
Targeting Gastrointestinal Cancers with Carvacrol: Mechanistic Insights and Therapeutic Potential

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Methodology
- •
- Studies investigating the effects of carvacrol on esophageal, gastric, colorectal, pancreatic, and liver cancer using animal models or in vitro experiments.
- •
- Research evaluating carvacrol alone or in combination with other bioactive compounds.
- •
- Preclinical studies (both in vitro and in vivo) that report on molecular alterations (such as altered gene or protein expression) or biological outcomes (such as inhibiting tumor growth, halting metastasis, or inducing apoptosis).
- •
- English-language publications in peer-reviewed journals.
- •
- Research studies that do not specifically focus on the cancers of interest (e.g., general cancer research or studies on mixed cancer types without separate analyses).
- •
- Research that does not evaluate the effects of carvacrol.
- •
- Articles missing applicable biological, clinical, or molecular results or statistics.
- •
- Non-peer-reviewed publications.
- •
- Non-English-language publications.
3. Chemistry and Derivatization
4. Pathophysiology of Gastrointestinal Cancer
5. Therapeutic Effects of Carvacrol on Gastrointestinal Cancers
5.1. Esophageal Cancer
5.2. Gastric Cancer
5.3. Pancreatic Cancer
5.4. Liver Cancer
5.5. Colorectal Cancer
6. Toxicological Profile and Safety Assessment of Carvacrol
7. Role of Nanotechnology and Synergism
7.1. Nanotechnology Applications
7.2. Synergistic Therapeutic Approaches
8. Conclusions and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Marino, P.; Mininni, M.; Deiana, G.; Marino, G.; Divella, R.; Bochicchio, I.; Giuliano, A.; Lapadula, S.; Lettini, A.R.; Sanseverino, F. Healthy Lifestyle and Cancer Risk: Modifiable Risk Factors to Prevent Cancer. Nutrients 2024, 16, 800. [Google Scholar] [CrossRef] [PubMed]
- Mee, T.; Kirkby, N.F.; Defourny, N.N.; Kirkby, K.J.; Burnet, N.G. The use of radiotherapy, surgery and chemotherapy in the curative treatment of cancer: Results from the FORTY (Favourable Outcomes from RadioTherapY) project. Br. J. Radiol. 2023, 96, 20230334. [Google Scholar] [CrossRef] [PubMed]
- Schirrmacher, V. From chemotherapy to biological therapy: A review of novel concepts to reduce the side effects of systemic cancer treatment (Review). Int. J. Oncol. 2019, 54, 407–419. [Google Scholar] [CrossRef]
- Liparulo, J.T.; Knab, T.D.; Parker, R.S. Toxicity-Centric Cancer Chemotherapy Treatment Design. Ifac Pap. 2020, 53, 16353–16358. [Google Scholar] [CrossRef]
- Dulf, P.L.; Mocan, M.; Coada, C.A.; Dulf, D.V.; Moldovan, R.; Baldea, I.; Farcas, A.D.; Blendea, D.; Filip, A.G. Doxorubicin-induced acute cardiotoxicity is associated with increased oxidative stress, autophagy, and inflammation in a murine model. Naunyn Schmiedebergs Arch. Pharmacol. 2023, 396, 1105–1115. [Google Scholar] [CrossRef]
- Albini, A.; Pennesi, G.; Donatelli, F.; Cammarota, R.; De Flora, S.; Noonan, D.M. Cardiotoxicity of anticancer drugs: The need for cardio-oncology and cardio-oncological prevention. J. Natl. Cancer Inst. 2010, 102, 14–25. [Google Scholar] [CrossRef]
- Debnath, J.; Singh, H.P.; George, R.A.; Satija, L.; Chawla, N.; Sarma, Y.S.; Vaidya, A.; Grewal, D.S. Reversible Bleomycin Toxicity. Med. J. Armed Forces India 2010, 66, 290–291. [Google Scholar] [CrossRef]
- Chou, W.H.; McGregor, B.; Schmidt, A.; Carvalho, F.L.F.; Hirsch, M.S.; Chang, S.L.; Kibel, A.; Mossanen, M. Cyclophosphamide-associated bladder cancers and considerations for survivorship care: A systematic review. Urol. Oncol. 2021, 39, 678–685. [Google Scholar] [CrossRef]
- Ranjan, A.; Ramachandran, S.; Gupta, N.; Kaushik, I.; Wright, S.; Srivastava, S.; Das, H.; Srivastava, S.; Prasad, S.; Srivastava, S.K. Role of Phytochemicals in Cancer Prevention. Int. J. Mol. Sci. 2019, 20, 4981. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.Y.; Lei, S.Z.; Xu, W.J.; Lai, Y.X.; Zhang, Y.Y.; Wang, Y.; Wang, Z.L. Rising above: Exploring the therapeutic potential of natural product-based compounds in human cancer treatment. Tradit. Med. Res. 2025, 10, 18. [Google Scholar] [CrossRef]
- George, B.P.; Chandran, R.; Abrahamse, H. Role of Phytochemicals in Cancer Chemoprevention: Insights. Antioxidants 2021, 10, 1455. [Google Scholar] [CrossRef]
- Ahmad, S.S.; Garg, C.; Bhat, A.H.; Kaur, S. Phytochemicals in Cancer Therapy: Modulating Cell Cycle, Angiogenesis, and Epithelial-Mesenchymal Transition. Rev. Bras. Farmacogn. 2025, 35, 255–274. [Google Scholar] [CrossRef]
- Rudzinska, A.; Juchaniuk, P.; Oberda, J.; Wisniewska, J.; Wojdan, W.; Szklener, K.; Mandziuk, S. Phytochemicals in Cancer Treatment and Cancer Prevention-Review on Epidemiological Data and Clinical Trials. Nutrients 2023, 15, 1896. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Li, J.; Shi, L. A Carvacrol-Rich Essential Oil Extracted From Oregano (Origanum vulgare “Hot & Spicy”) Exerts Potent Antibacterial Effects Against Staphylococcus aureus. Front. Microbiol. 2021, 12, 741861. [Google Scholar] [CrossRef]
- Imran, M.; Aslam, M.; Alsagaby, S.A.; Saeed, F.; Ahmad, I.; Afzaal, M.; Arshad, M.U.; Abdelgawad, M.A.; El-Ghorab, A.H.; Khames, A.; et al. Therapeutic application of carvacrol: A comprehensive review. Food Sci. Nutr. 2022, 10, 3544–3561. [Google Scholar] [CrossRef]
- Sampaio, L.A.; Pina, L.T.S.; Serafini, M.R.; Tavares, D.D.S.; Guimarães, A.G. Antitumor Effects of Carvacrol and Thymol: A Systematic Review. Front. Pharmacol. 2021, 12, 702487. [Google Scholar] [CrossRef]
- Gandova, V.; Lazarov, A.; Fidan, H.; Dimov, M.; Stankov, S.; Denev, P.; Ercisli, S.; Stoyanova, A.; Gulen, H.; Assouguem, A.; et al. Physicochemical and biological properties of carvacrol. Open Chem. 2023, 21, 20220319. [Google Scholar] [CrossRef]
- Sharifi-Rad, M.; Varoni, E.M.; Iriti, M.; Martorell, M.; Setzer, W.N.; Del Mar Contreras, M.; Salehi, B.; Soltani-Nejad, A.; Rajabi, S.; Tajbakhsh, M.; et al. Carvacrol and human health: A comprehensive review. Phytother. Res. 2018, 32, 1675–1687. [Google Scholar] [CrossRef]
- Chroho, M.; Rouphael, Y.; Petropoulos, S.A.; Bouissane, L. Carvacrol and Thymol Content Affects the Antioxidant and Antibacterial Activity of Origanum compactum and Thymus zygis Essential Oils. Antibiotics 2024, 13, 139. [Google Scholar] [CrossRef] [PubMed]
- Javed, H.; Meeran, M.F.N.; Jha, N.K.; Ojha, S. Carvacrol, a Plant Metabolite Targeting Viral Protease (M(pro)) and ACE2 in Host Cells Can Be a Possible Candidate for COVID-19. Front. Plant Sci. 2020, 11, 601335. [Google Scholar] [CrossRef]
- Sivaranjani, A.; Sivagami, G.; Nalini, N. Chemopreventive effect of carvacrol on 1,2-dimethylhydrazine induced experimental colon carcinogenesis. J. Cancer Res. Ther. 2016, 12, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Alamri, M.A.; Abdel-Kader, M.S.; Salkini, M.A.; Alamri, M.A. Thymol and carvacrol derivatives as anticancer agents; synthesis, in vitro activity, and computational analysis of biological targets. RSC Adv. 2024, 14, 30662–30672. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.; Saleh, E.I.M.M.; Kar, P.; Roy, A.; Sharma, N.R. Synthesis of Carvacrol Derivatives as Potential New Anticancer Agent against Lung Cancer. Molecules 2022, 27, 4597. [Google Scholar] [CrossRef]
- Bansal, A.; Kaushik, V.; Sharma, N.R. Synthesis and anti-metastatic evaluation of carvacrol derivative, 2-hydroxy-6-isopropyl-3-methylbenzalehyde. Mater. Today-Proc. 2022, 57, 739–747. [Google Scholar] [CrossRef]
- Vasconcelos, A.P.; Xavier, F.J.S.; Castro, A.; Lima, M.F.; Terceiro, L.E.L.; Silva, F.P.L.; Vasconcellos, M.L.A.A.; Dantas, B.B.; Barbosa, A.M.; Duarte, S.S.; et al. Synthesis and Analysis of Carvacrol-Derived Morita-Baylis-Hillman Adducts as Potential Anticancer Agents. J. Braz. Chem. Soc. 2024, 35, e-20240022. [Google Scholar] [CrossRef]
- Mastelic, J.; Jerkovic, I.; Blazevic, I.; Poljak-Blazi, M.; Borovic, S.; Ivancic-Bace, I.; Smrecki, V.; Zarkovic, N.; Brcic-Kostic, K.; Vikic-Topic, D.; et al. Comparative study on the antioxidant and biological activities of carvacrol, thymol, and eugenol derivatives. J. Agr. Food Chem. 2008, 56, 3989–3996. [Google Scholar] [CrossRef]
- Bizari, L.; Borim, A.A.; Leite, K.R.M.; Gonçalves, F.D.; Cury, P.M.; Tajara, E.H.; Silva, A.E. Alterations of the CCND1 and HER-2/neu (ERBB2) proteins in esophageal and gastric cancers. Cancer Genet. Cytogen 2006, 165, 41–50. [Google Scholar] [CrossRef]
- Ishida, H.; Kasajima, A.; Fujishima, F.; Akaishi, R.; Ueki, S.; Yamazaki, Y.; Onodera, Y.; Gao, X.; Okamoto, H.; Taniyama, Y.; et al. p16 in highly malignant esophageal carcinomas: The correlation with clinicopathological factors and human papillomavirus infection. Virchows Arch. 2021, 478, 219–229. [Google Scholar] [CrossRef]
- Zhan, N.; Dong, W.G.; Tang, Y.F.; Wang, Z.S.; Xiong, C.L. Analysis of HER2 gene amplification and protein expression in esophageal squamous cell carcinoma. Med. Oncol. 2012, 29, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Ayyappan, S.; Prabhakar, D.; Sharma, N. Epidermal Growth Factor Receptor (EGFR)-targeted Therapies in Esophagogastric Cancer. Anticancer. Res. 2013, 33, 4139–4155. [Google Scholar]
- Zhu, K.; Yang, X.; Tai, H.; Zhong, X.; Luo, T.; Zheng, H. HER2-targeted therapies in cancer: A systematic review. Biomark. Res. 2024, 12, 16. [Google Scholar] [CrossRef]
- Pharoah, P.D.P.; Guilford, P.; Caldas, C.; Consortiu, I.G.C.L. Incidence of gastric cancer and breast cancer in CDH1 (E-cadherin) mutation carriers from hereditary diffuse gastric cancer families. Gastroenterology 2001, 121, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Bordin, M.C.; Grehan, N.; Huntsman, D.; Suriano, G.; Machado, J.C.; Kiviluoto, T.; Aaltonen, L.; Jackson, C.E.; Seruca, R.; et al. Screening E-cadherin in gastric cancer families reveals germline mutations only in hereditary diffuse gastric cancer kindred. Hum. Mutat. 2002, 19, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Iqbal, N. Human Epidermal Growth Factor Receptor 2 (HER2) in Cancers: Overexpression and Therapeutic Implications. Mol. Biol. Int. 2014, 2014, 852748. [Google Scholar] [CrossRef]
- Yonemura, Y.; Ninomiya, I.; Yamaguchi, A.; Fushida, S.; Kimura, H.; Ohoyama, S.; Miyazaki, I.; Endou, Y.; Tanaka, M.; Sasaki, T. Evaluation of immunoreactivity for erbB-2 protein as a marker of poor short term prognosis in gastric cancer. Cancer Res. 1991, 51, 1034–1038. [Google Scholar]
- Graziano, F.; Fischer, N.W.; Bagaloni, I.; Di Bartolomeo, M.; Lonardi, S.; Vincenzi, B.; Perrone, G.; Fornaro, L.; Ongaro, E.; Aprile, G.; et al. TP53 Mutation Analysis in Gastric Cancer and Clinical Outcomes of Patients with Metastatic Disease Treated with Ramucirumab/Paclitaxel or Standard Chemotherapy. Cancers 2020, 12, 2049. [Google Scholar] [CrossRef]
- Ma, S.; Meng, G.; Liu, T.; You, J.; He, R.; Zhao, X.; Cui, Y. The Wnt signaling pathway in hepatocellular carcinoma: Regulatory mechanisms and therapeutic prospects. Biomed. Pharmacother. 2024, 180, 117508. [Google Scholar] [CrossRef]
- Lanfredini, S.; Thapa, A.; O’Neill, E. RAS in pancreatic cancer. Biochem. Soc. Trans. 2019, 47, 961–972. [Google Scholar] [CrossRef]
- Shi, Y.; Zheng, H.; Wang, T.; Zhou, S.; Zhao, S.; Li, M.; Cao, B. Targeting KRAS: From metabolic regulation to cancer treatment. Mol. Cancer 2025, 24, 9. [Google Scholar] [CrossRef] [PubMed]
- Luo, J. KRAS mutation in pancreatic cancer. Semin. Oncol. 2021, 48, 10–18. [Google Scholar] [CrossRef]
- Danishevich, A.; Bilyalov, A.; Nikolaev, S.; Khalikov, N.; Isaeva, D.; Levina, Y.; Makarova, M.; Nemtsova, M.; Chernevskiy, D.; Sagaydak, O.; et al. CDKN2A Gene Mutations: Implications for Hereditary Cancer Syndromes. Biomedicines 2023, 11, 3343. [Google Scholar] [CrossRef]
- Voutsadakis, I.A. Mutations of p53 associated with pancreatic cancer and therapeutic implications. Ann. Hepatobiliary Pancreat. Surg. 2021, 25, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Ullah, I.; Sun, W.; Tang, L.; Feng, J. Roles of Smads Family and Alternative Splicing Variants of Smad4 in Different Cancers. J. Cancer 2018, 9, 4018–4028. [Google Scholar] [CrossRef] [PubMed]
- Cappell, M.S. Pathophysiology, clinical presentation, and management of colon cancer. Gastroenterol. Clin. North. Am. 2008, 37, 1–24. [Google Scholar] [CrossRef]
- Narayan, S.; Roy, D. Role of APC and DNA mismatch repair genes in the development of colorectal cancers. Mol. Cancer 2003, 2, 41. [Google Scholar] [CrossRef]
- Liu, C.Q.; Ma, Y.L.; Qin, Q.; Wang, P.H.; Luo, Y.; Xu, P.F.; Cui, Y. Epidemiology of esophageal cancer in 2020 and projections to 2030 and 2040. Thorac. Cancer 2023, 14, 3–11. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Then, E.O.; Lopez, M.; Saleem, S.; Gayam, V.; Sunkara, T.; Culliford, A.; Gaduputi, V. Esophageal Cancer: An Updated Surveillance Epidemiology and End Results Database Analysis. World J. Oncol. 2020, 11, 55–64. [Google Scholar] [CrossRef]
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of esophageal cancer: Update in global trends, etiology and risk factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, A.K.; El-Serag, H.B. Esophageal carcinoma. N. Engl. J. Med. 2014, 371, 2499–2509. [Google Scholar] [CrossRef] [PubMed]
- Abbas, G.; Krasna, M. Overview of esophageal cancer. Ann. Cardiothorac. Surg. 2017, 6, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.B.; Yang, Z.K.; Su, Y.H.; Cheng, Y.W. Carvacrol Induces Cell Apoptosis in Human Esophageal Squamous Carcinoma the Human Esophageal Squamous Carcinoma Cell Line (KYSE-150) Cells. J. Biomater. Tiss. Eng. 2021, 11, 1844–1847. [Google Scholar] [CrossRef]
- Morgan, E.; Arnold, M.; Camargo, M.C.; Gini, A.; Kunzmann, A.T.; Matsuda, T.; Meheus, F.; Verhoeven, R.H.A.; Vignat, J.; Laversanne, M.; et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020–2040: A population-based modelling study. E Clin. Med. 2022, 47, 101404. [Google Scholar] [CrossRef]
- Tsekrekos, A.; Okumura, Y.; Rouvelas, I.; Nilsson, M. Gastric Cancer Surgery: Balancing Oncological Efficacy against Postoperative Morbidity and Function Detriment. Cancers 2024, 16, 1741. [Google Scholar] [CrossRef]
- Gunes-Bayir, A.; Kiziltan, H.S.; Kocyigit, A.; Guler, E.M.; Karatas, E.; Toprak, A. Effects of natural phenolic compound carvacrol on the human gastric adenocarcinoma (AGS) cells in vitro. Anticancer. Drugs 2017, 28, 522–530. [Google Scholar] [CrossRef]
- Gunes-Bayir, A.; Kocyigit, A.; Guler, E.M.; Bilgin, M.G.; Ergun, I.S.; Dadak, A. Effects of carvacrol on human fibroblast (WS-1) and gastric adenocarcinoma (AGS) cells in vitro and on Wistar rats in vivo. Mol. Cell Biochem. 2018, 448, 237–249. [Google Scholar] [CrossRef]
- Gunes-Bayir, A.; Guler, E.M.; Bilgin, M.G.; Ergun, I.S.; Kocyigit, A.; Dadak, A. Anti-Inflammatory and Antioxidant Effects of Carvacrol on N-Methyl-N′-Nitro-N-Nitrosoguanidine (MNNG) Induced Gastric Carcinogenesis in Wistar Rats. Nutrients 2022, 14, 2848. [Google Scholar] [CrossRef]
- Ramai, D.; Smith, E.R.; Wang, Y.; Huang, Y.; Obaitan, I.; Chandan, S.; Dhindsa, B.; Papaefthymiou, A.; Morris, J.D. Epidemiology and Socioeconomic Impact of Pancreatic Cancer: An Analysis of the Global Burden of Disease Study 1990-2019. Dig. Dis. Sci. 2024, 69, 1135–1142. [Google Scholar] [CrossRef]
- Li, T.; Lin, C.; Wang, W. Global, regional, and national burden of pancreatic cancer from 1990 to 2021, its attributable risk factors, and projections to 2050: A systematic analysis of the global burden of disease study 2021. BMC Cancer 2025, 25, 189. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef]
- Zhao, Z.; Liu, W. Pancreatic Cancer: A Review of Risk Factors, Diagnosis, and Treatment. Technol. Cancer Res. Treat. 2020, 19, 1533033820962117. [Google Scholar] [CrossRef]
- Eroglu Gunes, C.; Secme, M.; Kurar, E.; Donmez, H. Apoptotic and Anti-Metastatic Effect of Carvacrol in PANC-1 Human Pancreatic Cancer Cells. Nat. Prod. Biotechnol. 2022, 2, 42–50. [Google Scholar]
- Tan, E.Y.; Danpanichkul, P.; Yong, J.N.; Yu, Z.; Tan, D.J.H.; Lim, W.H.; Koh, B.; Lim, R.Y.Z.; Tham, E.K.J.; Mitra, K.; et al. Liver cancer in 2021: Global burden of disease study. J. Hepatol. 2024, 82, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef]
- Lakkis, N.A.; Mokalled, N.M.; Osman, M.H.; Musharrafieh, U.M.; Eljammal, M. Liver Cancer and Risk Factors in the MENA Region: Epidemiology and Temporal Trends Based on the 2019 Global Burden of Disease Data. Cancer Control 2024, 31, 10732748241297346. [Google Scholar] [CrossRef]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491. [Google Scholar] [CrossRef]
- Jayakumar, S.; Madankumar, A.; Asokkumar, S.; Raghunandhakumar, S.; Gokula dhas, K.; Kamaraj, S.; Divya, M.G.J.; Devaki, T. Potential preventive effect of carvacrol against diethylnitrosamine-induced hepatocellular carcinoma in rats. Mol. Cell Biochem. 2012, 360, 51–60. [Google Scholar] [CrossRef]
- Yin, Q.H.; Yan, F.X.; Zu, X.Y.; Wu, Y.H.; Wu, X.P.; Liao, M.C.; Deng, S.W.; Yin, L.L.; Zhuang, Y.Z. Anti-proliferative and pro-apoptotic effect of carvacrol on human hepatocellular carcinoma cell line HepG-2. Cytotechnology 2012, 64, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Yousef, E.H.; Abo El-Magd, N.F.; El Gayar, A.M. Carvacrol enhances anti-tumor activity and mitigates cardiotoxicity of sorafenib in thioacetamide-induced hepatocellular carcinoma model through inhibiting TRPM7. Life Sci. 2023, 324, 121735. [Google Scholar] [CrossRef]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef] [PubMed]
- Papier, K.; Bradbury, K.E.; Balkwill, A.; Barnes, I.; Smith-Byrne, K.; Gunter, M.J.; Berndt, S.I.; Le Marchand, L.; Wu, A.H.; Peters, U.; et al. Diet-wide analyses for risk of colorectal cancer: Prospective study of 12,251 incident cases among 542,778 women in the UK. Nat. Commun. 2025, 16, 375. [Google Scholar] [CrossRef] [PubMed]
- Olfatifar, M.; Rafiei, F.; Sadeghi, A.; Ataei, E.; Habibi, M.A.; Pezeshgi Modarres, M.; Ghalavand, Z.; Houri, H. Assessing the Colorectal Cancer Landscape: A Comprehensive Exploration of Future Trends in 216 Countries and Territories from 2021 to 2040. J. Epidemiol. Glob. Health 2025, 15, 5. [Google Scholar] [CrossRef]
- Abed, A.T.; AlMudhafar, A.M.; Hadi, N.R. Anti-Cancer Study of Carvacrol in Hypoxic-Induced Colorectal Cancer Cell. J. Angiother. 2024, 8, 1–6. [Google Scholar] [CrossRef]
- Pakdemirli, A.; Karaca, C.; Sever, T.; Daşkin, E.; Leblebici, A.; Yiğitbaşi, T.; Başbinar, Y. Carvacrol alters soluble factors in HCT-116 and HT-29 cell lines. Turk. J. Med. Sci. 2020, 50, 271–276. [Google Scholar] [CrossRef]
- Arigesavan, K.; Sudhandiran, G. Carvacrol exhibits anti-oxidant and anti-inflammatory effects against 1, 2-dimethyl hydrazine plus dextran sodium sulfate induced inflammation associated carcinogenicity in the colon of Fischer 344 rats. Biochem. Biophys. Res. Commun. 2015, 461, 314–320. [Google Scholar] [CrossRef]
- Zotti, M.; Colaianna, M.; Morgese, M.G.; Tucci, P.; Schiavone, S.; Avato, P.; Trabace, L. Carvacrol: From Ancient Flavoring to Neuromodulatory Agent. Molecules 2013, 18, 6161–6172. [Google Scholar] [CrossRef]
- Burt, S. Essential oils: Their antibacterial properties and potential applications in foods—A review. Int. J. Food Microbiol. 2004, 94, 223–253. [Google Scholar] [CrossRef]
- Llana-Ruiz-Cabello, M.; Maisanaba, S.; Puerto, M.; Prieto, A.I.; Pichardo, S.; Moyano, R.; González-Pérez, J.A.; Cameán, A.M. Genotoxicity evaluation of carvacrol in rats using a combined micronucleus and comet assay. Food Chem. Toxicol. 2016, 98, 240–250. [Google Scholar] [CrossRef]
- Barnwal, P.; Vafa, A.; Afzal, S.M.; Shahid, A.; Hasan, S.K.; Alpashree; Sultana, S. Benzo(a)pyrene induces lung toxicity and inflammation in mice: Prevention by carvacrol. Hum. Exp. Toxicol. 2018, 37, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Bhardwaj, M.; Shukla, S.; Min, S.H.; Choi, D.K.; Bajpai, V.K.; Huh, Y.S.; Kang, S.C. Carvacrol inhibits cytochrome P450 and protects against binge alcohol-induced liver toxicity. Food Chem. Toxicol. 2019, 131, 110582. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Bhardwaj, M.; Shukla, S.; Lee, H.; Oh, M.H.; Bajpai, V.K.; Huh, Y.S.; Kang, S.C. Carvacrol encapsulated nanocarrier/ nanoemulsion abrogates angiogenesis by downregulating COX-2, VEGF and CD31 in vitro and in vivo in a lung adenocarcinoma model. Colloids Surf. B Biointerfaces 2019, 181, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Ghorani, V.; Alavinezhad, A.; Rajabi, O.; Mohammadpour, A.H.; Boskabady, M.H. Safety and tolerability of carvacrol in healthy subjects: A phase I clinical study. Drug Chem. Toxicol. 2021, 44, 177–189. [Google Scholar] [CrossRef]
- Baranauskaite, J.; Kubiliene, A.; Marksa, M.; Petrikaite, V.; Vitkevičius, K.; Baranauskas, A.; Bernatoniene, J. The Influence of Different Oregano Species on the Antioxidant Activity Determined Using HPLC Postcolumn DPPH Method and Anticancer Activity of Carvacrol and Rosmarinic Acid. Biomed. Res. Int. 2017, 2017, 1681392. [Google Scholar] [CrossRef]
- Bouhtit, F.; Najar, M.; Moussa Agha, D.; Melki, R.; Najimi, M.; Sadki, K.; Boukhatem, N.; Bron, D.; Meuleman, N.; Hamal, A.; et al. New Anti-Leukemic Effect of Carvacrol and Thymol Combination through Synergistic Induction of Different Cell Death Pathways. Molecules 2021, 26, 410. [Google Scholar] [CrossRef]
- Stojanović, N.M.; Stevanović, M.; Randjelović, P.; Mitić, K.; Petrović, V.; Sokolović, D.; Mladenović, B.; Lalić, J.; Radulović, N.S. Low dose of carvacrol prevents rat pancreas tissue damage after L-arginine application, while higher doses cause pancreatic tissue impairment. Food Chem. Toxicol. 2019, 128, 280–285. [Google Scholar] [CrossRef]
- Keawchaoon, L.; Yoksan, R. Preparation, characterization and in vitro release study of carvacrol-loaded chitosan nanoparticles. Colloids Surf. B Biointerfaces 2011, 84, 163–171. [Google Scholar] [CrossRef]
- Khan, I.; Bahuguna, A.; Kumar, P.; Bajpai, V.K.; Kang, S.C. In vitro and in vivo antitumor potential of carvacrol nanoemulsion against human lung adenocarcinoma A549 cells via mitochondrial mediated apoptosis. Sci. Rep. 2018, 8, 144. [Google Scholar] [CrossRef]
- Yadav, R.; Chawra, H.S.; Dubey, G.; Alam, M.S.; Kumar, V.; Sharma, P.; Upadhayay, N.K.; Yadav, T. Herbal based nanoparticles as a possible and potential treatment of cancer: A review. Explor. Target. Antitumor Ther. 2025, 6, 1002285. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.L.d.; Dantas, A.G.B.; Melo, C.d.O.; Felício, I.M.; Oliveira, E.E. Nanotechnology as a tool to improve the biological activity of carvacrol: A review. J. Drug Deliv. Sci. Technol. 2022, 76, 103834. [Google Scholar] [CrossRef]
- Akhlaq, A.; Ashraf, M.; Omer, M.O.; Altaf, I. Carvacrol-Fabricated Chitosan Nanoparticle Synergistic Potential with Topoisomerase Inhibitors on Breast and Cervical Cancer Cells. ACS Omega 2023, 8, 31826–31838. [Google Scholar] [CrossRef] [PubMed]
- Maryam, K.; Shakeri, S.; Kiani, K. Preparation and in vitro investigation of antigastric cancer activities of carvacrol-loaded human serum albumin nanoparticles. IET Nanobiotechnology 2015, 9, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.; Mohideen, A.P.; Seshadri, V.D.; Rengarajan, T. Biosynthesized tin oxide-sodium alginate-polyethylene glycol-carvacrol nanocomposite shows anticancer activity on esophagus squamous carcinoma cells. Process Biochem. 2022, 121, 403–412. [Google Scholar] [CrossRef]
- Taibi, M.; Elbouzidi, A.; Haddou, M.; Baraich, A.; Ou-Yahia, D.; Bellaouchi, R.; Mothana, R.A.; Al-Yousef, H.M.; Asehraou, A.; Addi, M.; et al. Evaluation of the Interaction between Carvacrol and Thymol, Major Compounds of Ptychotis verticillata Essential Oil: Antioxidant, Anti-Inflammatory and Anticancer Activities against Breast Cancer Lines. Life 2024, 14, 1037. [Google Scholar] [CrossRef]
- Azimi, S.; Esmaeil Lashgarian, H.; Ghorbanzadeh, V.; Moradipour, A.; Pirzeh, L.; Dariushnejad, H. 5-FU and the dietary flavonoid carvacrol: A synergistic combination that induces apoptosis in MCF-7 breast cancer cells. Med. Oncol. 2022, 39, 253. [Google Scholar] [CrossRef]

{kind=link}
| Serial number | Type of Cancer | Biological Model | Physiological Effects | Mechanism of Action | References |
|---|---|---|---|---|---|
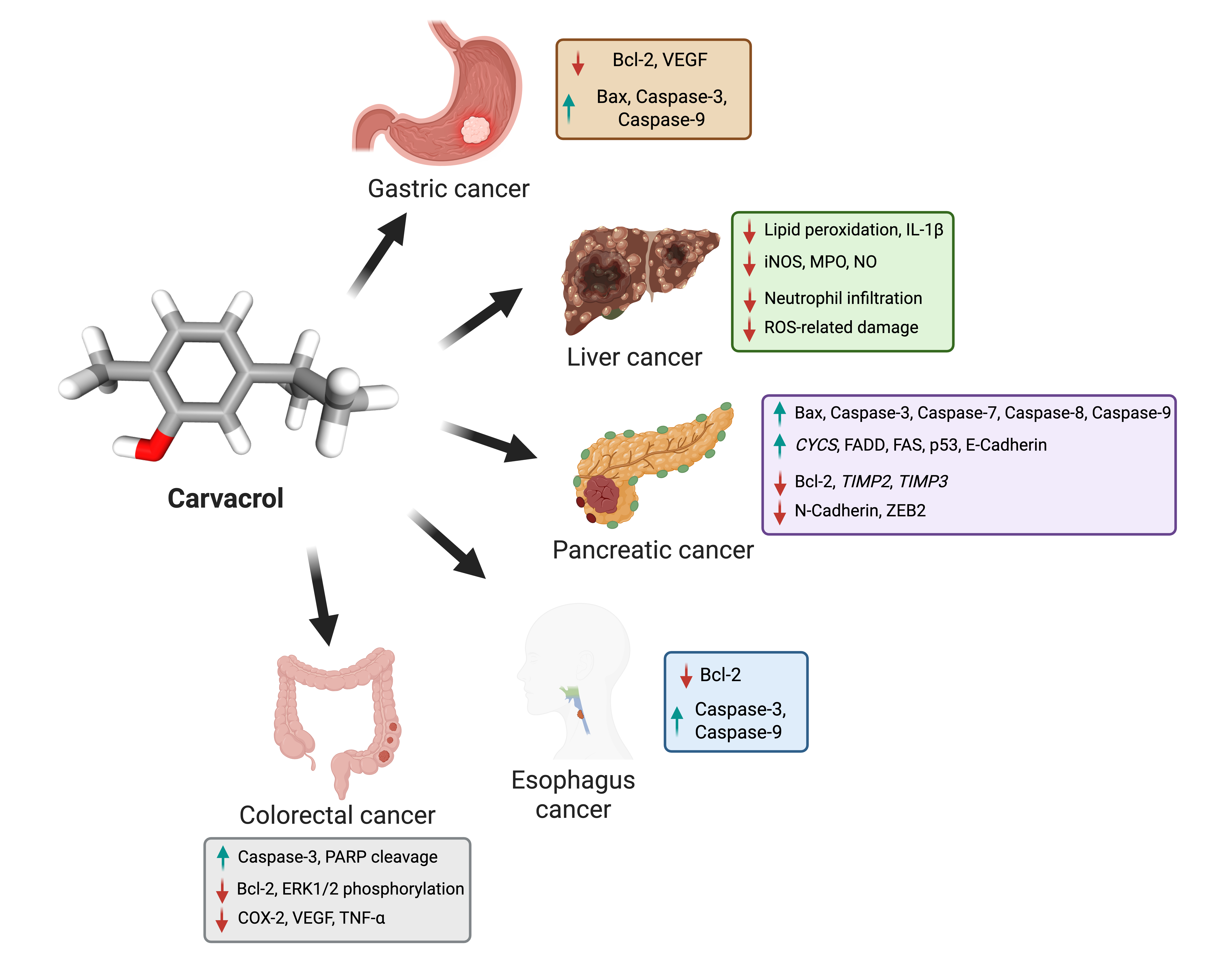
| 1 | Esophageal cancer | KYSE-150 | Inhibits cell proliferation and induces cell apoptosis. | ↑ caspase-3 and caspase-9 and ↓ Bcl-2 | [54] |
| 2 | Gastric cancer | AGS | Inhibits cell proliferation-induced DNA damage, apoptosis, and ROS generation. | ↓ Bcl-2 and ↑ Bax, caspase-9, and caspase-3 | [58] |
| 3 | Pancreatic cancer | PANC-1 cells | Triggers apoptosis while demonstrating anti-proliferative and anti-migratory properties. | ↑ epithelial markers like E-Cadherin, TIMP2, TIMP3, Bax, caspase-3, caspase-7, caspase-8, caspase-9, cytochrome c, FADD, FAS, and p53 ↓ mesenchymal markers like N-Cadherin, ZEB2, and Bcl-2 | [65] |
| PANC-1 cells | Inhibits proliferation, induces apoptosis, and suppresses metastasis. | Inhibit Atg16L1 and Beclin-1 | |||
| 4 | Liver cancer | HepG2 | Hepatoprotection, inducing apoptosis and inhibiting tumor proliferation. | ↓ lipid peroxidation, restoring key liver enzymes (AST, ALT, ALP, LDH, cGT) and ↑ SOD, CAT, GPx, GR, GSH | [70] |
| HepG2 | Causes apoptosis. | ↑ caspase-3, promoting PARP cleavage, ↓ Bcl-2, and modulating the MAPK signaling pathway ↓ ERK1/2 phosphorylation while activating p38 | [71] | ||
| 5 | Colorectal cancer | SW480 cells | Anti-proliferative and inhibiting angiogenesis. | ↓ TGF-α and ↑ anti-growth factors VE | [77] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patwa, N.; Singh, G.; Sharma, V.; Chaudhary, P.; Sharma, B.; Haque, S.; Yadav, V.; Satapathy, S.R.; Tuli, H.S. Targeting Gastrointestinal Cancers with Carvacrol: Mechanistic Insights and Therapeutic Potential. Biomolecules 2025, 15, 777. https://doi.org/10.3390/biom15060777
Patwa N, Singh G, Sharma V, Chaudhary P, Sharma B, Haque S, Yadav V, Satapathy SR, Tuli HS. Targeting Gastrointestinal Cancers with Carvacrol: Mechanistic Insights and Therapeutic Potential. Biomolecules. 2025; 15(6):777. https://doi.org/10.3390/biom15060777
Chicago/Turabian StylePatwa, Nitika, Gagandeep Singh, Vikas Sharma, Priyanka Chaudhary, Bunty Sharma, Shafiul Haque, Vikas Yadav, Shakti Ranjan Satapathy, and Hardeep Singh Tuli. 2025. "Targeting Gastrointestinal Cancers with Carvacrol: Mechanistic Insights and Therapeutic Potential" Biomolecules 15, no. 6: 777. https://doi.org/10.3390/biom15060777
APA StylePatwa, N., Singh, G., Sharma, V., Chaudhary, P., Sharma, B., Haque, S., Yadav, V., Satapathy, S. R., & Tuli, H. S. (2025). Targeting Gastrointestinal Cancers with Carvacrol: Mechanistic Insights and Therapeutic Potential. Biomolecules, 15(6), 777. https://doi.org/10.3390/biom15060777