


Temporal Dynamic Alterations of Regional Homogeneity in Parkinson’s Disease: A Resting-State fMRI Study
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. MRI Data Acquisition
2.3. Rs-fMRI Data Preprocessing
2.4. ReHo Calculation
2.5. DReHo Calculation
2.6. Support Vector Machine Analysis
2.7. Statistical Analysis
3. Results
3.1. Clinical and Demographic Characteristics
3.2. Difference in ReHo between PD Patients and Controls
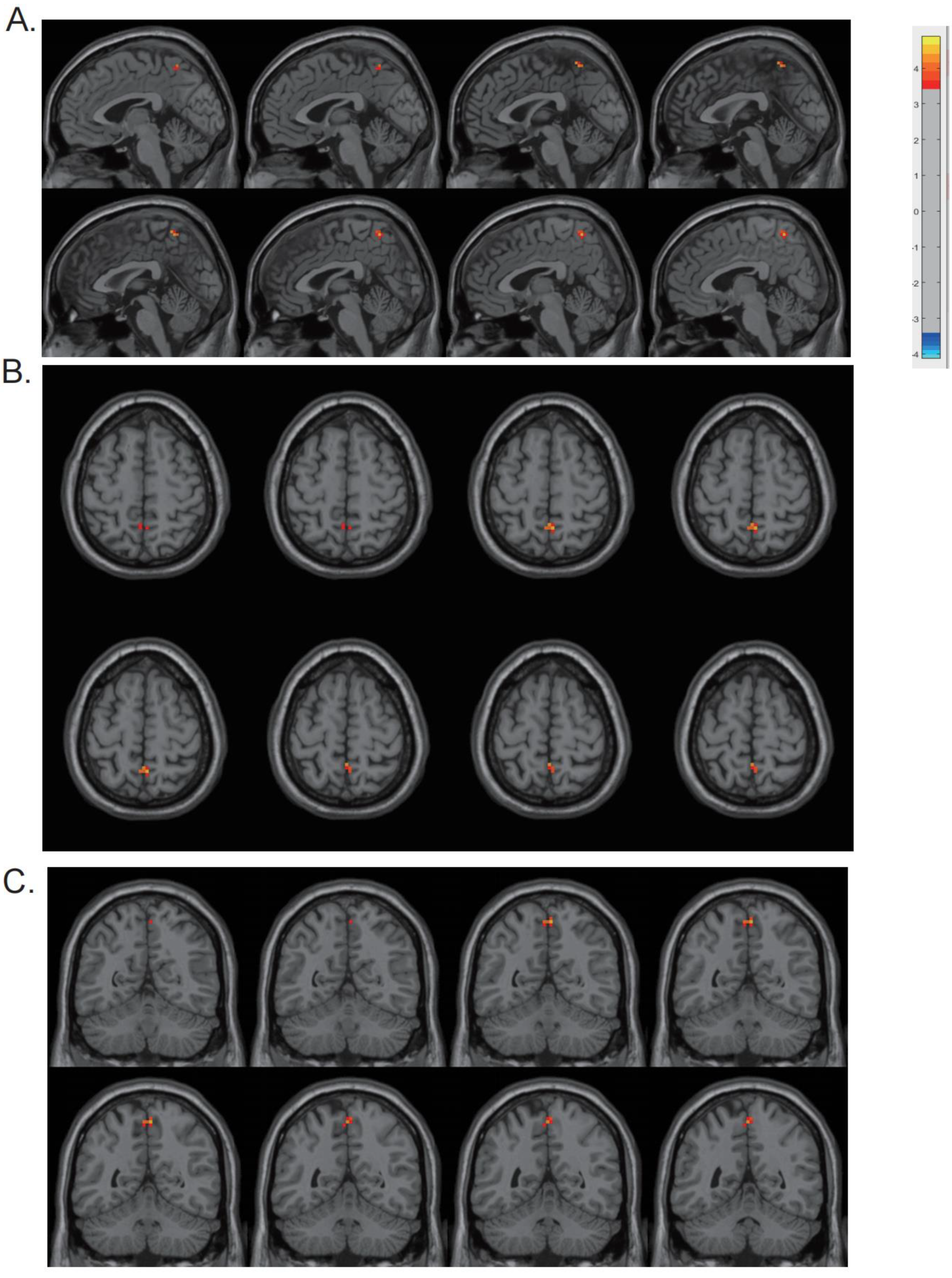
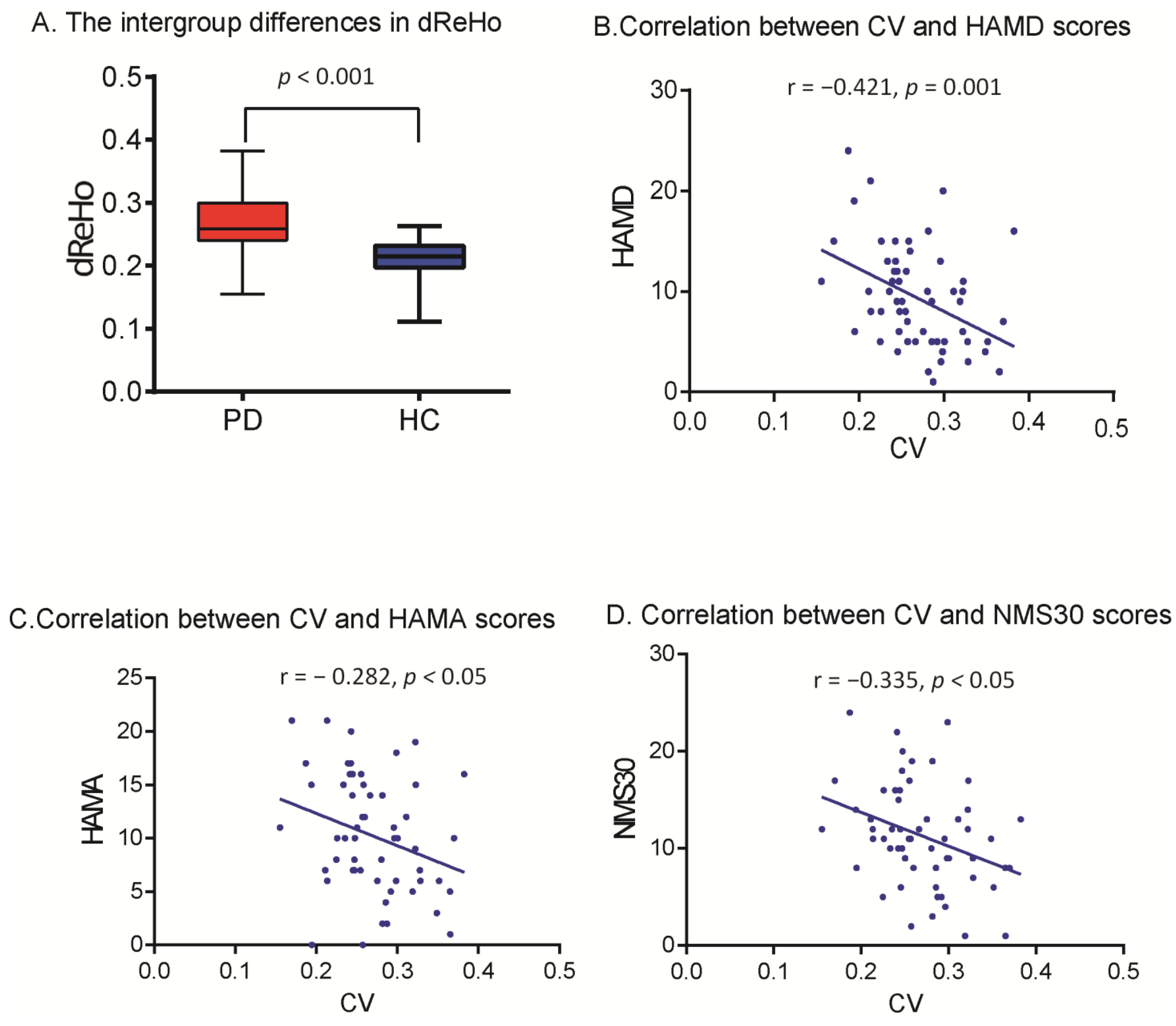
3.3. DReHo Analysis and Correlation Analysis
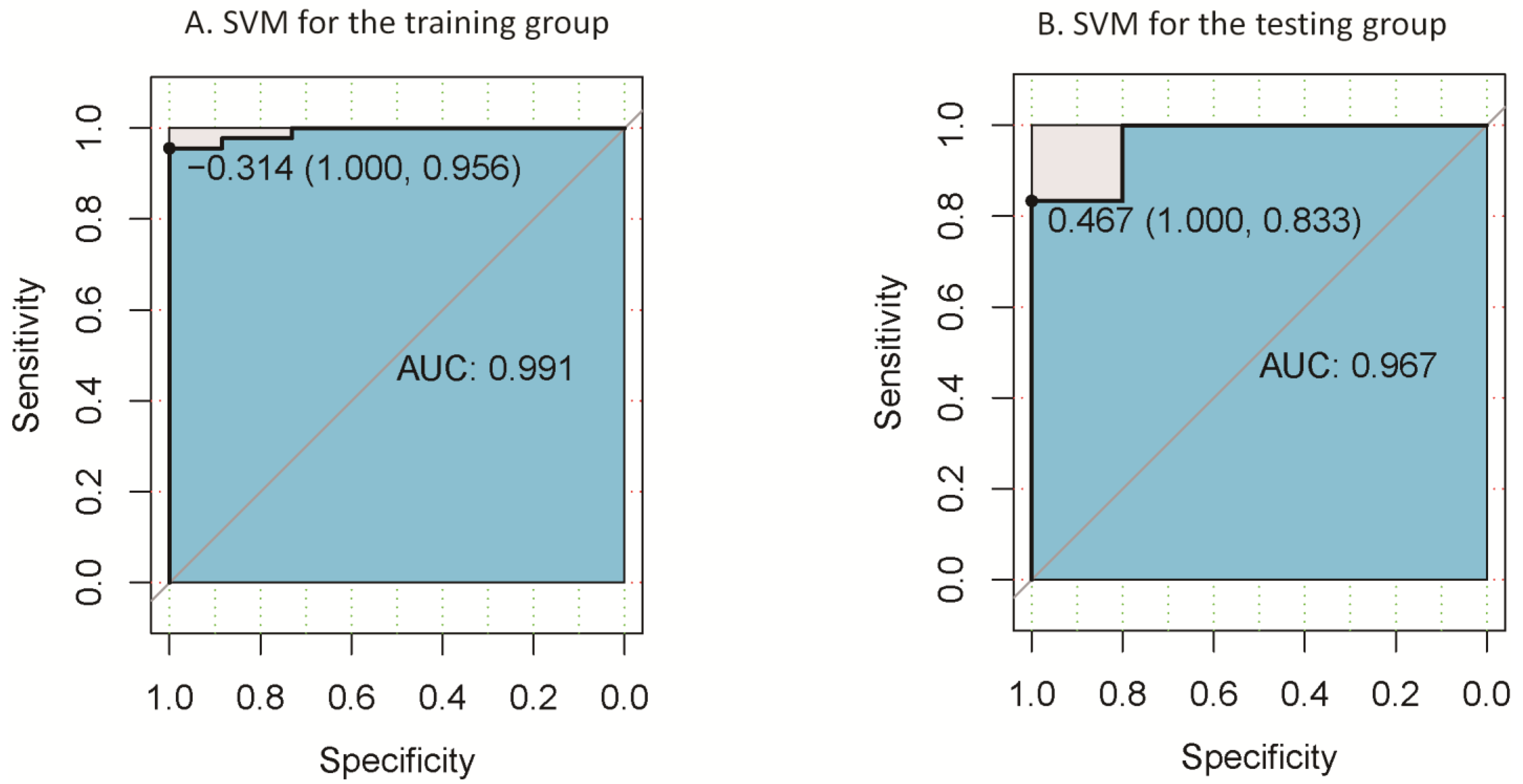
3.4. Classification Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef] [PubMed]
- Sveinbjornsdottir, S. The clinical symptoms of Parkinson’s disease. J. Neurochem. 2016, 139 (Suppl. S1), 318–324. [Google Scholar] [CrossRef] [PubMed]
- McGregor, M.M.; Nelson, A.B. Circuit Mechanisms of Parkinson’s Disease. Neuron 2019, 101, 1042–1056. [Google Scholar] [CrossRef] [PubMed]
- Michel, P.P.; Hirsch, E.C.; Hunot, S. Understanding Dopaminergic Cell Death Pathways in Parkinson Disease. Neuron 2016, 90, 675–691. [Google Scholar] [CrossRef] [PubMed]
- Barkhof, F.; Haller, S.; Rombouts, S.A. Resting-state functional MR imaging: A new window to the brain. Radiology 2014, 272, 29–49. [Google Scholar] [CrossRef] [PubMed]
- Zang, Y.; Jiang, T.; Lu, Y.; He, Y.; Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage 2004, 22, 394–400. [Google Scholar] [CrossRef]
- Choe, I.H.; Yeo, S.; Chung, K.C.; Kim, S.H.; Lim, S. Decreased and increased cerebral regional homogeneity in early Parkinson’s disease. Brain Res. 2013, 1527, 230–237. [Google Scholar] [CrossRef]
- Jiang, S.; Wang, M.; Zhang, L.; Yuan, Y.; Tong, Q.; Ding, J.; Wang, J.; Xu, Q.; Zhang, K. Regional homogeneity alterations differentiate between tremor dominant and postural instability gait difficulty subtypes of Parkinson’s disease. J. Neural Transm. 2016, 123, 219–229. [Google Scholar] [CrossRef]
- Borroni, B.; Premi, E.; Formenti, A.; Turrone, R.; Alberici, A.; Cottini, E.; Rizzetti, C.; Gasparotti, R.; Padovani, A. Structural and functional imaging study in dementia with Lewy bodies and Parkinson’s disease dementia. Park. Relat. Disord. 2015, 21, 1049–1055. [Google Scholar] [CrossRef]
- Pan, P.; Zhan, H.; Xia, M.; Zhang, Y.; Guan, D.; Xu, Y. Aberrant regional homogeneity in Parkinson’s disease: A voxel-wise meta-analysis of resting-state functional magnetic resonance imaging studies. Neurosci. Biobehav. Rev. 2017, 72, 223–231. [Google Scholar] [CrossRef]
- Liu, F.; Wang, Y.; Li, M.; Wang, W.; Li, R.; Zhang, Z.; Lu, G.; Chen, H. Dynamic functional network connectivity in idiopathic generalized epilepsy with generalized tonic-clonic seizure. Hum. Brain. Mapp. 2017, 38, 957–973. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Wei, Y.; Zhao, J.; Nie, J. (Eds.) The dynamic measurements of regional brain activity for resting-state fMRI: D-ALFF, d-fALFF and d-ReHo. roceedings of International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; pp. 190–197. [Google Scholar]
- Chen, J.; Sun, D.; Shi, Y.; Jin, W.; Wang, Y.; Xi, Q.; Ren, C. Dynamic Alterations in Spontaneous Neural Activity in Multiple Brain Networks in Subacute Stroke Patients: A Resting-State fMRI Study. Front. Neurosci. 2018, 12, 994. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Lu, F.; Hu, C.; Wang, J.; Zhang, S.; Zhang, S.; Yang, G.; Zhang, J. Dynamic alterations of spontaneous neural activity in patients with amyotrophic lateral sclerosis. Brain. Imaging Behav. 2021, 15, 2101–2108. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Li, M.; Fu, S.; Li, G.; Wang, T.; Yin, Y.; Jiang, G.; Lin, J.; Li, W.; Fang, J.; et al. Alterations of Dynamic Regional Homogeneity in Trigeminal Neuralgia: A Resting-State fMRI Study. Front. Neurol. 2019, 10, 1083. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Li, Z.; Lin, Y.; Yu, J.; Peng, G.; Zhang, K.; Jia, X.; Luo, B. Depression Affects Intrinsic Brain Activity in Patients With Mild Cognitive Impairment. Front. Neurosci. 2019, 13, 1333. [Google Scholar] [CrossRef] [PubMed]
- Wee, C.Y.; Yang, S.; Yap, P.T.; Shen, D.; Alzheimer’s Disease Neuroimaging, I. Sparse temporally dynamic resting-state functional connectivity networks for early MCI identification. Brain Imaging Behav. 2016, 10, 342–356. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, H.; Gao, Y.; Wee, C.Y.; Li, G.; Shen, D.; Alzheimer’s Disease Neuroimaging Initiative. High-order resting-state functional connectivity network for MCI classification. Hum. Brain. Mapp. 2016, 37, 3282–3296. [Google Scholar] [CrossRef]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov. Disord. 2007, 22, 1689–1707, quiz 1837. [Google Scholar] [CrossRef]
- Jia, X.-Z.; Wang, J.; Sun, H.-Y.; Zhang, H.; Liao, W.; Wang, Z.; Yan, C.-G.; Song, X.-W.; Zang, Y.-F. RESTplus: An improved toolkit for resting-state functional magnetic resonance imaging data processing. Sci. Bull. 2019, 64, 953–954. [Google Scholar] [CrossRef]
- Ashburner, J. A fast diffeomorphic image registration algorithm. Neuroimage 2007, 38, 95–113. [Google Scholar] [CrossRef] [PubMed]
- Friston, K.J.; Williams, S.; Howard, R.; Frackowiak, R.S.; Turner, R. Movement-related effects in fMRI time-series. Magn. Reson. Med. 1996, 35, 346–355. [Google Scholar] [CrossRef]
- Yan, C.G.; Wang, X.D.; Zuo, X.N.; Zang, Y.F. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics 2016, 14, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.-G.; Yang, Z.; Colcombe, S.J.; Zuo, X.-N.; Milham, M.P. Concordance among indices of intrinsic brain function: Insights from inter-individual variation and temporal dynamics. Sci. Bull. 2017, 62, 1572–1584. [Google Scholar] [CrossRef] [PubMed]
- Zalesky, A.; Breakspear, M. Towards a statistical test for functional connectivity dynamics. Neuroimage 2015, 114, 466–470. [Google Scholar] [CrossRef]
- Liu, F.; Guo, W.; Yu, D.; Gao, Q.; Gao, K.; Xue, Z.; Du, H.; Zhang, J.; Tan, C.; Liu, Z.; et al. Classification of different therapeutic responses of major depressive disorder with multivariate pattern analysis method based on structural MR scans. PLoS ONE 2012, 7, e40968. [Google Scholar] [CrossRef]
- Jenkinson, M.; Bannister, P.; Brady, M.; Smith, S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 2002, 17, 825–841. [Google Scholar] [CrossRef]
- Li, Y.; Liang, P.; Jia, X.; Li, K. Abnormal regional homogeneity in Parkinson’s disease: A resting state fMRI study. Clin. Radiol. 2016, 71, e28–e34. [Google Scholar] [CrossRef]
- Yeo, S.; Lim, S.; Choe, I.H.; Choi, Y.G.; Chung, K.C.; Jahng, G.H.; Kim, S.H. Acupuncture stimulation on GB34 activates neural responses associated with Parkinson’s disease. CNS Neurosci. Ther. 2012, 18, 781–790. [Google Scholar] [CrossRef]
- Yue, Y.; Jiang, Y.; Shen, T.; Pu, J.; Lai, H.Y.; Zhang, B. ALFF and ReHo Mapping Reveals Different Functional Patterns in Early- and Late-Onset Parkinson’s Disease. Front. Neurosci. 2020, 14, 141. [Google Scholar] [CrossRef]
- Gu, L.; Shu, H.; Xu, H.; Wang, Y. Functional brain changes in Parkinson’s disease: A whole brain ALE study. Neurol. Sci. 2022, 43, 5909–5916. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Long, X.; Zang, Y.; Wang, L.; Hallett, M.; Li, K.; Chan, P. Regional homogeneity changes in patients with Parkinson’s disease. Hum. Brain Mapp. 2009, 30, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Zhao, H.; Li, C.M.; Ma, X.X.; Chen, M.; Li, S.H.; Wang, R.; Lou, B.H.; Chen, H.B.; Su, W. The Relationship between Side of Onset and Cerebral Regional Homogeneity in Parkinson’s Disease: A Resting-State fMRI Study. Parkinsons Dis. 2020, 2020, 5146253. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wei, L.; Hu, X.; Xie, B.; Zhang, Y.; Wu, G.R.; Wang, J. Akinetic-rigid and tremor-dominant Parkinson’s disease patients show different patterns of intrinsic brain activity. Park. Relat. Disord. 2015, 21, 23–30. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K.; Rub, U.; de Vos, R.A.; Jansen Steur, E.N.; Braak, E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Cavanna, A.E.; Trimble, M.R. The precuneus: A review of its functional anatomy and behavioural correlates. Brain 2006, 129 (Pt 3), 564–583. [Google Scholar] [CrossRef]
- Nobili, F.; Abbruzzese, G.; Morbelli, S.; Marchese, R.; Girtler, N.; Dessi, B.; Brugnolo, A.; Canepa, C.; Drosos, G.C.; Sambuceti, G.; et al. Amnestic mild cognitive impairment in Parkinson’s disease: A brain perfusion SPECT study. Mov. Disord. 2009, 24, 414–421. [Google Scholar] [CrossRef]
- Tang, C.C.; Poston, K.L.; Dhawan, V.; Eidelberg, D. Abnormalities in metabolic network activity precede the onset of motor symptoms in Parkinson’s disease. J. Neurosci. 2010, 30, 1049–1056. [Google Scholar] [CrossRef]
- Syrimi, Z.J.; Vojtisek, L.; Eliasova, I.; Viskova, J.; Svatkova, A.; Vanicek, J.; Rektorova, I. Arterial spin labelling detects posterior cortical hypoperfusion in non-demented patients with Parkinson’s disease. J. Neural Transm. 2017, 124, 551–557. [Google Scholar] [CrossRef]
- Thibes, R.B.; Novaes, N.P.; Lucato, L.T.; Campanholo, K.R.; Melo, L.M.; Leite, C.C.; Amaro, E., Jr.; Barbosa, E.R.; Bor-Seng-Shu, E.; Cardoso, E.F.; et al. Altered Functional Connectivity Between Precuneus and Motor Systems in Parkinson’s Disease Patients. Brain Connect 2017, 7, 643–647. [Google Scholar] [CrossRef]
- Jia, X.; Li, Y.; Li, K.; Liang, P.; Fu, X. Precuneus Dysfunction in Parkinson’s Disease With Mild Cognitive Impairment. Front Aging Neurosci. 2018, 10, 427. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Shin, S.A.; Lee, J.Y.; Nam, H.; Lim, J.S.; Kim, Y.K. Precuneus degeneration and isolated apathy in patients with Parkinson’s disease. Neurosci. Lett. 2017, 653, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Song, X.; Li, E.; Liu, J.; Yuan, Y.; Liu, W.; Liu, Y. Altered Resting-State Brain Activity and Connectivity in Depressed Parkinson’s Disease. PLoS ONE 2015, 10, e0131133. [Google Scholar] [CrossRef] [PubMed]
- Zanigni, S.; Sambati, L.; Evangelisti, S.; Testa, C.; Calandra-Buonaura, G.; Manners, D.N.; Terlizzi, R.; Poda, R.; Oppi, F.; Lodi, R.; et al. Precuneal Thickness and Depression in Parkinson Disease. Neurodegener Dis. 2017, 17, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Hanakawa, T.; Katsumi, Y.; Fukuyama, H.; Honda, M.; Hayashi, T.; Kimura, J.; Shibasaki, H. Mechanisms underlying gait disturbance in Parkinson’s disease: A single photon emission computed tomography study. Brain 1999, 122 Pt 7, 1271–1282. [Google Scholar] [CrossRef]
- Manoliu, A.; Meng, C.; Brandl, F.; Doll, A.; Tahmasian, M.; Scherr, M.; Schwerthoffer, D.; Zimmer, C.; Forstl, H.; Bauml, J.; et al. Insular dysfunction within the salience network is associated with severity of symptoms and aberrant inter-network connectivity in major depressive disorder. Front. Hum. Neurosci. 2013, 7, 930. [Google Scholar] [CrossRef]
- Li, B.; Liu, L.; Friston, K.J.; Shen, H.; Wang, L.; Zeng, L.L.; Hu, D. A treatment-resistant default mode subnetwork in major depression. Biol. Psychiatry 2013, 74, 48–54. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD | HCs | p-Value | |
|---|---|---|---|
| No. of subjects | 57 | 31 | |
| Age | 64.16 ± 8.13 | 62.42 ± 7.19 | 0.122 |
| Gender (M/F) | 28/29 | 16/15 | 0.823 |
| Disease duration | 6.49 ± 3.59 | N/A | N/A |
| H-Y staging | 2.20 ± 0.69 | N/A | N/A |
| UPDRS | 49.90 ± 18.82 | N/A | N/A |
| MMSE | 28.05 ± 1.95 | 27.71 ± 2.25 | 0.528 |
| HAMD | 9.30 ± 5.14 | N/A | N/A |
| HAMA | 10.21 ± 5.49 | N/A | N/A |
| NMSQ | 11.30 ± 5.32 | N/A | N/A |
| Region | Cluster Size (Voxel) | MNI (x, y, z) | t-Value |
|---|---|---|---|
| Right Posterior Cerebellar Lobe | 17 | (15, −81, −54) | −5.5695 |
| Left Medial Temporal Lobe | 52 | (−27, 0, −42) | 5.1186 |
| Right Medial Temporal Lobe | 74 | (27, 9, −39) | 5.4905 |
| Right Precentral Gyrus | 123 | (39, −9, 42) | −5.7469 |
| Supplementary Motor Area | 70 | (0, 24, 48) | −5.2007 |
| Region | Cluster Size (Voxel) | MNI (x, y, z) | t-Value |
|---|---|---|---|
| Precuneus | 13 | (3, −54, 60) | 4.5626 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, K.; Tian, Y.; Chen, H.; Ma, X.; Li, S.; Li, C.; Wu, S.; Liu, F.; Du, Y.; Su, W. Temporal Dynamic Alterations of Regional Homogeneity in Parkinson’s Disease: A Resting-State fMRI Study. Biomolecules 2023, 13, 888. https://doi.org/10.3390/biom13060888
Li K, Tian Y, Chen H, Ma X, Li S, Li C, Wu S, Liu F, Du Y, Su W. Temporal Dynamic Alterations of Regional Homogeneity in Parkinson’s Disease: A Resting-State fMRI Study. Biomolecules. 2023; 13(6):888. https://doi.org/10.3390/biom13060888
Chicago/Turabian StyleLi, Kai, Yuan Tian, Haibo Chen, Xinxin Ma, Shuhua Li, Chunmei Li, Shaohui Wu, Fengzhi Liu, Yu Du, and Wen Su. 2023. "Temporal Dynamic Alterations of Regional Homogeneity in Parkinson’s Disease: A Resting-State fMRI Study" Biomolecules 13, no. 6: 888. https://doi.org/10.3390/biom13060888
APA StyleLi, K., Tian, Y., Chen, H., Ma, X., Li, S., Li, C., Wu, S., Liu, F., Du, Y., & Su, W. (2023). Temporal Dynamic Alterations of Regional Homogeneity in Parkinson’s Disease: A Resting-State fMRI Study. Biomolecules, 13(6), 888. https://doi.org/10.3390/biom13060888