
Public Health Interventions Delivered by Pharmacy Professionals in Low- and Middle-Income Countries in Africa: A Systematic Scoping Review

Abstract
1. Introduction
2. Methods
2.1. Search Strategy and Information Sources
2.2. Electronic Search
2.3. Hand-Searching of Key Journals, Theses and Dissertations, and Relevant Organizations
2.4. Data Extraction
2.5. Data Charting
- the country setting (e.g., LMICs in Africa),
- the setting type (e.g., community pharmacy, hospital pharmacy, health center, hospital),
- the intervention type (e.g., advice, testing, monitoring),
- the health condition (e.g., diabetes, hypertension, Asthma, malaria),
- The aims of the study and the aims of the intervention,
- The type of study design (e.g., randomized controlled trial (RCT), quasi-experimental, single-arm before and after intervention, quantitative cross-sectional survey, qualitative study, mixed-method design,
- Outcomes and processes assessed,
- The sample size,
- Characteristics of the sample (e.g., gender, age, health status),
- Resource investment (e.g., training),
- Mode of delivery,
- The number of required interactions to deliver the intervention,
2.6. Collating, Summarizing, and Reporting the Findings
- Level A: Evidence from meta-analysis or systematic reviews of randomized controlled trials.
- Level B: Evidence from randomized controlled trials.
- Level C: Evidence from quasi-experimental or intervention studies
- Level D: Evidence from observational studies or quantitative surveys or well-designed qualitative studies
- Level E: Expert opinion, case reports.
3. Results
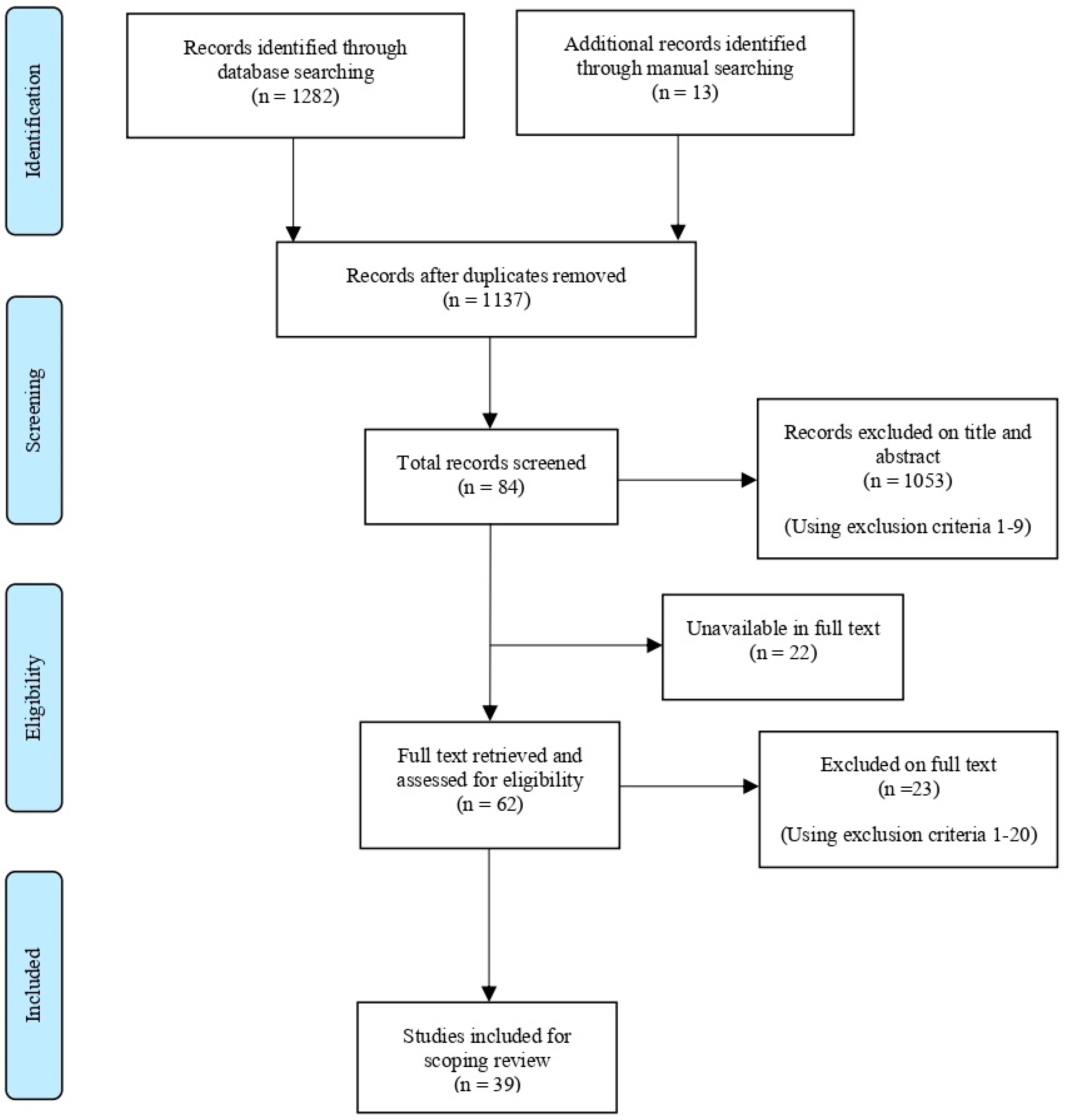
3.1. Study Selection
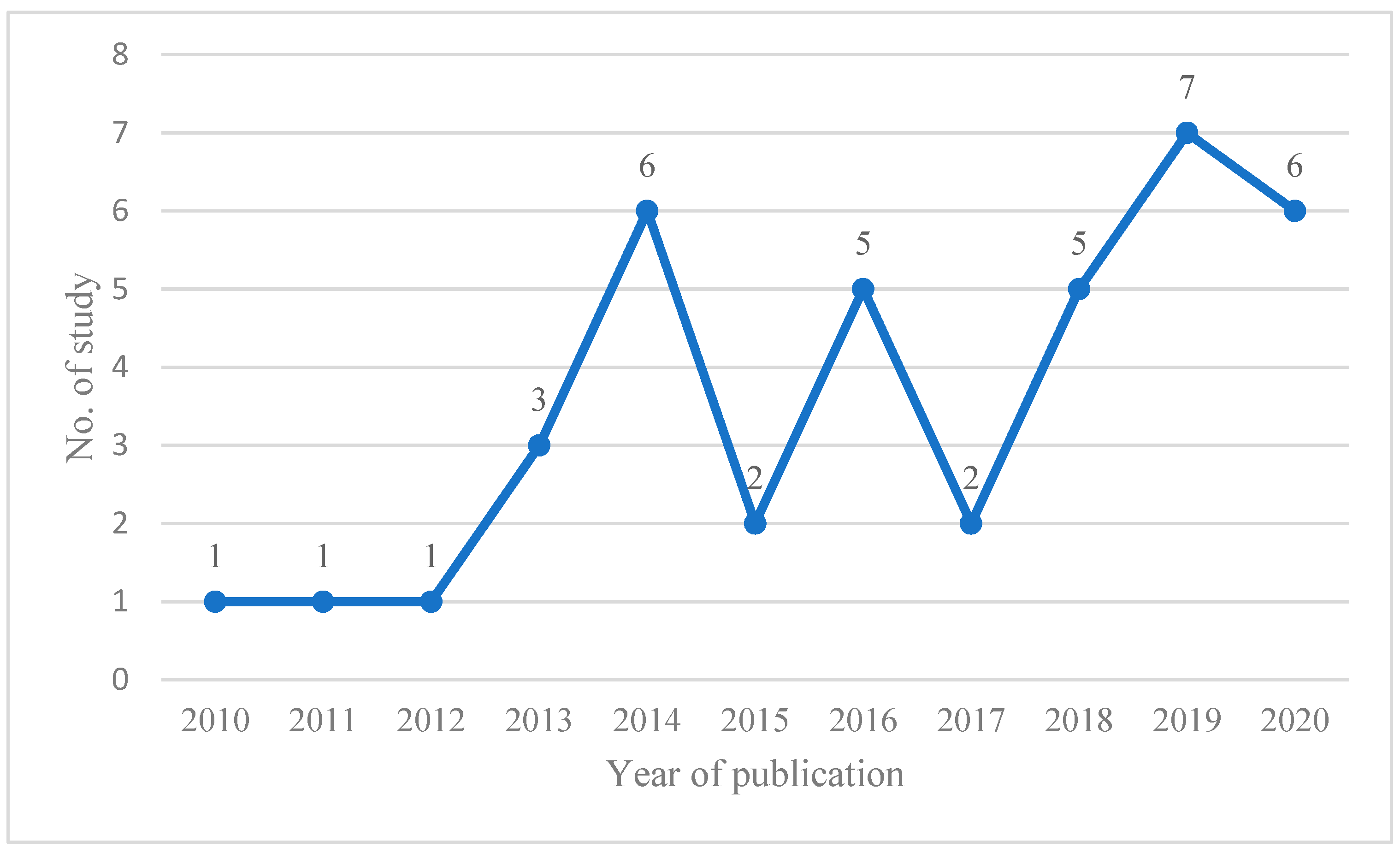
3.2. Study Characteristics
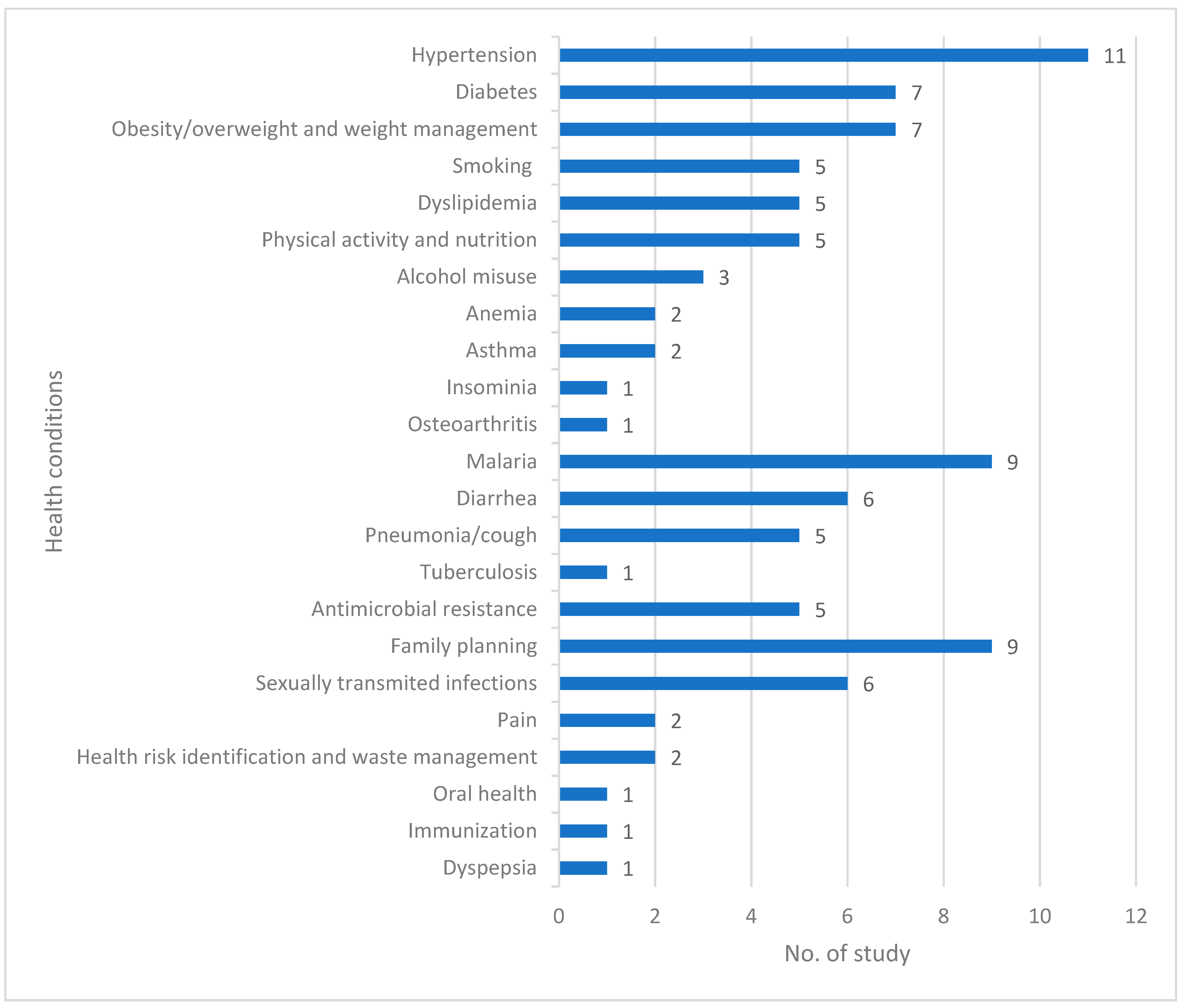
3.3. Scope of Public Health Interventions and Quality of Evidence
- Non-communicable diseases (NCDs) (n = 15),
- Infectious diseases (n = 12),
- Antimicrobial resistance (n = 5),
- Sexual and reproductive health (n = 11),
- Other health conditions (n = 5)
3.3.1. Noncommunicable Diseases (NCDs)
3.3.2. Infectious Disease
3.3.3. Antimicrobial Resistance
3.3.4. Sexual and Reproductive Health
3.3.5. Other Health Conditions
3.4. The Strength and Level of Evidence
4. Discussion
4.1. Strengths and Limitations of this Scoping Review
4.2. Implication
- Randomized and interventional studies that compare the effectiveness of the delivery public health services by pharmacy professionals.
- Studies exploring the experiences and challenges faced by pharmacy professionals in providing public health services and identifying strategies to overcome these barriers.
- Studies investigating the impact of policy and regulatory changes on the delivery of public health services by pharmacy professionals in LMICs.
- Studies evaluating the effectiveness of interprofessional collaboration between pharmacists and other health professionals in delivering public health services in LMICs.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Kaseje, D.; Juma, P.; Oindo, M. Public health in Africa: What is new—The context, the gains, the losses, the renewed public health, and the way forward. J. Kidney Int. 2005, 68, S49–S59. [Google Scholar] [CrossRef] [PubMed]
- Nkengasong, J.N.; Tessema, S.K. Africa Needs a New Public Health Order to Tackle Infectious Disease Threats. Cell 2020, 183, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Agyei-Mensah, S.; de-Graft Aikins, A. Epidemiological transition and the double burden of disease in Accra, Ghana. J. Urban Health 2010, 87, 879–897. [Google Scholar] [CrossRef]
- Peer, N. The converging burdens of infectious and non-communicable diseases in rural-to-urban migrant Sub-Saharan African populations: A focus on HIV/AIDS, tuberculosis and cardio-metabolic diseases. Trop. Dis. Travel Med. Vaccines 2015, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- De-Graft Aikins, A.; Unwin, N.; Agyemang, C.; Allotey, P.; Campbell, C.; Arhinful, D. Tackling Africa’s chronic disease burden: From the local to the global. Glob. Health 2010, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Magadi, M.A. The disproportionate high risk of HIV infection among the urban poor in sub-Saharan Africa. AIDS Behav. 2013, 17, 1645–1654. [Google Scholar] [CrossRef]
- Royal Pharmaceutical Society. Professional Standards for Public Health Practice for Pharmacy. 2014. Available online: https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Professional%20standards/Professional%20standards%20for%20public%20health/public-health-standards---appendix-1.pdf (accessed on 5 February 2021).
- World Health Organization. The State of the Health Workforce in the WHO African Region; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Faculty of Public Health. Short Headline Definition of Healthcare Public Health. 2017. Available online: https://www.fph.org.uk/media/1879/hcph-definition-final.pdf (accessed on 16 February 2021).
- International Pharmaceutical Federation (FIP). FIP Statement of Policy the Role of the Pharmacist in the Prevention and Treatment of Chronic Disease, Approved by FIP Council, Brazil. 2006. Available online: https://www.fip.org/file/4338 (accessed on 24 February 2021).
- International Pharmaceutical Federation (FIP). Beating Non-Communicable Diseases in the Community: The Contribution of Pharmacists. 2019. Available online: https://www.fip.org/files/content/publications/2019/beating-ncds-in-the-community-the-contribution-of-pharmacists.pdf (accessed on 24 February 2021).
- Emmerton, L.M.; Smith, L.; Lemay, K.S.; Krass, I.; Saini, B.; Bosnic-Anticevich, S.Z.; Reddel, H.K.; Burton, D.L.; Stewart, K.; Armour, C.L. Experiences of community pharmacists involved in the delivery of a specialist asthma service in Australia. BMC Health Serv. Res. 2012, 12, 164. [Google Scholar] [CrossRef]
- Periasamy, U.; Sidik, S.M.; Rampal, L.; Fadhilah, S.I.; Akhtari-Zavare, M.; Mahmud, R. Effect of chemotherapy counseling by pharmacists on quality of life and psychological outcomes of oncology patients in Malaysia: A randomized control trial. Health Qual. Life Outcomes 2017, 15, 104. [Google Scholar] [CrossRef]
- Wiedenmayer, K.; Summers, R.S.; Mackie, C.A.; Gous, A.G.; Everard, M.; Tromp, D.; World Health Organization. Developing Pharmacy Practice: A Focus on Patient Care—Handbook; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Kruk, M.E.; Myers, M.; Varpilah, S.T.; Dahn, B.T. What is a resilient health system? Lessons from Ebola. Lancet 2015, 385, 1910–1912. [Google Scholar] [CrossRef]
- Azhar, S.; Hassali, M.A.; Ibrahim, M.I.M.; Ahmad, M.; Masood, I.; Shafie, A.A. The role of pharmacists in developing countries: The current scenario in Pakistan. Hum. Resour. Health 2009, 7, 54. [Google Scholar] [CrossRef]
- Smith, F. Community pharmacy in Ghana: Enhancing the contribution to primary health care. J. Health Policy Plan. 2004, 19, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Erku, D.A.; Mersha, A.G. Involvement of community pharmacists in public health priorities: A multi-center descriptive survey in Ethiopia. PLoS ONE 2017, 12, e0180943. [Google Scholar] [CrossRef] [PubMed]
- Amadi, C.E.; Lawal, F.O.; Mbakwem, A.C.; Ajuluchukwu, J.N.; Oke, D.A. Knowledge of cardiovascular disease risk factors and practice of primary prevention of cardiovascular disease by Community Pharmacists in Nigeria: A cross-sectional study. Int. J. Clin. Pharm. 2018, 40, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Marfo, A.F.; Owusu-Daaku, F.T. Evaluation of a pharmacist-led hypertension preventative and detection service in the Ghanaian community pharmacy: An exploratory study. Int. J. Pharm. Pract. 2016, 24, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.S.-E.; Mahmoud, A.A.; Ali, A.A. Involvement of Sudanese community pharmacists in public health activities. Int. J. Clin. Pharm. 2013, 35, 393–400. [Google Scholar] [CrossRef]
- Akol, A.; Chin-Quee, D.; Wamala-Mucheri, P.; Namwebya, J.H.; Mercer, S.J.; Stanback, J. Getting closer to people: Family planning provision by drug shops in Uganda. Glob. Health Sci. Pract. 2014, 2, 472–481. [Google Scholar] [CrossRef]
- Liambila, W.; Obare, F.; Keesbury, J. Can private pharmacy providers offer comprehensive reproductive health services to users of emergency contraceptives? Evidence from Nairobi, Kenya. Patient Educ. Couns. 2010, 81, 368–373. [Google Scholar] [CrossRef]
- Mugo, P.M.; Duncan, S.; Mwaniki, S.; Thiong’O, A.N.; Gichuru, E.; Okuku, H.S.; Van Der Elst, E.M.; Smith, A.D.; Graham, S.; Sanders, E.J. Cross-sectional survey of treatment practices for urethritis at pharmacies, private clinics and government health facilities in coastal Kenya: Many missed opportunities for HIV prevention. Sex. Transm. Infect. 2013, 89, 583–589. [Google Scholar] [CrossRef]
- Awor, P.; Wamani, H.; Tylleskar, T.; Jagoe, G.; Peterson, S. Increased Access to Care and Appropriateness of Treatment at Private Sector Drug Shops with Integrated Management of Malaria, Pneumonia and Diarrhoea: A Quasi-Experimental Study in Uganda. PLoS ONE 2014, 9, e115440. [Google Scholar] [CrossRef]
- Mengistu, G.; Gietnet, K.; Amare, F.; Sisay, M.; Hagos, B.; Misganaw, D. Self-Reported and Actual Involvement of Community Pharmacy Professionals in the Management of Childhood Diarrhea: A Cross-Sectional and Simulated Patient Study at two Towns of Eastern Ethiopia. Clin. Med. Insights Pediatr. 2019, 13, 1–6. [Google Scholar] [CrossRef]
- Rutta, E.; Tarimo, A.; Delmotte, E.; James, I.; Mwakisu, S.; Kasembe, D.; Konduri, N.; Silumbe, R.; Kakanda, K.; Valimba, R. Understanding private retail drug outlet dispenser knowledge and practices in tuberculosis care in Tanzania. Int. J. Tuberc. Lung Dis. 2014, 18, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Rampamba, E.M.; Meyer, J.C.; Helberg, E.A.; Godman, B. Empowering hypertensive patients in south africa to improve their disease management: A pharmacist-led intervention. J. Res. Pharm. Pract. 2019, 8, 208–213. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Update from the Seventy-Fourth World Health Assembly. 2021. Available online: https://www.who.int/news/item/27-05-2021-update-from-the-seventy-fourth-world-health-assembly-27-may-2021 (accessed on 16 February 2021).
- World Health Organization (WHO). Strengthening the Inclusion of Reproductive, Maternal, Newborn and Child (RMNCH) Health in Concept Notes to the Global Fund; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- International Pharmaceutical Federation (FIP). FIP Reference Paper on the Effective Utilization of Pharmacists in Improving Maternal, Newborn and Child Health (MNCH). 2011. Available online: https://www.fip.org/file/1416 (accessed on 16 February 2021).
- Jackson, J.K.; Sweidan, M.; Spinks, J.M.; Snell, B.; Duncan, G.J. Public Health-Recognising the Role of Australian Pharmacists. J. Pharm. Pract. Res. 2004, 34, 290–292. [Google Scholar] [CrossRef]
- Costa, S.; Santos, C.; Silveira, J. Community Pharmacy Services in Portugal. Ann. Pharmacother. 2006, 40, 2228–2234. [Google Scholar] [CrossRef]
- Anderson, S. Community pharmacy and public health in Great Britain, 1936 to 2006: How a phoenix rose from the ashes. J. Epidemiol. Community Health 2007, 61, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: 2014 Edition; The Joanna Briggs Institute: Adelaide, Australia, 2014. [Google Scholar]
- Ayele, A.A.; Islam, M.S.; Cosh, S.; East, L. Involvement and practice of community pharmacists in maternal and child health services: A systematic review. Res. Soc. Adm. Pharm. 2021, 17, 643–652. [Google Scholar] [CrossRef]
- Stokes, G.; Rees, R.; Khatwa, M.; Stansfield, C.; Burchett, H.; Dickson, K.; Brunton, G.; Thomas, J. Public Health Service Provision by Community Pharmacies: A Systematic Map of Evidence; Department of Health Reviews Facility: London, UK, 2019. [Google Scholar]
- Agomo, C.O. The role of community pharmacists in public health: A scoping review of the literature. J. Pharm. Health Serv. Res. 2011, 3, 25–33. [Google Scholar] [CrossRef]
- Anderson, C.; Blenkinsopp, A.; Armstrong, M. Feedback from community pharmacy users on the contribution of community pharmacy to improving the public’s health: A systematic review of the peer reviewed and non-peer reviewed literature 1990–2002. Health Expect. 2004, 7, 191–202. [Google Scholar] [CrossRef]
- Rychetnik, L.; Frommer, M.; Hawe, P.; Shiell, A. Criteria for evaluating evidence on public health interventions. J. Epidemiol. Community Health 2002, 56, 119–127. [Google Scholar] [CrossRef]
- World Bank. World Bank Global Index LMIC List 2020. Available online: https://data.worldbank.org/income-level/low-and-middle-income (accessed on 22 February 2021).
- Bello, S.I.; Bello, I.K. Impacts of Community Pharmacists on Self-medication Management among Rural Dwellers, Kwara State Central, Nigeria. Dhaka Univ. J. Pharm. Sci. 2013, 12, 1–9. [Google Scholar] [CrossRef]
- Amadi, C.; Lawal, F.; Ajiboye, W.; Agbim, R.; Mbakwem, A.; Ajuluchukwu, J.; Oke, D.A. Opportunistic screening of cardiovascular disease risk factors in community pharmacies in Nigeria: A cross-sectional study. Int. J. Clin. Pharm. 2020, 42, 1469–1479. [Google Scholar] [CrossRef] [PubMed]
- Nelissen, H.E.; Cremers, A.L.; Okwor, T.J.; Kool, S.; van Leth, F.; Brewster, L.; Makinde, O.; Gerrets, R.; Hendriks, M.E.; Schultsz, C.; et al. Pharmacy-based hypertension care employing mHealth in Lagos, Nigeria—A mixed methods feasibility study. BMC Health Serv. Res. 2018, 18, 934. [Google Scholar] [CrossRef] [PubMed]
- Adje, D.U.; Williams, F.E.; Oparah, A.C. Outcome of cardiovascular risk assessment among rural community dwellers in ezionum, Nigeria-implications for public health. Afr. Health Sci. 2019, 19, 2112–2120. [Google Scholar] [CrossRef]
- Michael, D.; Kezakubi, D.; Juma, A.; Todd, J.; Reyburn, H.; Renju, J. The feasibility and acceptability of screening for hypertension in private drug retail outlets: A pilot study in Mwanza region, Tanzania. Int. Health 2016, 8, 360–366. [Google Scholar] [CrossRef]
- Tesfaye, Z.T.; Yismaw, M.B. Community’s extent of use and approval of extended pharmacy services in community pharmacies in Southwest Ethiopia. PLoS ONE 2020, 15, e0230863. [Google Scholar] [CrossRef]
- Belachew, S.A.; Muluneh, N.Y.; Erku, D.A.; Netere, A.K. A cross sectional study on beliefs and roles of community pharmacy professionals in preventing and managing metabolic syndrome in an Ethiopian setting. PLoS ONE 2020, 15, e0244211. [Google Scholar] [CrossRef]
- Teka, N.T.; Baye, A.M. Counseling practice of community pharmacists for diabetes mellitus patients in Addis Ababa, Ethiopia. BMC Res. Notes 2018, 11, 700. [Google Scholar] [CrossRef]
- Adje, D.; Umar, M.; Gadanya, M.; Rufai, R. Impact of pharmacists’health educational intervention on anemia in pregnancy in rural settings in Kano, Nigeria. Int. J. Pharm. Sci. Res. 2020, 11, 2403–2410. [Google Scholar]
- Amorha, K.C.; Okonta, M.J.; Ukwe, C.V. Impact of pharmacist-led educational interventions on asthma control and adherence: Single-blind, randomised clinical trial. Int. J. Clin. Pharm. 2020, 43, 689–697. [Google Scholar] [CrossRef]
- Patrick, O.K.; Joshua, A.K.; Oluwafunmi, A. Evaluation of community pharmacists’ involvement in the treatment of malaria in Nigeria. Int. J. Pharm. Pharm. Sci. 2011, 3, 107–112. [Google Scholar]
- Maloney, K.; Ward, A.; Krenz, B.; Petty, N.; Bryson, L.; Dolkart, C.; Visser, T.; Le Menach, A.; Scott, V.K.; Cohen, J.M.; et al. Expanding access to parasite-based malaria diagnosis through retail drug shops in Tanzania: Evidence from a randomized trial and implications for treatment. Malar. J. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Kitutu, F.E.; Kalyango, J.N.; Mayora, C.; Selling, K.E.; Peterson, S.; Wamani, H. Integrated community case management by drug sellers influences appropriate treatment of paediatric febrile illness in South Western Uganda: A quasi-experimental study. Malar. J. 2017, 16, 425. [Google Scholar] [CrossRef] [PubMed]
- Kahabuka, C.; Kvåle, G.; Hinderaker, S.G. Care-Seeking and Management of Common Childhood Illnesses in Tanzania—Results from the 2010 Demographic and Health Survey. PLoS ONE 2013, 8, e58789. [Google Scholar] [CrossRef]
- Poyer, S.; Musuva, A.; Njoki, N.; Okara, R.; Cutherell, A.; Sievers, D.; Lussiana, C.; Memusi, D.; Kiptui, R.; Ejersa, W.; et al. Fever case management at private health facilities and private pharmacies on the Kenyan coast: Analysis of data from two rounds of client exit interviews and mystery client visits. Malar. J. 2018, 17, 112. [Google Scholar] [CrossRef] [PubMed]
- Ansah, E.K.; Narh-Bana, S.A.; Bonful, H.A.; Bart-Plange, C.; Cundill, B.; Gyapong, M.; Whitty, C. The impact of providing rapid diagnostic malaria tests on fever management in the private retail sector in Ghana: A cluster randomized trial. BMJ 2015, 350, h1019. [Google Scholar] [CrossRef] [PubMed]
- Kwarteng, A.; Malm, K.L.; Febir, L.G.; Tawiah, T.; Adjei, G.; Nyame, S.; Agbokey, F.; Twumasi, M.; Amenga-Etego, S.; Danquah, D.A.; et al. The Accuracy and Perception of Test-Based Management of Malaria at Private Licensed Chemical Shops in the Middle Belt of Ghana. Am. J. Trop. Med. Hyg. 2019, 100, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.S.; Mahmoud, A.A.; Ali, A.A. The role of Sudanese community pharmacists in patients’ self-care. Int. J. Clin. Pharm. 2014, 36, 412–419. [Google Scholar] [CrossRef]
- Ayele, A.A.; Mekuria, A.B.; Tegegn, H.G.; Gebresillassie, B.M.; Mekonnen, A.B.; Erku, D.A. Management of minor ailments in a community pharmacy setting: Findings from simulated visits and qualitative study in Gondar town, Ethiopia. PLoS ONE 2018, 13, e0190583. [Google Scholar] [CrossRef]
- Brink, A.J.; Messina, A.P.; Feldman, C.; Richards, G.A.; Becker, P.J.; Goff, D.A.; Bauer, K.A.; Nathwani, D.; van den Bergh, D.; on behalf of theNetcare Antimicrobial Stewardship Study Alliance. Antimicrobial stewardship across 47 South African hospitals: An implementation study. Lancet Infect. Dis. 2016, 16, 1017–1025. [Google Scholar] [CrossRef]
- Messina, A.P.; van den Bergh, D.; Goff, D.A. Antimicrobial Stewardship with Pharmacist Intervention Improves Timeliness of Antimicrobials Across Thirty-three Hospitals in South Africa. Infect. Dis. Ther. 2015, 4, 5–14. [Google Scholar] [CrossRef]
- Brink, A.J.; Messina, A.P.; Feldman, C.; Richards, G.A.; van den Bergh, D.; on behalf of the Netcare Antimicrobial Stewardship Study Alliance. From guidelines to practice: A pharmacist-driven prospective audit and feedback improvement model for peri-operative antibiotic prophylaxis in 34 South African hospitals. J. Antimicrob. Chemother. 2017, 72, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, U.; Sulaiman, S.A.S.; Adesiyun, A.G. Impact of pharmacist-led antibiotic stewardship interventions on compliance with surgical antibiotic prophylaxis in obstetric and gynecologic surgeries in Nigeria. PLoS ONE 2019, 14, e0213395. [Google Scholar] [CrossRef]
- Gonsalves, L.; Wyss, K.; Gichangi, P.; Hilber, A.M. Pharmacists as youth-friendly service providers: Documenting condom and emergency contraception dispensing in Kenya. Int. J. Public Health 2020, 65, 487–496. [Google Scholar] [CrossRef]
- Corroon, M.; Kebede, E.; Spektor, G.; Speizer, I. Key Role of Drug Shops and Pharmacies for Family Planning in Urban Nigeria and Kenya. Glob. Health Sci. Pract. 2016, 4, 594–609. [Google Scholar] [CrossRef] [PubMed]
- Lebetkin, E.; Orr, T.; Dzasi, K.; Keyes, E.; Shelus, V.; Mensah, S.; Nagai, H.; Stanback, J. Injectable Contraceptive Sales at Licensed Chemical Seller Shops in Ghana: Access and Reported Use in Rural and Periurban Communities. Int. Perspect. Sex. Reprod. Health 2014, 40, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Gonsalves, L.; Wyss, K.; Gichangi, P.; Say, L.; Hilber, A.M. Regulating pharmacists as contraception providers: A qualitative study from Coastal Kenya on injectable contraception provision to youth. PLoS ONE 2019, 14, e0226133. [Google Scholar] [CrossRef]
- Mugo, P.M.; Prins, H.A.B.; Wahome, E.W.; Mwashigadi, G.M.; Thiong’O, A.N.; Gichuru, E.; Omar, A.; Graham, S.M.; Sanders, E.J. Engaging young adult clients of community pharmacies for HIV screening in Coastal Kenya: A cross-sectional study. Sex. Transm. Infect. 2014, 91, 257–259. [Google Scholar] [CrossRef]
- Brown, D.; Portlock, J.; Rutter, P. Review of services provided by pharmacies that promote healthy living. Int. J. Clin. Pharm. 2012, 34, 399–409. [Google Scholar] [CrossRef]
- International Pharmaceutical Federation (FIP). Establishing Tobacco-Free Communities: A Practical Guide for Pharmacists; International Pharmaceutical Federation: The Hague, The Netherlands, 2015; Available online: https://www.fip.org/files/fip/publications/2015-12-Establishing-tobacco-free-communities.pdf (accessed on 24 February 2021).
- Taylor, J.; Krska, J.; Mackridge, A. A community pharmacy-based cardiovascular screening service: Views of service users and the public. Int. J. Pharm. Pract. 2012, 20, 277–284. [Google Scholar] [CrossRef]
- Saramunee, K.; Krska, J.; Mackridge, A.; Richards, J.; Suttajit, S.; Phillips-Howard, P.A. How to enhance public health service utilization in community pharmacy?: General public and health providers’ perspectives. Res. Soc. Adm. Pharm. 2014, 10, 272–284. [Google Scholar] [CrossRef] [PubMed]
- White, L.; Klinner, C.; Carter, S. Consumer perspectives of the Australian Home Medicines Review Program: Benefits and barriers. Res. Soc. Adm. Pharm. 2012, 8, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Walker, R. Pharmaceutical public health: The end of pharmaceutical care. Pharm. J. 2000, 264, 340–341. [Google Scholar]
- World Health Organization (WHO). Noncommunicable Diseases 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 28 May 2021).
- World Health Organization (WHO). Communicable Diseases 2021. Available online: https://www.afro.who.int/health-topics/communicable-diseases#:~:text=Communicable%2C%20or%20infectious%20diseases%2C%20are%20caused%20by%20microorganisms,are%20caused%20by%20ingesting%20contaminated%20food%20or%20water (accessed on 28 May 2021).
- World Health Organization (WHO). Sexual and Reproductive Health Fact Sheet 2017. Available online: https://www.afro.who.int/publications/sexual-and-reproductive-health-fact-sheet (accessed on 13 March 2021).
- World Health Organization (WHO). Antimicrobial Resistance 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 24 June 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Themes | Included Studies and Aims of Interventions | Study Settings (n) | Intervention Component, Mode of Delivery and Training (n) | Study Designs (n) | Number of Settings |
|---|---|---|---|---|---|
| NCDs | 15 studies identified Interventions: Cardiovascular risk factors including diabetes, hypertension, obesity | Nigeria (7) Ethiopia (4) Ghana, South Africa, Sudan and Tanzania (1 each) Community pharmacies (12), and health centers or hospitals (3) | Risk identification and reduction screening for cardiovascular risk factors (7) Disease management: interventions included counselling or advice, education, medication management (8) In person service delivery (15) Use of mobile health technology (1) Staff training on service delivery (7) Length of training reported in 3 studies and were one or two days | Cross-sectional study design to gather and analyze data on service provision (10) Single-blind randomized controlled trial (1) Quasi-experimental design (1) Single group before and after intervention studies (3) | More than one setting or multi-center (11) More than 100 individuals (6) |
| Infectious Diseases | 12 studies identified: Malaria (8) Diarrheal disease (6) Pneumonia (5) Tuberculosis (1) | Tanzania (3) Ghana (2) Ethiopia (2) Uganda (2) Nigeria, Kenya and Sudan (1 each) Community pharmacies or accredited drug dispensing outlets or drug shops or licensed chemical shops or drug stores/vendors | Interventions focused on testing and treatment of conditions Additional interventions: referral to others, counselling and education In person service delivery (12) Staff training on service delivery (6) Length of training reported in 5 studies, and were 3 days (2), 5 days (2) and 1 week (1) | Cross-sectional study design (8) Mixed-method design including survey and qualitative interview (1) Quasi-experimental design (2) Cluster-randomized trial (1) Randomized interventional study (1) | More than one setting or multi-center (12) Data collected from 100 or more participants (7) |
| Sexual and reproductive health | 11 studies were identified: sexually transmitted infections (STIs) (5), and reproductive health (6) | Kenya (5) Ethiopia (2) Uganda, Ghana, and Sudan (1 each), and Nigeria and Kenya (1) Community pharmacies or licensed chemical seller or drug shops | Interventions focused on screening and treatment of STIs, and family planning Additional interventions: referral to others, counselling and education In person service delivery (11) Staff training on service delivery (7) Length of training reported in one study, and was 6 weeks | Cross-sectional study design (10) Quantitative (8) Qualitative design involving FGDs, in-depth interviews, KIIs (2) Controlled interventional design (1) | More than one setting or multi-center (11) Data collected from 100 or more participants (4) |
| Antimicrobial resistance | 5 studies were identified aimed at evaluating antibiotic stewardship interventions | South Africa (3) Ethiopia (1) Nigeria (1) Community pharmacies (1) Hospital (4) | Interventions: reviewing and auditing antimicrobial therapy, protocol development, feedback, and in-service education In person service delivery (5) Additional written protocol and mobile phone messages (2) Staff training on service delivery (2) | Cross-sectional (1) Single group before and after intervention (4) | More than one setting or multi-center (5) Data collected from 100 or more participants (4) |
| Other health conditions | 5 studies focused on back pain, dyspepsia, immunization, oral health, unused medicine or waste, minor ailment, and community health risk identification | Ethiopia (3) Nigeria (1) Sudan (1) community pharmacies | Vaccine distribution, providing information, conducting need assessments, counselling, diagnosing and treating conditions, and referral to physician In person service delivery (5) | cross-sectional design (5) | More than one setting or multi-center (4) Data collected from 100 or more participants (1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gebresillassie, B.M.; Howells, K.; Ashiru-Oredope, D. Public Health Interventions Delivered by Pharmacy Professionals in Low- and Middle-Income Countries in Africa: A Systematic Scoping Review. Pharmacy 2023, 11, 24. https://doi.org/10.3390/pharmacy11010024
Gebresillassie BM, Howells K, Ashiru-Oredope D. Public Health Interventions Delivered by Pharmacy Professionals in Low- and Middle-Income Countries in Africa: A Systematic Scoping Review. Pharmacy. 2023; 11(1):24. https://doi.org/10.3390/pharmacy11010024
Chicago/Turabian StyleGebresillassie, Begashaw Melaku, Kelly Howells, and Diane Ashiru-Oredope. 2023. "Public Health Interventions Delivered by Pharmacy Professionals in Low- and Middle-Income Countries in Africa: A Systematic Scoping Review" Pharmacy 11, no. 1: 24. https://doi.org/10.3390/pharmacy11010024
APA StyleGebresillassie, B. M., Howells, K., & Ashiru-Oredope, D. (2023). Public Health Interventions Delivered by Pharmacy Professionals in Low- and Middle-Income Countries in Africa: A Systematic Scoping Review. Pharmacy, 11(1), 24. https://doi.org/10.3390/pharmacy11010024