
CLSI Validation of Exchangeable Copper Determination in Serum by ICP-MS: A Focus on Alzheimer’s Disease and Wilson Disease

 ,
,  ,
,  ,
, 
Abstract

1. Introduction
2. Methods
2.1. Subjects
2.2. Analytical Methods
2.3. Reagents and Solutions
2.4. Assay
2.5. Biochemical and Molecular Investigations: Standard Copper Studies
2.6. Statistical Methods
2.7. Analytical Validation of Exchangeable Copper (ExcCu) According to CLSI Guidelines
3. Results
3.1. Exchangeable Copper Test CLSI Validation
3.2. Precision (EP05-A3)
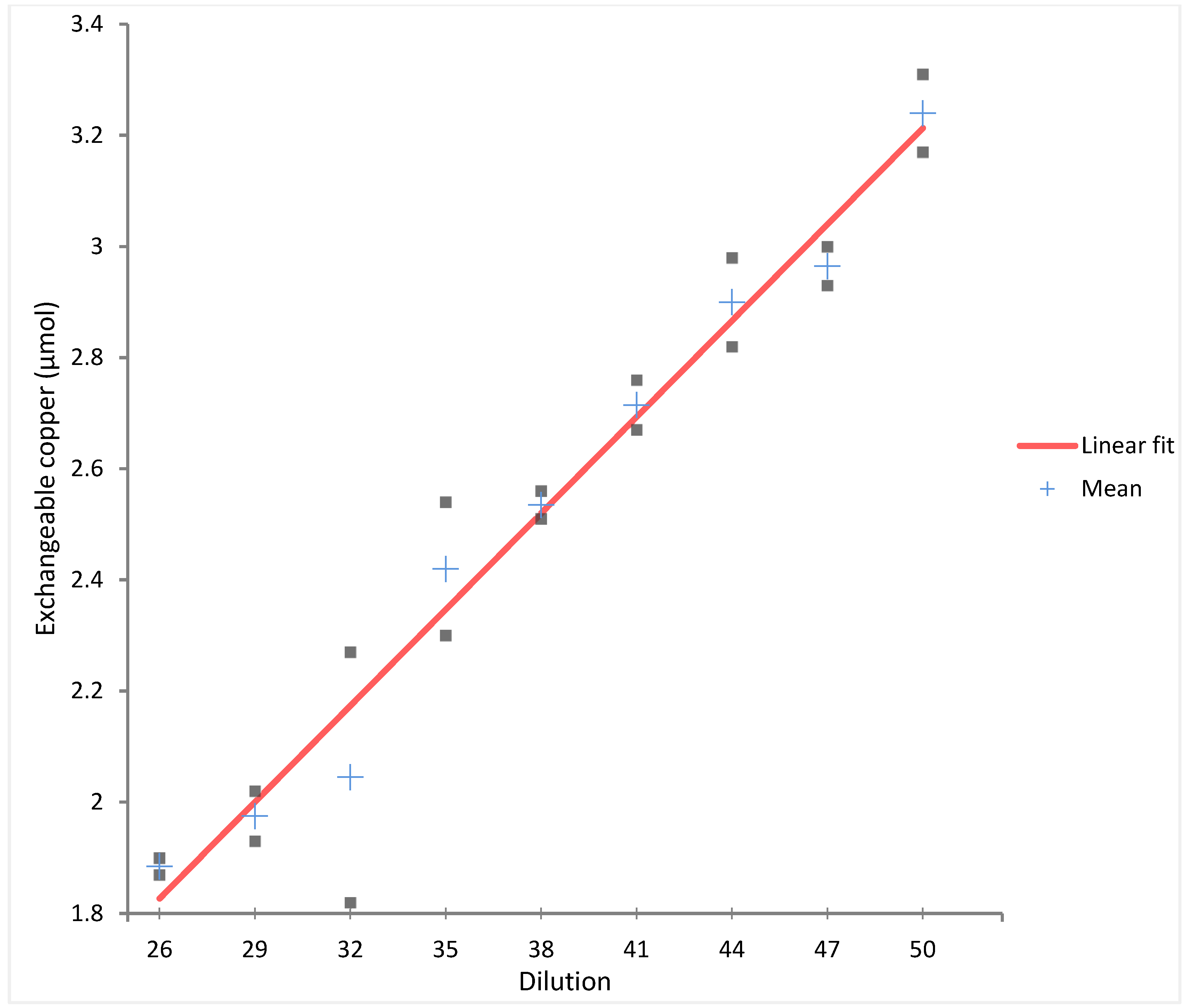
3.3. Linearity (EP06-A)
3.4. Limit of Detection (EP17-A)
- -
- LoB (Limit of Blank): 0.0002 µmol/L
- -
- LoD (Limit of Detection): 0.0397 µmol/L
3.5. Recovery
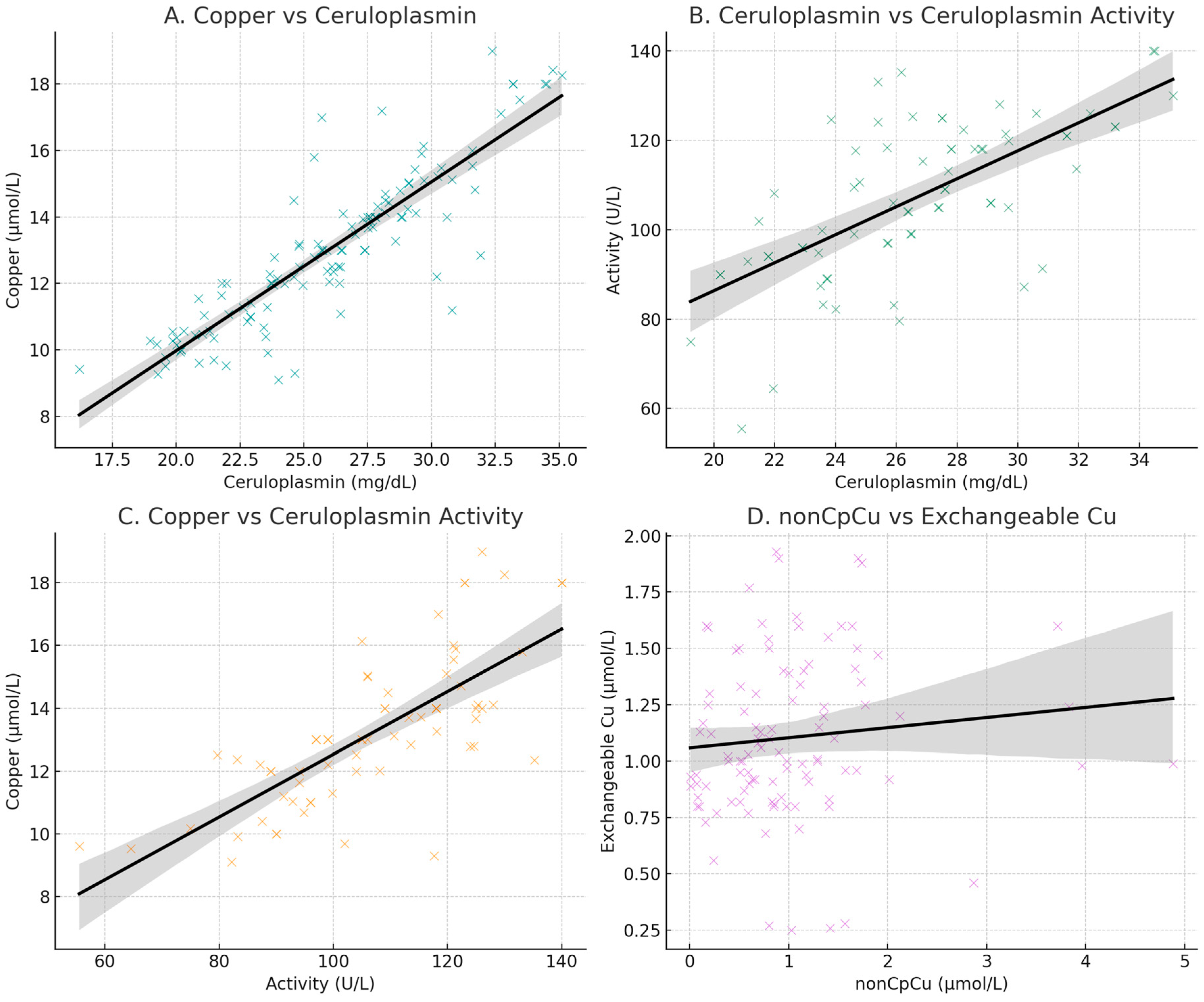
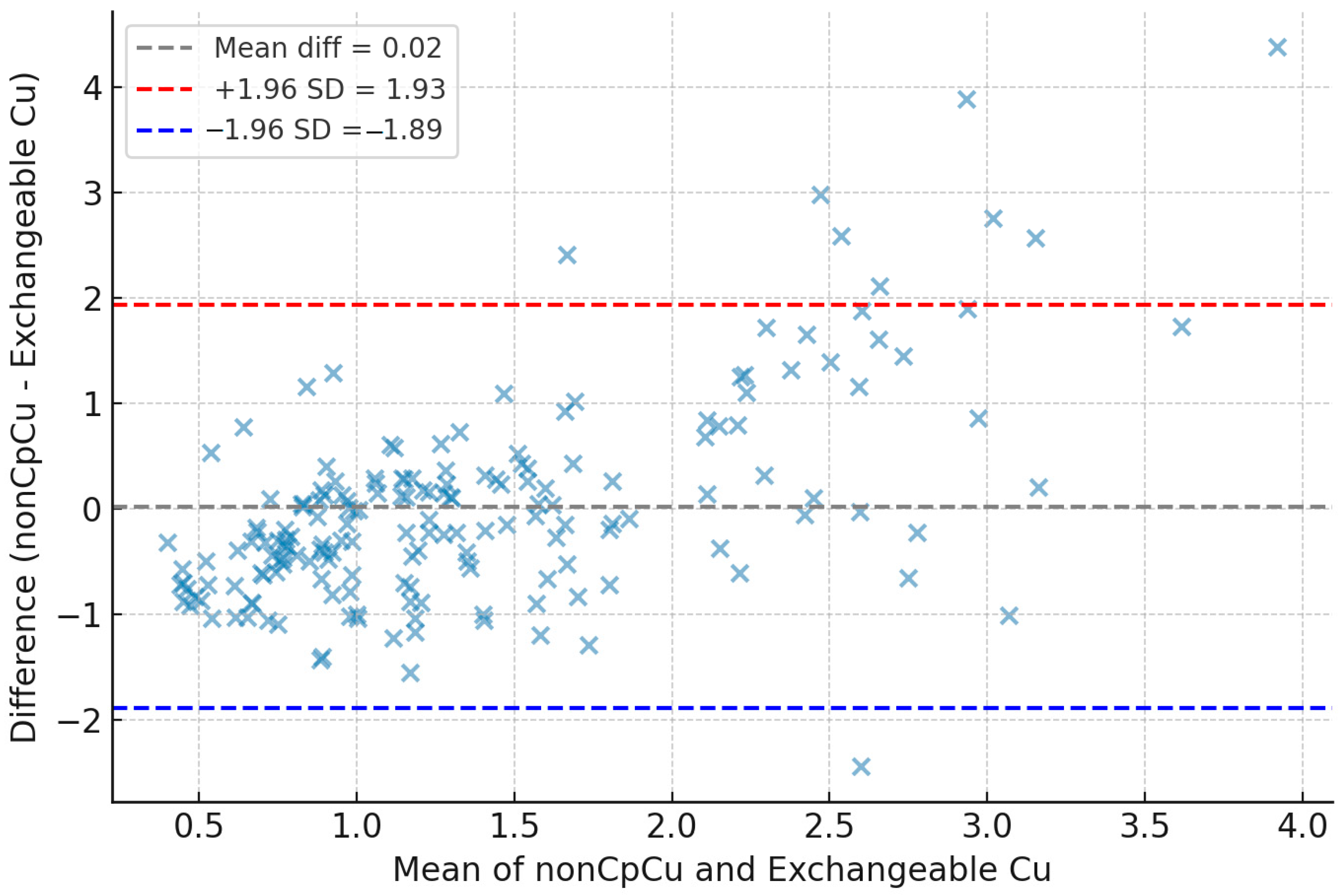
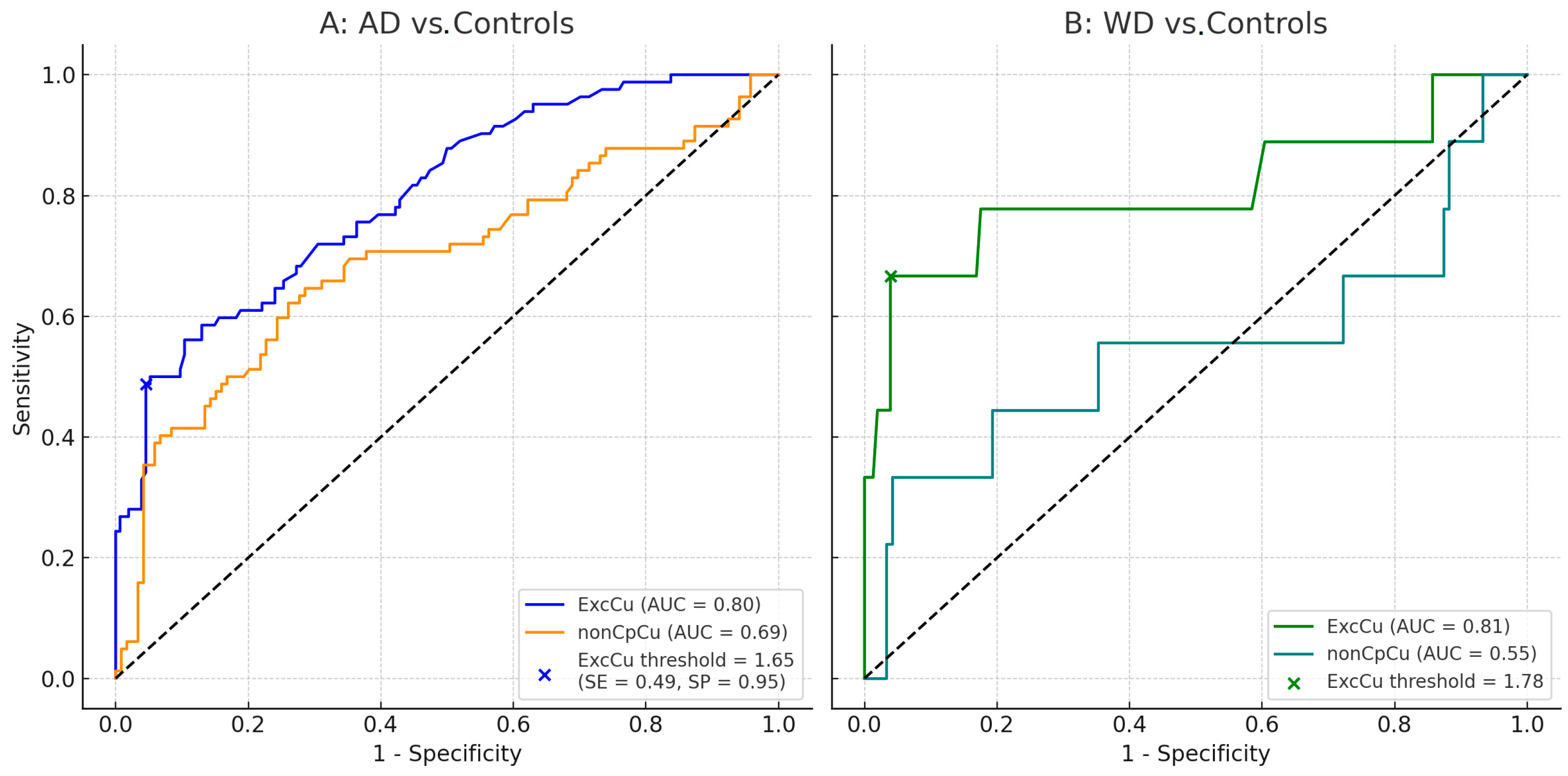
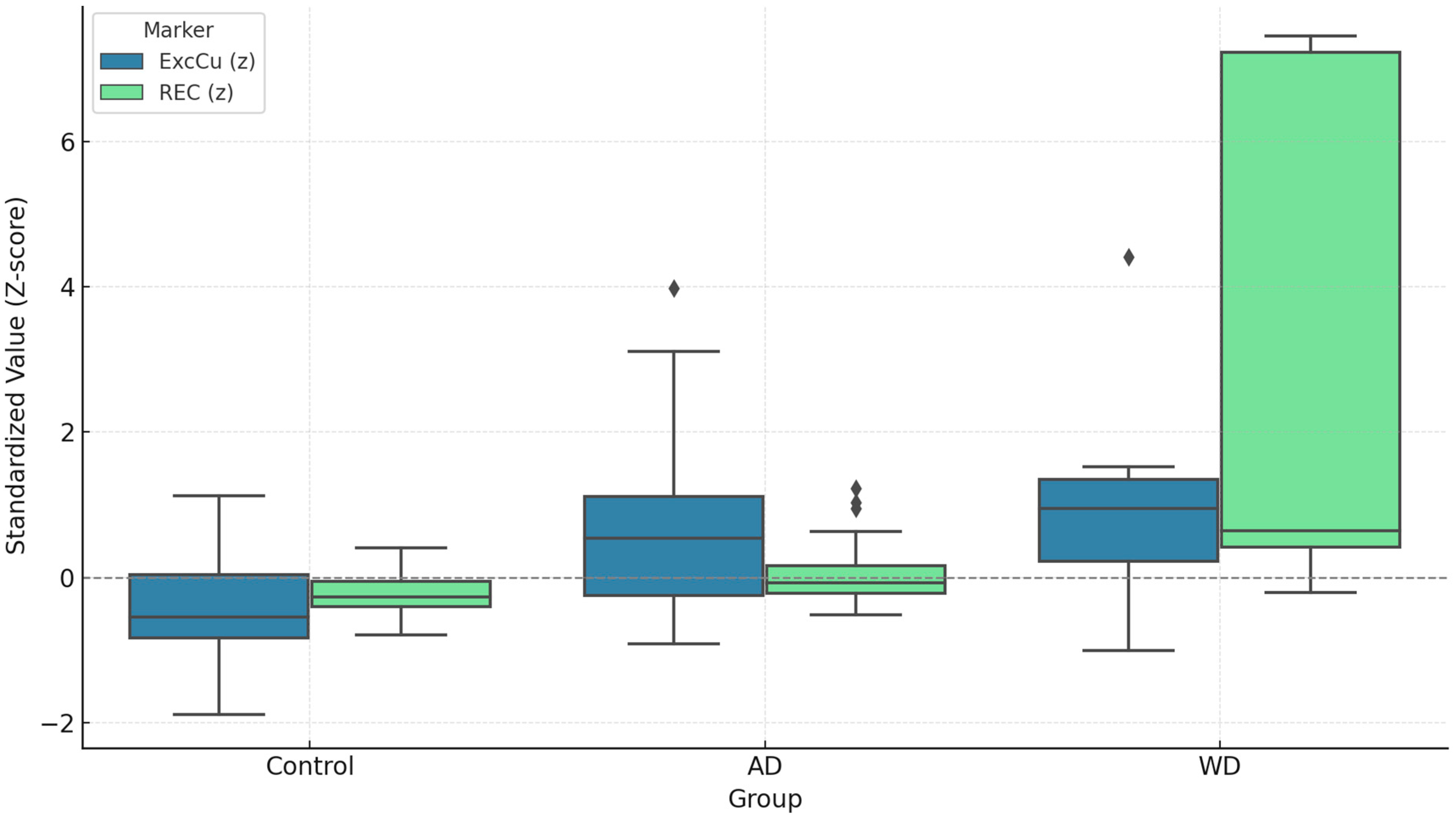
3.6. Agreement and Concordance Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Dyck, C.H.; Swanson, C.J.; Aisen, P.; Bateman, R.J.; Chen, C.; Gee, M.; Kanekiyo, M.; Li, D.; Reyderman, L.; Cohen, S.; et al. Lecanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 388, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Mintun, M.A.; Lo, A.C.; Duggan Evans, C.; Wessels, A.M.; Ardayfio, P.A.; Andersen, S.W.; Shcherbinin, S.; Sparks, J.; Sims, J.R.; Brys, M.; et al. Donanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2021, 384, 1691–1704. [Google Scholar] [CrossRef] [PubMed]
- Bateman, R.J.; Smith, J.; Donohue, M.C.; Delmar, P.; Abbas, R.; Salloway, S.; Wojtowicz, J.; Blennow, K.; Bittner, T.; Black, S.E.; et al. Two Phase 3 Trials of Gantenerumab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 389, 1862–1876. [Google Scholar] [CrossRef]
- Andrews, D.; Ducharme, S.; Chertkow, H.; Sormani, M.P.; Collins, D.L.; Alzheimer’s Disease Neuroimaging Initiative. The higher benefit of lecanemab in males compared to females in CLARITY AD is probably due to a real sex effect. Alzheimers Dement. 2025, 21, e14467. [Google Scholar] [CrossRef]
- Salloway, S.; Chalkias, S.; Barkhof, F.; Burkett, P.; Barakos, J.; Purcell, D.; Suhy, J.; Forrestal, F.; Tian, Y.; Umans, K.; et al. Amyloid-Related Imaging Abnormalities in 2 Phase 3 Studies Evaluating Aducanumab in Patients with Early Alzheimer Disease. JAMA Neurol. 2022, 79, 13–21. [Google Scholar] [CrossRef]
- Campbell, C.H.; Brown, R.; Linder, M.C. Circulating ceruloplasmin is an important source of copper for normal and malignant animal cells. Biochim. Biophys. Acta 1981, 678, 27–38. [Google Scholar] [CrossRef]
- Ala, A.; Walker, A.P.; Ashkan, K.; Dooley, J.S.; Schilsky, M.L. Wilson’s disease. Lancet 2007, 369, 397–408. [Google Scholar] [CrossRef]
- Roberts, E.A.; Schilsky, M.L.; American Association for Study of Liver Diseases. Diagnosis and treatment of Wilson disease: An update. Hepatology 2008, 47, 2089–2111. [Google Scholar] [CrossRef]
- Li, Y.Q.; Tan, S.S.; Wu, D.; Zhang, Q.; Wang, T.; Zheng, G. The role of intracellular and extracellular copper compartmentalization in Alzheimer’s disease pathology and its implications for diagnosis and therapy. Front. Neurosci. 2025, 19, 1553064. [Google Scholar] [CrossRef]
- Squitti, R.; Ventriglia, M.; Simonelli, I.; Bonvicini, C.; Costa, A.; Perini, G.; Binetti, G.; Benussi, L.; Ghidoni, R.; Koch, G.; et al. Copper Imbalance in Alzheimer’s Disease: Meta-Analysis of Serum, Plasma, and Brain Specimens, and Replication Study Evaluating ATP7B Gene Variants. Biomolecules 2021, 11, 960. [Google Scholar] [CrossRef]
- Scolari Grotto, F.; Glaser, V. Are high copper levels related to Alzheimer’s and Parkinson’s diseases? A systematic review and meta-analysis of articles published between 2011 and 2022. Biometals 2024, 37, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Tabuas-Pereira, M.; Guerreiro, R.; Kun-Rodrigues, C.; Almeida, M.R.; Bras, J.; Santana, I. Whole-exome sequencing reveals PSEN1 and ATP7B combined variants as a possible cause of early-onset Lewy body dementia: A case study of genotype-phenotype correlation. Neurogenetics 2022, 23, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Bandmann, O.; Weiss, K.H.; Kaler, S.G. Wilson’s disease and other neurological copper disorders. Lancet Neurol. 2015, 14, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Mercer, S.W.; Wang, J.; Burke, R. In Vivo Modeling of the Pathogenic Effect of Copper Transporter Mutations That Cause Menkes and Wilson Diseases, Motor Neuropathy, and Susceptibility to Alzheimer’s Disease. J. Biol. Chem. 2017, 292, 4113–4122. [Google Scholar] [CrossRef]
- Tsvetkov, P.; Coy, S.; Petrova, B.; Dreishpoon, M.; Verma, A.; Abdusamad, M.; Rossen, J.; Joesch-Cohen, L.; Humeidi, R.; Spangler, R.D.; et al. Copper induces cell death by targeting lipoylated TCA cycle proteins. Science 2022, 375, 1254–1261. [Google Scholar] [CrossRef]
- Walshe, J.M.; Clinical Investigations Standing Committee of the Association of Clinical Biochemists. Wilson’s disease: The importance of measuring serum caeruloplasmin non-immunologically. Ann. Clin. Biochem. 2003, 40, 115–121. [Google Scholar] [CrossRef]
- Squitti, R.; Siotto, M.; Cassetta, E.; Idrissi, I.G.; Colabufo, N.A. Measurements of serum non-ceruloplasmin copper by a direct fluorescent method specific to Cu(II). Clin. Chem. Lab. Med. 2017, 55, 1360–1367. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Squitti, R.; Catalli, C.; Gigante, L.; Marianetti, M.; Rosari, M.; Mariani, S.; Bucossi, S.; Mastromoro, G.; Ventriglia, M.; Simonelli, I.; et al. Non-Ceruloplasmin Copper Identifies a Subtype of Alzheimer’s Disease (CuAD): Characterization of the Cognitive Profile and Case of a CuAD Patient Carrying an RGS7 Stop-Loss Variant. Int. J. Mol. Sci. 2023, 24, 6377. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Wilson’s disease. J. Hepatol. 2012, 56, 671–685. [Google Scholar] [CrossRef] [PubMed]
- El Balkhi, S.; Poupon, J.; Trocello, J.M.; Leyendecker, A.; Massicot, F.; Galliot-Guilley, M.; Woimant, F. Determination of ultrafiltrable and exchangeable copper in plasma: Stability and reference values in healthy subjects. Anal. Bioanal. Chem. 2009, 394, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- El Balkhi, S.; Trocello, J.M.; Poupon, J.; Chappuis, P.; Massicot, F.; Girardot-Tinant, N.; Woimant, F. Relative exchangeable copper: A new highly sensitive and highly specific biomarker for Wilson’s disease diagnosis. Clin. Chim. Acta 2011, 412, 2254–2260. [Google Scholar] [CrossRef]
- McMillin, G.A.; Travis, J.J.; Hunt, J.W. Direct measurement of free copper in serum or plasma ultrafiltrate. Am. J. Clin. Pathol. 2009, 131, 160–165. [Google Scholar] [CrossRef]
- Catalani, S.; Paganelli, M.; Gilberti, M.E.; Rozzini, L.; Lanfranchi, F.; Padovani, A.; Apostoli, P. Free copper in serum: An analytical challenge and its possible applications. J. Trace Elem. Med. Biol. 2018, 45, 176–180. [Google Scholar] [CrossRef]
- Twomey, P.J.; Viljoen, A.; House, I.M.; Reynolds, T.M.; Wierzbicki, A.S. Relationship between serum copper, ceruloplasmin, and non-ceruloplasmin-bound copper in routine clinical practice. Clin. Chem. 2005, 51, 1558–1559. [Google Scholar] [CrossRef]
- Twomey, P.J.; Viljoen, A.; House, I.M.; Reynolds, T.M.; Wierzbicki, A.S. Copper:caeruloplasmin ratio. J. Clin. Pathol. 2007, 60, 441–442. [Google Scholar] [CrossRef]
- Twomey, P.J.; Wierzbicki, A.S.; Reynolds, T.M.; Viljoen, A. The copper/caeruloplasmin ratio in routine clinical practice in different laboratories. J. Clin. Pathol. 2009, 62, 60–63. [Google Scholar] [CrossRef]
- Guillaud, O.; Brunet, A.S.; Mallet, I.; Dumortier, J.; Pelosse, M.; Heissat, S.; Rivet, C.; Lachaux, A.; Bost, M. Relative exchangeable copper: A valuable tool for the diagnosis of Wilson disease. Liver Int. 2018, 38, 350–357. [Google Scholar] [CrossRef]
- Spirea, D.; Vanlemmens, C.; Parant, F.; Antonini, T.; Bost, M.; Lachaux, A.; Belmalih, A.; Guillaud, O.; Dumortier, J.; Couchonnal, E. Performance of Relative Exchangeable Copper for the Diagnosis of Wilson Disease in Acute Liver Failure. J. Inherit. Metab. Dis. 2025, 48, e70024. [Google Scholar] [CrossRef]
- Heissat, S.; Harel, A.; Um, K.; Brunet, A.S.; Hervieu, V.; Guillaud, O.; Dumortier, J.; Lachaux, A.; Mintz, E.; Bost, M. Evaluation of the accuracy of exchangeable copper and relative exchangeable copper (REC) in a mouse model of Wilson’s disease. J. Trace Elem. Med. Biol. 2018, 50, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Ozarda, Y. Reference intervals: Current status, recent developments and future considerations. Biochem. Med 2016, 26, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Kenney, S.M.; Cox, D.W. Sequence variation database for the Wilson disease copper transporter, ATP7B. Hum. Mutat. 2007, 28, 1171–1177. [Google Scholar] [CrossRef]
- Schushan, M.; Bhattacharjee, A.; Ben-Tal, N.; Lutsenko, S. A structural model of the copper ATPase ATP7B to facilitate analysis of Wilson disease-causing mutations and studies of the transport mechanism. Metallomics 2012, 4, 669–678. [Google Scholar] [CrossRef]
- Michalczyk, A.A.; Rieger, J.; Allen, K.J.; Mercer, J.F.; Ackland, M.L. Defective localization of the Wilson disease protein (ATP7B) in the mammary gland of the toxic milk mouse and the effects of copper supplementation. Biochem. J. 2000, 352 Pt 2, 565–571. [Google Scholar] [CrossRef]
- Lutsenko, S.; Barnes, N.L.; Bartee, M.Y.; Dmitriev, O.Y. Function and regulation of human copper-transporting ATPases. Physiol. Rev. 2007, 87, 1011–1046. [Google Scholar] [CrossRef]
- Kupila-Rantala, T.; Dabek, J.T.; Hyvonen-Dabek, M. A high resolution PIXE measurement for blood plasma ultrafiltrate. Application to loosely bound copper. Biol. Trace Elem. Res. 1996, 55, 173–179. [Google Scholar] [CrossRef]
- Solovyev, N.; Ala, A.; Schilsky, M.; Mills, C.; Willis, K.; Harrington, C.F. Biomedical copper speciation in relation to Wilson’s disease using strong anion exchange chromatography coupled to triple quadrupole inductively coupled plasma mass spectrometry. Anal. Chim. Acta 2020, 1098, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo Busto, M.E.; Cuello-Nunez, S.; Ward-Deitrich, C.; Morley, T.; Goenaga-Infante, H. A fit-for-purpose copper speciation method for the determination of exchangeable copper relevant to Wilson’s disease. Anal. Bioanal. Chem. 2022, 414, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.; Sandahl, T.; Ala, A.; Cassiman, D.; Couchonnal-Bedoya, E.; Cury, R.G.; Czlonkowska, A.; Denk, G.; D’Inca, R.; de Assis Aquino Gondim, F.; et al. Non-ceruloplasmin copper and urinary copper in clinically stable Wilson disease: Alignment with recommended targets. JHEP Rep. 2024, 6, 101115. [Google Scholar] [CrossRef] [PubMed]
- Braga, F.; Szoke, D.; Valente, C.; Panteghini, M. Biologic variation of copper, ceruloplasmin and copper/ceruloplasmin ratio (Cu:Cp) in serum. Clin. Chim. Acta 2013, 415, 295–296. [Google Scholar] [CrossRef]
- Chen, G.; Xi, E.; Gu, X.; Wang, H.; Tang, Q. The study on cuproptosis in Alzheimer’s disease based on the cuproptosis key gene FDX1. Front. Aging Neurosci. 2024, 16, 1480332. [Google Scholar] [CrossRef]
- Jia, F.; Han, W.; Gao, S.; Huang, J.; Zhao, W.; Lu, Z.; Zhao, W.; Li, Z.; Wang, Z.; Guo, Y. Novel cuproptosis metabolism-related molecular clusters and diagnostic signature for Alzheimer’s disease. Front. Mol. Biosci. 2024, 11, 1478611. [Google Scholar] [CrossRef]
- Ma, M.M.; Zhao, J.; Liu, L.; Wu, C.Y. Identification of cuproptosis-related genes in Alzheimer’s disease based on bioinformatic analysis. Eur. J. Med. Res. 2024, 29, 495. [Google Scholar] [CrossRef]
- Hu, R.; Xiao, Z.; Qiao, M.; Liu, C.; Wu, G.; Wang, Y.; Dong, M.; Huang, Z. Construction and validation of a bioinformatics-based screen for cuproptosis-related genes and risk model for Alzheimer’s disease. Mol. Med. Rep. 2024, 30, 194. [Google Scholar] [CrossRef]
- Zeng, Y.; Qian, S.; Cao, Y.; Xiao, W. Unravelling the complex interplay of cuproptosis, lncRNAs, and immune infiltration in Alzheimer’s disease: A step towards novel therapeutic targets. Ann. Hum. Biol. 2024, 51, 2342531. [Google Scholar] [CrossRef]
- Zhang, E.; Dai, F.; Chen, T.; Liu, S.; Xiao, C.; Shen, X. Diagnostic models and predictive drugs associated with cuproptosis hub genes in Alzheimer’s disease. Front. Neurol. 2022, 13, 1064639. [Google Scholar] [CrossRef]
- Lai, Y.; Lin, C.; Lin, X.; Wu, L.; Zhao, Y.; Lin, F. Identification and immunological characterization of cuproptosis-related molecular clusters in Alzheimer’s disease. Front. Aging Neurosci. 2022, 14, 932676. [Google Scholar] [CrossRef]
- Squitti, R.; Ventriglia, M.; Gennarelli, M.; Colabufo, N.A.; El Idrissi, I.G.; Bucossi, S.; Mariani, S.; Rongioletti, M.; Zanetti, O.; Congiu, C.; et al. Non-Ceruloplasmin Copper Distincts Subtypes in Alzheimer’s Disease: A Genetic Study of ATP7B Frequency. Mol. Neurobiol. 2017, 54, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Squitti, R.; Faller, P.; Hureau, C.; Granzotto, A.; White, A.R.; Kepp, K.P. Copper Imbalance in Alzheimer’s Disease and Its Link with the Amyloid Hypothesis: Towards a Combined Clinical, Chemical, and Genetic Etiology. J. Alzheimers Dis. 2021, 83, 23–41. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ExcCu Level (µmol/L) | Mean | Repeatability SD (CV%) | Within-Lab SD (CV%) | |
|---|---|---|---|---|
| Low (0.86) | 0.862 | 0.035 (4.1%) | 0.059 (6.8%) | |
| Medium (1.21) | 1.209 | 0.048 (4.0%) | 0.061 (5.0%) | |
| High (2.08) | 2.080 | 0.056 (2.7%) | 0.092 (4.4%) | |
| (A) Low ExcCu level (0.86 µmol/L). | ||||
| Component | % of Total | SD | 95% CI | CV |
| Repeatability | 36.0% | 0.035 | 0.029 to 0.045 | 4.1% |
| Between Run | 18.3% | 0.025 | 0.000 to 0.045 | 2.9% |
| Within Day | 54.3% | 0.043 | 0.036 to 0.057 | 5.0% |
| Between Day | 45.7% | 0.040 | 0.021 to 0.064 | 4.6% |
| Within Laboratory | 100.0% | 0.059 | 0.050 to 0.078 | 6.8% |
| (B) Medium ExcCu level (1.21 µmol/L). | ||||
| Component | % of Total | SD | 95% CI | CV |
| Repeatability | 63.8% | 0.048 | 0.040 to 0.062 | 4.0% |
| Between Run | 14.0% | 0.023 | 0.000 to 0.049 | 1.9% |
| Within Day | 77.8% | 0.053 | 0.045 to 0.069 | 4.4% |
| Between Day | 22.2% | 0.029 | 0.000 to 0.052 | 2.4% |
| Within Laboratory | 100.0% | 0.061 | 0.053 to 0.077 | 5.0% |
| (C) High ExcCu level (2.08 µmol/L). | ||||
| Component | % of Total | SD | 95% CI | CV |
| Repeatability | 37.8% | 0.056 | 0.046 to 0.072 | 2.7% |
| Between Run | 12.8% | 0.033 | 0.000 to 0.063 | 1.6% |
| Within Day | 50.6% | 0.065 | 0.055 to 0.085 | 3.1% |
| Between Day | 49.4% | 0.064 | 0.038 to 0.102 | 3.1% |
| Within Laboratory | 100.0% | 0.092 | 0.077 to 0.122 | 4.4% |
| Linear Fit | |||||
| Parameter | Estimate | SE | t | DF | p-Value |
| Constant | 0.3255 | 0.14239 | 2.29 | 16 | 0.0362 |
| X | 0.05775 | 0.0036715 | −256.64 | 16 | <0.0001 |
| 2nd-Order Polynomial Fit | |||||
| Parameter | Estimate | SE | t | DF | p-Value |
| Constant | 0.4129 | 0.78564 | 0.53 | 15 | 0.6069 |
| X | 0.05295 | 0.04255 | −22.26 | 15 | <0.0001 |
| X2 | 6.313 × 10−5 | 0.00055764 | 0.11 | 15 | 0.9114 |
| 3rd-Order Polynomial Fit | |||||
| Parameter | Estimate | SE | t | DF | p-Value |
| Constant | 3.155 | 4.5581 | 0.69 | 14 | 0.5002 |
| X | −0.1750 | 0.3755 | −3.13 | 14 | 0.0074 |
| X2 | 0.006212 | 0.010078 | 0.62 | 14 | 0.5475 |
| X3 | −5.393 × 10−5 | 8.8262 × 10−5 | −0.61 | 14 | 0.5509 |
| Limit of Blank (LoB) | ||||
| N | Mean | SD | Alpha | Critical Value (LoB) |
| 60 | 0.00010 | 0.00008 | 5% | 0.0002 |
| Limit of Detection (LoD) | ||||
| N | Pooled SD | Beta | Detection Limit (LoD) | |
| 60 | 0.02387 | 5% | 0.0397 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Squitti, R.; Pal, A.; Ivanova, I.D.; Marianetti, M.; Rongioletti, M. CLSI Validation of Exchangeable Copper Determination in Serum by ICP-MS: A Focus on Alzheimer’s Disease and Wilson Disease. Biomolecules 2025, 15, 788. https://doi.org/10.3390/biom15060788
Squitti R, Pal A, Ivanova ID, Marianetti M, Rongioletti M. CLSI Validation of Exchangeable Copper Determination in Serum by ICP-MS: A Focus on Alzheimer’s Disease and Wilson Disease. Biomolecules. 2025; 15(6):788. https://doi.org/10.3390/biom15060788
Chicago/Turabian StyleSquitti, Rosanna, Amit Pal, Irena D. Ivanova, Massimo Marianetti, and Mauro Rongioletti. 2025. "CLSI Validation of Exchangeable Copper Determination in Serum by ICP-MS: A Focus on Alzheimer’s Disease and Wilson Disease" Biomolecules 15, no. 6: 788. https://doi.org/10.3390/biom15060788
APA StyleSquitti, R., Pal, A., Ivanova, I. D., Marianetti, M., & Rongioletti, M. (2025). CLSI Validation of Exchangeable Copper Determination in Serum by ICP-MS: A Focus on Alzheimer’s Disease and Wilson Disease. Biomolecules, 15(6), 788. https://doi.org/10.3390/biom15060788