
A Guide to a Pharmacist-Led Pharmacogenetic Testing and Counselling Service in an Interprofessional Healthcare Setting

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Service Design
2.2. Service Refinement
3. Results
3.1. Service Description
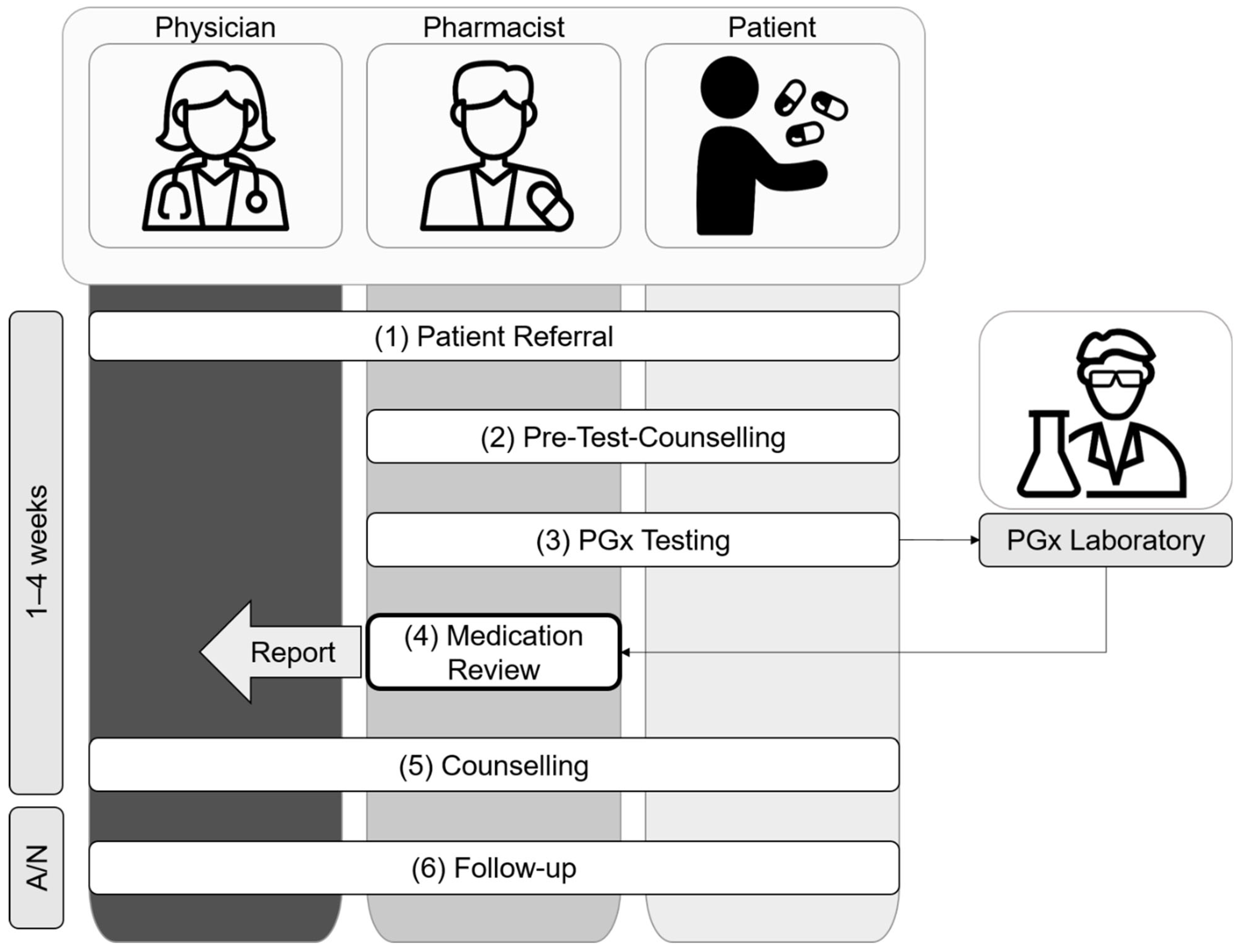
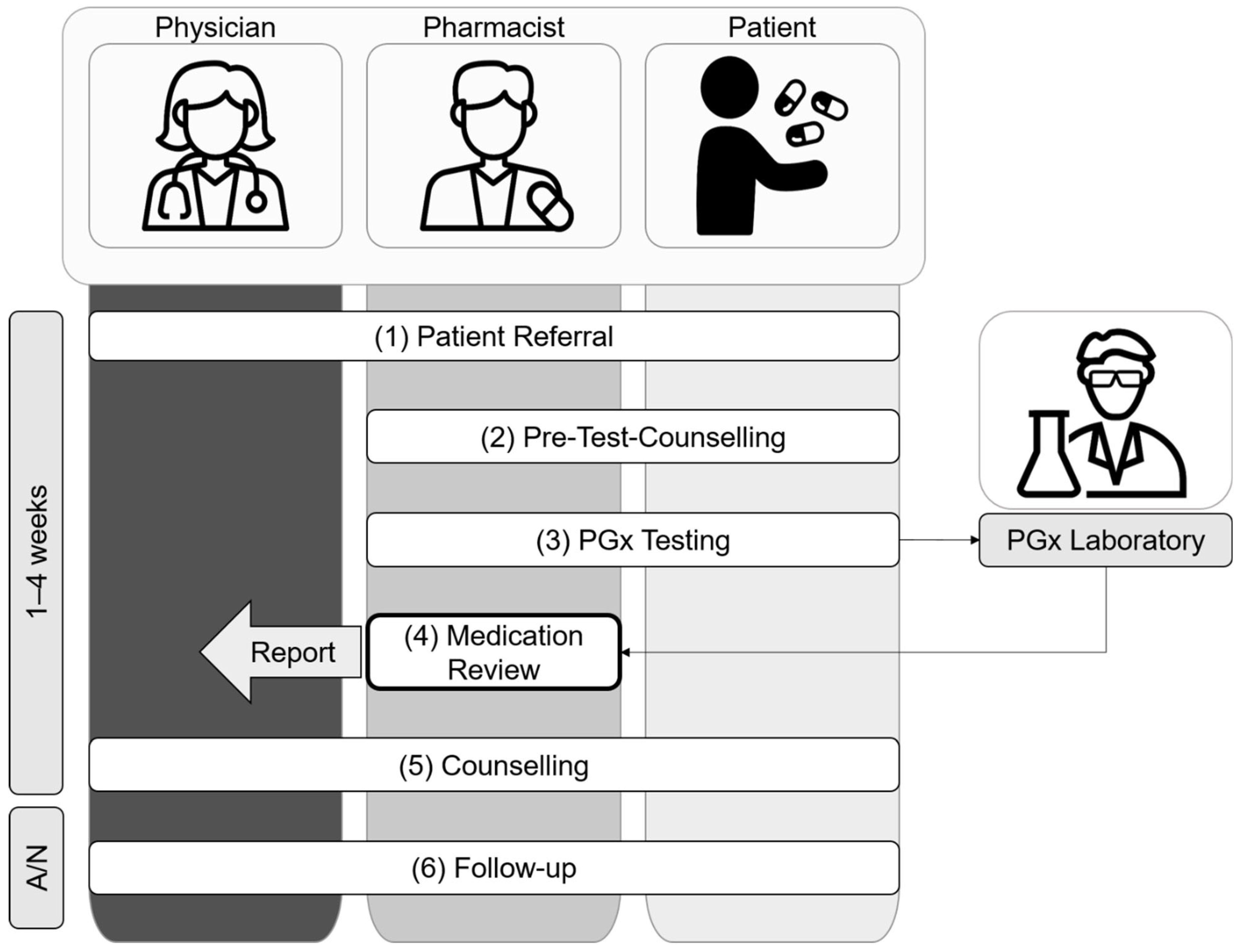
- 1.
- Patient Referral
- 2.
- Pre-Test CounsellingAfter referral to the pharmacist-led PGx service, the pharmacist and the patient meet face-to-face at the community/hospital pharmacy or at the hospital ward for a pre-test counselling visit to decide whether to proceed with PGx testing, following these steps:
- 2.1
- The pharmacist informs the patient about the goals, potential significance, and limits of PGx testing. In addition, the pharmacist answers any questions that the patient may have about PGx testing;
- 2.2
- The pharmacist performs a medication reconciliation and preliminary medication review of type 2a [11], using the Swiss polymedication check form [28] as an interview guide to (i) assess the patient’s current medication regimen; (ii) clarify the patient’s medication history, including experienced ADR and TF; (iii) identify any non-genetic drug related problems (e.g., drug–drug interaction, smoking, nutrition, renal and liver function, medication adherence, allergies). The pharmacist then clarifies any remaining ambiguities with family members or institutions providing care (e.g., home care, dispensing pharmacy, prescribing physician), provided that the patient agrees to do so. If urgent action is required due to identified drug-related problems (e.g., contraindications, need for therapeutic drug monitoring), the pharmacist immediately consults with the treating physician;
- 2.3
- The pharmacist decides whether to proceed with PGx testing based on the information that is available from the patient interview (2.2.). More precisely, there must either be pharmacogenetic recommendations available (e.g., CPIC guidelines) or a rationale from the drug’s metabolism for potential DGIs, for at least one substance or drug class that is indicated as suspicious. Substances are classified as conspicuous, e.g., either due to ADR and/or TF (reactive approach), or when considered for planned treatments (preemptive approach);
- 2.4
- The pharmacist collects the patient’s written informed consent for PGx testing. A copy of the signed informed consent is given to the patient. The pharmacist ensures that any questions the patient may have are answered. If the patient needs more time to decide, the further procedure may be postponed.
- 3.
- PGx Testing
- 4.
- Medication Review
- 5.
- Counselling
- 6.
- Follow-up
3.2. Service Refinement
4. Discussion
5. Conclusions and Outlook
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meyer zu Schwabedissen, H.E. The Role of Pharmacogenomics in Individualized Medicine. In Individualized Medicine–Ethical, Economical and Historical Perspectives; Fischer, T., Langanke, M., Marschall, P., Michl, S., Eds.; Springer: Cham, Switzerland, 2015; Volume 7, pp. 93–112. [Google Scholar]
- Owen, R.P.; Sangkuhl, K.; Klein, T.E.; Altman, R.B. Cytochrome P450 2D6. Pharm. Genom. 2009, 19, 559–562. [Google Scholar] [CrossRef] [Green Version]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Swen, J.J.; Nijenhuis, M.; De Boer, A.; Grandia, L.; Maitland-Van Der Zee, A.H.; Mulder, H.; Rongen, G.A.P.J.M.; Van Schaik, R.H.N.; Schalekamp, T.; Touw, D.J.; et al. Pharmacogenetics: From Bench to Byte—An Update of Guidelines. Clin. Pharmacol. Ther. 2011, 89, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Jeiziner, C.; Suter, K.; Wernli, U.; Barbarino, J.M.; Gong, L.; Whirl-Carrillo, M.; Klein, T.E.; Szucs, T.D.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E. Pharmacogenetic information in Swiss drug labels—A systematic analysis. Pharm. J. 2021, 21, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Bousman, C.A.; Forbes, M.; Jayaram, M.; Eyre, H.; Reynolds, C.F.; Berk, M.; Hopwood, M.; Ng, C. Antidepressant prescribing in the precision medicine era: A prescriber’s primer on pharmacogenetic tools. BMC Psychiatry 2017, 17, 60. [Google Scholar] [CrossRef] [Green Version]
- Zanger, U.M.; Schwab, M. Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Dunbar-Jacob, J.; Erlen, J.A.; Schlenk, E.A.; Ryan, C.M.; Sereika, S.M.; Doswell, W.M. Adherence in chronic disease. Annu. Rev. Nurs. Res. 2000, 18, 48–90. [Google Scholar] [CrossRef]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.-J.; Swen, J.J. Phenoconversion of Cytochrome P450 Metabolism: A Systematic Review. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef]
- Brown, J.T.; Bishop, J.R.; Schneiderhan, M.E. Using pharmacogenomics and therapeutic drug monitoring to guide drug selection and dosing in outpatient mental health comprehensive medication management. Ment. Health Clin. 2020, 10, 254–258. [Google Scholar] [CrossRef]
- Griese-Mammen, N.; Hersberger, K.E.; Messerli, M.; Leikola, S.; Horvat, N.; Van Mil, J.W.F.; Kos, M. PCNE definition of medication review: Reaching agreement. Int. J. Clin. Pharm. 2018, 40, 1199–1208. [Google Scholar] [CrossRef]
- Chenoweth, M.J.; Giacomini, K.M.; Pirmohamed, M.; Hill, S.L.; Schaik, R.H.N.; Schwab, M.; Shuldiner, A.R.; Relling, M.V.; Tyndale, R.F. Global Pharmacogenomics Within Precision Medicine: Challenges and Opportunities. Clin. Pharmacol. Ther. 2020, 107, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Stäuble, C.K.; Lampert, M.L.; Allemann, S.; Hatzinger, M.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E.; Imboden, C.; Mikoteit, T. Pharmacist-guided pre-emptive pharmacogenetic testing in antidepressant therapy (PrePGx): Study protocol for an open-label, randomized controlled trial. Trials 2021, 22, 919. [Google Scholar] [CrossRef] [PubMed]
- Van Der Wouden, C.; Cambon-Thomsen, A.; Cecchin, E.; Cheung, K.; Dávila-Fajardo, C.; Deneer, V.; Dolžan, V.; Ingelman-Sundberg, M.; Jönsson, S.; Karlsson, M.; et al. Implementing Pharmacogenomics in Europe: Design and Implementation Strategy of the Ubiquitous Pharmacogenomics Consortium. Clin. Pharmacol. Ther. 2017, 101, 341–358. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, A.K.; Zai, C.C.; Altar, C.A.; Tanner, J.A.; Davies, P.E.; Traxler, P.; Li, J.; Cogan, E.S.; Kucera, M.T.; Gugila, A.; et al. Clinical utility of combinatorial pharmacogenomic testing in depression: A Canadian patient- and rater-blinded, randomized, controlled trial. Transl. Psychiatry 2022, 12, 101. [Google Scholar] [CrossRef]
- Stäuble, C.K.; Jeiziner, C.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E.; Lampert, M.L. Pharmacogenetics in Pharmaceutical Care—Piloting an Application-Oriented Blended Learning Concept. Pharmacy 2021, 9, 152. [Google Scholar] [CrossRef]
- Crown, N.; Sproule, B.A.; Luke, M.J.; Piquette-Miller, M.; McCarthy, L.M. A Continuing Professional Development Program for Pharmacists Implementing Pharmacogenomics into Practice. Pharmacy 2020, 8, 55. [Google Scholar] [CrossRef] [Green Version]
- Arwood, M.J.; Dietrich, E.A.; Duong, B.Q.; Smith, D.M.; Cook, K.; Elchynski, A.; Rosenberg, E.I.; Huber, K.N.; Nagoshi, Y.L.; Wright, A.; et al. Design and Early Implementation Successes and Challenges of a Pharmacogenetics Consult Clinic. J. Clin. Med. 2020, 9, 2274. [Google Scholar] [CrossRef]
- Lanting, P.; Drenth, E.; Boven, L.; Van Hoek, A.; Hijlkema, A.; Poot, E.; Van Der Vries, G.; Schoevers, R.; Horwitz, E.; Gans, R.; et al. Practical Barriers and Facilitators Experienced by Patients, Pharmacists and Physicians to the Implementation of Pharmacogenomic Screening in Dutch Outpatient Hospital Care—An Explorative Pilot Study. J. Pers. Med. 2020, 10, 293. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Stäuble, C.K.; Lampert, M.L.; Mikoteit, T.; Hatzinger, M.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E. Nonresponse to high-dose bupropion for depression in a patient carrying CYP2B6*6 and CYP2C19*17 variants: A case report. Pharmacogenomics 2020, 21, 1145–1150. [Google Scholar] [CrossRef]
- Jeiziner, C.; Stäuble, C.K.; Lampert, M.L.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E. Enriching Medication Review with a Pharmacogenetic Profile—A Case of Tamoxifen Adverse Drug Reactions. Pharm. Pers. Med. 2021, 14, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Stäuble, C.K.; Lampert, M.L.; Mikoteit, T.; Hatzinger, M.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E. Severe Adverse Drug Reactions to Quetiapine in Two Patients Carrying CYP2D6*4 Variants: A Case Report. Int. J. Mol. Sci. 2021, 22, 6480. [Google Scholar] [CrossRef] [PubMed]
- Stäuble, C.K.; Lampert, M.L.; Mikoteit, T.; Hatzinger, M.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E. Pharmacogenetic-Guided Antidepressant Selection as an Opportunity for Interprofessional Collaboration: A Case Report. Life 2021, 11, 673. [Google Scholar] [CrossRef] [PubMed]
- Jeiziner, C.; Allemann, S.S.; Hersberger, K.E.; Meyer Zu Schwabedissen, H.E. Is Pharmacogenetic Panel Testing Applicable to Low-Dose Methotrexate in Rheumatoid Arthritis?—A Case Report. Pharm. Pers. Med. 2022, 15, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Stäuble, C.K.; Meier, R.; Lampert, M.L.; Mikoteit, T.; Hatzinger, M.; Allemann, S.S.; Hersberger, K.E.; Meyer zu Schwabedissen, H.E. Case Report: Non-Response to Fluoxetine in a homozygous 5-HTTLPR S-Allele Carrier of the Serotonin Transporter Gene. Front. Psychiatry 2022, accepted. [Google Scholar] [CrossRef]
- Jeiziner, C.; Meyer Zu Schwabedissen, H.E.; Hersberger, K.E.; Allemann, S.S. Pharmacogenetic testing and counseling in the community pharmacy: Evaluation of a new pharmacist-led service. 2022; submitted for publication. [Google Scholar]
- Messerli, M.; Blozik, E.; Vriends, N.; Hersberger, K.E. Impact of a community pharmacist-led medication review on medicines use in patients on polypharmacy—A prospective randomised controlled trial. BMC Health Serv. Res. 2016, 16, 145. [Google Scholar] [CrossRef] [Green Version]
- Phan, L.; Jin, Y.; Zhang, H.; Qiang, W.; Shekhtman, E.; Shao, D.; Revoe, D.; Villamarin, R.; Ivanchenko, E.; Kimura, M.; et al. ALFA: Allele Frequency Aggregator. Available online: https://www.ncbi.nlm.nih.gov/snp/docs/gsr/alfa/ (accessed on 10 February 2022).
- Van Der Wouden, C.H.; Bank, P.C.D.; Özokcu, K.; Swen, J.J.; Guchelaar, H.-J. Pharmacist-Initiated Pre-Emptive Pharmacogenetic Panel Testing with Clinical Decision Support in Primary Care: Record of PGx Results and Real-World Impact. Genes 2019, 10, 416. [Google Scholar] [CrossRef] [Green Version]
- Luke, M.J.; Krupetsky, N.; Liu, H.; Korenvain, C.; Crown, N.; Toenjes, S.; Sproule, B.A.; Piquette-Miller, M.; Guirguis, L.M.; McCarthy, L.M. Pharmacists as Personalized Medicine Experts (PRIME): Experiences Implementing Pharmacist-Led Pharmacogenomic Testing in Primary Care Practices. Pharmacy 2021, 9, 201. [Google Scholar] [CrossRef]
- Botschaft zum Bundesgesetz Über Genetische Untersuchungen Beim Menschen (5 July 2017). Bundesblatt 2017, 5597–5756. Available online: https://www.fedlex.admin.ch/eli/fga/2017/1501/de (accessed on 3 May 2021).


{kind=link}
{kind=link}
| Characteristic | Category | Number (%) or Median (IQR) |
|---|---|---|
| Subjects, n | - | 142 |
| Age (years), median (IQR) | - | 52 (40–63) (min. 18, max. 88) |
| Gender, n (%) | Female | 93 (65.5) |
| Male | 49 (34.5) | |
| Referring party, n (%) | Medical specialist | 92 (64.8) |
| General practitioner | 25 (17.6) | |
| Pharmacist | 25 (17.6) | |
| Enrollment setting, n (%) | Community pharmacy | 85 (59.9) |
| Hospital pharmacy | 57 (40.1) | |
| Main diagnosis, n (%) | Mental and behavioral disorders (ICD-10: F) | 86 (60.6) |
| Diseases of the musculoskeletal system and connective tissue (ICD-10: M) | 30 (21.1) | |
| Diseases of the circulatory system (ICD-10: I) | 15 (10.6) | |
| Other * | 11 (7.8) | |
| Number of prescribed medicines, median (IQR) | - | 6 (4–9) |
| Polypharmacy (≥5 prescribed medicines), n (%) | - | 92 (62.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stäuble, C.K.; Jeiziner, C.; Bollinger, A.; Wiss, F.M.; Hatzinger, M.; Hersberger, K.E.; Ihde, T.; Lampert, M.L.; Mikoteit, T.; Meyer zu Schwabedissen, H.E.; et al. A Guide to a Pharmacist-Led Pharmacogenetic Testing and Counselling Service in an Interprofessional Healthcare Setting. Pharmacy 2022, 10, 86. https://doi.org/10.3390/pharmacy10040086
Stäuble CK, Jeiziner C, Bollinger A, Wiss FM, Hatzinger M, Hersberger KE, Ihde T, Lampert ML, Mikoteit T, Meyer zu Schwabedissen HE, et al. A Guide to a Pharmacist-Led Pharmacogenetic Testing and Counselling Service in an Interprofessional Healthcare Setting. Pharmacy. 2022; 10(4):86. https://doi.org/10.3390/pharmacy10040086
Chicago/Turabian StyleStäuble, Céline K., Chiara Jeiziner, Anna Bollinger, Florine M. Wiss, Martin Hatzinger, Kurt E. Hersberger, Thomas Ihde, Markus L. Lampert, Thorsten Mikoteit, Henriette E. Meyer zu Schwabedissen, and et al. 2022. "A Guide to a Pharmacist-Led Pharmacogenetic Testing and Counselling Service in an Interprofessional Healthcare Setting" Pharmacy 10, no. 4: 86. https://doi.org/10.3390/pharmacy10040086
APA StyleStäuble, C. K., Jeiziner, C., Bollinger, A., Wiss, F. M., Hatzinger, M., Hersberger, K. E., Ihde, T., Lampert, M. L., Mikoteit, T., Meyer zu Schwabedissen, H. E., & Allemann, S. S. (2022). A Guide to a Pharmacist-Led Pharmacogenetic Testing and Counselling Service in an Interprofessional Healthcare Setting. Pharmacy, 10(4), 86. https://doi.org/10.3390/pharmacy10040086