4. Discussion and Conclusions
The search for new diagnostic and therapeutic methods in CD is very important because this chronic and incurable gastrointestinal disease characterized by alternating periods of exacerbation and remission mainly affects young people. In this group of patients, absorption disorders often occur and lead to weight loss. In addition, patients with active disease often limit their food intake due to abdominal pain, nausea and discomfort after the consumption of certain products, which leads to an insufficient supply of iron and malnutrition. Similarly, our patients were mainly young subjects who significantly differed in age and weight from the controls.
Cytokines play a crucial role in the pathogenesis, diagnosis and prevention of Crohn’s disease (CD) [
10,
11,
12,
13,
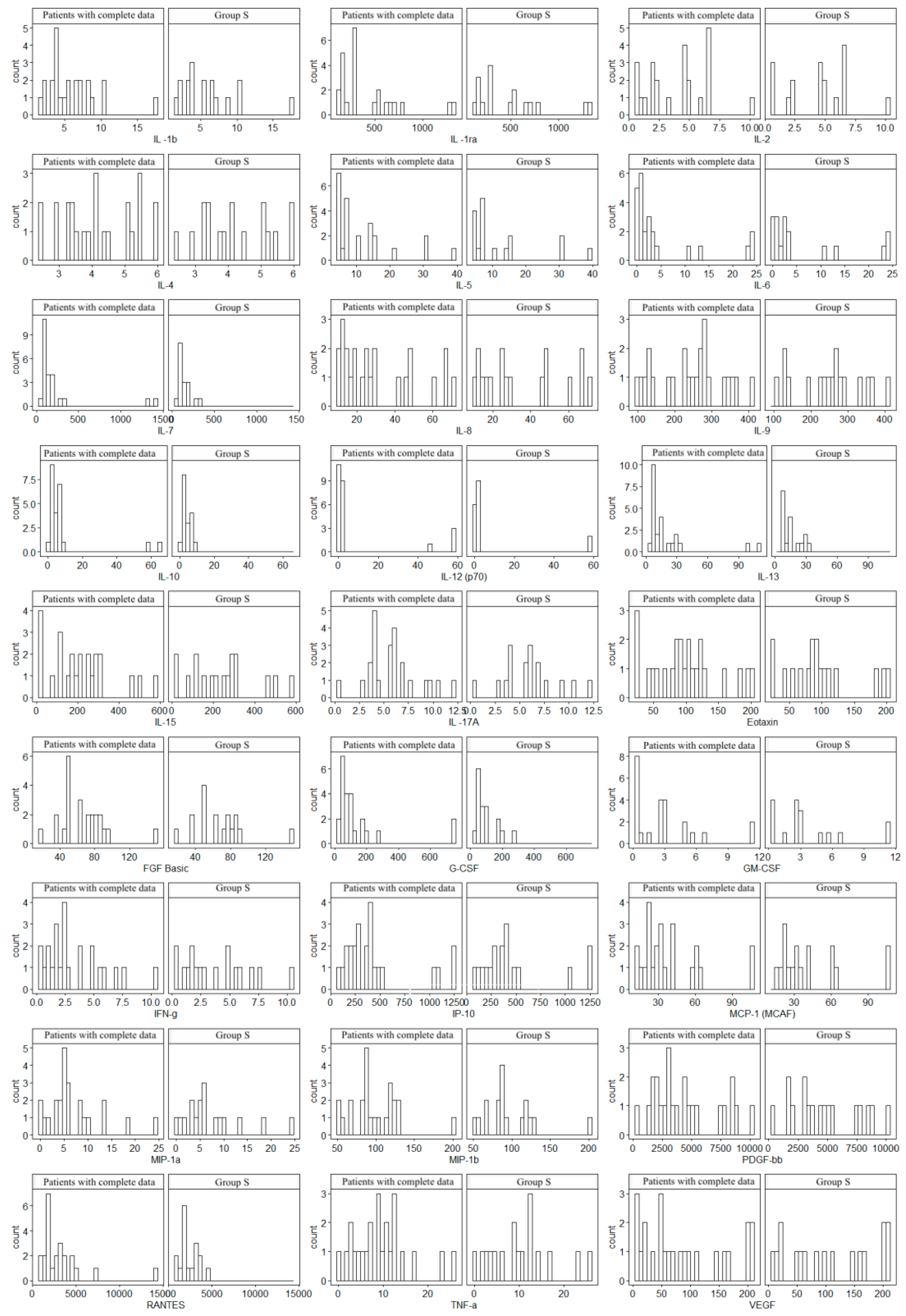
14]. Numerous authors and researchers have extensively discussed the role of cytokines in Crohn’s disease. These studies emphasize primarily the importance of cytokines such as TNF-α, IL-6, IL-10, IL-12, IL-17 and IL-23 in the disease’s pathogenesis, particularly their roles in promoting or regulating inflammation. In our study, we included the analysis of variability in the concentrations of 28 cytokines–IL-1β, IL-1RA, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12 (p70), IL-13, IL-15, IL-17A, eotaxin, FGF-basic, G-CSF, GM-CSF, IFN-γ, IP-10, MCP-1 (MCAF), MIP-1α, MIP-1β, PDGF-BB, RANTES, TNF-α and VEGF in correlations with radiological parameters assessed by magnetic resonance enterography (MRE), fecal calprotectin (FCAL) levels and clinical evaluation according to the Crohn’s Disease Activity Index (CDAI). There are no similar studies in the available literature.
It has long been known that the imbalance between pro-inflammatory cytokines is responsible for disorders of intestinal immune mechanisms in IBD [(IL-1(IL-1α, IL-1β), IL-2, IL-6, IL-8, IL-12, IL -17, IL-23, TNF-α, IFN-γ)] and anti-inflammatory cytokines (IL-4, IL-10, IL-11, IL-13). Additionally, particular interest has been aroused by the specific type of response in CD and UC, which determines the cytokine profile in the pathogenesis of these diseases. It has been proven that the cellular response dominates in CD, hence the main cytokines responsible for the development of the inflammatory reaction are those released by activated effector lymphocytes (Th1 and Th17 subpopulations). Th1 lymphocytes produce mainly IL-2, IFN-γ and TNF-α, while Th17 lymphocytes mainly produce IL-17 and IL-22. It is also known that there is an imbalance between the above-mentioned cytokines produced by effector T lymphocytes (activated subpopulations of Th1 and Th17 lymphocytes) and cytokines produced by Treg (regulatory) lymphocytes, i.e., IL-10 and TGF, which are responsible for inhibiting excessive inflammatory response. In UC, however, there is an increased expression of a subpopulation of Th2 lymphocytes, which results in the activation of NKT cells (a subpopulation of lymphocytes that have the characteristics of both lymphocytes and NK cells), resulting in the production mainly of IL-5 and IL-13 [
16].
Martinez-Fiero et al. [
17] analysed the 27 protein profiles of serum from 53 participants (23 UC, 11 CD, and 19 controls) according to pharmacologic therapy and laboratory and clinical findings in IBD. In this work, elevated serum levels of G-CSF, IL-1Ra and PDGF-BB were associated with IBD endoscopic activity. PDGF-BB also correlated with serum levels of IL-4, IL-8, IL-15 and IL-17, reflecting the diversity of molecular pathways that operate in parallel in IBD and the complexity of interactions between them. Also, their result showed that, compared with controls serum IL-15, eotaxin, MCP-1 and PDGF-BB levels were higher in CD but not in UC patients, which is partially consistent with our research, where significantly higher concentrations of eotaxin, MCP-1, PDGF-BB among others: IFN-γ, IP-10, MIP-1β, RANTES, TNF-α and VEGF in Group S were reported compared to Group C. Interestingly, in our study, serum IL-15 was not significantly higher in Group S than in Group C, but actually, except for IL-5, IL-12 and IL-15, the levels of most cytokines and soluble receptor antagonist (IL-1RA) were significantly higher in Group S than in Group C.
Acute phase protein (CRP) and FCAL are commonly used markers of inflammation in CD, which allows the monitoring of the disease course and response to treatment. CRP is produced in the liver in response to inflammation induced by IL-1, IL-6 and TNF-α. A highly significant positive correlation was observed between IFN-γ and CRP, and FCAL levels (
p < 0.01). Moreover, FCAL levels showed a significant positive correlation with Th1- and Th17-associated cytokines (IL-6, TNF-β, SAA and IL-17A) [
18]. Despite certain limitations (lack of specificity), it is useful in assessing disease activity. In correlation with other markers, it allows the course of CD and response to treatment to be monitored. Fecal calprotectin, on the other hand, is a protein formed in the liver with the participation of cytokines, whose blood concentration changes as a result of response to inflammation. Fecal calprotectin is commonly used as a biomarker in CD and in differentiating CD from irritable bowel syndrome (IBS), which has a different pathogenesis despite similar symptoms. It has been proven that increasing FCAL levels in routine tests predicts disease progression regardless of the presence of symptoms and location of CD. Stable normal FCAL levels are also considered a positive prognostic marker for maintaining clinical remission. Other studies have suggested that FCAL levels may be a non-invasive marker of mucosal healing. Research is conducted on other biomarkers that can potentially be used in clinical decision-making [
7,
19,
20,
21,
22]. Recent advances have also demonstrated that the combination of MRE with calprotectin has improved the diagnostic accuracy and monitoring of CD. According to Jones and colleagues [
23], Fecal calprotectin correlates well with the MRE assessment of ileal CD, and MRE parameters are associated with long-term biologic- and surgery-free remission. Other authors [
24,
25] suggest that inflammation detected by MRE is often associated with low endoscopic healing index and FCAL in similar proportions.
In recent years, cytokines have been considered promising biomarkers since long-term follow-ups have shown that this group of proteins plays a vital role in the pathogenesis of CD, particularly with regard to the disproportion between pro-inflammatory and anti-inflammatory cytokines [
7,
19,
26,
27,
28]. The assessment of their concentrations can be useful for establishing an appropriate diagnosis and assessing the severity of disease activity. Additionally, it can be a potential prognostic tool for predicting the course of the disease and facilitating the development of new therapeutic methods, including biological treatment [
29,
30,
31]. According to the literature, it is clinically more useful to determine several biomarkers at the same time, and their combined assessment can be an effective tool for monitoring patients. It might replace invasive testing in the future or reduce the number of tests. Among the promising cytokines, interleukin 6 (IL-6) is crucial. It has a pro-inflammatory activity. Many authors, such as Nikolaus et al. [
31], found elevated serum levels of IL-6 in patients with active CD. Similarly, in the group of our patients, the concentrations of IL-6 were significantly higher compared to the controls. There are also reports that the assessment of IL-6 can be used as a biomarker in predicting response to biological therapy, although study results are inconclusive [
28,
32]. However, this is an interesting point for further research since IL-6 has been the focus of attention for many years (the possibility of targeted anti-IL-6 therapy in patients with severe CD) [
33]. Cytokine regulatory networks have important implications for the development and progression of the disease [
31], which is demonstrated by the failure of IL-10 in treating CD. Initially, IL-10 supplementation had beneficial effects in mouse models, and clinical trials showed that recombinant IL-10 was safe and well tolerated in humans. Unfortunately, the effect of clinical trials in humans was disappointing. Based on current research, IL-10 supplementation cannot be a universal treatment method in CD, but it can provide the expected effect in a well-selected small group of patients [
34]. In our subjects, the levels of IL-10 were significantly higher compared to the control group, which shows how important it is to determine the concentration of cytokines because, in these patients, IL-10 supplementation would certainly not be beneficial and could even exacerbate the already ongoing inflammation.
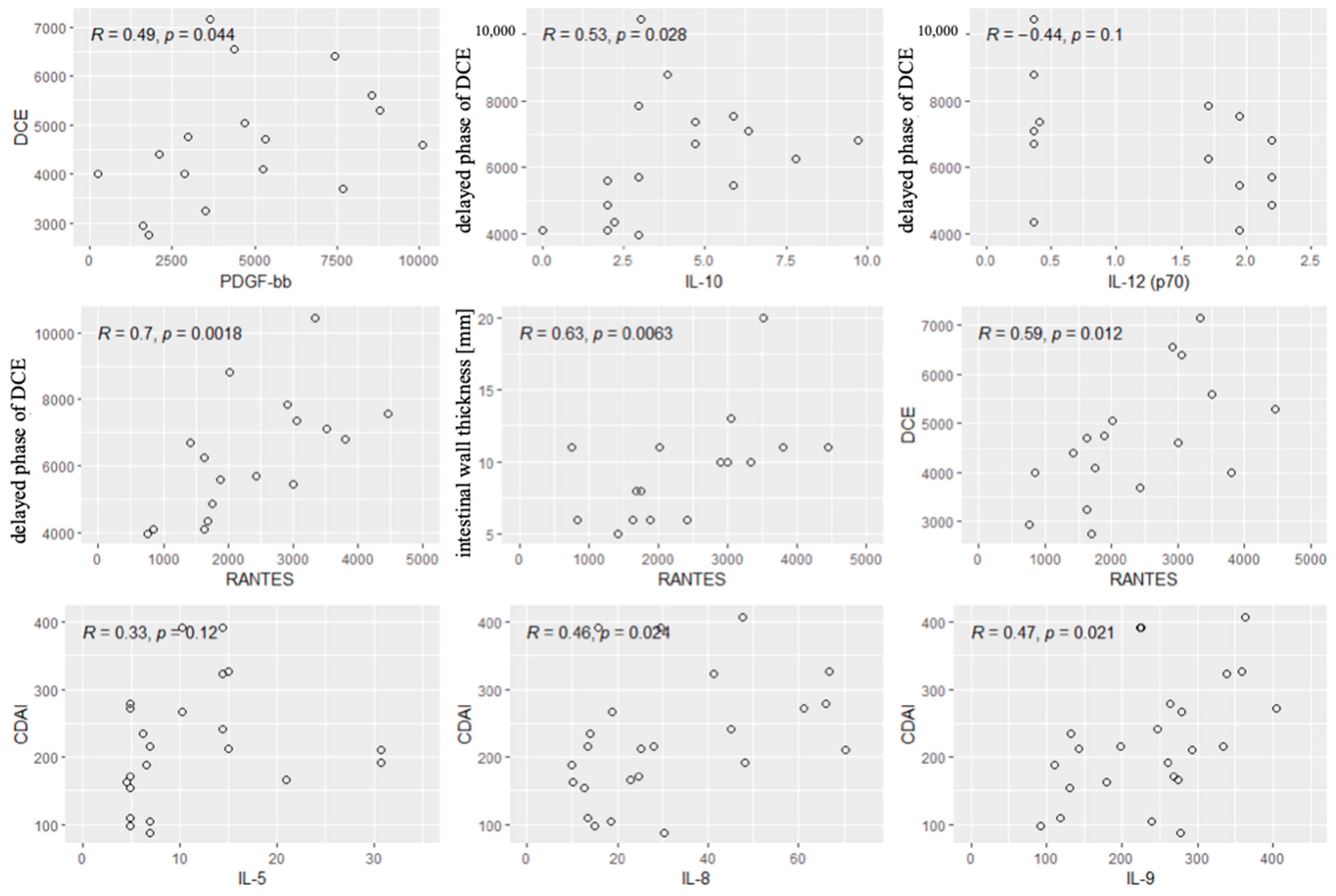
Another interesting biomarker is RANTES, a chemokine synthesized by T lymphocytes, which has a pro-inflammatory effect. Ansari et al. [
35] found that the concentrations of RANTES were elevated in CD. However, significantly higher levels of RANTES were noted in ulcerative colitis (UC) compared to CD. Therefore, it seems important to consider the concentration of RANTES in differential diagnosis (UC vs. CD) and when inflammatory changes in the intestinal wall are suspected. This study showed correlations between RANTES and MRE parameters indicative of inflammation in the intestinal wall, such as wall thickening and contrast enhancement on DCE. A similar correlation was found between platelet-derived growth factor (PDGF) and the enhancement of the intestinal wall on DCE, which is in line with the literature data related to increased PDGF levels in patients with active CD [
36]. These correlations indicate that it is worth considering the assessment of PDGF and RANTES levels in a group of patients with suspected inflammatory bowel changes. The concentration of RANTES seems crucial in correlation with the contrast enhancement of the intestinal wall and its thickness. As we know, the clinical severity of the disease does not always correlate with the symptoms reported by patients and the CDAI. It may be useful to determine disease activity using other non-invasive markers that can precede the clinical manifestation of the disease and the symptoms reported by patients. Currently, scientists are focusing on defining the goal of therapy and then striving to achieve it in accordance with the “treat to target” strategy. This treatment method aims to reduce the activity and inhibit the progression of the disease based on the assessment of the activity of the inflammatory process (including through the assessment of biomarkers and endoscopic examinations), and not on the basis of the symptoms. This strategy involves regularly assessing disease activity and then adapting and modifying therapy to achieve the intended clinical effect. Thus, cytokines, such as RANTES and PDGF-BB, can support the radiological monitoring of CD, allowing for a more comprehensive assessment of patients. Confirmation comes from the latest research by Fang et al. [
37] which indicates that PDGF-BB levels in mucosal tissue may be independent risk factors for active IBD. Moreover, PDGF-BB levels were positively correlated with M1 macrophage markers.
Nevertheless, long-term research is still needed to determine the most appropriate goals of selected therapeutic strategies and their final effects [
30].
The literature shows the correlations of individual biomarkers with disease activity measured using the CDAI. To date, there has not been sufficiently strong evidence that the determination of the level of a single interleukin could be a sufficient tool to assess CD activity. However, determining several biomarkers is more clinically useful and reliable, and their combined assessment can be an effective tool for monitoring patients. Bourgonje et al. [
32] proved that the combined assessment of four biomarkers (serum amyloid A, IL-6, IL-8 and eotaxin 1) reliably predicted disease activity in correlation with endoscopic assessment. In another study, Słowińska-Solnica et al. [
38] showed that the combined assessment of biomarkers offered better results in the diagnosis of CD than each of these markers alone. The best results were obtained by assessing IL-23, CRP, IL-6 and IL-17 together. Also, more accurate results were obtained for the combined assessment of IL-6 and CRP than for each biomarker separately. In addition, there have been some findings that the concentration of IL-6 correlated well with the CDAI, and its concentration could predict a clinical response during biological therapy [
28,
39]. Surprisingly, no correlation was found between the CDAI and IL-6 levels in the study group. However, correlations were reported between IL5, IL-8 and IL-9 levels and the CDAI, which could contribute to a broader use of these interleukins to monitor patients with CD. IL-5 is a chemotactic agent for the survival and activation of eosinophils, which play a role in mucosal immunity [
35]. During active inflammation, eosinophils increase IL-4, IL-5 and IL-13 expression, indicating a shift to the Th2 response. In response to IL-5, eosinophils are released into the peripheral circulation, after which they can migrate to the gastrointestinal tract after the binding of chemoattractant molecules:CCL11, eotaxin1, CCL24–eotaxin2, CCL26 -eotaxin3, CCL5-regulated upon activation, normal T cell expressed and secreted (RANTES), CCL7–MCP-3 and CCL13 (MCP-4) [
40]. Eotaxines are chemokines that bind to eosinophils’ surface receptor CCR3, resulting in eosinophil migration and homing in the lamina propria of the bowel mucosa [
41]. In some cases of Crohn’s disease, eosinophil infiltration is observed, particularly during inflammation or in areas of active disease. Eosinophils in surgical specimens of resected ileum of CD patients have been linked to an increased risk of early recurrence, while peripheral blood eosinophilia has been shown to predict clinically active disease in pediatric CD patients and has been associated with increased disease severity [
42,
43].
In the case of IL-8, next to the demonstrated correlation with the CDAI, an additional advantage is its high accuracy in differentiating patients with IBD from IBS. IL-8 (also known as CXCL8) is a pro-inflammatory chemokine primarily involved in the recruitment and activation of neutrophils. The synthesis of IL-8 is strongly stimulated by IL1-β, TNF-α, and bacterial lipopolysaccharides (LPS) [
44]. It plays a significant role in the innate immune response and is produced by various cells, including macrophages, epithelial cells and endothelial cells. IL-8 is a potent chemoattractant for neutrophils, which are a hallmark of acute inflammation in Crohn’s disease. Studies have shown that IL-8 levels are elevated in the serum, stool and mucosal tissues of patients with active Crohn’s disease. IL-8 is thought to perpetuate the inflammatory cycle by recruiting more neutrophils and enhancing the release of reactive oxygen species (ROS) and proteolytic enzymes [
45].
IL-9 is a cytokine primarily associated with the Th9 subset of T-helper cells. It has pleiotropic effects, influencing mast cells, eosinophils and epithelial cells, and is involved in allergic responses and mucosal immunity [
46]. IL-9 levels are elevated in the intestinal tissues of patients with Crohn’s disease. It promotes the production of other pro-inflammatory cytokines (e.g., TNF-α, IL-6) and chemokines that amplify the inflammatory response. By activating mast cells and fibroblasts, IL-9 contributes to extracellular matrix remodeling and fibrotic changes [
47]. IL-5, IL-8 and IL-9 contribute to Crohn’s disease through distinct yet interconnected pathways involving immune cell recruitment, barrier dysfunction and chronic inflammation. Their roles vary across disease stages and phenotypes, with potential synergies in amplifying inflammation and fibrosis. Understanding these relationships could guide more targeted therapeutic strategies [
47].
Scaioli et al. [
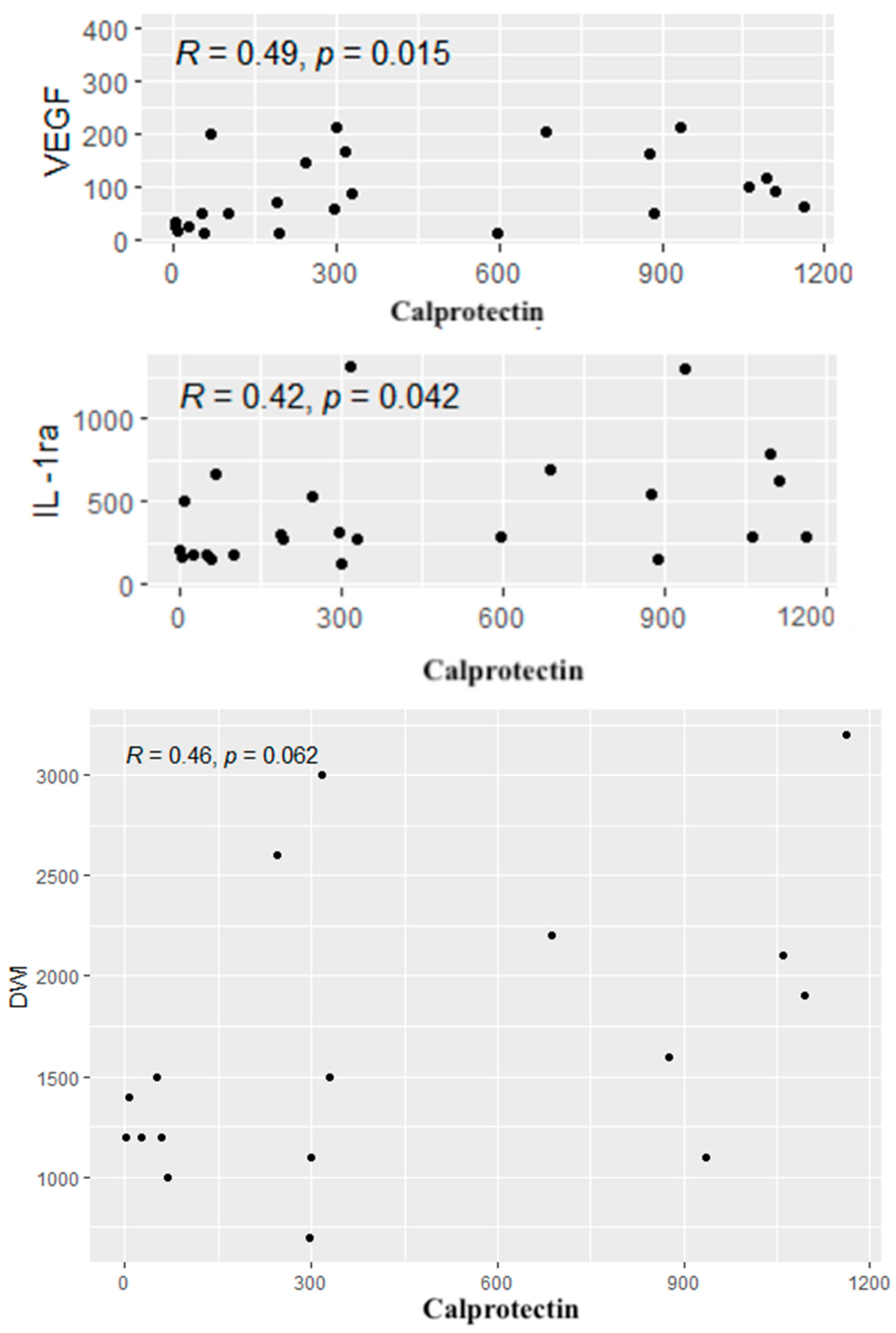
47] focused on the correlation between the calprotectin concentration in the stool with the CDAI. Their study showed that patients with a CDAI value from 100 to 150 had an increased probability of increased fecal calprotectin levels and asymptomatic mucosal inflammation. Their study also found that asymptomatic patients with a CDAI = 120 had a 60% chance of having endoscopically/histologically evident active disease. Therefore, the authors of the study showed that it could be useful to analyze a group of patients with a CDAI value ranging from 100 to 150. Our study showed positive correlations of calprotectin levels with selected cytokine concentrations (IL-1RA, VEGF), which confirms the importance of calprotectin as a biomarker of inflammation in CD. However, we found no correlation between calprotectin concentrations and the CDAI. IL-1RA is an IL-1R receptor antagonist mainly produced together with IL-1 to prevent overstimulation and inflammatory response. The correlation we demonstrated suggests that it is worth considering the assessment of IL-1RA in CD, although the IL-1RA/IL-1 ratio is probably a more reliable factor. Casini Raggi et al. [
48] suggested that the impaired imbalance between Il-1RA and IL-1 could indicate a disturbance in homeostasis and the ratio was strongly correlated with disease severity. This finding is significant since it has also been previously reported that the concentration of IL-1RA needed to be about 100 times higher compared to IL-1 to effectively inhibit IL-1 signaling [
49,
50]. In our opinion, it was essential to demonstrate a correlation between the growth factor involved in the formation of the blood vessel network, such as VEGF, and the concentration of calprotectin. VEGF is a protein considered to be the most potent factor promoting angiogenesis. One paper showed that serum VEGF levels correlated well with the clinical picture of patients and the parameter could also be used to predict response to anti-TNF-α therapy. Eder et al. (2015) [
51] suggested that VEGF could be an additional marker of CD activity and the assessment of its concentration in blood serum could be useful in optimizing the treatment with anti-TNF-α and in selecting patients who could benefit from this therapy. Therefore, our demonstration of the correlation between VEGF and fecal calprotectin levels is further evidence of the possible use of this growth factor as a biomarker in CD. When monitoring patients with CD, attention should be paid to the course of the disease, its activity and endoscopic surveillance since the long-term course of the disease increases the risk of carcinogenesis, and patients with IBD are also affected with colorectal cancer, usually at a younger age than the general population [
52]. It is believed that chronic inflammation in the intestinal wall is one of the crucial factors in the pathogenesis of colorectal cancer and adenocarcinoma of the small intestine. It has been proven that the ongoing inflammatory process and the imbalance between the initiation and inhibition of the inflammatory response affected neoplastic transformation, cell proliferation, angiogenesis and metastasis. It is also believed that many of the interleukins associated with CD, including IFN-γ, IL-1, IL-2, IL-6, IL-8 and IL-17, play an essential role in carcinogenesis [
53,
54,
55,
56]. Further research is warranted on the mechanism of action of individual cytokines and their importance in CD since they allow the improvement of existing therapies and the creation of new ways for regulating cytokine pathways that emerge during clinical trials. It is important to search for new diagnostic methods and specific markers that could speed up the diagnosis of this group of patients, contribute to a quick accurate diagnosis, facilitate therapeutic decisions and could also be a prognostic factor for the further course of the disease. The search continues for methods of patient monitoring, which would be characterized by non-invasiveness and would allow for frequent follow-ups. Examinations should be extended to include the dynamic assessment of the cytokine networks during the disease’s course. It is also essential to observe how patients react to a specific therapy, which may make it easier to select patients for each treatment. Such a personalized medicine approach tailored individually to the patient’s needs seems to have the best chance of achieving the intended long-term goals and the expected clinical results [
30].
Limitations of the Study
The present study has some limitations. Firstly, the number of CD patients is relatively low; from this perspective, the results should be intended as exploratory in this specific cohort. Lastly, the results provide preliminary insight into the utility of using selected inflammatory markers in correlation with MRE for Crohn’s diseases diagnosis. A larger cohort would be necessary to confirm these findings and to assess the broader applicability of MRE across diverse patient subgroups. We are actively planning to increase the study group in future research to include a larger and more diverse population. This expansion could improve the generalizability of our findings and perhaps tailor a personalized treatment strategy.
5. Conclusions
The analysis of inflammatory marker concentrations and their correlations with radiological parameters in patients with CD indicates the following:
1. The determination of cytokine concentrations, such as IL-1β, IL-2, IL-4, IL-6, IL-7, IL-8, IL-9, IL-10, IL-13, IL-17, eotaxin, IFN-γ, IP-10, MCP-1, MIP-1β, PDGF-BB, RANTES, TNF-α VEGF and IL-1RA, can be a valuable tool in the diagnosis and assessment of CD activity. These markers can help diagnose the disease and monitor its course.
2. The concentrations of PDGF-BB, RANTES, IL-10 and IL-12 showed correlations with radiological parameters assessed by MRE, which characterize active inflammation. These cytokines have a particular potential as markers for the assessment of CD activity.
3. MRE parameter values showed no significant correlation with fecal calprotectin levels or disease severity as assessed by the CDAI. None of these indicators can be used as a single indicator of CD activity.
Research on the mechanisms of cytokine action in CD may lead to finding more effective treatment methods and contribute to faster diagnosis. The combined assessment of many inflammatory markers, including cytokines, with imaging results, may be more effective in assessing disease activity. This can lead to the development of more precise diagnostic tools that may potentially reduce the need for invasive examinations.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}