
“There Is Method to This Madness” A Qualitative Investigation of Home Medication Management by Older Adults



Abstract
1. Introduction
2. Materials and Methods
Data Analysis
3. Results
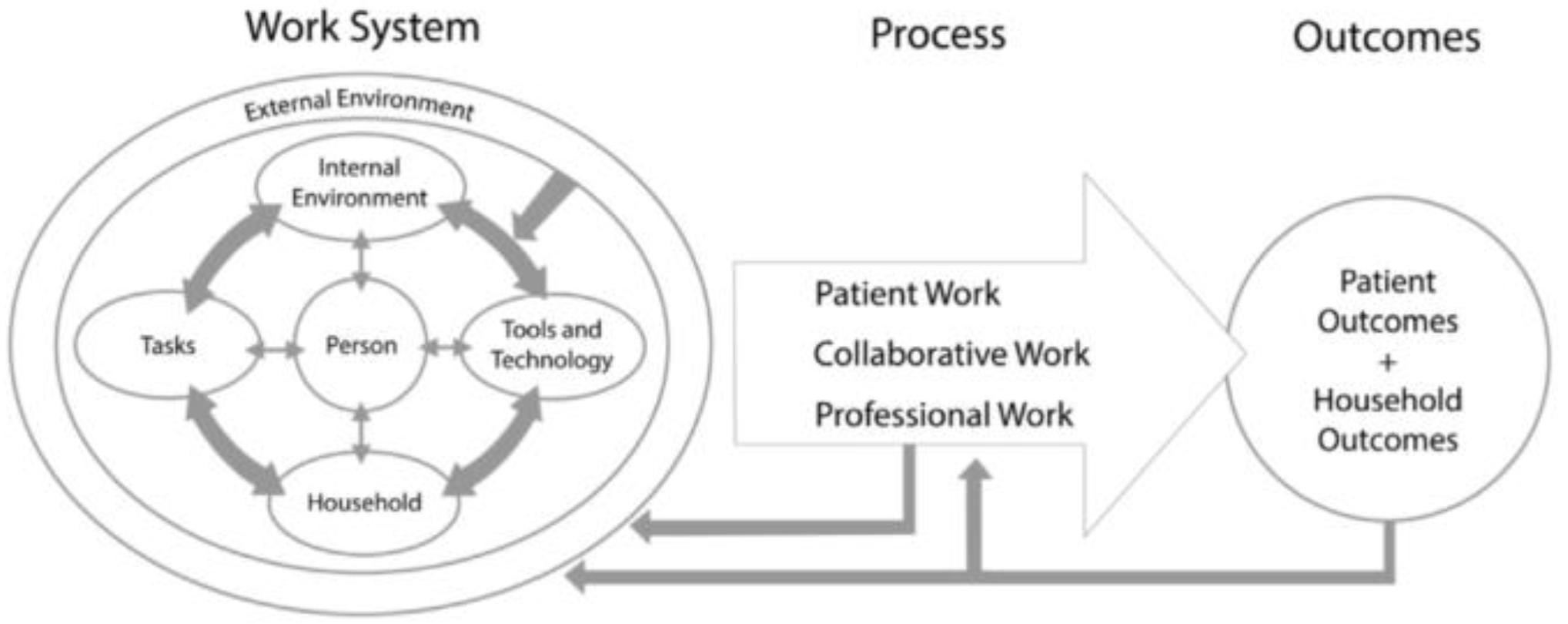
3.1. The Home Medication Management Work System
3.1.1. Person
3.1.2. Tools and Technology
“…that’s [my medication list] in my purse… the first time the [pharmacy staff] printed it out for me.”2W [medication list]
“I took the information off of the bottle, the pharmacy bottle [and put them in a grid] … I just did that [the grid] myself with a ruler [on paper].”7M [medication list]
“…having trouble with swallowing some of the pills so I use a pill cutter.”3M [pill cutter]
“if I Google [check the internet for] the number [on the pill], I can find out what the med is”5W [internet]
3.1.3. Household
“She [my wife] reminds me to take them [my drugs].”11M [Others in household] [routine cue]
“Oh my husband will sit there and he says, “Did you take your pills?”5W [Others in household] [routine cue]
“My husband has a medication that’s costing him a hundred and fifty bucks every time he refills it. That’s out-of-pocket. That’s not what the insurance company kicks in behind him. Really?”9W [cost concern]
“…you fall into a hole [donut hole; a coverage gap in most Medicare drug plans]… Do I want to pay for my [meds]? Well, living in Iowa, you know how cold it was last winter? It was cold. Do I want to eat? Do I want to stay warm? I won’t take my meds.”11M [cost-concerns]
“I think $5 a week would be pretty expensive. Or $10 a week would be expensive. That would be $520 a year. I could handle $120 but not the $520. So I could call and find out and maybe start the pill thing. That would be pretty convenient. I think I need help. I really do. It’s just getting very confusing sometimes. Especially if I run out of pills and I don’t have them, or vacations. I wish that the pill thing [pharmacy prescription medicine pre-packaging service] would be for free.”12M [cost-concerns]
3.2. Home Medication Management Processes
3.2.1. Patient Work
“Like I go through mine and I make sure that I have … Well, there’s a half of pill that I take for my heart. I make sure that’s in there. I make sure my [brand name medication] is in there. I make sure my metformin is. I take one blue pill. I put them in a little dish and kind of spread them apart and I take three of these. I make sure there’s three of those in there.”12M [medication sorting]
“I think I portioned them all out and then I just take whatever … I don’t have the original bottles on those. I just de-cap them, I’d say. But I could tell you probably what they are, but I don’t take those very often.”6W [repackaging]
“When I get up, I take my medications where I brush my teeth.”4W [routine cue]
“sometimes you have to communicate with your physician when they give you a prescription and it might be a case of doing more harm than good. He started me out originally on one kind of high blood pressure medicine and I realized that I was coughing all the time and it was giving me a chronic cough. I finally said I don’t think this one’s a good one for me. Then he switched it and then I stopped coughing.”4W [monitoring]
“as we get older, we get confused about our meds and especially if you have two that look very similar to each other. I know to look on them and there’s different numbers on there, then I also know that if I Google the number, I can find out what the med is.”5W [verification]
3.2.2. Collaborative Work
“Well, and I think, you know, docs [doctors] can fall into ruts, too. I mean, you know, I’ve not ever had a bad doctor, but you know, they get into routines, so they just, you know, “Oh, it’s Mary. Okay. Well, she’s … yeah. Yeah. She’s still overweight. Yeah, she’s still got… oh, yeah … Her bloodwork’s good. Okay. Renew her meds. Done,” without thinking, “Oh, she’s taken that med for how long?” You know, that kind of thing.”9W [medication inertia]
“To me, a pharmacy is a trust issue. I don’t know what it’s like to go to [chain pharmacies]. I go to [my pharmacy], and I’ve gone there for 40 years. Why would I change?”9W [trust]
3.3. Outcomes: Personally Important Well-Being Goals of Home Medication Management
“…they [insurance plan] were pretty insistent that they wanted to do mail-order meds. And I finally yelled and said, “Do I have to change companies? How many times do I have to say ‘no’?” To me, that doesn’t make sense. I need to deal with somebody locally because if I’ve got a question, I want to be able to call. I like knowing where my meds come from.”9W [control over medication supply]
3.4. Interpretation across the SAHMM Domains: “There Is Method to This Madness”
“That might be my husband’s. Yeah. That’s why it’s [medication container] upside down, ‘cause it’s his. That’s his way, he knows that he took it. The next time he takes it, he flips it up. It’s his little system. I just leave it alone.”5W [there is method to this madness]
4. Discussion
4.1. Implications for Primary Care
4.2. Limitations
4.3. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Guide
- What is the hardest part about managing your medications at home?
- What do you do to make managing your medications easier?
- Have you ever had something happen with your medications where you had to call the doctor or pharmacist?
- What are your thoughts about meeting with a pharmacist about your medications?
- Where do you keep your medicines? What about OTCs, vitamins, others?
- What is your process during a typical day?
- Does anyone help you with managing your medicines? If so, please describe how that occurs.
- Do you keep a list or write anything down to help?
- What tools, such as a med box do you use?
- Do you have any tricks or cues to help you manage your medications?
- Have you ever had a mix-up with your medicines or how you take them? Could you describe that?
References
- da Silva, A.F.; de Paula Silva, J. Polypharmacy, automedication, and the use of potentially inappropriate medications: Cause of intoxications in the elderly. Rev. Med. Minas Gerais 2022, 32, e32101. [Google Scholar] [CrossRef]
- Young, E.H.; Pan, S.; Yap, A.G.; Reveles, K.R.; Bhakta, K. Polypharmacy prevalence in older adults seen in United States physician offices from 2009 to 2016. PLoS ONE 2021, 16, e0255642. [Google Scholar] [CrossRef] [PubMed]
- Charlesworth, C.J.; Smit, E.; Lee, D.S.H.; Alramadhan, F.; Odden, M.C. Polypharmacy Among Adults Aged 65 Years and Older in the United States: 1988–2010. J. Gerontol. Ser. A 2015, 70, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Schöttker, B.; Muhlack, D.C.; Hoppe, L.K.; Holleczek, B.; Brenner, H. Updated analysis on polypharmacy and mortality from the ESTHER study. Eur. J. Clin. Pharmacol. 2018, 74, 981–982. [Google Scholar] [CrossRef]
- Leelakanok, N.; Holcombe, A.L.; Lund, B.C.; Gu, X.; Schweizer, M.L. Association between polypharmacy and death: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 2017, 57, 729–738.e10. [Google Scholar] [CrossRef]
- Lu, W.H.; Wen, Y.W.; Chen, L.K.; Hsiao, F.Y. Effect of polypharmacy, potentially inappropriate medications and anticholinergic burden on clinical out-comes: A retrospective cohort study. Can. Med. Assoc. J. 2015, 187, E130. [Google Scholar] [CrossRef]
- Sganga, F.; Landi, F.; Ruggiero, C.; Corsonello, A.; Vetrano, D.L.; Lattanzio, F.; Cherubini, A.; Bernabei, R.; Onder, G. Polypharmacy and health outcomes among older adults discharged from hospital: Results from the CRIME study. Geriatr. Gerontol. Int. 2015, 15, 141–146. [Google Scholar] [CrossRef]
- Payne, R.A.; Abel, G.; Avery, A.J.; Mercer, S.W.; Roland, M.O. Is polypharmacy always hazardous? A retrospective cohort analysis using linked electronic health records from primary and secondary care. Br. J. Clin. Pharmacol. 2014, 77, 1073–1082. [Google Scholar] [CrossRef]
- Chang, T.I.; Park, H.; Kim, D.W.; Jeon, E.K.; Rhee, C.M.; Kalantar-Zadeh, K.; Kang, E.W.; Kang, S.-W.; Han, S.H. Polypharmacy, hospitalization, and mortality risk: A nationwide cohort study. Sci. Rep. 2020, 10, 18964. [Google Scholar] [CrossRef]
- Lee, E.H.; Park, J.O.; Cho, J.P.; Lee, C.A. Prioritising Risk Factors for Prescription Drug Poisoning Among Older Adults: A Multi-Method Study. Int. J. Environ. Res. Public Health 2021, 18, 5948. [Google Scholar] [CrossRef]
- A Mohammed, M.; Moles, R.J.; Chen, T. Medication-related burden and patients’ lived experience with medicine: A systematic review and metasynthesis of qualitative studies. BMJ Open 2016, 6, e010035. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, S.J.; Ramalho de Oliveira, D. Understanding the meaning of medications for patients: The medication experience. Pharm. World Sci. 2008, 30, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Witry, M.; Parry, R.; McDonough, R.; Deninger, M. Analysis of medication adherence-related notes from a service-oriented community pharmacy. Res. Soc. Adm. Pharm. 2018, 14, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.A.; Duwe, E.A.G. Prescribing Providers Estimate Patients’ Adherence to Hypertension and Type 2 Diabetes Medications from Patients’ Medication-Taking Routines: An Observational Study. J. Gen. Intern. Med. 2019, 34, 1688–1690. [Google Scholar] [CrossRef]
- Holden, R.J.; Schubert, C.C.; Mickelson, R.S. The patient work system: An analysis of self-care performance barriers among elderly heart failure patients and their informal caregivers. Appl. Ergon. 2015, 47, 133–150. [Google Scholar] [CrossRef]
- Mickelson, R.S.; Holden, R.J. Medication management strategies used by older adults with heart failure: A systems-based analysis. Eur. J. Cardiovasc. Nurs. 2018, 17, 418–428. [Google Scholar] [CrossRef]
- Holden, R.J.; Valdez, R.S.; Schubert, C.C.; Thompson, M.J.; Hundt, A.S. Macroergonomic factors in the patient work system: Examining the context of patients with chronic illness. Ergonomics 2017, 60, 26–43. [Google Scholar] [CrossRef]
- Doucette, W.R.; Vinel, S.; Pennathur, P. Initial development of the Systems Approach to Home Medication Management (SAHMM) model. Res. Soc. Adm. Pharm. 2017, 13, 39–47. [Google Scholar] [CrossRef]
- Carayon, P.; Karsh, B.-T.; Gurses, A.P.; Holden, R.J.; Hoonakker, P.; Hundt, A.S.; Montague, E.; Rodriguez, A.J.; Wetterneck, T.B. Macroergonomics in Health Care Quality and Patient Safety. Rev. Hum. Factors Ergon. 2013, 8, 4–54. [Google Scholar] [CrossRef]
- Carayon, P.; Wetterneck, T.B.; Rivera-Rodriguez, A.J.; Hundt, A.S.; Hoonakker, P.; Holden, R.; Gurses, A.P. Human factors systems approach to healthcare quality and patient safety. Appl. Ergon. 2014, 45, 14–25. [Google Scholar] [CrossRef]
- Holden, R.J.; Valdez, R.S. Conceptualizing the patient work system, Part B: Macroergonomic challenges. In Proceedings of the 11th International Symposium on Human Factors in Organizational Design and Management-XI Nordic Ergonomics Society Annual Conference, Copenhagen, Denmark, 17–20 August 2014. [Google Scholar]
- Schwartz, J.K. Pillbox use, satisfaction, and effectiveness among persons with chronic health conditions. Assist. Technol. 2017, 29, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Tordoff, J.; Simonsen, K.; Thomson, W.M.; Norris, P.T. It’s just routine.” A qualitative study of medicine-taking amongst older people in New Zealand. Pharm. World Sci. 2010, 32, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.J.; Van Oss, T. Using Daily Routines to Promote Medication Adherence in Older Adults. Am. J. Occup. Ther. 2013, 67, 91–99. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Boeije, H. A Purposeful Approach to the Constant Comparative Method in the Analysis of Qualitative Interviews. Qual. Quant. 2002, 36, 391–409. [Google Scholar] [CrossRef]
- Carayon, P. Sociotechnical systems approach to healthcare quality and patient safety. Work 2012, 41, 3850–3854. [Google Scholar] [CrossRef]
- Burish, T.G.; Carey, M.P.; Wallston, K.A.; Stein, M.J.; Jamison, R.N.; Lyles, J.N. Health Locus of Control and Chronic Disease: An External Orientation May Be Advantageous. J. Soc. Clin. Psychol. 1984, 2, 326–332. [Google Scholar] [CrossRef]
- Notenboom, K.; Beers, E.; Riet-Nales, D.A.; Egberts, T.; Leufkens, H.G.M.; Jansen, P.A.F.; Bouvy, M. Practical Problems with Medication Use that Older People Experience: A Qualitative Study. J. Am. Geriatr. Soc. 2014, 62, 2339–2344. [Google Scholar] [CrossRef]
- Synnes, O.; Orøy, A.J.; Råheim, M.; Bachmann, L.; Ekra, E.M.R.; Gjengedal, E.; Høie, M.; Jørgensen, E.; Michaelsen, R.K.A.; Sundal, H.; et al. Finding ways to carry on: Stories of vulnerability in chronic illness. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1819635. [Google Scholar] [CrossRef]
- Affleck, G.; Tennen, H.; Pfeiffer, C.; Fifield, J. Appraisals of control and predictability in adapting to a chronic disease. J. Personal. Soc. Psychol. 1987, 53, 273. [Google Scholar] [CrossRef]
- Stanton, A.L.; Revenson, T.A.; Tennen, H. Health Psychology: Psychological Adjustment to Chronic Disease. Annu. Rev. Psychol. 2007, 58, 565–592. [Google Scholar] [CrossRef] [PubMed]
- Dills, H.; Shah, K.; Messinger-Rapport, B.; Bradford, K.; Syed, Q. Deprescribing Medications for Chronic Diseases Management in Primary Care Settings: A Systematic Review of Randomized Controlled Trials. J. Am. Med. Dir. Assoc. 2018, 19, 923–935.e2. [Google Scholar] [CrossRef] [PubMed]
- Dharmarajan, T.S.; Choi, H.; Hossain, N.; Munasinghe, U.; Lakhi, F.; Lourdusamy, D.; Onuoha, S.; Murakonda, P.; Skokowska-Lebelt, A.; Kanagala, M.; et al. Deprescribing as a clinical improvement focus. J. Am. Med. Dir. Assoc. Assoc. 2020, 21, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Kruse, W.; Rampmaier, J.; Frauenrath-Volkers, C.; Volkert, D.; Wankmüller, I.; Micol, W.; Oster, P.; Schlierf, G. Drug-prescribing patterns in old age. Eur. J. Clin. Pharmacol. 1991, 41, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, I. Patients are experts in their own field: The interests of patients and healthcare professionals are intertwined. BMJ 2003, 326, 1276–1277. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, R. The expert patient: A new approach to chronic disease management for the twenty-first century. Clin. Med. 2002, 2, 227–229. [Google Scholar] [CrossRef]
- Gallagher, K.M.; Updegraff, J.A. Health Message Framing Effects on Attitudes, Intentions, and Behavior: A Meta-analytic Review. Ann. Behav. Med. 2011, 43, 101–116. [Google Scholar] [CrossRef]
- Stuijt, C.; Bekker, C.; Bemt, B.V.D.; Karapinar, F. Effect of medication reconciliation on patient reported potential adverse events after hospital discharge. Res. Soc. Adm. Pharm. 2021, 17, 1426–1432. [Google Scholar] [CrossRef]
- Hilmer, S.N.; Gnjidic, D.; Le Couteur, D.G. Thinking through the medication list: Appropriate prescribing and depre-scribing in robust and frail older patients. Aust. Fam. Physician 2012, 41, 924–928. [Google Scholar]
- Wickens, C.D.; Gordon, S.E.; Liu, Y.; Lee, J. An Introduction to Human Factors Engineering; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2004; Volume 2. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age | Gender | Oral Medications | Storage Location and Process | Pillbox/Med Organizer |
|---|---|---|---|---|---|
| 1W | 91 | W | 5 | Kitchen: General medication shelf in the kitchen area; uses dining table to sort meds and fill pillbox Bathroom: Medicine cabinet | Yes; 7-day organizer with AM/PM compartments |
| 2W | 68 | W | 7 | Kitchen: dedicated tub Bedroom: on nightstand | Yes; 7-day organizer with AM/PM compartments |
| 3M | 84 | M | 7 | Kitchen: Counter-top and dining table Bathroom: Medicine cabinet | Yes; 7-day organizer and a second filled two days at a time for AM/PM supplements |
| 4W | 63 | W | 4 | Bathroom: Medicine Cabinet—stacks all medications in the cabinet with the current medications placed in front for easy reach | No; takes medications directly out of the vials |
| 5W | 62 | W | 5 | Kitchen: Dedicated medicine basket kept on a counter-top | Yes, Both bottles and pillboxes, and sets out doses |
| 6W | 89 | W | 10 | Kitchen: top of microwave, uses repurposed bottles and dish with pills Bedroom: Drawer | Yes; 7-day organizer with AM/PM compartments; uses 4 |
| 7M | 74 | M | 10 | Kitchen: Dedicated cabinet | Yes; 7-day organizer with AM/PM |
| 8W | 85 | W | 13 | Kitchen: Counter-top Bedroom: Drawer, in a clear plastic bag | Yes; 7-day organizers with AM/PM compartments; uses 2 |
| 9W | 70 | W | 6 | Kitchen: Dedicated Cabinet, uses table weekly to sort and fill organizer; Bathroom: stores additional medications | Yes; 7-day organizer |
| 10W | 74 | W | 6 | Kitchen: Counter-top Bathroom: Dedicated cabinet, with separate sides for morning and evening medications in the cabinet | No; takes medication directly out of vial. Uses pill box only when traveling |
| 11M | 64 | M | 5 | Kitchen: Cupboard—keeps medications in a vial; refills pill boxes from vials weekly | Yes; 7-day pill organizer; uses 2 |
| 12M | 66 | M | 15 | Kitchen: Dedicated plastic bag placed on counter-top | Yes; 7-day organizer with 4-daily doses |
| Home Medication Management Components | Quotes |
|---|---|
| Person | Older adults aged 55 or older who are long-term medication users for managing one or more chronic conditions. “remembering to take them [medications] is probably the hardest thing I have just ‘cause I get sidetracked and I’ve noticed I don’t remember things as well, so I guess that’s why I would say I’m getting older and easily distracted.” 5W [forgetting] |
| Tools and Technology | “I try to update my medication list if I’m doing something different or if they’ve added something to my [medications].” 6W [Medication list] “I had one off of the computer, but my computer word processor’s not working right now…” 7M [medication list-updating] “I like to Google things on the internet and I looked to see what any side effects would be.” 10W [internet] |
| Household | “the medicine cabinet is in the bathroom. So, let’s go to the bathroom first. I also have some in the kitchen. Those are the ones I normally take once a day or twice a day.” 10W [storage location] “It’s like when our kids are here, all of a sudden, our whole routine was helter-skelter, but we got it all worked in.” 3M [other household members] “I would hate to be … and not be able to use meds every day because of the cost. There’s several times I thought, “Well geez, I’m gonna go every other day.” And then I thought, and she [my wife] says, “No, you’re not.” 12M [cost concerns] |
| Patient work | “As we get older, we get confused about our meds and especially if you have two that look very similar to each other. I know to look on them and there’s different numbers on there, then I also know that if I Google the number, I can find out what the med is.” 5W [verification] |
| Collaborative work | “I’ll tell you what. This [number of medications] is ridiculous… He’s really tried to get me off a couple of them for me.” 12M [taking too many medicines] “I feel like I get support from my pharmacy on managing my meds and from my docs too. I think we’ve got a good exchange going. Establishing a relationship with the patients. They’re not afraid to ask questions or feel like taking their time. I think that just human interaction really lays a basis for the information flow.” 3M [personable communication] |
| Theme: “There is method to this madness” | “I always put my morning ones over here. I fill them in the evening … This’ll be for … I took my morning ones, this is for after supper. Then, I’ll refill before my nighttime. This’ll be for my nighttime. They’re all in different containers, so I know I’m getting the right thing. I take an anti-biotic, first thing in the morning. The way I remind myself is I leave the glass on the counter that we use for our last meds of the day, so the glass is still there when I get up in the morning. Its still sitting there and it reminds me to take my anti-biotic. There’s method to this madness.” 3M “Here is a new one. Gabapentin. This says, “Take one tablet my mouth three times a day.” So, okay. That to me means morning, noon, and night. But I don’t take any afternoon pills because I forget them all the time. So I take two in the morning and one at night.” 7M “I get up [in the morning], I’ll have my coffee and then I’ll decide to eat something and then at that time I try to take the pills at the same time. Where I get off is like I said, if he [my husband] pours my cup of coffee and I don’t go to the cupboard to get the cup then I don’t get triggered sometimes.” 5W |
| Theme: Maintaining control | “She [my physician] told me when she gave them [the sleeping pills] to me that I could take two, and I don’t allow myself to do that. I can get up on five hours of sleep and/or six and do a day. It doesn’t matter, so I’m not going to let these guys have too much control of my life, but they do help.” 6W |
| Theme: Avoiding vulnerability | “it [taking too many meds] makes me feel like I’m a sick person. Medically, I’m pretty sick. I used to be on, like, 15 prescriptions so Dr. [mentioned doctor’s name] got me off a couple of them and he’s tried the [brand medication] and that did not work. I had to get right back on it again. I know I can’t be without it.” 12M |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fadare, O.; Witry, M. “There Is Method to This Madness” A Qualitative Investigation of Home Medication Management by Older Adults. Pharmacy 2023, 11, 42. https://doi.org/10.3390/pharmacy11020042
Fadare O, Witry M. “There Is Method to This Madness” A Qualitative Investigation of Home Medication Management by Older Adults. Pharmacy. 2023; 11(2):42. https://doi.org/10.3390/pharmacy11020042
Chicago/Turabian StyleFadare, Olajide, and Matthew Witry. 2023. "“There Is Method to This Madness” A Qualitative Investigation of Home Medication Management by Older Adults" Pharmacy 11, no. 2: 42. https://doi.org/10.3390/pharmacy11020042
APA StyleFadare, O., & Witry, M. (2023). “There Is Method to This Madness” A Qualitative Investigation of Home Medication Management by Older Adults. Pharmacy, 11(2), 42. https://doi.org/10.3390/pharmacy11020042