
The Impact of Glucagon-like Peptide 1 Receptor Agonists on Obstructive Sleep Apnoea: A Scoping Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
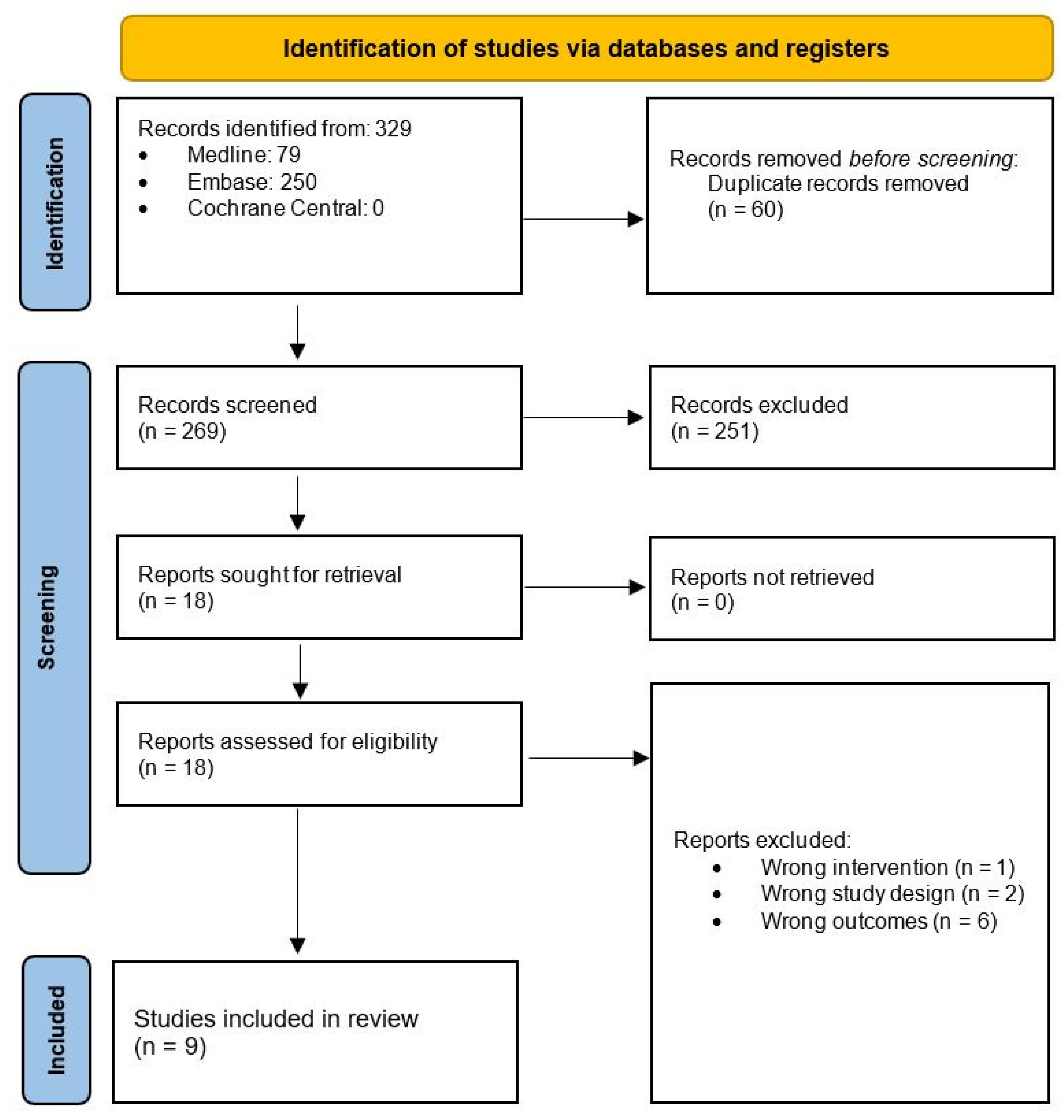
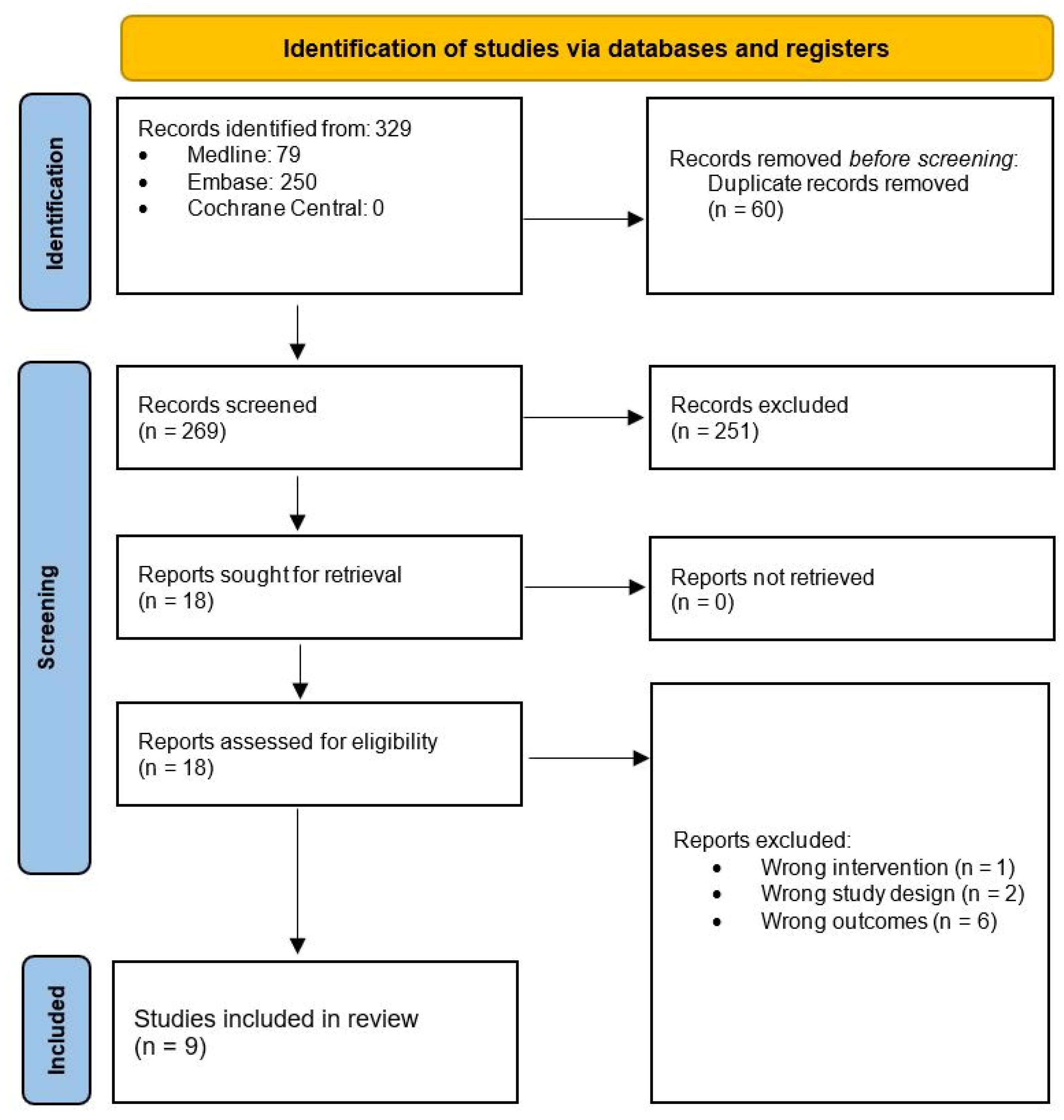
2.3. Literature Screening and Data Extraction
2.4. Methodological Quality and Risk of Bias Assessment
3. Results
3.1. Overview of Included Studies
3.2. GLP-1RA and Obstructive Sleep Apnoea and Hypopneoa Syndrome (OSAHS)
3.3. GLP-1RA and Daytime Sleepiness
3.4. Quality and Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Search Query
- exp glucagon like peptide 1 receptor agonist/
- ((glucagon like peptide 1 receptor* or glucagon like peptide one receptor* or GLP-1RA*) adj3 (agonist* or antagonist* or medication* or drug* or agent* or analog*)).mp.
- (semaglutide or liraglutide or exenatide or albiglutide or dulaglutide or lixisenatide or Ozempic or Wegovy or Rybelsus or Saxenda or Adlyxin or Trulicity or Mounjaro).mp.
- 1 or 2 or 3
- exp *sleep disordered breathing/
- (sleep* or apn?ea or obesity hypoventilation syndrome*).ti,ab,kf.
- 5 or 6
- 4 and 7
- 8 not animal experiment/
- 9 not conference abstract.pt.
References
- Sultana, R.; Sissoho, F.; Kaushik, V.P.; Raji, M.A. The Case for Early Use of Glucagon-like Peptide-1 Receptor Agonists in Obstructive Sleep Apnea Patients with Comorbid Diabetes and Metabolic Syndrome. Life 2022, 12, 1222. [Google Scholar] [CrossRef] [PubMed]
- Veasey, S.C.; Rosen, I.M. Obstructive Sleep Apnea in Adults. N. Engl. J. Med. 2019, 380, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- García de Lucas, M.D.; Olalla Sierra, J.; Piña Fernández, J. Liraglutide treatment in a patient with HIV, type 2 diabetes and sleep apnoea-hypopnoea syndrome. Diabetes Metab. 2015, 41, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Blackman, A.; Foster, G.D.; Zammit, G.; Rosenberg, R.; Aronne, L.; Wadden, T.; Claudius, B.; Jensen, C.B.; Mignot, E. Effect of liraglutide 3.0 mg in individuals with obesity and moderate or severe obstructive sleep apnea: The SCALE Sleep Apnea randomized clinical trial. Int. J. Obes. 2016, 40, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Yuan, H.; Wang, D.; Yuan, Q.; Shi, X. Effects of liraglutide on sleep-disordered breathing and diabetic microangiopathy in patients with type 2 diabetes mellitus and obstructive sleep apnea-hypopnea syndrome. Chin. J. Diabetes Mellit. 2020, 12, 86–91. [Google Scholar]
- Jiang, W.; Li, W.; Cheng, J.; Li, W.; Cheng, F. Efficacy and safety of liraglutide in patients with type 2 diabetes mellitus and severe obstructive sleep apnea. Sleep Breath. 2022, 27, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.S.; Simakajornboon, N.; Szczesniak, R.V. Treatment of obstructive sleep apnea with glucagon like peptide-1 receptor agonist. In C30 New Insights in Pathogenesis of Sleep Disordered Breathing; American Thoracic Society: San Diego, CA, USA, 2015; p. A4144-A. [Google Scholar]
- O’Donnell, C.; Crilly, S.; O’Mahony, A.; O’Riordan, B.; Traynor, M.; Gitau, R.; McDonald, K.; Ledwidge, M.; O’Shea, D.; Murphy, D.J.; et al. Continuous positive airway pressure but not Liraglutide-mediated weight loss improves early cardiovascular disease in obstructive sleep apnea: Data from a randomized proof-of-concept study. medRxiv. 2023. [Google Scholar] [CrossRef]
- Sprung, V.S.; Kemp, G.J.; Wilding, J.P.; Adams, V.; Murphy, K.; Burgess, M.; Emegbo, S.; Thomas, M.; Needham, A.J.; Weimken, A.; et al. Randomised, Controlled Multicentre trial of 26 weeks subcutaneous liraglutide (a glucagon-like peptide-1 receptor Agonist), with or without continuous positive airway pressure (CPAP), in patients with type 2 diabetes mellitus (T2DM) and obstructive sleep apnoEa (OSA)(ROMANCE): Study protocol assessing the effects of weight loss on the apnea–hypnoea index (AHI). BMJ Open 2020, 10, e038856. [Google Scholar] [PubMed]
- Idris, I.; Abdulla, H.; Tilbrook, S.; Dean, R.; Ali, N. Exenatide improves excessive daytime sleepiness and wakefulness in obese patients with type 2 diabetes without obstructive sleep apnoea. J. Sleep Res. 2013, 22, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Peralta, F.; Abreu, C.; Castro, J.C.; Alcarria, E.; Cruz-Bravo, M.; Garcia-Llorente, M.J.; Albornos, C.; Moreno, C.; Cepeda, M.; Almodóvar, F. An association between liraglutide treatment and reduction in excessive daytime sleepiness in obese subjects with type 2 diabetes. BMC Endocr. Disord. 2015, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Doerr, E.; Stockman, M.C.; Rizo, I. Mechanism of Glucagon-Like Peptide 1 Improvements in Type 2 Diabetes Mellitus and Obesity. Curr. Obes. Rep. 2019, 8, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Papaetis, G.S. GLP-1 receptor agonists, SGLT-2 inhibitors, and obstructive sleep apnoea: Can new allies face an old enemy? Arch. Med. Sci. Atheroscler. Dis. 2023, 8, e19. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Year | Study Type | Location | Intervention | Cohort | Level of Evidence (Oxford Centre for Evidence-Based Medicine; OCEBM) |
|---|---|---|---|---|---|---|
| García de Lucas [4] | 2015 | Case report | Spain | Off-label liraglutide commencing at 0.6 mg/day and uptitrated to 1.2 mg/day | 62-year-old man with multiple comorbidities including Human immunodeficiency virus (HIV), type 2 diabetes mellitus, hyperlipidaemia, obesity and moderate sleep apnoea | 4 |
| Blackman [5] | 2016 | Randomised controlled trial | Canada, USA | 32 weeks of liraglutide 3.0 mg compared to placebo in addition to diet and exercise | Obese adults aged between 18–64 with diagnosis of moderate or severe obstructive sleep apnoea and unwilling or unable to use continuous positive airway pressure (CPAP) devices | 1b |
| Liu [6] | 2020 | Retrospective non randomised clinical trial | China | Liraglutide compared to conventional anti-hyperglycaemic drugs | Adults with type 2 diabetes mellitus and obstructive sleep apnoea | 2b |
| Jiang [7] | 2022 | Randomised controlled trial | China | Off-label liraglutide commencing at 0.6 mg/day and uptitrated to 1.8 mg/day | Adults aged 18–75 with diagnosis of type 2 diabetes mellitus not being treated with dipeptidyl peptidase IV (DPP-IV) or GLP1-RA treatment and severe obstructive sleep apnoea currently being managed with CPAP. | 1b |
| Amin [8] | 2015 | Abstract of randomised controlled trial | USA | Undisclosed GLP-1RA starting at 0.6 mg/day and uptitrating to 1.8 ng/day | Adults with moderate obstructive sleep apnoea | 5 |
| O’Donnell [9] | 2023 | Randomised proof of concept study | Ireland | Off-label liraglutide regimen alone compared to liraglutide and CPAP compared to CPAP alone. | Non-diabetic patients with moderate to severe obstructive sleep apnoea | 2b |
| Sprung [10] | 2020 | Protocol | UK | Liraglutide 1.8 mg/day compared to liraglutide and CPAP compared to CPAP alone | Patients with newly diagnosed obstructive sleep apnoea, obesity and type 2 diabetes mellitus | 5 |
| Idris [11] | 2013 | Exploratory placebo controlled clinical trial | UK | Exenatide therapy was initiated at a 5μg twice-daily dose by subcutaneous injection and increased to 10 μg twice daily within 4 weeks of treatment initiation. | Obese adult patients with diabetes but no formal diagnosis of obstructive sleep apnoea | 3b |
| Gomez-Peralta [12] | 2015 | Retrospective non randomised clinical trial | Spain | Liraglutide | Obese adult patients with type 2 diabetes | 2b |
| Study | Representative of the Exposed Cohort | Selection of External Control/Non-Exposed Cohort | Ascertainment of Exposure | Outcome of Interest not Present at the Start of the Study | Study Controls for Intervention of GLP-1RA | Study Control for External Confounders | Assessment of Outcomes/Ascertainment of Exposure | Sufficient Follow-Up/Same Method of Ascertainment for Cases and Controls | Adequacy of Follow-Up/Non-Response Rate | Total Score (/9) |
|---|---|---|---|---|---|---|---|---|---|---|
| García de Lucas 2015 [4] | − | − | + | − | − | − | + | − | − | 2 |
| Blackman 2016 [5] | − | + | + | − | + | + | + | − | − | 5 |
| Liu 2020 [6] | − | − | + | − | + | − | + | − | − | 3 |
| Jiang 2022 [7] | − | + | + | − | + | + | + | − | − | 5 |
| Amin 2015 [8] | − | − | + | − | + | − | + | − | − | 3 |
| O’Donnell 2023 [9] | − | + | + | − | + | + | + | − | − | 5 |
| Sprung 2020 [10] | − | − | + | − | + | − | + | − | − | 3 |
| Idris 2013 [11] | − | − | + | + | − | + | + | − | − | 4 |
| Gomez-Peralta 2015 [12] | − | + | + | + | − | − | + | − | − | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, K.D.R.; Le, K.; Foo, F. The Impact of Glucagon-like Peptide 1 Receptor Agonists on Obstructive Sleep Apnoea: A Scoping Review. Pharmacy 2024, 12, 11. https://doi.org/10.3390/pharmacy12010011
Le KDR, Le K, Foo F. The Impact of Glucagon-like Peptide 1 Receptor Agonists on Obstructive Sleep Apnoea: A Scoping Review. Pharmacy. 2024; 12(1):11. https://doi.org/10.3390/pharmacy12010011
Chicago/Turabian StyleLe, Khang Duy Ricky, Kelvin Le, and Felicia Foo. 2024. "The Impact of Glucagon-like Peptide 1 Receptor Agonists on Obstructive Sleep Apnoea: A Scoping Review" Pharmacy 12, no. 1: 11. https://doi.org/10.3390/pharmacy12010011
APA StyleLe, K. D. R., Le, K., & Foo, F. (2024). The Impact of Glucagon-like Peptide 1 Receptor Agonists on Obstructive Sleep Apnoea: A Scoping Review. Pharmacy, 12(1), 11. https://doi.org/10.3390/pharmacy12010011