
Adverse Childhood Experiences and Prescription Stimulant Use in Adults: A Systematic Review

Abstract
1. Introduction
1.1. Nonmedical Prescription Stimulant Use
1.2. Adverse Childhood Experiences
2. Methods
2.1. Search and Retrieval
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- The study investigated the relationship between nonmedical prescription stimulant use and ACEs;
- The study included only adult participants;
- The sample size of the study was n > 1;
- The study was published in the last 10 years;
- The study was originally published in English;
- The study used an original or secondary dataset;
- The study was published in a peer-reviewed journal.
2.2.2. Exclusion Criteria
- The study did not explicitly identify nonmedical prescription stimulant misuse;
- The study did not explicitly examine the relationship between ACEs and nonmedical prescription stimulant use;
- The study did not include ACEs and prescription stimulants use, or misuse was investigated in nonadult samples (i.e., child and adolescent samples);
- Meta-analyses, systematic reviews, protocols for future research, and case studies were excluded;
- The study was not published in English;
- The study was not published in a peer-reviewed journal.
2.2.3. Data Extraction
3. Results
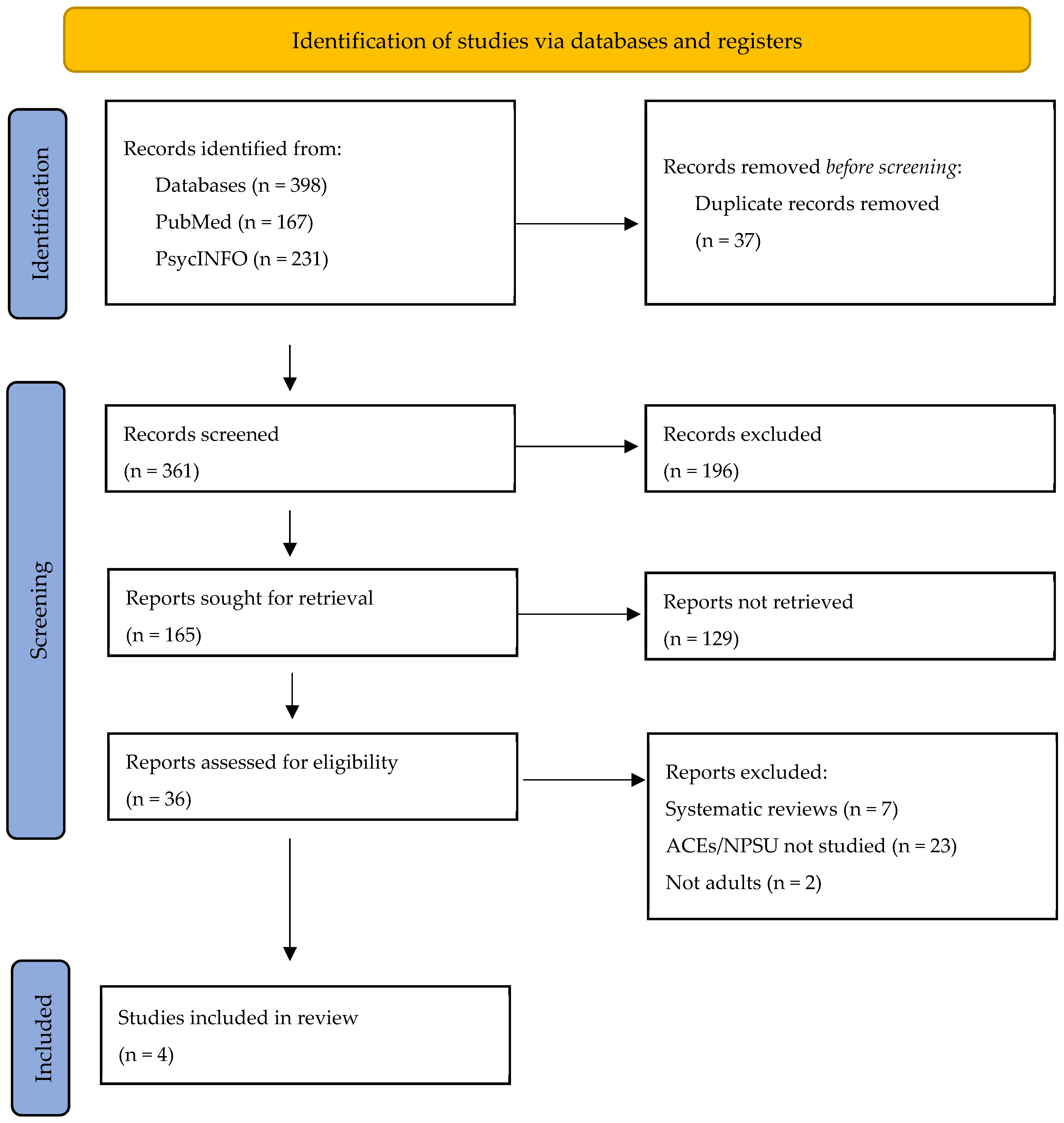
3.1. Study Selection
3.2. Summary of Included Articles
3.2.1. Review of NPSU and ACEs
3.2.2. Adverse Childhood Experiences and NPSU
3.2.3. Specific Prescription Stimulant Medications and ACEs
3.2.4. Summary of Demographic Findings: Age, Gender, Race, Ethnicity, Specific Populations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adler, L.A.; Dirks, B.; Deas, P.; Raychaudhuri, A.; Dauphin, M.; Saylor, K.; Weisler, R. Self-Reported quality of life in adults with attention-deficit/hyperactivity disorder and executive function impairment treated with lisdexamfetamine dimesylate: A randomized, double-blind, multicenter, placebo-controlled, parallel-group study. BMC Psychiatry 2013, 13, 253. [Google Scholar] [CrossRef] [PubMed]
- DuPaul, G.J.; Weyandt, L.L.; Rossi, J.S.; Vilardo, B.A.; O’dell, S.M.; Carson, K.M.; Verdi, G.; Swentosky, A. Double-Blind, Placebo-Controlled, Crossover Study of the Efficacy and Safety of Lisdexamfetamine Dimesylate in College Students with ADHD. J. Atten. Disord. 2012, 16, 202–220. [Google Scholar] [CrossRef] [PubMed]
- Weyandt, L.; Oster, D.; Marraccini, M.E.; Gudmundsdottir, B.; Munro, B.; Zavras, B.M.; Kuhar, B. Pharmacological interventions for adolescents and adults with ADHD: Stimulant and nonstimulant medications and misuse of prescription stimulants. Psychol. Res. Behav. Manag. 2014, 7, 223–249. [Google Scholar] [CrossRef]
- Lakhan, S.E.; Kirchgessner, A. Prescription stimulants in individuals with and without attention deficit hyperactivity disorder: Misuse, cognitive impact, and adverse effects. Brain Behav. 2012, 2, 661–677. [Google Scholar] [CrossRef] [PubMed]
- Weyandt, L.L.; Oster, D.R.; Gudmundsdottir, B.G.; Dupaul, G.J.; Anastopoulos, A.D. Neuropsychological functioning in college students with and without ADHD. Neuropsychology 2016, 31, 160–172. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Prescription Stimulant Misuse and Prevention Among Youth and Young Adults. p. PEP21–06-01–003, 2021, [Online]. Available online: https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/PEP21-06-01-003.pdf (accessed on 19 April 2023).
- Benson, K.; Flory, K.; Humphreys, K.L.; Lee, S.S. Misuse of Stimulant Medication Among College Students: A Comprehensive Review and Meta-analysis. Clin. Child Fam. Psychol. Rev. 2015, 18, 50–76. [Google Scholar] [CrossRef] [PubMed]
- Francis, A.R.; Weyandt, L.L.; Anastopoulos, A.D.; DuPaul, G.J.; Shepard, E. Outcomes and Predictors of Stimulant Misuse in College Students with and without ADHD. J. Atten. Disord. 2022, 26, 779–793. [Google Scholar] [CrossRef]
- Kennedy, S. Raising Awareness about Prescription and Stimulant Abuse in College Students through On-Campus Community Involvement Projects. J. Undergrad. Neurosci. Educ. 2018, 17, A50–A53. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30618499%0Ahttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC6312145 (accessed on 16 April 2023).
- Arria, A.M.; Geisner, I.M.; Cimini, M.D.; Kilmer, J.R.; Caldeira, K.M.; Barrall, A.L.; Vincent, K.B.; Fossos-Wong, N.; Yeh, J.-C.; Rhew, I.; et al. Perceived academic benefit is associated with nonmedical prescription stimulant use among college students. Addict. Behav. 2018, 76, 27–33. [Google Scholar] [CrossRef]
- Weyandt, L.L.; DuPaul, G.J. College Students with ADHD: Current Issues and Future Directions, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2012; p. XIII-122. [Google Scholar] [CrossRef]
- Weyandt, L.; DuPaul, G.J.; Verdi, G.; Rossi, J.S.; Swentosky, A.J.; Vilardo, B.S.; O’dell, S.M.; Carson, K.S. The Performance of College Students with and without ADHD: Neuropsychological, Academic, and Psychosocial Functioning. J. Psychopathol. Behav. Assess. 2013, 35, 421–435. [Google Scholar] [CrossRef]
- Weyandt, L.L.; Oster, D.R.; Marraccini, M.E.; Gudmundsdottir, B.G.; Munro, B.A.; Rathkey, E.S.; McCallum, A. Prescription stimulant medication misuse: Where are we and where do we go from here? Exp. Clin. Psychopharmacol. 2016, 24, 400–414. [Google Scholar] [CrossRef]
- Magnotti, S.B.; Beatty, A.; Bickford, E.; Channell, I.B.; Weyandt, L. Prescription Stimulant Misuse Among Nursing Students. J. Addict. Nurs. 2023, 34, 216–223. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. REPRINT OF: Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 2019, 56, 774–786. [Google Scholar] [CrossRef]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e356–e366. [Google Scholar] [CrossRef] [PubMed]
- Leza, L.; Siria, S.; López-Goñi, J.J.; Fernández-Montalvo, J. Adverse childhood experiences (ACEs) and substance use disorder (SUD): A scoping review. Drug Alcohol Depend. 2021, 221, 108563. [Google Scholar] [CrossRef] [PubMed]
- Emslie, G.J.; Kennard, B.D.; Mayes, T.L.; Nakonezny, P.A.; Zhu, L.; Tao, R.; Hughes, C.; Croarkin, P. Insomnia Moderates Outcome of Serotonin-Selective Reuptake Inhibitor Treatment in Depressed Youth. J. Child Adolesc. Psychopharmacol. 2012, 22, 21–28. [Google Scholar] [CrossRef]
- Pakdaman, S.; Unger, J.B.; Forster, M.; Rogers, C.J.; Sussman, S.Y.; Benjamin, S.M. Childhood Trauma and Prescription Drug Misuse in a College Population. Subst. Use Misuse 2021, 56, 140–144. [Google Scholar] [CrossRef]
- Merrick, M.T.; Ford, D.C.; Ports, K.A.; Guinn, A.S. Prevalence of Adverse Childhood Experiences From the 2011–2014 Behavioral Risk Factor Surveillance System in 23 States. JAMA Pediatr. 2018, 172, 1038–1044. [Google Scholar] [CrossRef] [PubMed]
- Cloitre, M.; Khan, C.; Mackintosh, M.A.; Garvert, D.W.; Henn-Haase, C.M.; Falvey, E.C.; Saito, J. Emotion regulation mediates the relationship between ACES and physical and mental health. Psychol. Trauma: Theory Res. Pract. Policy 2019, 11, 82–89. [Google Scholar] [CrossRef]
- Chandler, G.E.; Kalmakis, K.A.; Murtha, T. Screening Adults With Substance Use Disorder for Adverse Childhood Experiences. J. Addict. Nurs. 2018, 29, 172–178. [Google Scholar] [CrossRef]
- Tang, S.; Jones, C.M.; Wisdom, A.; Lin, H.-C.; Bacon, S.; Houry, D. Adverse childhood experiences and stimulant use disorders among adults in the United States. Psychiatry Res. 2021, 299, 113870. [Google Scholar] [CrossRef]
- Forster, M.; Grigsby, T.J.; Rogers, C.J.; Benjamin, S.M. The relationship between family-based adverse childhood experiences and substance use behaviors among a diverse sample of college students. Addict. Behav. 2018, 76, 298–304. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Fairman, R.T.; Vu, M.; Haardörfer, R.; Windle, M.; Berg, C.J. Prescription stimulant use among young adult college students: Who uses, why, and what are the consequences? J. Am. Coll. Health 2021, 69, 767–774. [Google Scholar] [CrossRef]
- Ruiz, E.; Beatty, A.; Weyandt, L. An Investigation of Diversity in Childhood and Adolescent Antidepressant Studies: A Systematic Review. J. Child Adolesc. Psychopharmacol. 2023, 33, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Menschner, C.; Maul, A. Key Ingredients for Successful Trauma-Informed Care Implementation. 2016; pp. 1–12. Available online: https://www.samhsa.gov/sites/default/files/programs_campaigns/childrens_mental_health/atc-whitepaper-040616.pdf (accessed on 10 April 2023).
- Mckenzie, A.; Meshkat, S.; Lui, L.M.; Ho, R.; Di Vincenzo, J.D.; Ceban, F.; Cao, B.; McIntyre, R.S. The effects of psychostimulants on cognitive functions in individuals with attention-deficit hyperactivity disorder: A systematic review. J. Psychiatr. Res. 2022, 149, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Schnarrs, P.W.; Stone, A.L.; Salcido, R.; Baldwin, A.; Georgiou, C.; Nemeroff, C.B. Differences in adverse childhood experiences (ACEs) and quality of physical and mental health between transgender and cisgender sexual minorities. J. Psychiatr. Res. 2019, 119, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schuler, M.; Evans-Polce, J.R.; Collins, L.R. Disparities in substance use behaviors and disorders among adult sexual minorities by age, gender, and sexual identity. J. Drug Alc. Dep. 2018, 189, 139–146. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Article | Sample | ACEs | Stimulant(s) | Age (M) | Gender (Female) | Race and/or Ethnicity |
|---|---|---|---|---|---|---|
| [19] | 3899 college students | Parental substance use & mental health; Verbal, physical, & sexual abuse; Homelessness | Adderall | 24.55 | 69.9% | Hispanic: 55% White: 27.9% Asian/Pacific Islander: 16% |
| [23] | 36,309 adults | Household: substance use, mental illness, incarceration, domestic violence, parental separation or divorce; Verbal, physical, emotional, & sexual abuse | Stimulant | N/A | N/A | N/A |
| [24] | 2953 college students | Household substance use; Domestic violence; Verbal, physical, & sexual abuse | Ritalin, Adderall | 21.34 | 73% | Hispanic: 37% White: 33%; Black: 4% Asian/Pacific Islander: 15% Multiracial 7%; Other: 4% |
| [26] | 3418 college students | Parental mental health & substance use; Sexual, physical, & emotional abuse; Maltreatment | Adderall, Vyvanse, Ritalin, Concerta | 20.72 | 54.8% | White: 82% Nonwhite: 18% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beatty, A.; Shepard, E.; Bickford, E.; Weyandt, L. Adverse Childhood Experiences and Prescription Stimulant Use in Adults: A Systematic Review. Pharmacy 2024, 12, 52. https://doi.org/10.3390/pharmacy12020052
Beatty A, Shepard E, Bickford E, Weyandt L. Adverse Childhood Experiences and Prescription Stimulant Use in Adults: A Systematic Review. Pharmacy. 2024; 12(2):52. https://doi.org/10.3390/pharmacy12020052
Chicago/Turabian StyleBeatty, Avery, Emily Shepard, Erek Bickford, and Lisa Weyandt. 2024. "Adverse Childhood Experiences and Prescription Stimulant Use in Adults: A Systematic Review" Pharmacy 12, no. 2: 52. https://doi.org/10.3390/pharmacy12020052
APA StyleBeatty, A., Shepard, E., Bickford, E., & Weyandt, L. (2024). Adverse Childhood Experiences and Prescription Stimulant Use in Adults: A Systematic Review. Pharmacy, 12(2), 52. https://doi.org/10.3390/pharmacy12020052