstruction in subjects aged 40 years or over. Braz. J. Med. Biol. Res. 2007, 40, 1615–1621. [Google Scholar] [CrossRef] [PubMed]
- Ching, S.; Pang, Y.; Price, D.; Cheong, A.; Lee, P.; Irmi, I. Detection of airflow limitation using a handheld spirometer in a primary care setting. Respirology 2014, 19, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Fathima, M.; Naik-Panvelkar, P.; Saini, B.; Armour, C. The role of community pharmacists in screening and subsequent management of chronic respiratory diseases: A systematic review. Pharm. Pract. (Granada) 2013, 11, 228–245. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Twigg, M.; Thornley, T. Chronic obstructive pulmonary disease case finding by community pharmacists: A potential cost-effective public health intervention. Int. J. Pharm. Pract. 2015, 23, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Calverley, P.M.; Nordyke, R.J.; Halbert, R.; Isonaka, S.; Nonikov, D. Development of a population-based screening questionnaire for COPD. COPD J. Chronic Obstr. Pulm. Dis. 2005, 2, 225–232. [Google Scholar] [CrossRef]


{kind=link}
| Variables | No Airflow Limitation (n = 29) | Have Airflow Limitation (n = 21) | P-Values |
|---|---|---|---|
| Age, years (median) | 53 | 56 | |
| Age ≥ 60, n (%) | 8 (28%) | 9 (43%) | 0.336 |
| Age < 60, n (%) | 21 (72%) | 12 (57%) | |
| Female gender, n (%) | 19 (66%) | 11 (52%) | 0.371 |
| Male gender, n (%) | 10 (34%) | 10 (48%) | |
| Smoking history, pack-years | - | - | |
| <20, n (%) | 16 (55%) | 5 (24%) | 0.029 |
| ≥20, n (%) | 13 (45%) | 16 (76%) | |
| Respiratory symptoms, n (%) MRC breathlessness grade ≥3 | 12 (41%) | 15 (71%) | 0.039 |
| Presence of co-morbidities, n (%) | 20 (69%) | 20 (95%) | 0.025 |
| Co-Morbidity | No Airflow Limitation (n = 29) | Have Airflow Limitation (n = 21) |
|---|---|---|
| Hypertension (HTN), n (%) | 4 (14%) | 9 (43%) |
| Cardiovascular diseases, n (%) | 3 (10%) | 5 (24%) |
| Hyperlipidaemia, n (%) | 7 (24%) | 4 (19%) |
| Depression, n (%) | 5 (17%) | 10 (48%) |
| Diabetes, n (%) | 4 (14%) | 4 (19%) |
| Osteoporosis, n (%) | 2 (7%) | 3 (14%) |
| Peripheral Vascular Disease (PVD), n (%) | 6 (21%) | 3 (14%) |
| Predictors of Airflow Limitation in Smokers (n = 50) | |
|---|---|
| Independent variables | Odds ratio (95% CI) |
| Age ≥ 60 | 1.97 (0.600–6.45) |
| Gender (male) | 1.72 (0.55–5.45) |
| Smoking history ≥ 20 pack-years | 3.94 (1.13–13.64) |
| Presence of respiratory symptoms | 3.54 (1.06–11.77) |
| Presence of co-morbidities | 9 (1.04–77.81) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kayyali, R.; Hassan, Y.; Hesso, I.; Siva, R. Co-Morbidities as Predictors of Airflow Limitation among Smokers in England. Pharmacy 2018, 6, 45. https://doi.org/10.3390/pharmacy6020045
Kayyali R, Hassan Y, Hesso I, Siva R. Co-Morbidities as Predictors of Airflow Limitation among Smokers in England. Pharmacy. 2018; 6(2):45. https://doi.org/10.3390/pharmacy6020045
Chicago/Turabian StyleKayyali, Reem, Yusur Hassan, Iman Hesso, and Roshan Siva. 2018. "Co-Morbidities as Predictors of Airflow Limitation among Smokers in England" Pharmacy 6, no. 2: 45. https://doi.org/10.3390/pharmacy6020045
APA StyleKayyali, R., Hassan, Y., Hesso, I., & Siva, R. (2018). Co-Morbidities as Predictors of Airflow Limitation among Smokers in England. Pharmacy, 6(2), 45. https://doi.org/10.3390/pharmacy6020045